
Abstract
The aim of this study was to evaluate cognitive function 10 years after moderate-severe traumatic brain injury (TBI) and to investigate the associations among cognitive function, depression, and health-related quality of life (HRQoL). In this prospective cohort study, with measurements at 3, 6, 12, 18, 24, 36, and 120 months post-TBI, patients 18–67 years of age (n = 113) with moderate-severe TBI were recruited. Main outcome measures were depression (Center for Epidemiologic Studies-Depression Scale [CES-D]), subjective cognitive functioning (Cognitive Failure Questionnaire [CFQ]), objective cognitive functioning, and HRQoL (Medical Outcomes Study 36-Item Short Form Health Survey [SF-36]). Fifty of the initial 113 patients completed the 10 year follow-up. Twenty percent showed symptoms of depression (CES-D ≥ 16). These patients had more psychiatric symptoms at hospital discharge (p = 0.048) and were more often referred to rehabilitation or nursing homes (p = 0.015) than non-depressed patients. Further, they also had significantly lower scores in six of the eight subdomains of the SF-36. The non-depressed patients had equivalent scores to those of the Dutch norm-population on all subdomains of the SF-36. Cognitive problems at hospital discharge were related with worse cognitive outcome 10 years post-TBI, but not with depression or HRQoL. Ten years after moderate-severe TBI, only weak associations (p < 0.05) between depression scores and two objective cognitive functioning scores were found. However, there were moderate associations (p < 0.01) among depression scores, HRQoL, and subjective cognitive functioning. Therefore, signaling and treatment of depressive symptoms after moderate-severe TBI may be of major importance for optimizing HRQoL in the long term. We did not find strong evidence for associations between depression and objective cognitive functioning in the long term post-TBI. Disease awareness and selective dropping out may play a role in long-term follow-up studies in moderate-severe TBI. More long-term research is needed in this field.
Introduction
T
Long-term cognitive functioning was investigated by Ponsford and coworkers, who followed 141 mild-severe TBI patients at 2, 5, and 10 years post-injury, with the Structured Outcome Questionnaire, a patient-reported outcome measurement instrument, and found that >60% of the participants reported memory problems and >50% reported difficulty concentrating, slowed thinking, cognitive fatigue, and word-finding difficulties. 8 Problems with planning, initiative, self-centeredness, and impulsivity were reported by 25–45% of the sample. 8 In the TBI Model Systems Database, it was found that of the 292 patients followed up to 5 years after TBI, only 16% reached the maximum score on the Cognitive subdomain of the Functional Independence Measure (FIM) at 1 year, after which 26% improved, 61% stayed the same, and 14% worsened at 5 years post-injury. 9 Marsh and coworkers performed neuropsychological tests on the domains of: intelligence, attention, verbal and visual memory, visual-spatial construction, and executive functions, 5 years after moderate-severe TBI. 10 Although the prevalence of impairment varied across the cognitive domains, the data showed deficits in all six domains and pointed out that complete cognitive recovery in the long term is unlikely. 10 In a review article by Dikmen and coworkers, the association between severity of TBI and cognitive deficits in the available literature was investigated. 12 The authors found clear evidence for an association between severe TBI and cognitive deficits 6–12 months post-injury. Only one study was performed 6 years after injury, and established that 70% of the severe TBI patients had clinically significant impairments, with learning and memory problems being the most common (56%). 12 For moderate TBI, they concluded that the evidence is limited/suggestive for an association with cognitive impairments. 12
The abovementioned studies agree that severity of TBI is related to cognitive deficits. Although depression is an important factor that may have a negative influence on cognitive functioning, the literature on the relationship between cognitive outcome and emotional state is limited, especially in the long term. Ponsford and coworkers compared cognitive functioning and emotional state between patients with good outcome and those with poor outcome based on the Glasgow Outcome Scale Extended (GOSE) 10 years post-TBI, but did not directly study the relationship between cognitive outcome and emotion. 13
Two review articles describe the increased prevalence of depression post-TBI; therefore, the presence of depression may influence the assessment of cognitive function. 14,15 However, it remains unclear whether cognitive function and emotional state are related in the long term post-TBI. From previous studies, we do know that health-related quality of life (HRQoL) is affected by symptoms of depression in the general population. 16 Also in TBI patients, relationships between symptoms of depression and HRQoL have been described. 17 –19
To our knowledge, no studies were performed on HRQoL and depression in relation to cognitive outcome in the long term (> 5 years) in moderate-severe TBI. Therefore, the aim of the present study was to evaluate cognitive functioning 10 years after moderate-severe TBI, and to investigate the associations among cognitive function, depression, and HRQoL in these patients.
Methods
Procedure
The design of the Rotterdam TBI study has been described in detail elsewhere. 20,21 In short, after informed consent and with approval of the Medical Ethics Committee (MEC), patients with moderate or severe TBI were consecutively enrolled between January 1999 and April 2004 at three Dutch level 1 trauma centers and prospectively followed. Measurements were completed at hospital discharge, and at 3, 6, 12, 18, 24, and 36 months post-TBI. In 2012, the Rotterdam TBI Study was extended with a 10 year-follow-up visit, which was approved by the MEC. New informed consent was obtained from all participants.
Participants
Inclusion criteria for the Rotterdam TBI study were admission to a hospital for moderate (Glasgow Coma Scale [GCS] score of 9–12) or severe (GCS score of 3–8) TBI caused by a non-penetrating trauma, and age at injury between 16 and 67 years. Exclusion criteria were insufficient knowledge of the Dutch language to participate in the study or important pre-traumatic neurological, oncological, or systemic impairments (e.g., spinal cord injury, psychiatric disorder, or cancer) that could interfere with TBI-related disability assessment. For the extended 10 year follow-up measurement, all patients who were originally included were approached and asked for participation.
Measurement instruments
Primary outcome
Questionnaires
Ten years post-injury, depression was measured with the Center for Epidemiologic Studies-Depression Scale (CES-D). The scale consists of 20 items, and scores range from 0 to 60; the higher the score, the more depressive symptoms are present. Scores of ≥16 are considered an indication of depression. 22 Up to 3 years after TBI, depression was measured with the Wimbledon Self Report Scale, on which a score >8 was considered symptomatic for depression. 23
The Cognitive Failure Questionnaire (CFQ) measures self-perceived cognitive mistakes in daily life based on 25 items. 24 Test subjects answer on a five point scale (range 0–4) how often they experience cognitive failures in daily life. A total score is calculated (range 0–100). The higher the score, the more cognitive mistakes are perceived. “Normal” scores range from 21 up to 43 (mean 31.8, SD 11.1). A cutoff score >43 was used to distinguish normal from abnormal scores. 25
The Functional Assessment Measure (FAM) was used to measure cognitive functioning at hospital discharge. The FAM was developed as an adjunct to the FIM to specifically address cognitive, behavioral, communication, and community functioning measures. The FAM consists of 12 items, and total scores range from 12 (totally dependent) to 84 (totally independent). 26
Neuropsychological tests
The Trail Making Test (TMT) A and B measures processing speed (TMT-A) and divided attention (TMT-B). 27 The test subject is asked to draw a line, in consecutive order, between numbers (TMT-A). On the TMT-B, test subjects need to switch between numbers and letters. The time needed to complete both these tasks is corrected for age and education and converted into T scores. T scores <40; for example, 1 SD below the mean, are defined as lowered scores.
The Digit Span (DS) is a subtest of the Wechsler Adult Intelligence Scale-III and measures attention and working memory. 28 Subjects are instructed to repeat numbers forward and backward. Raw scores are obtained for span length forward (DS-F) and backward (DS-B). Lowered span lengths are defined as fewer than five digits on the DS-F and fewer than four digits on the DS-B.
The Fifteen Word Task (15WT), the Dutch version of the Auditory Verbal Learning Test, was used to measure short and long-term memory and memory recognition. 29,30 Subjects were instructed to recall 15 unrelated words immediately after listening to them (repeated five times). After 20 min, a delayed recall and a recognition task is performed. Raw scores are calculated for the immediate total recall (15WT-TR; range 0–75), and delayed recall (15WT-DR; range 0–15). Raw scores are converted into decile scores corrected for age, gender, and education for both subscores. Decile scores <2.0 are defined as lowered scores.
The modified Six Elements Test (6ET) was used to measure executive function, and is part of the Behavior assessment of Dysexecutive Syndrome Test (BADS). 31 Test subjects are instructed to work on six tasks within 10 min, taking into account two rules. Based on the number of attempts and rules broken, a score of 1–4 is given.
The d2 test of attention was used to measure visual selective attention, processing speed and concentration. Participants need to identify as many as possible ‘d’ symbols in a specified period of time. A total performance score and a concentration performance score are calculated. The total performance score is calculated from the total of processed items minus total missed items and total wrong items; the concentration performance score is based on the total identified correct items minus total identified wrong items. 32
HRQoL
To assess HRQoL the Dutch version of the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36) was used. 33 –35 This is a reliable and valid instrument for several medical disorders, including TBI. 34,36,37 The SF-36 consists of 36 items measuring eight domains: Physical Functioning; Role Physical (the extent to which physical health interferes with daily activities); Bodily Pain; General Health; Vitality; Social Functioning; Role Emotional (the extent to which emotional health interferes with daily activities); and Mental Health. All domains are converted into a scale from 0 to 100, with 100 indicating the best potential condition. The eight domain scores were summarized into a physical component summary score (PCS) and a mental component summary score (MCS). The PCS and MCS are scored using norm- based methods; they both have a mean of 50 and an SD of 10 in the general United States population. 38 Age-adjusted norm values from the Dutch normative population were used. 34
Statistical analysis
Descriptive data of interval variables are presented with means and SDs and for categorical variables with numbers and proportions. Variables of interest included patient characteristics (age, gender, partner, educational level, pre-injury employment status), injury severity variables (length of hospital stay, TBI severity (moderate [GCS 9–12] or severe [GCS 3–8]), functional outcomes at hospital discharge (psychiatric symptoms [yes/no], GOS, Barthel Index [BI], FIM, FAM) and hospital discharge destination (home, rehabilitation center, nursing home). Differences between patients who were included and patients who were lost-to-follow-up were analyzed using X2 or exact tests for categorical data, and independent samples t tests for interval variables. The same statistical tests were used to compare patient characteristics, HRQoL, and cognitive functioning between two subgroups of persons with and without symptoms of depression.
Bivariate two tailed Pearson (for interval scales) and Spearman (for ordinal scales) correlations were used to study associations between the depression score (CES-D), HRQoL (PCS and MCS), cognitive functioning at hospital discharge (FAM), and subjective (CFQ) and objective cognitive functioning scores (d2, DS, TMT, 15WT, 6ET). Correlation coefficients <0.5 were considered to be weak, those between 0.5 and 0.7 were considered to be moderate, and those >0.7 were considered to be strong.
P values <0.05 were considered significant in all analyses. All statistical analyses were performed using SPSS for Windows version 21.0.
Results
Study population
All patients who previously participated in the Rotterdam TBI study (n = 113) were contacted by mail or phone. From these patients, 7 patients died during follow-up, 16 were untraceable, 20 refused to participate in the long-term follow-up, and 19 were unable to participate for logistical reasons (work obligations, on holiday, or abroad for the long term). Therefore, 51 patients were able to take part in the 10 year follow-up measurement. The drop-out rate was 17% after 3 years and 56% after 10 years of follow-up, of which 6% died. In one patient, no scores were available for depression and cognition and therefore, this patient was excluded. Patients who were included (n = 50) did not differ significantly from patients without 10 year follow-up (n = 63) in baseline characteristics, except for age at injury. Patients who participated were significantly older at the time of injury than those who were lost to follow-up (respectively 36.2 ± 14.2 vs. 30.7 ± 11.7, p = 0.029).
Estimated changes over 10 years of follow-up in the total cohort
Depression scores (Wimbledon Self-Report Scale [WSRS]) and cognitive functioning scores (FAM) up to 3 years post-TBI have been reported elsewhere; cognitive functioning significantly improved during the 1st year post-injury and stabilized thereafter, whereas depression scores started to improve after 18 months, up to 3 years post-TBI. 39 The proportion of patients with depression also improved from 19% at 3 months post-TBI to 14% after 3 years of follow-up. Between 3 and 10 years after TBI, the proportion of depressed patients increased from 14% to 20%, which was not significant (p < 0.291).
HRQoL scores up to 3 years post-TBI have also been reported before; the domain scores increased up to 2 years and stabilized between 2 and 3 years post-TBI. 40 Between 3 and 10 years after TBI, none of the domain scores changed significantly (Fig. 1). The PCS and MCS did not change significantly either; PCS decreased from 46 (SE 1.3) at 3 year follow-up to 45 (SE 1.5) at 10 year follow-up (p < 0.700), whereas MCS increased from 49 (SE 1.2) at 3 years to 51 (SE 1.5) at 10 year follow-up (p < 0.221).
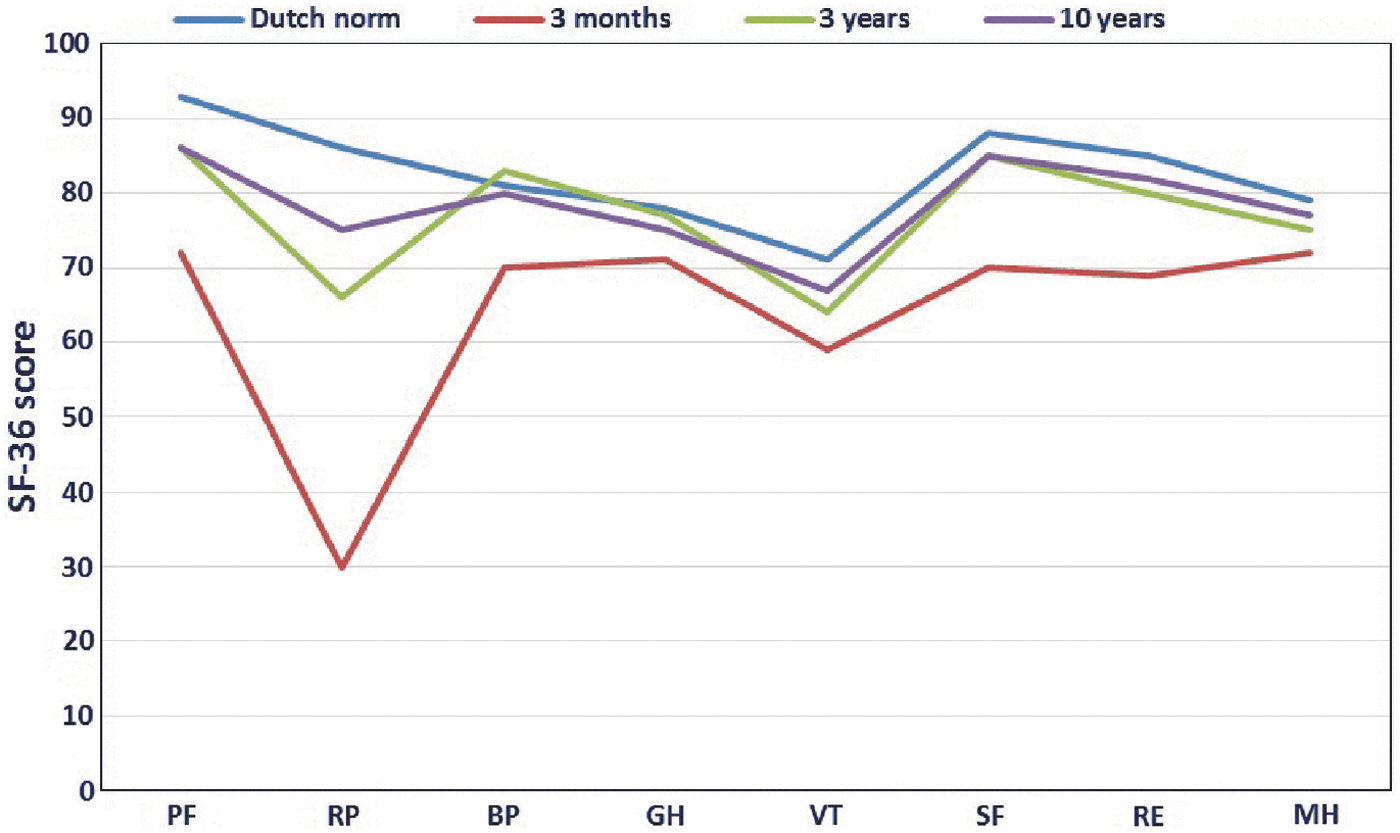
Change over time in health-related quality of life (HRQoL) for each domain of the Medical Outcomes Study 36-Item Short Form Health Survey (SF-36), from 3 months (red line), to 3 years (green line), up to 10 years post-TBI (purple line), in comparison with Dutch norms (blue line). 34 (PF, physical functioning; RP, role physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role emotional; MH, mental health.)
Depression and HRQOL 10 Years Post-TBI
Ten of 50 patients (20%) showed symptoms of depression (CES-D ≥ 16). We found that patients with depressive symptoms 10 years post-TBI differed significantly from those without symptoms regarding hospital discharge destination (p = 0.015) and psychiatric symptoms at hospital discharge (p = 0.048, Table 1). Patients with depressive symptoms were more frequently admitted to clinical rehabilitation or nursing homes or had psychiatric symptoms at hospital discharge, whereas patients without depressive symptoms were more often discharged home after the initial hospitalization. Differences between the groups in age, sex, living with partner or family, educational level (% high school), pre-injury employment, length of hospital stay, discharge FIM, FAM, BI, and GOS did not reach statistical significance (Table 1).
TBI, traumatic brain injury; CES-D, Center for Epidemiologic Studies-Depression Scale; GCS, Glasgow Coma Scale; FIM, Functional Independence Measure; FAM, Functional Assessment Measure; BI, Barthel Index; GOS, Glasgow Outcome Scale.
When the two groups were compared concerning HRQoL, measured with the SF-36, significantly worse scores were found in the subgroup of patients with depressive symptoms with regard to the following subdomains: Role Physical (p ≤ 0.001), General Health (p = 0.005), Vitality (p ≤ 0.001), Social Functioning (p ≤ 0.001), Role Emotional (p = 0.021), and Mental Health (p ≤ 0.001). Differences in physical functioning (p = 0.072) and bodily pain (p = 0.059) did not reach statistical significance, but the PCS (p = 0.001) and MCS (p = 0.008) did (Table 2). The group that showed no signs of depression had equivalent scores to those of the Dutch norm-population on all the subdomains of the SF-36 (Fig. 2).
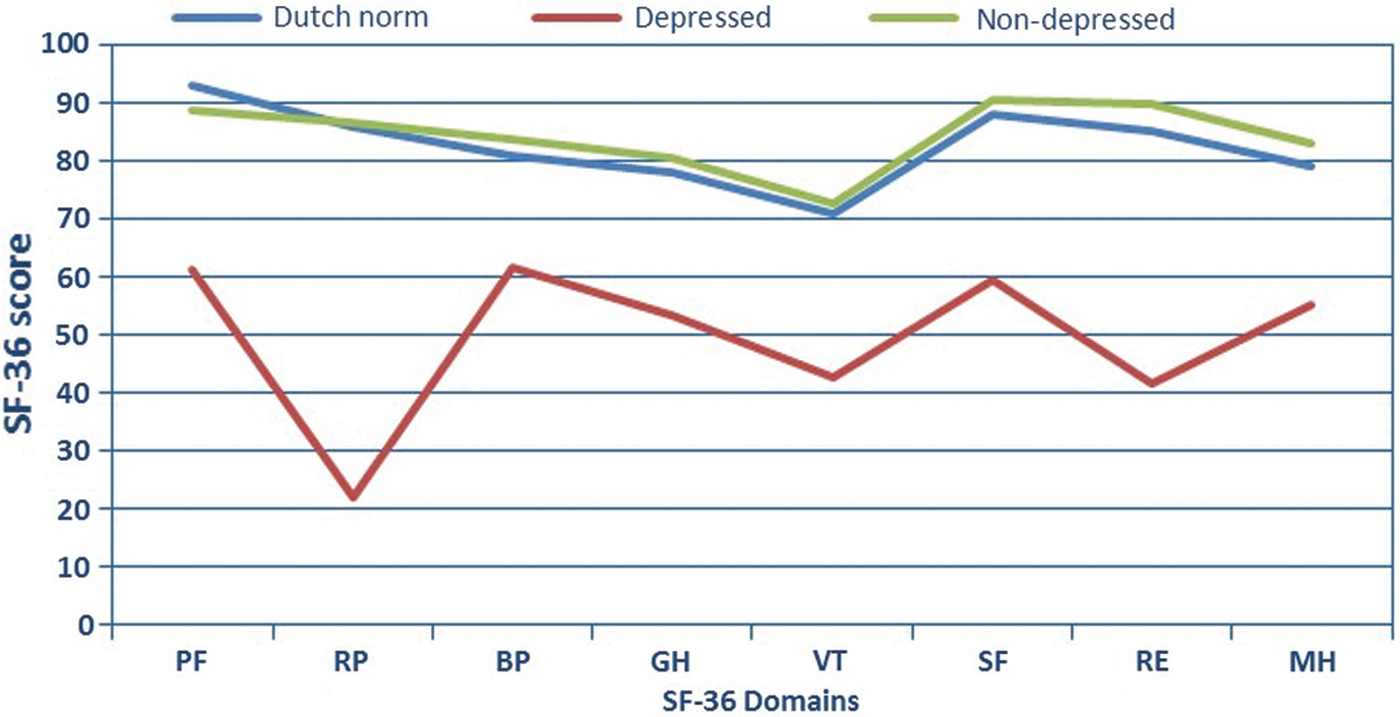
Health-related quality of life (HRQoL) domain scores for patients with (red line) and without (green line) symptoms of depression, 10 years post-TBI, in comparison with the Dutch norms (blue line). 34 (PF, physical functioning; RP, role physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role emotional; MH, mental health.)
HRQoL, health-related quality of life; CES-D, Center for Epidemiologic Studies-Depression Scale; PCS, Physical Component Summary Score; MCS, Mental Component Summary Score.
p value < 0.05.
Depression and cognitive function 10 years post-TBI
Patients with depressive symptoms reported more subjective cognitive complaints (measured with the CFQ) than patients without depressive symptoms (p = 0.013). Level of cognitive functioning was assessed through a series of objectively measured neuropsychological tests, including tests of attention and concentration, speed of information processing, memory, and executive functioning (Table 3). No significant differences were found between the subgroups with and without depressive symptoms on any of the cognitive tests, except for some measures of the d2 test. Patients with depressive symptoms had a lower number of items completed (p = 0.047). Further, a larger proportion of the group with depressive symptoms had T scores <40 compared with the group without symptoms, both on the d2 Concentration (p = 0.045) and the d2 Total Performance tests (p = 0.007). Focusing on the total group of patients, we found that 12% of patients were not able to perform the total cognitive test battery; especially, executive functioning (6ET) could not be assessed. Further, we found that the proportion of lowered test scores ranged from 4% to 6% for the DS, from 17% to 19% for the TMT, from 21% to 32% for the 15WT, and from 31% to 40% for the d2 test. In the general population, ∼15.9% has scores of 1 SD below the mean. Therefore, patients with TBI scored relatively low on memory tests (15WT), information processing speed (d2), and concentration (d2), compared with reference values.
CES-D, Center for Epidemiologic Studies-Depression Scale; CFQ, Cognitive Failure Questionnaire; DS-F, Digit Span Forward, d2-CP, d2 Concentration Performance; d2-TP, d2 Total Performance; TMT, Trail Making Test, 15WT-TR, 15 Word Task Total Recall, 15WT-DR, 15 Word Task Delayed Recall, DS-B, Digit Span Backward, 6ET, Six Elements Test.
p value < 0.05.
Associations among depression score, HRQoL, and cognitive functioning scores
Depression scores, were significantly (p < 0.001) associated with HRQoL, and subjective cognitive functioning scores at 10 years post-TBI (Table 4). Cognitive functioning at hospital discharge (FAM) was significantly associated with multiple objective cognitive test outcomes (p < 0.001) and with subjective cognitive functioning (p < 0.05) at 10 year follow-up, but not with depression or HRQoL. Both depression scores and mental health scores were weakly associated with parts of the objective tests of cognitive functioning (p < 0.05). Subjective cognitive functioning scores were not associated with any of the objective cognitive test results.
Correlation is significant at the 0.01 level (two tailed).
Correlation is significant at the 0.05 level (two tailed).
HRQoL, health-related quality of life; CES-D, Center for Epidemiologic Studies-Depression Scale; PCS, Physical Component Summary Score; MCS, Mental Component Summary Score; FAM, Functional Assessment Measure; CFQ, Cognitive Failure Questionnaire; DS-F, Digit Span Forward; DS-B, Digit Span Backward; 15WT-TR, 15 Word Task Total Recall; 15WT-DR, 15 Word Task Delayed Recall; d2-CP, d2 Concentration Performance; d2-TP, d2 Total Performance; TMT, Trail Making Test; 6ET, Six Elements Test.
Discussion
In this prospective 10 year-follow-up study in patients with moderate-severe TBI, we investigated the associations among depression, HRQoL, and cognition. In general, we found a prevalence of depressive symptoms of 20% in our study population, which is comparable with the prevalence of 17% reported by Scholten and coworkers, but is not in line with the study by Zgaljardic and coworkers, who reported a prevalence of 30–38%. 14,15 Remarkably, we found no reduction in HRQoL, but we found some underperformance on the cognitive test battery in the total group of patients, 10 years after moderate-severe TBI. Approximately 12% of patients were not able to perform the 6ET test of executive functioning, and up to 40% had low scores (> 1 SD) on one or more tests of memory, concentration, or information processing speed.
Focusing on patients with depressive symptoms, we found significantly worse scores on six of the eight HRQoL subdomains of the SF-36 than for those without symptoms. Patients with symptoms of depression also reported more subjective cognitive failures, which could not be confirmed by the scores on the neuropsychological tests, as patients did not perform worse on these tests, except for the d2 test, which measures concentration and speed of information processing. These findings are not in line with the hypothesis that depression would be related, not only to HRQoL, but also to problems of cognitive functioning. As the group of patients with depressive symptoms was small, we may not have had enough power to detect more subtle, but important differences. Therefore, we also looked for associations among depression score, HRQoL, and cognition scores on a continuous scale in the total group of patients. We only found weak correlations between the depression score and some of the cognitive test results 10 years post-TBI, whereas interrelations among depression score, HRQoL, and subjective cognitive functioning were clearly present. Further, cognitive functioning at hospital discharge was significantly related with objective cognitive functioning 10 years later. More specifically, a low hospital discharge FAM score was related to low scores on memory tasks, information processing speed, and executive functioning in the long term. However, discharge cognitive functioning was not related to HRQoL, or to depression in the long term. Moreover, subjective cognitive functioning was not related to objective cognitive functioning. Disease awareness may explain these contradictions in moderate-severe TBI; patients with reduced disease awareness may report good HRQoL. These patients may not have cognitive complaints or symptoms of depression, whereas cognitive outcome may be (severely) compromised. 41
The relationship between depression and HRQoL seems obvious; however, this study makes clear that this relationship is still present in the long term post-TBI. The longitudinal course of HRQoL has been described before, but not in relation to depression and cognition in the long term post-TBI. 40,42,43
Studies that objectively investigated cognitive function after moderate-severe TBI by means of standardized neuropsychological tests are often limited to a shorter follow-up period and show various results. For example, Spitz and coworkers studied 111 individuals with moderate-severe TBI, and objectively assessed the patients with a neuropsychological test battery at 3, 6, and 12 months post-injury and compared them with healthy subjects. 44 The participants scored significantly worse on all cognitive measures at 3 and 6 months. 44 At 12 months, six out of eight test scores still were significantly worse than those for healthy subjects; however, all cognitive measures showed gradual improvement over time. 44 Previously, we also found gradual improvement over time in the FAM score, which stabilized 1 year post-TBI. 39 In the study by Stenberg and coworkers, the clinical course of cognitive functioning, measured with the Barrow Neurological Institute Screen for Higher Cerebral Functions (BNIS), and depression, measured with the Hospital Anxiety and Depression Scale (HADS), was assessed in 78 patients with severe TBI for up to 1 year. 6 These authors also concluded that cognition improved over time, and appeared to be rather stable from 3 months to 1 year post-injury. 6 Significant correlations were found between cognitive functioning and HADS depression scores at 3 months and 1 year post-TBI. 6 In another study on neuropsychological functioning after severe TBI (n = 105) by Sigurdardottir and colleagues, the authors concluded that nearly two thirds of patients showed cognitive impairments in at least one of three cognitive domains 1 year after injury. 45
In a retrospective study 10 years post-TBI, Ponsford and coworkers compared cognitive functioning and emotional state among 60 patients with mild-severe TBI. 13 Two groups were made based on the GOSE, one group with good and one group with poor outcome. The patients with poor outcome performed more poorly on cognitive measures, such as information processing speed, attention, memory, and executive function, and showed higher levels of anxiety on the HADS. 13 Another retrospective study performed by Hoofien and coworkers evaluated 76 patients with severe TBI by means of standardized scales and neuropsychological tests at an average of 14.1 years post-injury. 46 This study indicated primarily severe long-term psychiatric problems, such as depression, anxiety, and hostility. 46 In the cognitive domain, a lower range of intellectual ability and slower psychomotor ability and processing speed was reported. 46
The abovementioned studies describe cognitive impairments mainly for up to 1 year. The study with a longer follow-up period also described cognitive disorders in patients with poor GOSE scores. A strength of our study is that it provides some insight in the course of cognitive functioning in the period beyond 1 year post-onset. Our results suggest that cognitive problems at hospital discharge gradually improve and stabilize 1 year post-TBI and are related with cognitive outcome 10 years later, but not with depression or HRQoL. In our study, cognitive difficulties were objectively detected in a subgroup of patients, 10 years post-TBI, whereas HRQoL was equivalent to Dutch norms. Therefore, this study suggests that most of the moderate-severe patients with TBI function rather well in the long-term, but also that a subset of these patients experience depression, reduced quality of life, and subjective cognitive complaints. We found that almost all these patients already were referred to rehabilitation centers/nursing homes. It will be a challenge to predict which patients will need extra attention during rehabilitation to prevent these long-term problems. We found that patients with cognitive problems at hospital discharge are at risk for long-term problems, but other factors may also play a role. The current study is unique, to our knowledge, for studying this subject 10 years post-TBI in a prospective cohort study.
Limitations
The long-term follow-up and prospective study design are a strength of this study. Nevertheless, selection bias may be a limitation, because of the large drop-out after 10 years of follow-up. Of the 113 patients who agreed to participate, 17% were lost to follow-up after 3 years, and 56% were lost after 10 years. However, our drop-out rates are comparable to those of other long-term prospective cohort studies. 9,47,48
The CES-D is a self-report scale not specifically designed for use with TBI patients; it was originally intended for use in the general population. However, in the meta-analysis performed by Osborn and coworkers, eight studies on TBI, which used the CES-D, could be identified. 49 In this meta-analysis, a higher prevalence of depression post-TBI was found, when using the CES-D (prevalence = 0.48) compared with, for example, the HADS (0.32) or Beck Depression Inventory (BDI) (0.43), which might have had an effect on our results. 49 In our study, however, the proportion of patients with depression was rather small (20%).
The neuropsychological test battery consisted of tests that comprised several cognitive domains. However, because of time constraints, we chose only one test per domain, instead of two or more. This may have caused a less differentiated picture than a more comprehensive neuropsychological test battery would have.
Finally, we studied symptoms of depression, but we did not look into the use of antidepressants. 50 Failla and coworkers investigated the effect of depression and use of antidepressants on cognitive recovery after severe TBI. 51 No difference was found between patients with and those without post-traumatic depression. 51 The use of antidepressants was associated with cognitive impairment 1 year post-TBI, a factor we did not consider. Post-traumatic stress disorder might also be of influence on cognition and depressive symptoms; however, this effect was not investigated either. 50
Other factors we did not consider and that might have been of influence are degenerative disease and decreased life-span and their potential association with depression. 52 –54
Conclusion
The majority of patients had good HRQoL 10 years after moderate-severe TBI. Cognitive problems at hospital discharge were associated with cognitive deficits in the long term, but not with depression or HRQoL, which is possibly a result of reduced disease awareness. Depression score was significantly associated with HRQoL and subjective cognitive complaints, 10 years after moderate-severe TBI. Therefore, signaling and treatment of depressive symptoms during rehabilitation is of major importance for optimal functioning in the long term post-TBI. We did not find that these associations could be extended to objective cognitive functioning. However, selective dropping out may have been of influence, therefore the results should be interpreted with caution. More long-term research is needed to clarify the role of disease awareness in moderate-severe TBI.
Footnotes
Acknowledgments
This study was financially supported by the Netherlands Organisation for Health Research and Development (project no.: 1435.0020).
Author Disclosure Statement
No competing financial interests exist.