
Abstract
Until now, it is impossible to identify a fatal traumatic brain injury (TBI) before post-mortem radiological investigations or an autopsy take place. It would be preferable to have an additional diagnostic tool such as post-mortem biochemistry to get greater insight into the pathological pathways and survival times after sustaining TBI. Cerebrospinal fluid (CSF) and serum samples of 84 autopsy cases were collected from forensic autopsies with post-mortem intervals (PMI) of up to 148 h. The cases were categorized into a fatal TBI case group (n = 42) and non-TBI controls (n = 42). The values of glial fibrillary acidic protein (GFAP), brain-derived neurotrophic factor (BDNF), and neutrophil gelatinase-associated lipocalin (NGAL) were analyzed by means of quantitative chemiluminescent multiplex immunoassays. The main results indicate that the usage of liquid samples with good macroscopic quality is more relevant for meaningful biomarker analyses than the length of the PMI. All three proteins were shown to differentiate TBI fatalities from the controls in CSF. In serum, only GFAP could be shown to be able to identify TBI cases. This study is the first approach to measure the three proteins together in CSF and serum in autopsy cases. Determined threshold values may differentiate between fatal TBI and control cases. The presented results emphasize the possible use of post-mortem biochemistry as a supplemental tool in everyday forensic routine.
Introduction
A
Consequently, there have been aims to establish a way that can provide information about the circumstances of a traumatic death of an individual in a biochemical manner. However, no single marker has been detected that could completely meet these requirements to date, although several markers have shown promising results in the past. 2 –6 Resulting from clinical trials, there are further candidates that seem exceedingly promising and may be of great value for forensic research.
Glial fibrillary acidic protein (GFAP) is an intermediate filament protein of type III, whose main function is to provide stability in astrocytes in the central nervous system and is essential for the process of reactive astrogliosis and glial scar formation. Further, it is involved in the functioning of the blood–brain barrier. 7 It only becomes measurable in both CSF and serum when there is an underlying damage to the brain and, consequentially, the astrocytes, thus it can be regarded as a specific marker thereof, 8,9 although very small concentrations of certain GFAP isoforms could also be found in other human organs such as the spleen, bone marrow, or in Schwann cells. 10 Further, it has been proven that there is a correlation between GFAP levels after TBI and its severity. 11 Nevertheless, it is known that even mild TBIs, such as concussion, lead to elevated serum levels of GFAP, 12,13 whereas multiple traumas without impact to the head do not increase GFAP levels. 14
Brain-derived neurotrophic factor (BDNF) is a protein that belongs to the family of neurotrophins. BDNF is broadly expressed in the developing and adult mammalian brain. 15 Therefore, it contributes to the normal development of the brain, spinal cord, and peripheral nervous system as well as to cell morphology, changes in synaptic transmission, and formation of memories and is linked to mechanisms of neurogenesis. 16 BDNF is predominantly produced in neuronal cells 17 but also in other cells within the central nervous system. 18 When present in the peripheral blood system, BDNF is expressed by megakaryocytes 19 and other peripheral blood cells such as platelets, 20 because it is not transported from brain to the periphery under normal conditions. 17 There are several studies on how BDNF serum levels correlate with neurodegenerative diseases that present different results. 21,22 Nevertheless, what appears to be certain is that BDNF has beneficial effects in the brain after injury and stroke. 23,24
Neutrophil gelatinase-associated lipocalin (NGAL) is a protein that is most commonly expressed by blood cells, mainly neutrophils, in for example, kidneys and lungs of humans. In a clinical setting, NGAL is most commonly used as a marker for acute and chronic kidney damage. 25 The protein can also, in smaller amounts, be found in the brain, mainly in neurons, and peripheral nerves. 26 NGAL, as an iron-handling and acute phase protein, can transport hydrophobic ligands and it contributes to the immune system by modulating the oxidative stress reaction. Thereby, NGAL is upregulated by numerous stimuli such as multiple pro-inflammatory cytokines. 27 Serum NGAL levels increase in TBI cases reflecting the underlying trauma severity, however, the exact way and utility of NGAL expression after TBI remains poorly understood. 26
The aim of the present study was to investigate the potential of the three proteins GFAP, BDNF, and NGAL to serve as useful post-mortem cerebral biomarkers for determining traumatic cases of death, for example, TBI, and for estimation of survival times in forensic settings. These proteins were chosen because their usability for such questions was already shown in living subjects. However, until now, there has been no research data that evaluates the possible avail of measuring these proteins in cadaveric body fluids.
Methods
Sample collection
The study included paired samples of cerebrospinal fluid (CSF) and serum of 84 fatalities, upon which routine forensic autopsy was performed at the Institute of Legal Medicine of the University of Leipzig. A positive ethics committee vote was received (local code: 117-12-23012012).
Blood was collected from femoral veins using sterile syringes at the beginning of each autopsy. By analogy, CSF was obtained from the suboccipital subarachnoid space with a sterile syringe. Immediately afterward, both samples were centrifuged at 5000 rpm for 5 min at 4°C to receive blood-free CSF and serum samples, which were subsequently stored at −80°C carefully preventing any thawing afterward. For diminishing influences of post-mortem changes to the body and thus to the body fluids, we decided to decline samples of deceased showing any macroscopic signs of decay and putrefaction and determined a maximum post-mortem interval (PMI; here meaning the time between death of the individual and freeze-storage of the sample) of 150 h. The knowledge of existent neurodegenerative diseases or neoplasms of any kind also led to rejection of the particular case to avoid possible confounders.
Macroscopic findings during the autopsy were confirmed histologically afterward. The collected cases were sorted into four groups accordingly: traumatic brain injury (TBI, n = 42) defined as traumatic impact on the head that leads to any form of intracranial bleeding; isolated torso trauma in the broadest sense (ITT, n = 14) including both blunt and sharp force trauma to the whole body-foremost the neck and the front trunk-with exception of the head; diffuse cerebral hypoxia (DCH; n = 14) representing fatalities dying from suffocation, hanging, or strangulation and acute myocardial infarction (AMI; n = 14) that stands representative for sudden death cases due to an inner cause. Among the control cases, TBI was ruled out by the macroscopic findings of the head and brain as well as histological analysis subsequent to the forensic autopsy. None of the control cases indicated an existent TBI in their medical files or death certificates.
The TBI group was then, in conformity with other research on this topic, 4 –6 further divided into three subgroups concerning the survival time of the traumatic impact: acute death (survival time <2 h; n = 21), subacute death (survival time 2–72 h; n = 10), and delayed death (survival time >72 h; n = 11).
The survival time of the trauma cases (TBI as well as ITT group) was determined according to paramedic and police investigation records and pathological findings. For DCH and AMI cases, the survival time was defined as “none,” because they died almost immediately after the fatal circulatory collapse.
Additionally, we collected the initial documented Glasgow Coma Scale (GCS) score given by the emergency physicians and calculated the New Injury Severity Score (NISS) out of the autopsy results. 28 Further, we collected information about possible final cardiopulmonary resuscitation attempts to get further insight into the severity of traumatic impacts and the duration of the immediate phase of death with inherent hypoxia.
Laboratory procedures
Values of BDNF, GFAP, and NGAL were analyzed by means of quantitative chemiluminescent multiplex immunoassays (Randox Laboratories, Crumlin, United Kingdom) on an Evidence Investigator (Randox Laboratories) with complete blindness to all data for the research team during measurement.
Upper assay ranges were 7500 pg/mL (BDNF; sensitivity 0.59 pg/mL), 120 ng/mL (GFAP; sensitivity 0.18 ng/mL), and 2000 ng/mL (NGAL; sensitivity 17.8 ng/mL). The intra-assay precision for the assays ranges between 8.0 and 11.5% coefficient of variance (CV), whereas the inter-assay precision has been determined to range from 8.1 to 11.1% CV. Because the NGAL assay was not designed for usage with serum according to the manufacturer's details, we did not perform NGAL measurements in this body fluid. Firstly, all body fluid samples were measured undiluted. In cases where the assay ranges had been exceeded, we repeated the measurement of the samples with dilutions of 1:50.
The number of destroyed erythrocytes was estimated using a cobas c701 analyzer (Roche Diagnostics, Mannheim, Germany) by measuring absorbance at 600/570 nm of saline-diluted samples. Using specific corrective factors, the analyzer calculated the hemolysis indices of the samples as representation of hemolysis levels. The obtained values, thus, represent the concentration of free hemoglobin in the sample.
Statistical analysis
Statistical analysis was performed using the statistical software R (version 3.4.0, 2017; open source) and Microsoft Excel (2010; Bellevue, WA).
All correlations between marker levels, PMI, and the hemolysis indices as well as the individuals' demographic and clinical characteristics were computed using bivariate analyses (r). The groups were tested for statistically significant differences between all TBI cases and all controls as well as between all TBI cases and every single control group using Wilcoxon's rank-sum test (non-parametrical, two-sided). This test was also used to compare the different TBI survival time categories. Afterward, the Benjamini-Hochberg procedure 29 was conducted to avoid type I error accumulation. Adjusted p-values were considered statistically significant at p < 0.05.
Receiver operating characteristic (ROC) curve analysis was used to identify the sensitivity and specificity as well as potential threshold values by conservative estimations for the differentiation between TBI and controls using bootstrap replicates confidence intervals.
Results
Quality control
The hemolysis index of all samples was used as quality control and reflected the usability of the body fluid sample. The CSF samples showed clear quality in most cases (mean hemolysis index for CSF 6, range 0–288); yet discreet blood admixture could not always be prevented. Serum samples tended to have higher hemolysis indices (mean 82, range 10–400).
The correlation between hemolysis indices and the PMI (Fig. 1), between hemolysis indices and marker levels in CSF (Fig. 2A) as well as in serum (Fig. 2B) and between marker levels and PMI in both CSF (Fig. 3A) and serum (Fig. 3B) highlight that the usage of samples with good macroscopic quality is more relevant for meaningful biomarker analyses than the length of PMI, if adequate cooling can be guaranteed.

Scatter plot and corresponding regression lines depicting the association of hemolysis indices (H-Index) of cerebrospinal fluid (CSF; dots) and serum (arrowheads) with length of post-mortem interval (PMI, in hours). For CSF: r = 0.23, p < 0.05. For serum: r = 0.02, p = 0.89.

Scatter plots and corresponding regression lines depicting the association of marker levels (BDNF with dots, GFAP with arrowheads, NGAL with squares) and hemolysis indices (H-Index) in cerebrospinal fluid (CSF;
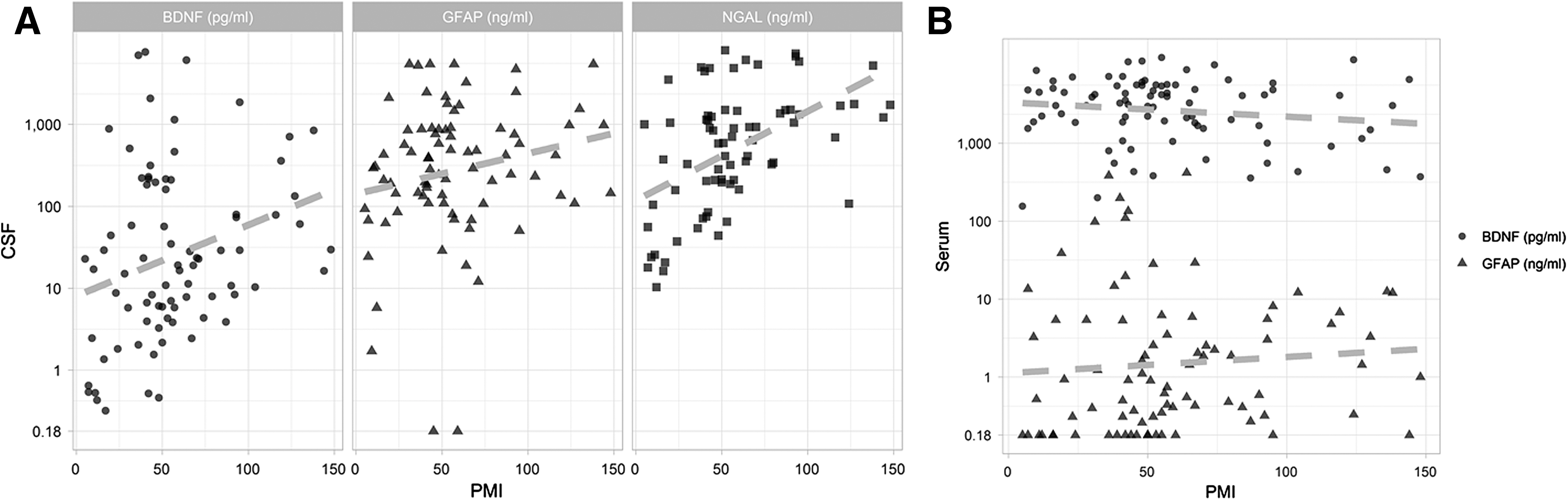
Scatter plots and corresponding regression lines depicting the association of marker levels (BDNF with dots, GFAP with arrowheads, NGAL with squares) and post-mortem interval (PMI, in hours) in cerebrospinal fluid (CSF;
Quite similar statistical relationships were achieved even when basic calculations assessing the correlations between marker levels and hemolysis indices or marker levels and PMI, were computed after subdividing the collected samples into TBI and control cases (Supplementary Table S1; see online supplementary material at
With the use of the NISS and the GCS score we intended to identify homogeneity of initial conditions among the four different case groups. As expected, both trauma groups showed comparable injury severity (median TBI 34, range 14–77 and median ITT 27, range 6–61), whereas both non-trauma groups could be registered without relevant detectable injuries (median DCH 4, range 0–21 and median AMI 1, range 0–6). However, the NISS did not show strong correlations to the marker values in both body fluids (Supplementary Table S2; see online supplementary material at
The CSF and serum values were neither affected by the gender or age of the deceased nor by the brain weight at time of the autopsy (Supplementary Table S2). Additionally, there were no passive increases in the brain weight detected after death with rising PMI (r = 0.07, p = 0.42).
Although CSF values of BDNF (r = 0.29, p = 0.08) and NGAL (r = 0.34, p = 0.05) correlated moderately to the presence of neurosurgery in TBI cases, CSF GFAP levels did not show such a relation (r = 0.05, p = 0.77). As expected, surgical attempts were used more often in TBI cases with longer survival (at least 6 h, r = 0.61, p < 0.05).
Different causes of death
Demographic characteristics and more detailed information about the causes of death of the studied control cases can be found in Table 1. Comparable data and summarized neuropathological details of the TBI cases with respect to the survival time categories are presented in Table 2.
CPR, cardiopulmonary resuscitation; f, female; GCS, initial Glasgow Coma Scale; h, hours; kg, kilograms; m, male; n.d., no documentation; NISS, New Injury Severity Score; PMI, post-mortem interval; y, years.
CC, cortical contusion; CPR, cardiopulmonary resuscitation; EDH, epidural hemorrhage; f, female; GCS, initial Glasgow Coma Scale; h, hours; ICH, intracerebral hemorrhage; kg, kilograms; m, male; min, minutes; n.d., no documentation; NISS, New Injury Severity Score; PMI, postmortem interval; SAH, subarachnoid hemorrhage; SDH, subdural hemorrhage; sec, seconds; TBI, traumatic brain injury; y, years.
The marker levels show opposite occurrences regarding the used body fluids. Whereas GFAP showed higher CSF than serum values in general, the CSF BDNF levels were lower than in the corresponding serum. Interestingly, GFAP concentrations showed a significant and strong positive correlation between both compartments (r = 0.47, p < 0.05), whereas BDNF failed to show such an inter-compartment relationship (r = 0.04, p = 0.71), see Figure 4. Unsurprisingly for the post-mortem setting, there were huge variations in marker values for all three proteins in both body fluids.
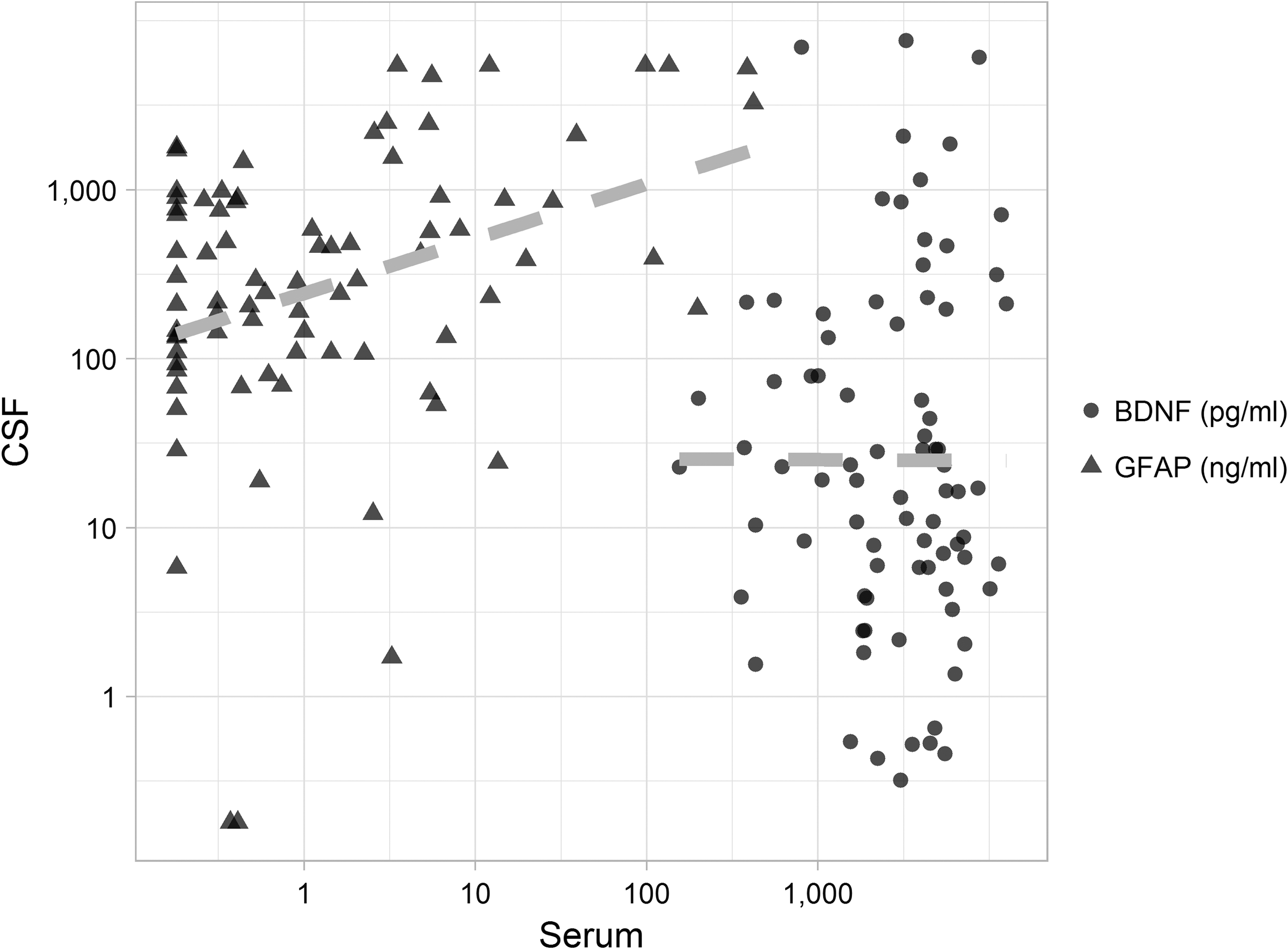
Scatter plot and corresponding regression lines depicting the correlation between marker levels in cerebrospinal fluid (CSF) and serum for BDNF (dots) and GFAP (arrowheads). For BDNF: r = 0.04, p = 0.71; for GFAP: r = 0.47, p < 0.05. BDNF, brain-derived neurotrophic factor; GFAP, glial fibrillary acidic protein.
In general, all three proteins were shown to differentiate TBI fatalities from non-TBI controls with different mechanisms of death in CSF (all p < 0.05). Consequently, the highest peak of all markers was listed in the TBI subgroups. Comparing all TBI cases with all controls in serum, only GFAP showed significant differences (p < 0.05).
Figure 5A,C and Figure 6A,C illustrate the measured GFAP and BDNF concentrations for all four groups in CSF and serum, as well as the subdivided survival time intervals after TBI. Figure 7A shows a comparable presentation for CSF NGAL values. A systematic overview of the obtained laboratory results is provided (all data as mean values and quartile deviation) in Table 3.
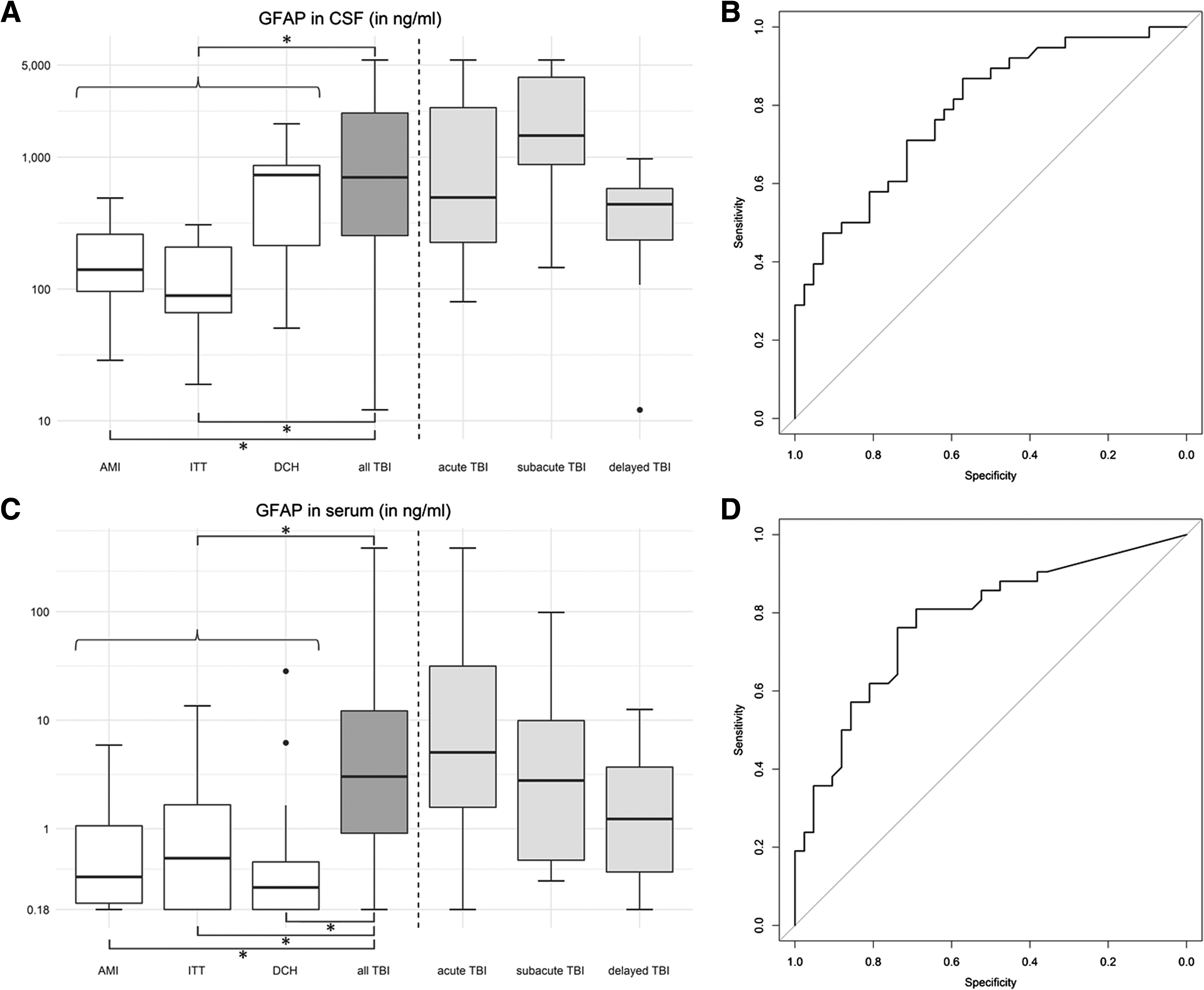
Post-mortem values of GFAP in CSF samples (n = 80;

Post-mortem values of BDNF in CSF samples (n = 80;
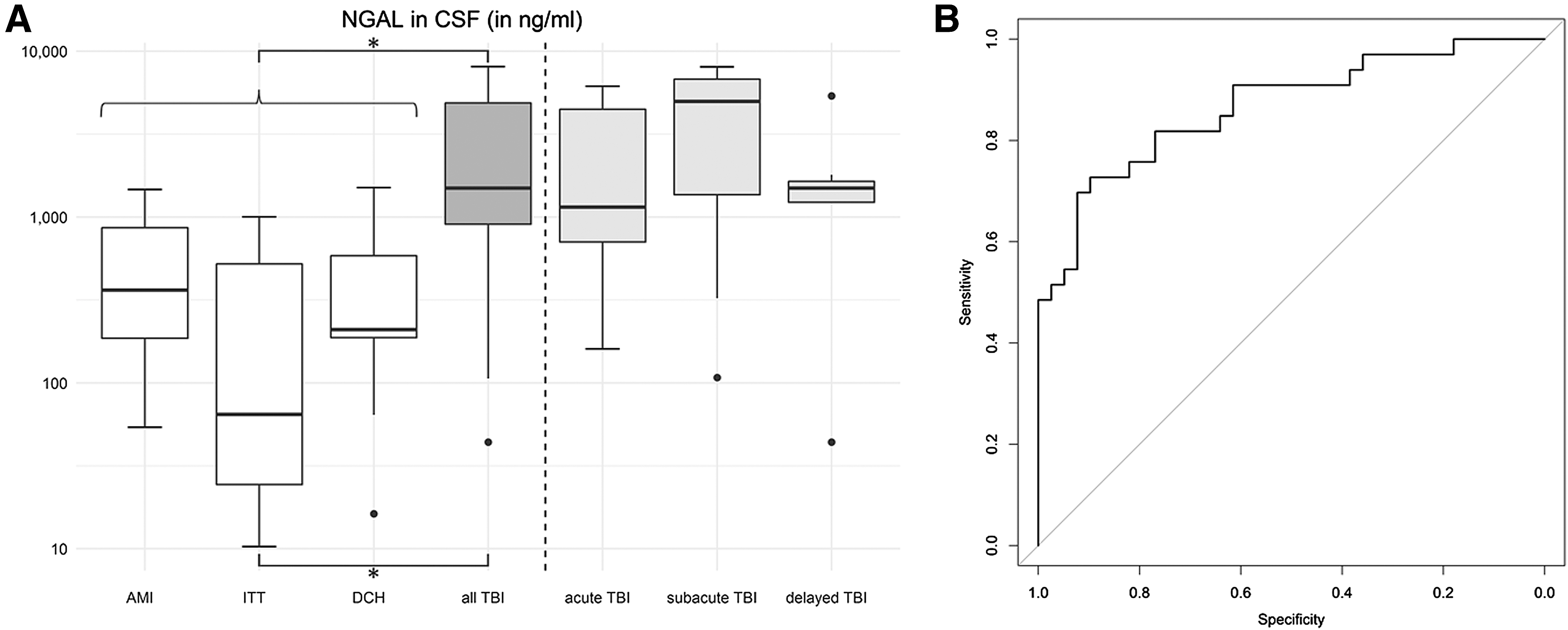
Post-mortem values of NGAL in CSF samples (n = 72;
The cases that suffered traumatic brain injury were subdivided according their survival time of the trauma (columns with gray background).
BDNF, brain-derived neurotrophic factor; CSF, cerebrospinal fluid; GFAP, glial fibrillary acidic protein; NGAL, neutrophil gelatinase-associated lipocalin; QD, quartile deviation; TBI, traumatic brain injury.
CSF and serum GFAP as well as CSF NGAL values did show significant differences between traumatic fatalities with or without head injury (see Fig. 5A,C and Fig. 7A). However, for CSF BDNF the comparison between TBI and ITT cases did not withstand the Benjamini-Hochberg procedure (adjusted p = 0.10).
Serum analyses of BDNF were not found to be suitable for cause of death differentiation (see Fig. 6C).
Diagnostic accuracy for TBI detection
Based on ROC curves, TBI cases could be differentiated from non-TBI fatalities via GFAP measurement using both body fluids (Fig. 5B,D). Using the diagnostic accuracy, a CSF GFAP level of >385.5 ng/mL (sensitivity 71.1%, specificity 71.4%) and a serum GFAP level of >0.91 ng/mL (sensitivity 76.2%, specificity 73.8%) substantiate the suspicion of an underlying TBI. The highest GFAP levels in control cases were exceeded in TBI cases, even when evincing very short survival times.
ROC curves for post-mortem BDNF measurement highlight its applicability for identifying TBI cases by measurement in CSF (Fig. 6B) but also its lack of diagnostic benefits in serum (Fig. 6D). A CSF BDNF level of 29.0 pg/mL (sensitivity 71.0%, specificity 83.3%) is documented as a conservative threshold value. This value was reached already by most of the acute deaths in the TBI group within survival times of <2 h and only in exceptional cases exceeded among the control group (false-positive results).
A comparable ROC curve was calculated for CSF NGAL levels (Fig. 7B). A threshold value could be determined at 1050.5 ng/mL (sensitivity 72.7%, specificity 89.7%) for a biochemical detection of a fatal TBI. The median CSF NGAL level observed in the TBI cases was not exceeded by any of the controls.
TBI survival time
CSF values of the three proteins tended to decline with rising survival times with the highest median levels in acute (for BDNF) and subacute (for GFAP and NGAL) phase after death. With rising survival times, the biomarker levels of the TBI cases approximated the levels of the controls.
However, no statistically significant differences of the marker levels were observed regarding the trauma survival time in neither CSF nor serum after application of the Benjamini-Hochberg procedure.
Discussion
The main objective of the present study was to identify significant biochemical changes of the three markers GFAP, BDNF, and NGAL in post-mortem CSF and serum samples following lethal TBI and determine the possible value of these findings in daily forensic practice, because these proteins have previously never been analyzed in combination in cadaveric human material. The main findings indicate that all tested markers are significantly elevated in CSF of TBI fatalities compared with all control cases and also compared with non-head-trauma cases. Further, we found that serum GFAP could also be suitable for detecting a lethal TBI.
Particularity of the post-mortem collection of the samples
A post-mortem setting generates a considerable heterogeneity of the collected sample material. Much remains unknown or not yet inspected in terms of decay and putrefaction following every individual's death. 30 Therefore, we decided to define a maximum PMI of 150 h to minimalize the possible post-mortem changes. Yet it still has to be assumed that early unspecific changes may occur already during agonal phases of death. 31
The hemolysis index as internal quality control showed that blood admixture strongly affects the protein levels in CSF. However, this cannot always be avoided, especially in cases with subarachnoid hemorrhage and thus represents the realistically achievable quality of post-mortem autopsy samples.
Protein levels depending on cause of death
Almost every sample of both serum and CSF showed at least slightly elevated levels of all three proteins, which might imply that cerebral damage due to oxygen deficiency is inevitable in the course of death itself regardless of its definite cause. 32 –34 It could also be shown that none of the three markers in neither body fluid can serve to estimate the survival time among the trauma cases with a forensically necessary precision.
However, the extent of all tested marker concentrations in CSF differs significantly when comparing TBI related fatalities to other casualties. Yet there are some particularities to every biochemical marker that need to be considered.
For GFAP, there are the following main observations to be made. Firstly, that in CSF, it is significantly higher in TBI cases than in the controls, except for the DCH cases. It is known that in living patients, serum GFAP is elevated following TBI and stroke as well (as an event that, by analogy to hanging or strangulation that constitute the DCH cases, causes relevant cerebral hypoxia), yet tending to higher concentration levels in the TBI cases. 35 Presumably, CSF levels act alike based on the knowledge of the glymphatic pathways that pass GFAP to the bloodstream. 36 Our results show a similar trend. Additionally, the results confirm the clinical observation that among ITT cases, GFAP levels increase in neither of the tested body fluids. 14 The presented threshold values originate from our studied collective and ought to be tested for their reliability in the future.
The results of BDNF CSF levels indicate a rather fast cerebral cell damage after TBI with the highest values in the acute phase after injury. Afterward, the levels decreased with rising survival times. In serum, there were no significant differences of BDNF concentrations between the groups to be observed, which can be explained when regarding the known fact that there is no transport of the protein to the peripheral blood system. 17
The results for NGAL CSF levels could make the protein a possible CSF biomarker to exclude an impact on the head in uncertain cases of death. Yet, the distinction of TBI and DCH cases is only minor. Thus, as a biomarker for delineation of internal from external damage on head and brain, NGAL should be considered from a critical perspective. Consequentially, although until now there is no scientific evidence on the exact pathomechanism, 26 it can be assumed that NGAL is expressed following TBI as well as following hanging or other forms of cerebral hypoxia according to a similar acute phase reaction, as it was reported before for other acute phase proteins. 33,37
Comparison with existent data from living patients
There are differences between the expectable marker levels in CSF and serum in living patients compared with those among deceased. In our research, the detected post-mortem levels tended to be above the clinical known measurement ranges as well as above former reported data of living patients that were achieved using the same laboratory methods. 38 –41 This fact has been reported before for most of the post-mortem trials in traumatic biochemistry. 4 –6 However, the relations between paired CSF and serum values were equal to those of living cohorts: there tend to be higher CSF levels of GFAP than in serum and vice versa for BDNF. 42,43 The fast release of the markers into CSF is most likely associated with the proximity to the brain tissue itself. 44
Limitations
Brain biomarker research is in desperate need of investigation and definition of brain-specific parameters to exclude relevant confounders for statistical interpretation of the data 45 and needs sufficient samples sizes for generalizable results. 46 Although GFAP is known to be rather sensitive for cerebral damage because it is expressed almost exclusively in astrocytes, it has been shown to be not trauma-specific. 37 Both BDNF and NGAL are expressed in several other tissues as well. 19,26 To the best of the authors' knowledge, the impact of kidney damage on NGAL CSF levels has not been assessed so far. Thus, the confounding relevance of such conditions remains unclear and, solely regarding our studied cohort, cannot be safely ruled out.
Yet, one can argue that an elevation of all three markers in CSF in one casualty could indicate a cerebral origin of the protein expression, as this is the only common source of all three. 47
Moreover, the unpreventable tissue changes with increasing PMI limit the possible use of forensic biochemistry to the early post-mortem stage in general. 31 The authors are aware of the fact that GFAP especially tends to undergo degradation processes with longer storage conditions as shown by Goede and colleagues. 48 The used chemiluminescent immunoassay is established for identifying the whole protein with 51 kDa and not for detecting GFAP- breakdown products. 10,49
This is the reason why we could not exclude possible influences of proteolytic processes with longer PMI in tissue, serum, and CSF; several single serum levels were beneath the detection limit of the laboratory kits used. It is of utmost importance to collect the body fluid samples as soon as possible, perhaps even during external post-mortem examination via external puncture, to reduce the unpredictable influence of the PMI to a minimum. 32 Unfortunately, such procedures are not stated in legislation in many countries. Until today, nothing is known about the passive post-mortem behavior of the three researched biomarkers in one and the same person in respect to the PMI. This important question remains to be answered in the near future by further research and therefore constitutes one of our working groups' currently researched subjects.
On top of that, one must consider neurodegenerative diseases as a possible confounder of the biochemical marker concentrations 50 because we defined it as an exclusion criterion. Thus, a possible impact of this cannot be safely denied.
Possible consequences for medicolegal practice
In every autopsy, samples of both blood and CSF are taken routinely and with minimal effort. Moreover, there are tendencies of innovation that develop toward virtual autopsies without opening the deceased bodies, solely using radiological and biochemical means. 51 Both facts emphasize the possible use of the presented results in everyday medicolegal routine.
The presented data indicate that the three markers in CSF could be suitable for biochemically detecting cases of death with an underlying TBI when reaching or exceeding determined threshold values. On top of that, serum GFAP also seems to be suitable for identification of TBI cases among all investigated casualties regardless of their definite cause of death using biochemical methods.
To provide the maximum specificity and sensitivity, measurement of a combination of more than one promising post-mortem biochemical marker of cerebral damage is advised and can be regarded as useful supplemental tool in forensic routine.
Footnotes
Acknowledgments
The authors would like to thank Ms. Aqeeda Singh (Dunedin, University of Otago, New Zealand) for correcting the English language of the manuscript as a native speaker.
Author Disclosure Statement
This work was partly supported by the German Ministry of Defense. BO has received reimbursement of travel costs from Randox Laboratories. The authors declare that no conflict of interest exists. The investigations were conducted in accordance with the human and ethical principles of the University of Leipzig (No. 117-12-23012012).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.