
Abstract
This study describes concussions and concussion-related outcomes sustained by high school soccer players by head impact location, sex, and injury mechanism. Data were obtained for the 2012/13–2015/16 school years from the National High School Sports-Related Injury Surveillance System, High School RIO™. This Internet-based sports injury surveillance system captures data reported by athletic trainers from an annual average of 162 U.S. high schools. Data were analyzed to describe circumstances of soccer concussion (e.g., symptomology, symptom resolution, and return-to-play time) by impact location (i.e., front- [face included], back-, side-, and top-of-the-head) and sex. Most concussions were from front-of-the-head impacts (boys, 30.5%; girls, 34.0%). Overall, 4.1 ± 2.2 and 4.6 ± 2.3 symptoms were reported in boys and girls, respectively. In boys, symptom frequency was not associated with head impact location (p = 0.66); an association was found in girls (p = 0.02), with the highest symptom frequency reported in top-of-the-head impacts (5.4 ± 2.2). Head impact location was not associated with symptom resolution time (boys, p = 0.21; girls, p = 0.19) or return-to-play time (boys, p = 0.18; girls, p = 0.07). Heading was associated with 28.0% and 26.5% of concussions in boys and girls, respectively. Most player-player contact concussions during heading occurred from side-of-the-head impacts (boys, 49.4%; girls, 43.2%); most heading-related ball contact concussions occurred from front-of-the-head (boys, 41.4%; girls, 42.6%) and top-of-the-head (boys, 34.5%; girls, 36.9%) impacts. Head impact location was generally independent of symptom resolution time, return-to-play time, and recurrence among high school soccer concussions. However, impact location may be associated with reported symptom frequency. Further, many of these clinical concussion descriptors were associated with sex.
Introduction
Soccer is one of the most popular youth sports in the United States, and its large participation may be associated with the large number of reported concussions. 1 Annually, an estimated 119,831 soccer-related concussions in youth ages 7–17 years present to emergency departments in the United States. 2 The high incidence of concussions to youth and adolescents, in addition to high school boys' and girls' soccer demonstrating concussion rates consistent with American football and ice hockey, 3 warrants studying risk factors associated with concussion incidence and severity.
It is important to examine head impact characteristics because gameplay in soccer includes ball contact while heading, as well as player contact that may unintentionally occur. Recent efforts have estimated soccer-related head impact exposure, 4 –10 although concussion incidence within these samples is small. Impact location (i.e., the area on the head to which impact occurred) is one characteristic worth examining, and has been investigated in elite and collegiate soccer players. 11,12 It is difficult to extend the results on collegiate and elite soccer player to youth and adolescents, given that collegiate soccer players experience greater cumulative head impacts than high school soccer players. 5 The skill set of elite and collegiate players may also not be representative of high school players. Impact location/direction influence brain axonal injury, concussion symptom frequency, and behavioral changes, as shown in studies using finite element modeling, human subjects, and animal subjects, respectively. 13 –15 A previous injury surveillance study examined impact location attributed to player-player contact concussions in high school American football. 16 However, unlike American football, many soccer athletes are female, who have higher concussion rates and longer recovery times than males according to previous studies. 3,17 –19
Examining head impact data for soccer-related concussions will help clinicians better understand those most at risk and develop evidence-based concussion prevention interventions. Such data are also important given recent epidemiological findings on heading-related concussions 18 and the ban on heading in youth players ≤10 years of age by the United States Soccer Federation (U.S. Soccer). 20 This epidemiological study of concussions sustained in high school soccer examines the association between head impact location (i.e., front, back, side, or top) and concussion-related outcomes (i.e., reported symptoms, symptom resolution time, and participation restriction time). Given recent literature, 18 we also examine this association in the context of differences related to sex and injury mechanism.
Methods
Sample
Data were obtained from the National High School Sports-Related Injury Surveillance System, High School RIO™ (Reporting Information Online), an Internet-based sports injury surveillance system. The surveillance system, which has been described previously, 21,22 includes a U.S. high school sample having one or more National Athletic Trainers' Association–affiliated athletic trainers (ATs) with valid email addresses. The High School RIO data used for the current study utilized a convenience sample (mean = 162 schools) during the 2012/13–2015/16 school years. Given that this study is a secondary data analysis that utilizes de-identified data, human subjects review was not necessary.
Data collection
Throughout the school year, ATs from participating high schools reported injury and athlete-exposure (AE) information weekly using a secure website. For each injury, the AT completed a detailed report on the injury (body part, diagnosis, severity, etc.) and injury event (activity, mechanism, etc.). ATs could define contact type (e.g., player, ball) as an injury mechanism, but were unable to discriminate whether contact was intentional or unintentional. ATs also reported whether injured players had previously sustained concussions (i.e., injury recurrence). Throughout the study, participating ATs were able to view and update previously submitted reports with new information (e.g., return-to-play).
Starting in the 2012/13 school year, ATs reported additional information regarding concussions sustained from all injury mechanisms, including the head impact location: back, front (including the face), side, top, or unknown (i.e., AT stated that he or she did not know, or AT did not report). ATs also reported symptoms, symptom resolution time, and return-to-play time. Symptoms utilized in RIO originate from those used within the National Collegiate Athletic Association Injury Surveillance System. 23 As with all captured data, we relied on ATs' expertise to determine the correct values for these variables. However, the actual method of detecting head impact location was not reported (e.g., observation, video review).
Injury and exposure definitions
An AE was defined as 1 athlete participating in a school-sanctioned practice or competition. Reported concussions included those that 1) resulted from participation in a school-sanctioned practice or competition and 2) required medical attention by an AT or physician. We did not provide a definition of concussion, because we relied on the expertise of each medically trained professional that reported concussion data to the High School RIO surveillance system.
Statistical analysis
We calculated injury rates as the number of concussions per 10,000 AEs, injury rate ratios (IRRs), injury proportion ratios (IPRs), chi-square tests (χ
2
), and Fisher's exact tests when insufficient sample sizes were present for chi-square tests. These analyses first focused on sex differences, followed by differences by head impact location within each sex. When examining differences in injury rates, we also replicated analyses within each head impact location. An example of an IRR comparing competition and practice rates is:
An example of an IPR comparing the reporting of drowsiness associated with concussions from impacts to the top of the head versus all other head impact locations is:
All analyses were conducted with SAS software (version 9.3; SAS Institute, Cary, NC). Significance level for all analyses was set a priori at p < 0.05.
Results
Concussion incidence and rates, by head impact location and sex
Participating ATs reported 1350 soccer-related concussions during 2012/13–2015/16 (Table 1). Most occurred in girls (67.5%) and during practices (80.9%). Regardless of injury mechanism (player-player contact or ball-player contact), most concussions were from front-of-the-head impacts (boys, 30.5%; girls, 34.0%), followed by the side-of-the-head (boys, 28.7%; girls, 26.7%), back-of-the-head (boys, 16.9%; girls, 15.8%), and top-of-the-head (boys, 3.6%; girls, 6.5%) impacts. An additional 244 concussions (18.1%) had an unknown impact location.
Concussion Frequencies, Injury Rates a , and Injury Rate Ratios Sustained in High School Soccer, by Head Impact Location, High School Sports-Related Injury Surveillance Study, United States, 2012/13–2015/16
Rates per 10,000 Athlete-Exposure.
AT stated that he or she did not know impact location, or AT did not report impact location (i.e., missing).
CI, confidence interval.
The 1350 concussions occurred during 1,271,931 AEs, for an injury rate of 10.61 per 10,000 AEs (95% confidence interval [CI], 10.05–11.18). The concussion rate was higher in competition than in practice in both boys (IRR = 8.78; 95% CI, 6.97–11.07) and girls (IRR = 10.06; 95% CI, 8.51–11.90). Concussion rates were higher in girls than boys overall, by event type, and within each head impact location group (Table 1). Head impact location distributions did not vary between competition and practice in boys (p = 0.44) and girls (P = 0.54); thus, further analyses combined competition and practice data.
Symptomatology
On average, 4.1 ± 2.2 and 4.6 ± 2.3 symptoms were reported among boys and girls, respectively (Table 2). Symptom frequency was higher in girls than boys (p = 0.001); however, when examined within each head impact location, only back-of-the-head impacts retained significance (p = 0.01). Among boys, symptom frequency was not associated with head impact location (p = 0.66). Among girls, symptom frequency was associated with head impact location (P = 0.02), with the highest average number reported in top-of-the-head impacts (5.4 ± 2.2).
Distributions of Reported Symptom Frequencies with Concussions among U.S. High School Soccer Athletes, by Impact Direction, High School Sports-Related Injury Surveillance Study, United States, 2012/13–2015/16
AT stated that he or she did not know impact location, or AT did not report impact location (i.e., missing).
SD, standard deviation.
Commonly reported symptoms included headache (boys, 94.8%; girls, 96.3%), dizziness/unsteadiness (boys, 74.5%; girls, 74.8%), and difficulty concentrating (boys, 51.7%; girls, 58.9%; Fig. 1). Symptoms more commonly reported among boys than girls included amnesia (p = 0.002) and loss of consciousness (p = 0.01). Head impact location was not associated with any single symptom among boys. Symptoms more commonly reported among girls than boys included difficulty concentrating (p = 0.01), drowsiness (p = 0.002), irritability (p < 0.001), nausea (p = 0.01), sensitivity to light/visual disturbance (p = 0.004), and sensitivity to noise (p < 0.001). Among girls, head impact location was associated with drowsiness (p = 0.05) and sensitivity to light (p = 0.009). Top-of-the-head impact concussions had larger proportions of reported drowsiness (IPR = 1.51; 95% CI, 1.17–1.94) and sensitivity to light (IPR = 1.31; 95% CI, 1.10–1.57) compared to all other concussions.
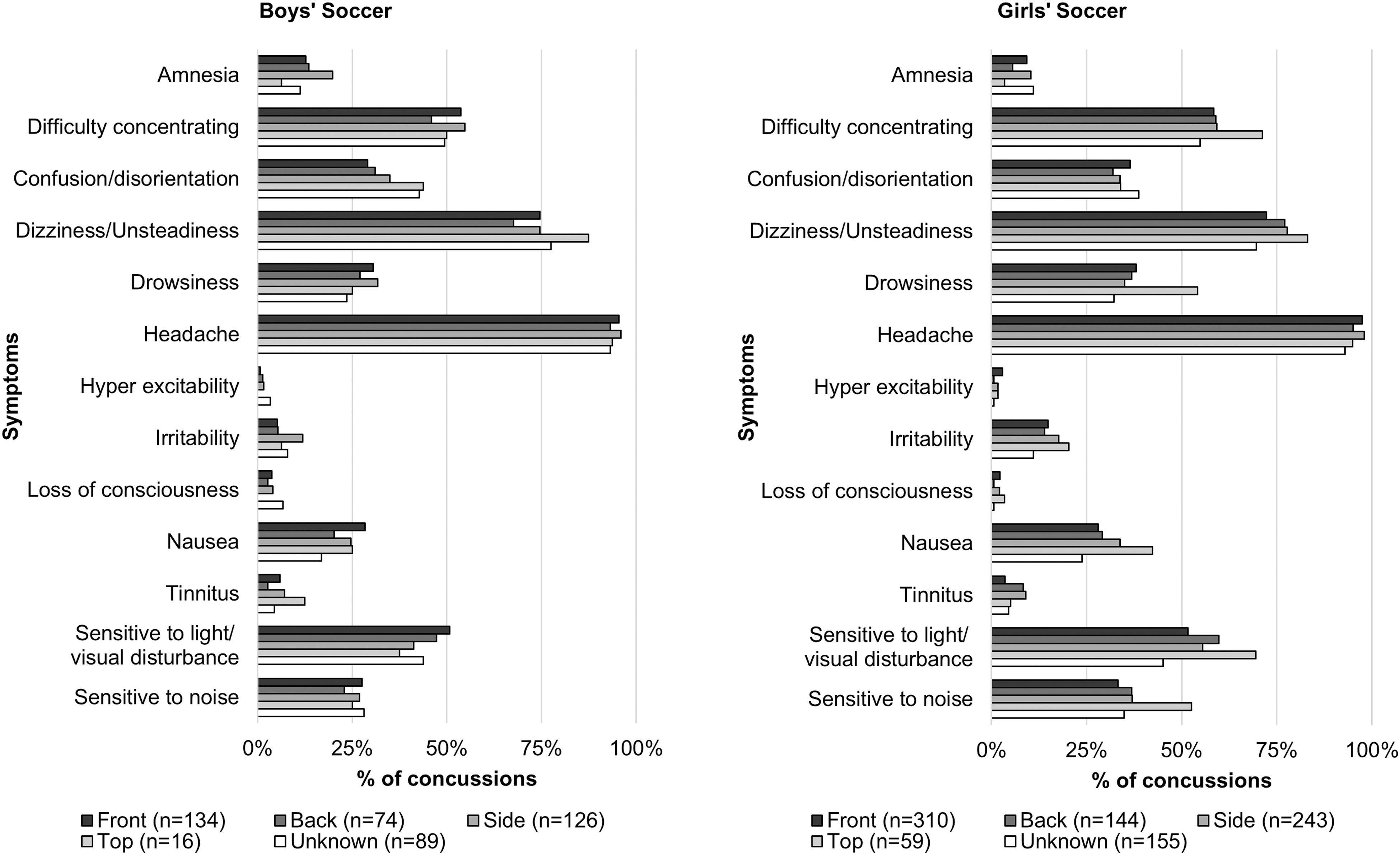
Proportion of concussions in U.S. high school soccer with reported symptoms, by head impact location, High School Sports-Related Injury Surveillance Study, United States, 2012/13–2015/16.
Symptom resolution time and return-to-play
Data on symptom resolution time were missing for 130 concussions (9.6%). For injuries with documented symptom resolution time data, most resolved within a week (boys, 66.6%; girls, 51.5%). Sex was associated with symptom resolution time (p < 0.001). The proportion of concussions requiring at least 1 week for symptom resolution was higher in girls than boys (IPR = 1.45; 95% CI, 1.24–1.70). Head impact location was not associated with symptom resolution time in boys (p = 0.21) or girls (p = 0.19).
Data on return-to-play time were missing for 125 concussions (9.3%). For injuries with documented return-to-play time data, most returned within 3 weeks (boys, 62.1%; girls, 60.4%). Sex was not associated with return-to-play time (p = 0.08). Head impact location was also not associated with return-to-play time in boys (p = 0.18) or girls (p = 0.07).
Recurrence
Sixteen concussions were missing recurrence data. Among all concussions with recurrence data, 6.9% and 10.5% were reported to be recurrent in boys and girls, respectively. Injury recurrence was associated with sex (p = 0.03); the proportion of concussions that were recurrent was higher in girls than boys (IPR = 1.52; 95% CI, 1.03–2.26). Injury recurrence was also associated with impact location among boys (p = 0.02), with top-of-the-head impacts having the largest proportion of concussions that were recurrent (12.5%), followed by unknown (11.9%), front-of-the-head (9.7%), back-of-the-head (4.1%), and side-of-the-head (1.6%) impacts. Injury recurrence was not associated with impact location among girls (p = 0.83).
Playing position
Data on playing position were missing for 159 concussions (11.8%). Positions comprising the most concussions were midfield (boys, 40.1%; girls, 40.3%) and defense (boys, 24.0%; girls, 25.0%). Sex was not associated with playing position (p = 0.96). Head impact location was not associated with playing position in boys (p = 0.58) or girls (p = 0.30).
Injury mechanism
Among boys, most were attributed to player-player contact (58.8%), followed by ball contact (23.0%). Similarly, among girls, most were attributed to player-player contact (42.3%), followed by ball contact (36.9%; Table 3). Among both boys and girls, most player-player contact concussions occurred from side-of-the-head (boys, 35.3%; girls, 34.0%) and front-of-the-head (boys, 29.1%; girls, 31.9%) impacts; however, most ball contact concussions occurred from front-of-the-head (boys, 48.5%; girls, 46.1%) impacts. All other mechanisms were associated with back-of-the-head impacts (boys, 41.3%; girls, 35.3%). Concussion rates were higher among girls than boys, overall, and when restricted to player-player contact or ball contact concussions. In addition, similar findings were found when stratified by head impact location.
Concussion Frequencies, Injury Rates a , and Injury Rate Ratios Sustained in High School Soccer, by Injury Mechanism and Head Impact Location, High School Sports-Related Injury Surveillance Study, United States, 2012/13–2015/16
Rates per 10,000 Athlete-Exposure.
AT stated that he or she did not know impact location, or AT did not report impact location (i.e., missing).
CI, confidence interval.
Heading-related concussions
Heading was associated with 28.0% and 26.5% of soccer concussions in boys and girls, respectively (Table 4). Commonly reported symptoms in heading-related concussions included headache (boys, 95.9%; girls, 96.7%), dizziness/unsteadiness (boys, 69.1%; girls, 75.9%), and difficulty concentrating (boys, 54.5%; girls, 64.3%). Most heading-related concussions were attributed to player-player contact (70.7%) among boys, followed by ball contact (23.6%). Among girls, most were attributed to ball contact (50.6%), followed by player-player contact (46.1%). Among both boys and girls, most heading-related, player-player contact concussions were attributed to head-to-head contact (boys, 74.4%; girls, 78.0%) and occurred from side-of-the-head (boys, 49.4%; girls, 43.2%) and front-of-the-head (boys, 31.0%; girls, 30.6%) impacts; however, most heading-related ball contact concussions occurred from front-of-the-head (boys, 41.4%; girls, 42.6%) and top-of-the-head (boys, 34.5%; girls, 36.9%) impacts. Heading-related concussion rates were higher in girls than boys, overall, and when restricted to player-player contact or ball contact concussions. Similar findings were found when stratified by head impact location.
Concussion Frequencies, Injury Rates a , and Injury Rate Ratios Sustained in High School Soccer While Heading the Ball, by Injury Mechanism and Head Impact Location, High School Sports-Related Injury Surveillance Study, United States, 2012/13–2015/16
Rates per 10,000 Athlete-Exposure.
AT stated that he or she did not know impact location, or AT did not report impact location (i.e., missing).
CI, confidence interval; n/a, not applicable.
Discussion
Head impact location was generally independent of differences in symptomology, symptom resolution time, return-to-play time, and recurrence among high school soccer players sustaining concussions. However, many of these clinical concussion descriptors were associated with sex. In particular, sex was associated with injury mechanism. Boys sustained a greater proportion of heading-related concussions from player-player contact, whereas girls sustained a greater proportion of heading-related concussions from ball contact.
Head-impact location findings
As in previous research in American football samples, 16,24,25 we found unequal head impact distributions related to concussions, with most occurring from front-of-the-head impacts. However, the symptom frequencies reported, symptom prevalence, symptom resolution time, return-to-play time, and recurrence were generally independent of impact location. An interesting exception was related to top-of-the-head impacts. In girls' soccer, concussions from top-of-the-head impacts had more symptoms than other impact locations and were more likely to be associated with drowsiness and sensitivity to light. In boys' soccer, concussions from top-of-the-head impacts resulted in the highest percentage of recurring concussions compared to other head impact locations. Top-of-the-head impacts in high school football have also been related to larger average symptom frequencies and increased concussion reoccurrence than front and back impact locations. 16 It is unclear how the interaction between top-of-the-head impacts and concussions is related to symptom frequency, increased symptom severity, and recurrent concussion risk. Concussion is thought to be a diffuse brain injury predominately caused by head rotation motion that creates brain axon shearing injury and disruption. 26,27 Concussions resulting from top-head-impacts do not fit head rotation concussion injury models. Maximal and minimal intracranial pressures can develop at the parietal cortex and the posterior cranial fossa during axial loading (top-head impacts), as demonstrated with finite element simulations, and may provide some insight into the relationship between top-head impacts causing concussion and clinical outcomes. 28 However, this remains largely speculative given that intracranial pressure changes are associated more with more-severe traumatic brain injuries, 29 whereas concussion is associated more with brain tissue shearing. 27 In addition, there is little overlap between the brain structures that are subjected to changes in intracranial pressures during top-head impacts, the associated brain structures' function, and the increased symptom types that were reported in the current study. Future research is warranted to better understand skull and brain loading during top-of-head impact events across all sporting events.
Similar to previous studies, 18 the most common injury mechanism was player-player contact and ball contact, which are situations commonly associated with contesting for the ball. 18 For both boys and girls, concussions most frequently occurred from side-of-the-head and front-of-the-head impacts in player-player contact scenarios. Findings were similar when examining heading-related concussions only. During heading events in competition, both players are contesting for the ball while it is in the air; although not documented in the current study, it is likely that each player's head was coming into contact at the side or front while trying to compete for the ball. Techniques to protect players from side-of-the-head and front-of-the-head impacts could be a starting point to better head protection during contested soccer heading events. It is important that these techniques are performed during uncontested and contested sessions during practice to ensure the players can transfer these skills to competition. This underscores the need for policy on heading exposures during practices. It also suggests teaching standardized programming may be warranted. Such programs, such as the National Soccer Coaches Association of America “Get aHEAD in Soccer,” emphasize safe heading techniques so that players are able to better protect their personal space while attempting headers in the air. 30 Further, U.S. Soccer has set forth guidelines banning heading in players ≤10 years and limiting heading exposure in practices for players 11–13 years. 20 Many of these policies do not affect our sample of high school students. Longitudinal concussion incidence monitoring alongside evaluative research on guideline compliance is necessary to better gauge long-term effects of these heading policies.
Sex difference findings
Sex is an important factor associated with concussion incidence and outcomes. Research has hypothesized why sex differences exist. 31,32 Theories range from the biological (neck muscle strength differences) 33 to the sociocultural (concussion symptom disclosure differences). 34,35 Despite these advances in hypothesis generation, more research specifically testing these hypotheses is encouraged. One notable finding in our study is related to injury mechanisms in heading-related concussions. Heading-related concussions were mostly attributed to player-player contact in boys, but almost equally distributed between ball contact and player-player contact in girls. Previously published soccer heading-related concussion research using the same epidemiological data collection system in academic years preceding our current study period demonstrated less-pronounced sex differences. Our data suggest that more girls' soccer concussions are reportedly attributed to ball contact in more recent years. 18 Distributions in head impact location did not vary by sex among heading-related concussions within each injury mechanism stratum. Given the limitations with data collected by surveillance, it is difficult to understand the reasons for which such sex differences exist. For example, the data could not discriminate whether contact was intentional/unintentional or anticipated/unanticipated. Further examination into these contact types is warranted given that errant/unintentional deflected balls—not purposeful heading—may be more likely to produce injurious head impacts. 36
Non-heading-related findings
Although much attention on concussions has focused on heading, and recent findings suggest that 90% of head impacts in collegiate women's soccer are from heading, 6 only 28.0% and 26.5% of all concussions in our study with reported head impact location were attributed to heading in boys and girls, respectively. Most concussions were attributed to non-heading-related activities. Defending, chasing after loose balls, and goaltending make up most of the non-heading-related concussions. 18 Although these concussions comprise the greater proportion of concussions, the current study did not characterize non-heading-related concussions in terms of factors such as on-field location and anticipated/unanticipated contact. Future surveillance efforts, coupled with etiological studies, can continue to better characterize soccer-related concussion epidemiology. At the same time, using head impact sensor technology in soccer-related research has increased recently. 4,6 –8 Integrating this with other data collection methods, such as video footage, 37,38 may help yield interesting and novel findings. Combining these efforts could lead to prevention programs to improve current prevention methods emphasizing “heads up/eyes up play,” which we believe will lead to greater open field collision anticipation.
Strengths and limitations
Our sample was limited to high schools with ATs and may not be generalizable to non-participating high schools or other levels of play (e.g., college, professional). Although the High School RIO Surveillance System captured symptomatology data related to sustaining concussions, numerous symptoms (i.e., sadness, trouble falling asleep, feeling like one is “in a fog,” and feeling “slowed down”) included in other symptom lists (Graded Symptom Checklist, Acute Concussion Evaluation, and Post-Concussion Symptom Scale) were not listed options in this surveillance system. In addition, RIO did not obtain specific information regarding how data specific to head impact location were collected (e.g., observation, video review). However, RIO relied upon medically trained professionals to document injuries, which results in higher-quality data than studies that relied upon coach reporting or player self-report. 39 Although consistency in assessing and diagnosing concussions among various providers is lacking, there is a consistent sports concussion definition accepted and widely publicized by an international expert group through periodic Consensus Statements on Concussion in Sport. 40 Further, ATs receive up-to-date and specific education regarding sports-related concussions diagnosis.
Conclusion
Impact location was generally independent of differences in concussion symptomology, symptom resolution time, return-to-play time, and recurrence. However, our study suggests that sex may be a more important clinical risk factor than head impact location. Given limitations with injury surveillance data, there is a continued need to examine methods to collect concussion and head impact data that are valid and reliable, yet cost-effective. Future research should investigate the diagnostic sensitivity and positive predictive value using varying data collection methods, including AT reporting, video replay, and head impact sensors.
Footnotes
Acknowledgments
The content of this report representing data collection by the National High School Sports-Related Injury Surveillance Study (High School Reporting Information Online) was funded, in part, by the Centers for Disease Control and Prevention grants R49/CE000674-01 and R49/CE001172-01. We also acknowledge the generous research funding contributions of the National Federation of State High School Associations, the National Operating Committee on Standards for Athletic Equipment, DonJoy Orthotics, and EyeBlack. The content of this report is solely the responsibility of the authors and does not necessarily represent the official views of the Centers for Disease Control and Prevention or any of the other institutions that provided financial support for this research.
Author Disclosure Statement
No competing financial interests exist.