
Abstract
The aims of this study were to document the frequency of major and minor depressive episodes in the first year after traumatic brain injury (TBI), taking into account TBI severity and pre-morbid history of major depression, and to describe trajectories of depressive episodes. Participants were 227 adults who were hospitalized post-TBI (76% male; mean age = 41 years; 50% mild, 33% moderate, and 17% severe TBI). Major and minor depressive episodes were assessed with the Mini International Neuropsychiatric Interview at three time points (4, 8, and 12 months after TBI). Overall, 29% of participants had a major depressive episode in at least one of the three assessments, with fairly stable rates across assessments. Participants with mild TBI were more likely than those with moderate/severe TBI to be diagnosed with major depression, as were individuals with a positive pre-morbid history of depression compared to those without such history. In addition, 13% of participants had a minor depressive episode in at least one of the three assessments. Rates of minor depression significantly decreased from 4 to 8–12 months post-injury. Results also revealed a wide variety of trajectories of depressive episodes across assessments. Of note, 52% of major depression cases still fulfilled diagnostic criteria 4 months later, whereas 38% of minor depression cases deteriorated to major depression at the following assessment. These findings suggest that depression is highly prevalent after TBI, and monitoring of patients with subthreshold depressive symptoms is warranted in order to prevent the development of full-blown major depressive episodes.
Introduction
T
Whereas depression appears to be equally frequent across TBI severity levels (i.e., mild-to-severe TBI), 17 –19 there may be injury severity-related differences in the time course of depression. For instance, one study found that individuals with delayed depression in the first year post-injury were more likely to have a severe TBI compared to those with low depression. 20 Also, more severely brain-injured individuals are believed to show impairments in self-awareness, which may be a protective factor buffering, to some extent, against the development of psychological distress after the injury. 21,22 As awareness develops, however, psychological distress is thought to increase. As such, individuals sustaining milder TBIs may be at risk of distress earlier because of their increased awareness of their deficits and prompter return to the community setting and to their pre-injury activities. 23
The first year post-TBI is a particularly critical period for depression. 1,24 Recently, Bombardier and colleagues 20 established four typical trajectories of depression within the first year in 559 individuals consecutively admitted for TBI at a U.S. Level 1 trauma center: low depression (around 70% of patients), delayed depression (13%), recovered depression (10%), and persistent depression (6%). This study used a cutoff on a self-reported measure, the nine-item depression module from the Patient Health Questionnaire (PHQ-9), to establish the presence of depression. Also using the PHQ-9, Hart and colleagues 17,25 suggested that minor and major depression form a continuum and that depressed individuals with TBI tend to fluctuate across these states as time goes by after the injury. Also supporting the observation of a continuum of depression severity, Alway and colleagues 1 found that a subsyndromal form of depression was the second-most common form of mood disturbance they documented after TBI.
A challenge faced by professionals during rehabilitation is to evaluate whether the distress, sadness, or frustration exhibited by patients is part of a normal response to an abnormal situation, 6 or if it, in fact, represents a pathology in need of treatment. In addition to an increased neurobiological vulnerability to depression potentially brought about by the injury, 26,27 TBI survivors go through major stressors attributed to the multitude of challenges they may face to adjust to sequelae and reintegrate into the community. Some clinicians, families, or patients themselves may assume that depressive symptoms are part of the normal recovery process during a certain period. One problem with this assumption is that the duration of the adjustment period is unknown and probably varies significantly from one individual to another. The challenge then becomes distinguishing between depressive symptoms that do not interfere with recovery, functioning, or rehabilitation interventions, and symptoms that are accompanied by clinically significant distress or impairment. If clinicians assume that depressive symptoms are normal and expected in the first year post-TBI, then there is a risk of not identifying individuals who are significantly depressed, and for whom a short and focused intervention could prevent a full-blown major depressive episode. 28
Following up on the work of Bombardier's and Hart's teams, 17,20,25 we wished to obtain a better understanding of the trajectory of minor and major depression in the first year post-injury using gold-standard neuropsychiatric assessments in a sample including the whole spectrum of injury severity from mild to severe. The first aim of the current study was to document the frequency of major and minor depressive episodes at three time points in the first year after TBI (4, 8, and 12 months post-injury), taking into account injury severity and pre-morbid history of major depression. We hypothesized that the rates of depression would be higher in individuals with milder injuries in the early months post-injury, and that depression would be more frequent in patients with a positive history of depression. The second aim was to describe trajectories of depression in the first year post-TBI. It was anticipated that, regardless of injury severity, among those with minor depression, a significant proportion would go on to develop a full-blown major depression episode in subsequent assessments.
Methods
The study protocol was approved by the ethical review boards of two healthcare facilities who collaborated in the study, the CHU de Québec-Université Laval (Level I trauma center) and the Institut de Réadaptation en Déficience Physique de Québec (IRDPQ; rehabilitation center).
Participants
Participants were adults between 18 and 65 years of age hospitalized in a Level I trauma center (CHU de Québec-Université Laval, Hôpital de l'Enfant-Jésus) after sustaining a TBI (mild, moderate, or severe). All patients with TBI consecutively admitted between April 2010 and November 2013 were approached to participate during their hospitalization. Individuals with a past history of neurological disease, such as stroke, moderate or severe TBI, brain tumor, or multiple sclerosis, were excluded. Spinal cord injury concomitant to the TBI and an inability to understand written or oral information in French or English or to provide informed consent were also grounds for exclusion.
Severity of the TBI is determined by physicians at the trauma center and is based on provincial guidelines, 29 which use the World Health Organization definition of TBI. 30,31 According to this definition, TBI results from an energy transfer from an external source to the skull and underlying structures, characterized by: 1) alteration or loss of consciousness (mild TBI, <30 min; moderate, <24 h; severe, >6 h); 2) post-traumatic amnesia (mild, <24 h; moderate, generally 1–14 days; severe, several weeks); 3) any transitory neurological sign such as any focal neurological sign, convulsion, or intracranial lesion (mild: positive or negative brain imaging results, possible neurological signs; moderate: generally positive brain imaging results, presence of focal neurological signs; severe: positive brain imaging results and presence of focal neurological signs); and 4) the initial score on the Glasgow Coma Scale (GCS) 32 (mild, 13–15; moderate, 9–12; severe, 3–8).
Procedure
Potential participants meeting selection criteria were identified by a research nurse working at the CHU de Québec-Université Laval. The nurse first obtained verbal consent from patients or their family (while they were on the ward) to be contacted at a later date by the research team. If they agreed, an information pamphlet on the study was provided. Approximately 3 months after TBI, the study coordinator contacted potential participants over the phone (or in person for those who were in inpatient rehabilitation three months post-injury) to provide information about the study. Individuals interested in participating were given a consent form and an appointment for the first interview. Sociodemographic characteristics were collected during this first contact with the research coordinator. Information about the injury, including the severity of the TBI, was obtained by consulting the medical records of participants at the trauma center. The study involved three assessments, conducted 4, 8, and 12 months (±2 weeks) after the injury. Each assessment included a face-to-face or telephone interview and a self-reported questionnaire sent out by mail. This article only reports data derived from the interviews. Participants received a compensation of $20 after each completed assessment. The research coordinator placed reminder calls 24–48 h before each interview and provided information regarding medical, psychiatric, and rehabilitation resources when needed.
Main outcome
Major and minor depressive episodes
These were assessed with the Mini International Neuropsychiatric Interview (MINI) for the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 33 a semistructured clinical interview for Axis I disorders based on the DSM-IV nosology. The validated French version of the MINI was used. 34 A major depressive episode (major DE) was defined as a period of at least 2 weeks, within the 4 months preceding the interview, with five or more of the nine core symptoms of depression, including depressed mood and/or loss of interest, and significant distress or functional impairment associated with the depressive symptoms. A minor depressive episode (minor DE; a research criteria set included in the DSM-IV in the “Criteria sets and axes for further study”) was defined as a period of at least 2 weeks with two to four of the nine symptoms of depression, including depressed mood and/or loss of interest, and associated distress or functional impairment. Pre-TBI (lifetime) history of major DEs and minor DEs was also assessed using the MINI at the first interview completed with the participant. During the interviews, participants were asked to list all medications they were using currently (they were encouraged to refer to their list of medication provided by their pharmacy). Their responses were categorized into medication classes, including antidepressants.
Interviewers and quality assurance
Phone and in-person interviews were conducted by three licensed psychologists and 5 graduate students in clinical psychology who had all completed at least their first year of doctoral studies, including courses and a practicum in psychological assessment and diagnosis. Interviewers were all individually trained to administer the MINI and supervised by a senior psychologist. Monthly team meetings with all interviewers, the first author and the senior psychologist were held during which complex cases were reviewed and differential diagnosis issues were resolved through consensus. All phone and in-person interviews were recorded and 14% (82 interviews of 576 total) were randomly selected and recoded by an independent interviewer who had not interviewed the participant, and did not consult the first coding. Inter-rater reliability was examined by computing Gwet's AC1 statistic 35 for each Axis I diagnosis (presence/absence). AC1 is an adjustment of Cohen's kappa statistic, which is unreliable when the events being measured are rare, as is the case with psychiatric diagnoses. 36 Gwet's AC1 was 0.87 for major DE and 0.90 for minor DE, suggesting very good reliability.
Statistical analyses
All analyses were performed using IBM SPSS Statistics for Windows (version 19). 37 Proportions of patients fulfilling the diagnostic criteria for a major or a minor DE at least once in the first year after TBI was calculated. The sample size allowed sufficient power to generate 95% confidence intervals (CIs) with ±6% of precision. For the first objective (rate of depression), generalized estimating equations were 38,39 used to model each binary dependent variable (presence/absence of major DE, presence/absence of minor DE), with three factors: severity of TBI (two-level nonrepeated factor: mild, moderate/severe TBI), pre-morbid history of major DE (two-level nonrepeated factor: positive, negative), and time (three-level repeated factor: 4, 8, and 12 months post-TBI). Main effects and two-way interactions were examined. When a significant main effect of time or interaction was found, post-hoc tests were computed and a Bonferroni correction was applied. With regard to the working correlation matrix, the exchangeable matrix (compound symmetry) was preferred over other options because of better (i.e., lower) corrected quasi-likelihood under independence model criteria. Among individuals not meeting criteria for either major or minor depression, the frequency of endorsement of individual symptoms of depression was reported for each time point.
All possible trajectories were described to determine the most common trajectories across the three assessments; trajectories of two consecutive assessments were examined to further document the persistence of depression in the sample. All occurrences of major DEs at 4 and 8 months were grouped together, and depression status at the next assessment (at 8 months for major DEs at 4 months, at 12 months for major DEs at 8 months) was described. The same procedure was applied for cases of minor DEs at 4 and 8 months and for cases without depression at 4 and 8 months. For this analysis of two-time trajectories, the total number of observations was 338: data from 168 participants at 4 months (time 1) who also completed the 8-month assessment (time 2), in addition to data from 170 participants at 8 months (time 1) who also completed the 12-month assessment (time 2). Therefore, participants could be accounted for more than once in the analysis.
Results
Sample description
From April 2010 to November 2013, there were 786 patients admitted to the trauma center with a diagnosis of TBI (Fig. 1). Of these, 427 patients were eligible. Among these, 87 were missed or could not be reached, and 104 declined to take part in the research when approached by the research nurse. The remaining 236 individuals (55% of eligible patients) were enrolled and completed at least one interview or questionnaire in the first year post-injury. Because the main outcome measures of the current article are depression diagnoses documented with the interview, 9 participants were not included in the analyses because they did not complete any of the three interviews, yielding a final sample of 227 participants (76% male, mean age of 41 years, and 50% moderate/severe TBI; see Table 1). Of these, 200 completed the interview at 4 months, 191 at 8 months, and 185 at 12 months post-injury. A total of 154 individuals completed all three interviews. Of the 576 interviews, 28% were conducted in person and 72% over the phone. Participants who were receiving inpatient or outpatient rehabilitation services were more likely to choose the face-to-face interview modality, given that the research center is located within the rehabilitation center. This could explain the gradually decreasing rate of face-to-face over time (37% at 4 months, 29% at 8 months, 19% at 12 months). Compared to eligible nonenrolled patients with available data (n = 168), participants were significantly more likely to have suffered a moderate/severe TBI compared to nonincluded participants (50% vs. 33%; χ2 (1, N = 386) = 10.86, p = 0.001; Cramer's V = 0.17). Enrolled and nonenrolled patients did not significantly differ on age (41.3 ± 15.1 vs. 40.6 ± 14.8 years; F (1, 388) = 0.25, p = 0.62; Cohen's d = 0.05), or sex (24% vs. 21% women; χ2 (1, N = 395) = 0.63, p = 0.43; Cramer's V = 0.04).
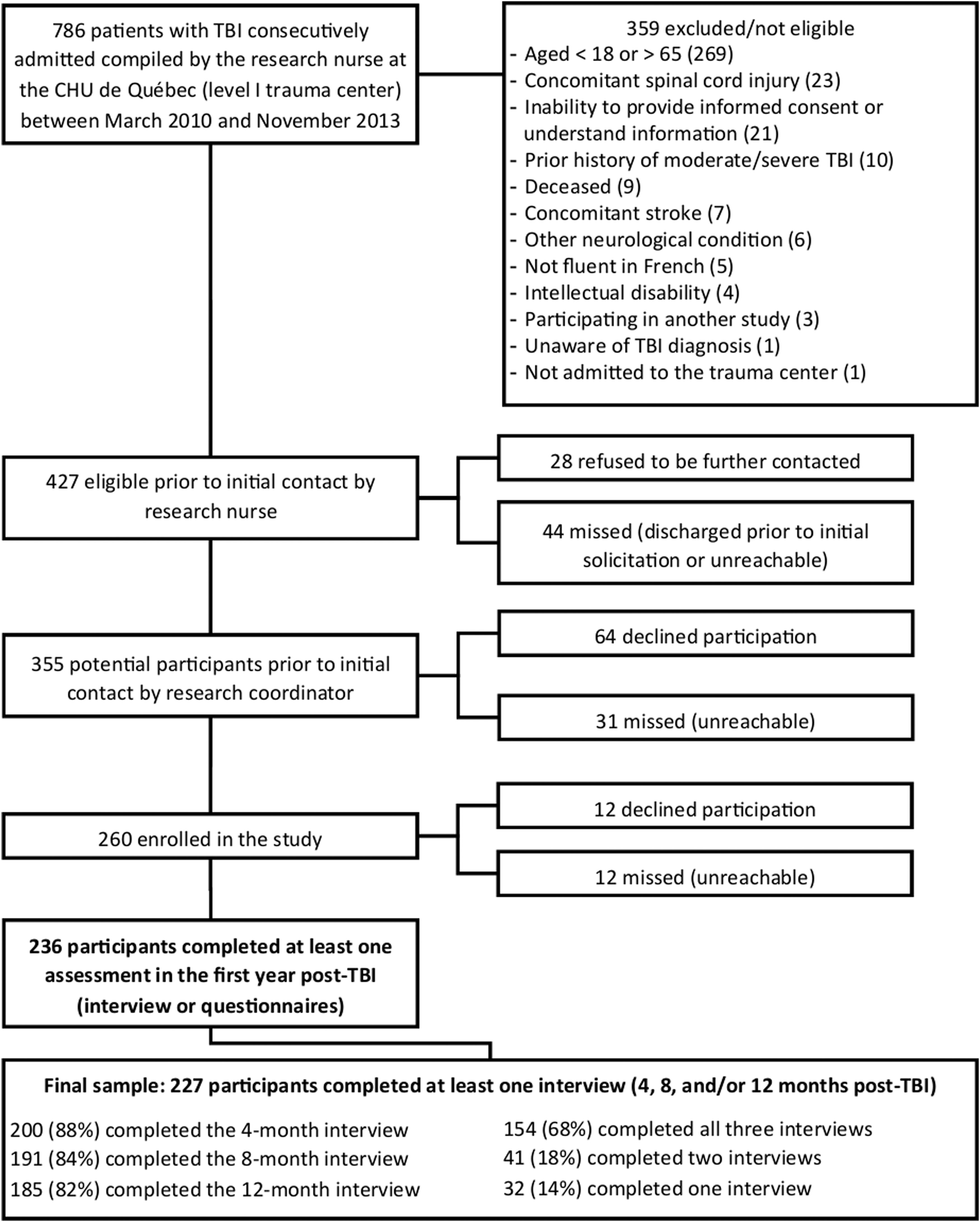
Flow chart of participants. TBI, traumatic brain injury.
All variables were self-reported, except Glasgow Coma Scale score, severity of TBI, and mechanism of injury, which were extracted from medical records.
TBI, traumatic brain injury; M, mean; SD, standard deviation.
Objective 1: Depression rates
Overall, 65 participants (28.6%) had a major DE at least once in the first year after TBI, whereas 30 other participants (13.2%) had a minor DE at least once in the first year without having a major DE at any assessment. Results of the severity × pre-morbid history of major DE × time generalized estimating equations, for each binary dependent variable (presence of major DE, minor DE), are shown in Table 2. The main time effect was not significant for major DE, suggesting stable rates over time overall. However, there was a significant time effect for minor DE, with post-hoc tests revealing a greater percentage of participants with minor DE at 4 months (16%) than at 8 (6%) and 12 months (8%) post-TBI. There was a significant effect of TBI severity for major DE, with participants with mild TBI being more likely to be diagnosed with a major DE compared to those with moderate/severe TBI, regardless of time (see Fig. 2A). Mild and moderate/severe TBI subgroups did not significantly differ on their rates of minor DE over time. As for the effect of pre-morbid history of major DE, participants with a positive history were more likely to present a major DE after the injury compared to those with a negative history, regardless of time. The effect of pre-morbid history of major DE was not significant for minor DE. There was no significant severity × time, pre-morbid history of major DE × time, or severity × pre-morbid history of major DE interaction for either major DE or minor DE (see Fig. 2B).

Frequency of minor and major DE at 4, 8, and 12 months according to (
Percentages and 95% CIs are estimated marginal means from the generalized estimating equations, for the total number of observations (e.g., data for mild and moderate/severe TBI subgroups combine the three assessment times). Statistics presented are Wald's chi-square, with the degrees of freedom and the total number of observations of the dependent variable for all three times combined. Levels with different letter subscripts (a,b) are significantly different from each other according to post-hoc tests with Bonferroni correction.
p < 0.05.
DE, depressive episode; TBI, traumatic brain injury; Mod/Sev, moderate/severe; CI, confidence interval.
Complementary analyses were conducted to determine whether there was a difference in depression rates between interview modalities and age groups. There was no significant difference between face-to-face and telephone interviews on the rates of major DE (18.7% vs. 15.8%; χ2 (1, N = 576) = 0.60, p = 0.44) or minor DE (8.4% vs. 9.2%; χ2 (1, N = 576) = 0.08, p = 0.77). There was no significant difference between three age groups on rates of major DE (18–30 years, 17%; 31–50 years, 16%; 51–65 years, 15%; χ2 (2, N = 576) = 0.18, p = 0.92) or minor DE (18–30 years, 9%; 31–50 years, 9%; 51–65 years, 8%; χ2 (2, N = 576) = 0.15, p = 0.93).
Antidepressant medication use was reported by 37.5% of participants with a major DE at 4 months, 48.3% at 8 months, and 62.5% at 12 months. For individuals with a minor DE, these rates were 20.0%, 27.3%, and 42.9%, respectively, whereas for participants with neither major nor minor depression, antidepressant use was reported by 15.7%, 15.4%, and 15.2%, respectively.
Figure 3 presents the proportion of participants endorsing depressive symptoms without meeting criteria for major or minor DE (but these may include persons with other Axis I disorders). The percentage reporting a period of at least 2 weeks with either depressed mood or loss of interest for most of the day, nearly every day (the two cardinal symptoms of depression), was 19.5% at 4 months, 9.5% at 8 months, and 9.7% at 12 months. Suicidality was also reported by 12% of participants without a minor or major DE at 4 months, 9% at 8 months, and 5% at 12 months; in 24% of these cases, another psychiatric disorder was diagnosed (i.e., anxiety, substance use, or adjustment disorder).
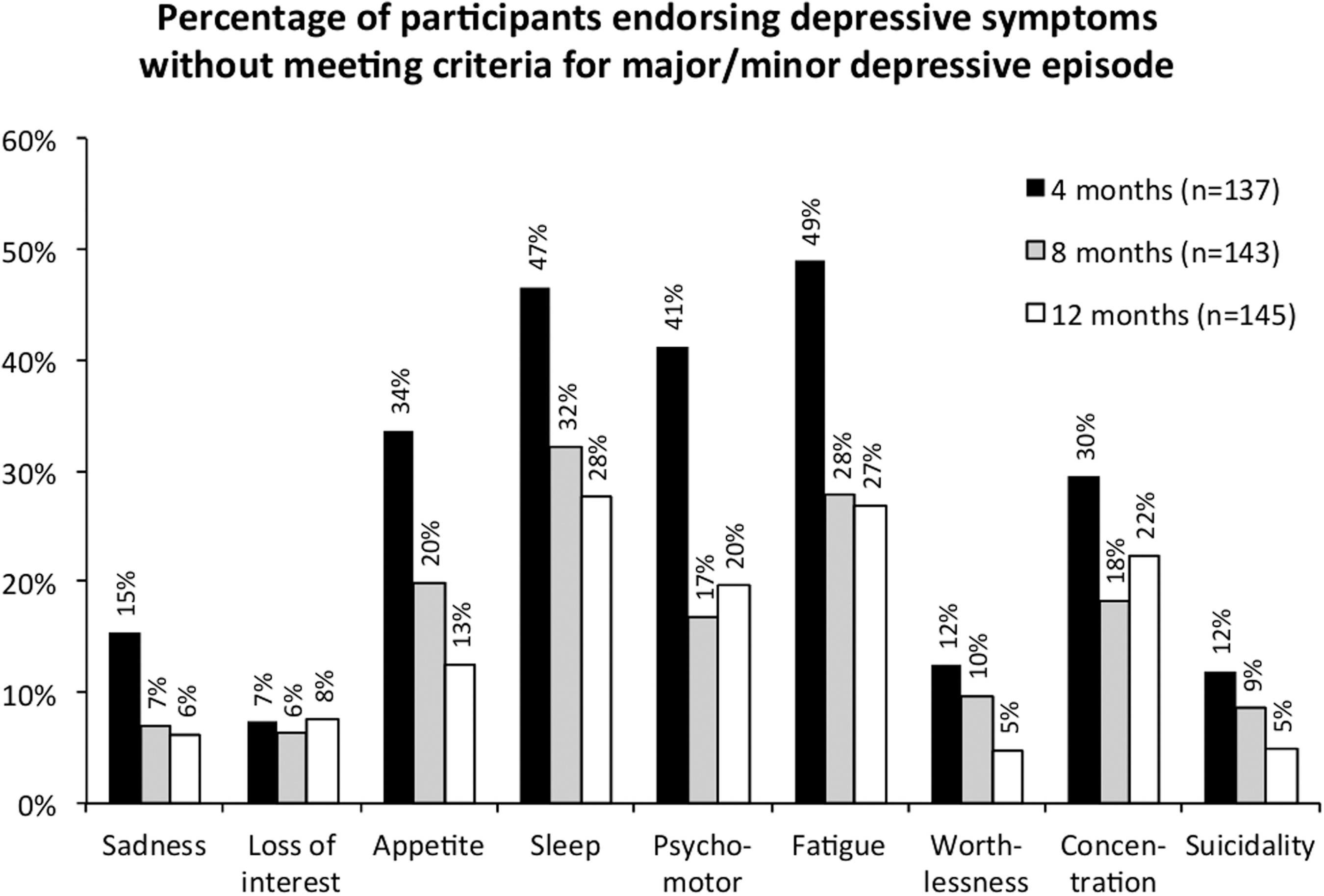
Percentage of persons without either major or minor depression endorsing each symptom of major depression at 4, 8, and 12 months post-injury.
Objective 2: Trajectories of depression
Among the 154 participants with complete data at all three assessments, 19 trajectories of depression were observed (when considering all possible combinations of either major, minor, or no depressive episode at each assessment). The most common trajectory was the absence of depression at the three time points (n = 90; 58%). The next four most common trajectories were: 1) major DE at 4 months, followed by no depression at 8 and 12 months (n = 9; 6%); 2) minor DE diagnosis at 4 months, followed by no depression at 8 and 12 months (n = 8; 5%); 3) no depression at 4 and 8 months, followed by major DE at 12 months (n = 6; 4%); and 4) no depression at 4 and 8 months, followed by minor DE (n = 6, 4%). Ten participants (6%) had a diagnosis of either minor DE or major DE at all three time points, including 5 participants with major DE at all assessments (3%).
Two-time trajectories of depressive episodes for the 338 interviews conducted at time 1 (4 or 8 months) for which data were also available at the following assessment (8 or 12 months) are shown in Figure 4. Among the 50 cases of major DE observed at time 1, 52% still had a major DE at time 2 (persistence), 2% had minor DE (partial recovery), and 46% were without depression (full recovery). Among the 37 cases of minor DE at time 1, 38% evolved into major DE at time 2 (aggravation), 16% were still categorized as minor DE (persistence), and 46% were without depression (recovery). Finally, among the 251 cases without depression at time 1, 5% developed a major DE and 6% developed a minor DE at time 2 (incidence), and 74% remained without depression.
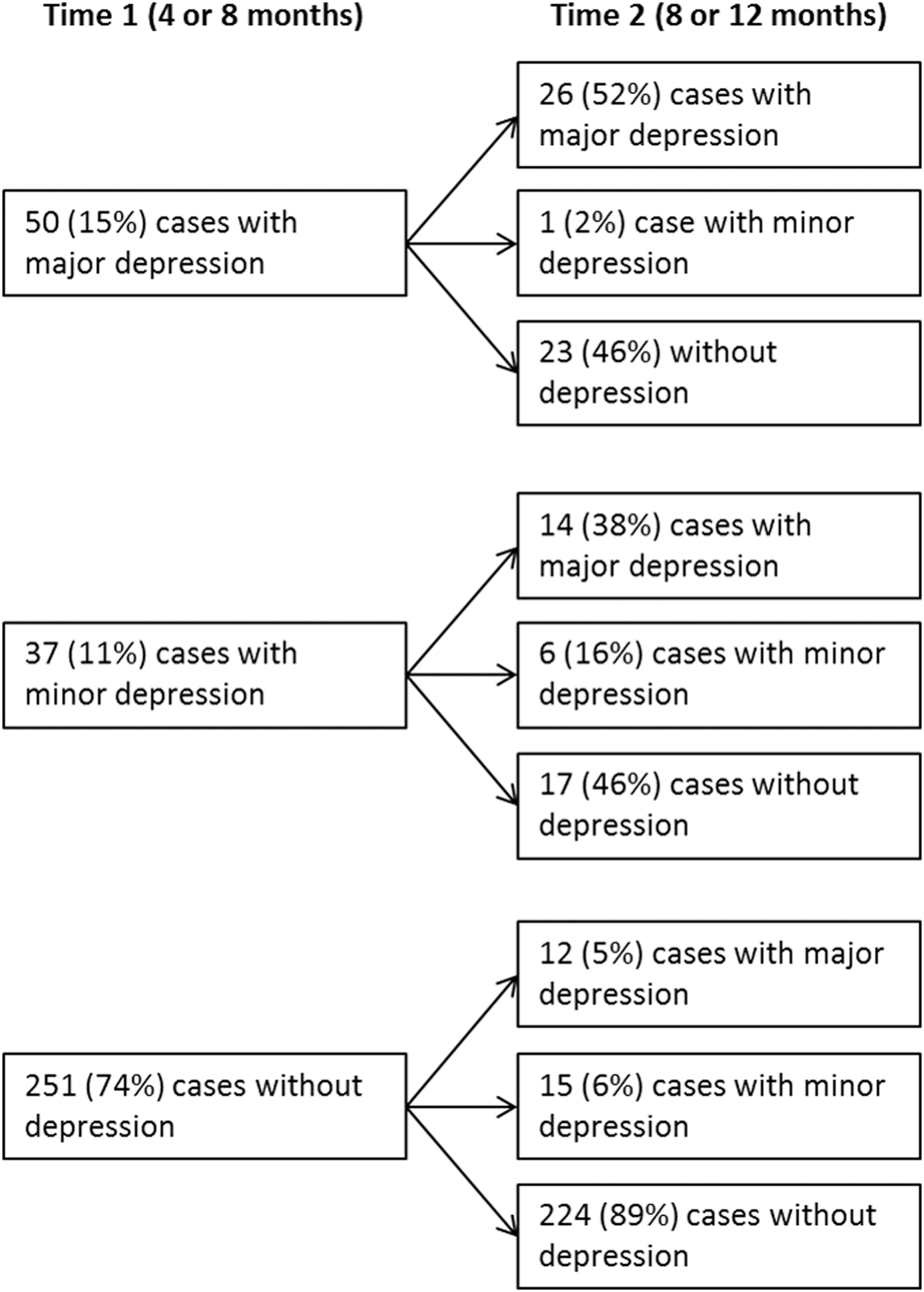
Two-time trajectories of cases with major, minor, or no depression. The total number of observations is 338: data from 168 participants at 4 months (time 1) who also completed the 8-month assessment (time 2) + data from 170 participants at 8 months (time 1) who also completed the 12-month assessment (time 2).
Discussion
In this study, we aimed to evaluate the rates and trajectories of major and minor depressive episodes during the first year after TBI, while taking into account injury severity and pre-morbid history of major depression. Using strict criteria with a DSM-based semistructured interview and trained interviewers, we found that, overall, 42% of participants were diagnosed with either minor (13%) or major (29%) DE at any one time point with a variety of potential trajectories. Although recovery of depressive episodes may occur in approximately half of cases, persistence or even worsening (i.e., minor depression converting into major depression) is at least as likely. Overall, a higher rate of major DE was found after mild TBI compared to moderate/severe TBI, and in individuals with a pre-morbid history of major DE compared to those without. These results highlight clearly the need to reassess periodically the presence, nature, and severity of depressive symptoms throughout the first year post-injury, at least.
Our results are comparable to that of Gould and colleagues 40 who also used gold-standard semistructured psychiatric interviews over the first year post-injury, although their sample was composed of persons having sustained predominantly moderate or severe TBI. In this study, they observed that 29.4% of their sample suffered from a major depressive disorder in the first 12 months post-injury. The depression rates observed in our study are, however, lower than those reported by another group using the PHQ-9, 41 who observed a cumulative rate of major depression of 53% over the first year post-injury. The use of different assessment methods likely explains the differences and may be capturing different severity ranges of the depressive continuum. In any event, the presence of major depression in our TBI sample is evaluated to be at least 6 times greater than the Canadian general population estimated at 4.7% over a 12-month period in 2013. 42
Minor depression, a category that was included in the DSM-IV for further study (but no longer included in the DSM-V), was diagnosed in 13% of our participants. Other studies have documented variants of subthreshold depressive disorders, one, for instance, reporting that 19.6% of their sample had a depressive disorder not otherwise specified (predominantly subthreshold depression). 40 Some researchers have suggested that minor depression may be as common as major depression after TBI and that it should be taken as seriously because of its association with increased disability, greater substance use, lower social participation, and lower quality of life, although to a lesser degree than major depression. 17 Unfortunately, the association between minor depressive episodes and such other negative outcomes was not be verified in the present study.
For individuals not meeting criteria for either major or minor depression, we nonetheless found that between 9% and 19% (depending on the time point) reported a period of at least 2 weeks with depressed mood or loss of interest (most of the day, nearly every day) in the last 4 months. Depressive symptoms are thus fairly common post-TBI, even in those not fulfilling criteria for a depressive episode, which renders the task difficult for clinicians, loved ones, and patients themselves to recognize when symptoms are no longer a manifestation of normal adaptation to the consequences of the injury, and merit professional attention. Contrary to major DE, minor DEs were observed more frequently at 4 months post-injury and were unrelated to pre-injury history of major depression, and, as such, these episodes could represent markers of more difficult adaptation to the consequences of the injury for some individuals.
Evaluating depression after TBI can be challenging. Several symptoms of depression, such as fatigue, attention/concentration problems, or difficulty with decision making, can be present, but it may be quite difficult to determine whether these are attributable to the injury itself (or its consequences, such as hospitalization) or to a psychological effect of the multiple stressors that characterize this condition. Our data show that fatigue, sleep disturbance, and psychomotor retardation, for example, are frequently observed in persons without depression (see Fig. 3). Interestingly, previous research has suggested that including symptoms such as fatigue or sleep disturbances does not lead to overdiagnosis of post-TBI depression. 28,43 However, our findings suggest that it may add to the difficulty clinicians have in deciding whether or not to attend to these symptoms, and whether they are part of a depressive syndrome. A careful evaluation of the cardinal symptoms of depression seems particularly important given that they may represent the beginning of a more serious condition.
Although previous studies did not find a link between depression and injury severity, 9,17,18,41,44,45 we observed that individuals with milder injuries were more frequently depressed in the early months post-injury. The fact that not all of these studies have prospectively studied depression at different time points during the first year post-injury may explain this discrepancy. In our study, the percentage of persons suffering from major DE was twice as high in the mild subgroup compared to the moderate/severe subgroup at the 4-month assessment, but this difference lessened at the subsequent time points. A greater awareness about TBI-related changes in persons with milder injuries compared to more severe cases, 21,22 prompter return home and to activity, and possibly less access to services may partly explain these findings. Persons with mild TBI are often conscious and bothered by the subtle difficulties they are experiencing while reintegrating their pre-injury activities, 46 although the current data cannot corroborate this assumption because self-awareness/anosognosia was not formally assessed. In many cases, return to activity is rapid and does not allow for a gradual habituation to lingering symptoms, thus possibly enhancing psychological distress. Because most patients with mild TBI do not receive rehabilitation care or are not systematically followed up, it potentially reduces the possibility of their mental health issues being identified and treated.
The effect of past history of major depression on the incidence of DE was clear in our study, with rates more than 3 times higher as compared to those without antecedents. This result is in line with those from a previous prospective study, 40 which observed that a history of a depressive disorder increased by 5.25 times the odds of suffering from major depression post-injury. These data call for effective evaluations of pre-injury psychiatric histories to help identify patients at increased risk of developing a depressive disorder after TBI.
Our trajectories indicate that 52% of persons who reported a major DE will still fulfill the criteria for the same diagnosis at an assessment taking place 4 months later. Further, 38% of individuals fulfilling the criteria for minor depression will go on to develop major depression within the next 4 months, confirming that this subthreshold form of depression must be taken very seriously. On a more positive note, trajectories do indicate that almost half (46%) of all individuals who suffer either a major or a minor DE no longer fulfill diagnostic criteria for a DE 4 months later (although it cannot be excluded that a relapse could occur in the future).
The results of our study suggest that persistence and worsening of depression is at least as possible as recovery (spontaneous or facilitated by services), thus calling for a watchful waiting approach including continuous monitoring (e.g., with scheduled screenings) over several months and even years after the injury. The present data also argue for a health service organization which allows easy re-entry into mental health services specialized for TBI in the months and years after the injury. Even in persons who have seemingly recovered from major depression, long-term monitoring may be necessary given that it is well known that a major DE is an important risk factor for a subsequent one. 15 As proposed by the National Institute for Health and Care Excellence guidelines and other researchers, 47,48 watchful waiting may go beyond active symptom monitoring, and can involve patient education about coping styles, and encouraging behavioral activation or engagement in regular physical exercise. Our data indicate that individuals without depression 4 months after TBI have a very good chance of remaining depression free in the first year at least. Nonetheless, around 11% are likely to experience depression, minor or major, in the next 4–8 months, thus suggesting that even in this subgroup it would be useful to implement some form of longer-term mental health monitoring and provide information about when and where to consult if their mental health deteriorates. It is now clear that TBI is a major risk factor for psychiatric illness, 1,49 and it is now widely accepted that TBI is a chronic condition. 50 As such, major clinical and scientific efforts should thus be geared toward preventing the development of psychiatric issues and promoting resilience, adaptation, and well-being. Ideally, these preventive efforts would involve teaching patients durable skills, for example, cognitive and behavioral strategies.
Our study results have to be interpreted in light of some limitations. First, despite our efforts to approach all adults hospitalized after a TBI, the final sample may not be completely representative of the target population, given that participants with mild TBI were more likely to be missed or refuse participation initially. Second, missing data may have altered the results given that participants who dropped out of the study may differ from those who completed all three assessments. However, our dropout rates are relatively low for a longitudinal study with individuals with TBI, and we used statistical models that are known to be robust to missing data. Third, psychiatric symptoms reported by individuals with TBI, especially when interviews were conducted over the phone, may have been compromised by a reluctance for self-disclosure, social desirability bias, recall bias (especially for premorbid history), or anosognosia. Fourth, there is a lack of data on the types of treatment received by participants, because medication data are self-reported and information on other interventions such as psychotherapy is missing. Several key methodological aspects strengthen the current cohort study, however, namely its longitudinal design including individuals with mild to severe TBI. The use of semistructured interviews based on the DSM, such as the MINI, represent a gold-standard approach in neuropsychiatry. Moreover, the training and supervision of interviewers, and an inter-rater reliability check for 14% of interviews, which yielded very high agreement, reinforce the integrity of diagnoses.
Our study highlights the significant proportion of persons suffering from depressive symptoms and the delicate balance between pathological and nonpathological states, with individuals fluctuating between these as their life adjusts after the injury. There is a clear need to be extremely attentive to depressive symptoms, at least by watchfully monitoring patients, and ideally putting into place preventive and early interventions. For those already suffering from full-blown depressive episodes, psychological and pharmacological therapies adapted to the specific needs of these patients are warranted and need to be further researched. Future research also needs to examine how depressed TBI survivors are identified, evaluated, and treated, and to understand why some persons do not seek treatment or do not have access to treatment.
Footnotes
Acknowledgments
The authors thank all participants who volunteered to take part in the study, Patricia Chabot, RN, and Nancy Lemieux, RN, who identified potential participants, Andrée-Anne Paradis-Giroux, PhD, for coordinating the final part of the data collection, Jean Leblond, PhD, for statistical advice, the graduate students who conducted interviews (Sarah Lavoie-Dugré, DPsy, Guillaume Lamontagne, DPsy, Danielle Tessier, DPsy, Alexandra Champoux-Tremblay, DPsy, and Stéphanie Ropars, DPsy), and the undergraduate students who collaborated with data entry. This study was supported by a grant from the Fonds de recherche du Québec–Santé (FRQ-S; 16375).
Author Disclosure Statement
No competing financial interests exist.