
Abstract
Post-traumatic stress disorder (PTSD) is commonly observed in military service members with mild traumatic brain injury (mTBI); however, the relationship between mTBI and PTSD is complex and not well understood. The present study aims to elucidate a link between the degree of alteration in limbic system-related white matter tracts and PTSD symptoms in an mTBI population. Diffusion-tensor imaging (DTI) with probabilistic tractography of the fronto-limbic pathways revealed decreased white matter integrity in the uncinate fasciculus in those with co-morbid mTBI and PTSD (n = 34), relative to those with only mTBI (n = 35). Additionally, fractional anisotropy (FA) and radial diffusivity (RD) measures in the bilateral uncinate fasciculus correlated with Post-Traumatic Stress Disorder Checklist Civilian version (PCL-C) scores, and primarily within the avoidance and re-experiencing domains. Findings from this study suggest the degree of traumatic injury within the limbic system could be directly related to post-traumatic stress and post-concussive symptoms, with disrupted white matter leading to significant PTSD outcomes.
Introduction
To date, almost 300,000 U.S. military service members worldwide have suffered a mild traumatic brain injury (mTBI). 1 Of these, it is estimated that 10–40% (depending on the military sub-population) were subsequently diagnosed with post-traumatic stress disorder (PTSD). 2 –4 In spite of the high rate of mTBI-PTSD co-morbidity, the neuropathological link between the two is not well understood, and there often exist confounding factors to the relationship. Using magnetic resonance imaging (MRI), researchers and clinicians have investigated the role of the limbic system, a prominent player in emotion regulation, in the development of PTSD. 5 One imaging modality in particular, diffusion-weighted imaging (DWI), has been used to characterize white matter tracts that interconnect brain regions within functional networks such as the limbic system. By investigating the integrity and morphology of these fiber bundles, structural connectivity can be assessed within key functional brain networks, including those critical to the neurocircuitry involved in emotional expression and regulation.
Current literature provides mixed findings regarding the link between mTBI and PTSD Hoge and colleagues 3 and Lew and co-workers 6 report a significant (43.9% and 42%, respectively) incidence of PTSD and other distress symptoms following mTBI. Notably, the incidence of PTSD in service members with mTBI is considerably higher than in the non-injured population (only 9.1% in Hoge and colleagues' study); other studies similarly report an increased likelihood of developing PTSD following mTBI. 7,8 However, in elucidating the direct relationship between mTBI and PTSD, there are a number of confounds to consider. Symptoms of mTBI and PTSD often overlap, 9 and pre-existing psychological state, predisposition to development of PTSD, and the extent of traumatic experiences on the battlefield are all potential contributing factors to the development of PTSD after injury. 10,11 Further, these same pre-existing conditions can influence the reporting of TBI outcomes. 12 Documentation of post-concussive symptoms is wide-ranging for those with mTBI, 13 with the most common complaints including anxiety, depression, and headache. 3,6 In addition, many service members with mTBI and sequelae report life-altering effects 5 and even 10 years post-injury. 14 –16
mTBI is characterized by normal MRI findings in clinical scans, 17,18 with some suggesting that the primary injury mechanism is diffuse axonal injury due to shearing and angular and rotational forces on the whole brain. 13,19,20 Relatedly, numerous studies have shown white matter abnormalities in those with mTBI, with a few linking these changes to PTSD, or other behavioral outcomes in the military population. Davenport and associates 21 and Lopez and colleagues 22 report decreased white matter integrity and regional brain volumes, respectively, in individuals with mTBI-PTSD co-morbidity as compared with those with only mTBI. Another study by Yeh and co-workers 23 found PTSD and associated symptoms correlated with reduced white matter integrity in service members with mTBI. In contrast, Sorg and colleagues 24 found changes in white matter integrity to be related to mild and moderate TBI independent of PTSD status.
PTSD can symptomatically be sub-divided into: (1) re-experiencing, (2) avoidance, and (3) hyperarousal, all of which are forms of emotional dysregulation. 25 Essential to emotion regulation is the ventro-limbic system of the brain, a network connecting the amygdala to frontal and prefrontal cortices with back-projection to the hypothalamus. 13 Some of these regions appear to be more disposed to alterations following mTBI. Notably, Niogi and associates 26 found 30% of mTBI patients had reduced integrity in the uncinate fasciculus and 41% in the anterior corona radiata. Given the suggested vulnerability to injury, it is possible that disruption of the limbic system leads to the development of PTSD in TBI patients. To this end, the present study investigated the relationship between white matter integrity and PTSD in male service members and veterans diagnosed with mTBI enrolled in the Brain Injury and Mechanisms of Action of Hyperbaric Oxygen for Persistent Post-concussive Symptoms after mild TBI (BIMA) study. We hypothesized that traumatic (mTBI) injury to the ventro-limbic pathways is associated with severity of PTSD symptoms, such that those with co-morbid PTSD and mTBI have decreased tract integrity compared with those with only mTBI. Further, we anticipated an association between measures of tract integrity and self-reported PTSD symptoms.
Methods
Participants
Participants in the BIMA study, a prospective study of mTBI, 27 were male U.S. service members and veterans. The current study analysis only examines the baseline time-point. Inclusion criteria for the BIMA study involved history of mTBI, at least 3 months of persistent post-concussive symptoms, and being no more than 5 years post-injury. 27 Head injury eligibility was determined by the Ohio State University TBI Identification Method, 28,29 a structured interview administered by site coordinators used to obtain the number and nature of self-reported lifetime TBIs as well as the frequency and severity of post-concussive symptoms. Although PTSD was not a criterion for enrollment, all participants were clinically assessed for PTSD using the Structured Clinical Interview for DSM-IV (SCID) diagnostic algorithm, 30 and 49% met criteria for PTSD. Self-reported PTSD symptoms were assessed using the Post-Traumatic Stress Disorder Checklist Civilian version 31 (PCL-C), a 17-item symptom scale (total score range 17–85) with higher scores reflective of more severe symptoms. Re-experiencing, avoidance/numbing, and hyperarousal domain scores as well as a total score were calculated from the scale. A number of other self-reported symptom assessments were administered as part of the larger BIMA study, as well as a full neuropsychological battery collected for all participants.
Image acquisition
Scanning was performed using a 3T Philips Achieva MRI scanner (Philips Healthcare, Best, The Netherlands). T1-weighted images were collected using a three-dimensional (3D) turbo field echo [TFE] gradient echo pulse sequence with the following parameters: repetition time [TR]/echo time [TE]1/deltaTE = 9.3 msec/1.65 msec/1.8 msec with a voxel size of 1 × 1 × 1 mm. Automated cortical reconstruction and volumetric segmentation of T1-weighted images were processed using the FreeSurfer software package. 32,33
DWIs were collected using a single-shot spin-echo echo-planar imaging [EPI] sequence with the following parameters: 32 directions of DWI (b = 1000 sec/mm 2 ), and one volume of non-DWI (b0), TR/TE of 10 sec/70 msec, voxel size of 2 × 2 × 2 mm. Pre-processing steps included distortion correction using B0 fieldmap, 34 motion correction, and diffusion tensor estimation using a linear fitting. 35
Image processing
Automated segmentation of major white matter tracts was carried out using TRACULA. 36 TRACULA is based on a Bayesian framework for global probabilistic tractography to perform automated segmentation of major white matter tracts by utilizing prior information on the anatomy of the white matter pathways from a set of training subjects, followed by constraining the priors using anatomical segmentation information on the individual subject level. The atlas used by TRACULA includes the following white matter regions: corticospinal tracts, inferior longitudinal fasciculi, uncinate fasciculi, forceps major/minor of the corpus callosum, anterior thalamic radiations, cingulate/angular cingulum bundles, and parietal/temporal superior longitudinal fasciculi (Fig. 1). Further detail on TRACULA methodology has been previously published. 36 Although all TRACULA atlas tracts were evaluated in the analysis, differences were primarily of interest in cingulate and angular cingulum bundles, anterior thalamic radiations, and the uncinate fasciculi, as these are known components of the limbic system network. 37 Regional tensor-based measures, including fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD), of each tract were then extracted for further analyses.

Three-dimensional (3D) rendering of tracts identified by TRACULA. Right uncinate fasciculus indicated by red arrow. Color image is available online.
Statistical analysis
All statistical analyses of regional diffusion measures of white matter tracts and other outcomes were performed in SPSS (IBM, SPSS Statistics v. 24). Age was used as a co-variate in all statistical analyses, as it was significantly different between PTSD and non-PTSD groups (Table 1) and it is known that white matter integrity changes with age. 38 For each diffusion-tensor imaging (DTI) measure on each individual tract, univariate general linear models were fitted with DTI measure as the outcome and PTSD diagnosis as a predictor with an adjustment for age in order to evaluate between-group differences in DTI measures for those with PTSD versus those without. Pearson partial correlation coefficients were computed to evaluate the association of DTI measure and self-reported PCL-C score for each DTI measure across individual tracts while controlling for age. This exploratory analysis was performed without correction for multiple comparisons and with an alpha of 0.05.
Demographics and Screening Scores for Patient Population (Mean and Standard Deviation)
Significantly different between groups (p < 0.05).
Significantly different between groups (p < 0.005).
Significantly different between groups (p < 0.0001).
Number of blast injuries is self-reported; PCL-C score range: 17–85; depression score: CESDS total score (range: 0–60); anxiety score: BAI total score (range: 0–63).
BAI, Beck Anxiety Inventory; CESDS, Center for Epidemiologic Studies Depression Scale; mTBI, mild traumatic brain injury; PCL-C, Post-Traumatic Stress Disorder Checklist Civilian version; PTSD, post-traumatic stress disorder.
Results
From September 2012 to May 2014, BIMA enrolled 71 participants. One participant was excluded from analyses due to poor image quality after pre-processing and one female participant was excluded due to known differences in DTI measures by gender. 39 Demographics and selected screening scores collected at baseline for all participants included in the current study analysis are shown in Table 1. There were a number of characteristics that differed between the mTBI and mTBI+PTSD populations in this study. Table 1 indicates significant differences in age, number of blast injuries, PCL-C score, depression score, 40 and anxiety score 41 between the groups.
Comparisons of white matter integrity measures for all atlas tracts are included in Supplementary Table 1 (see online supplementary material at
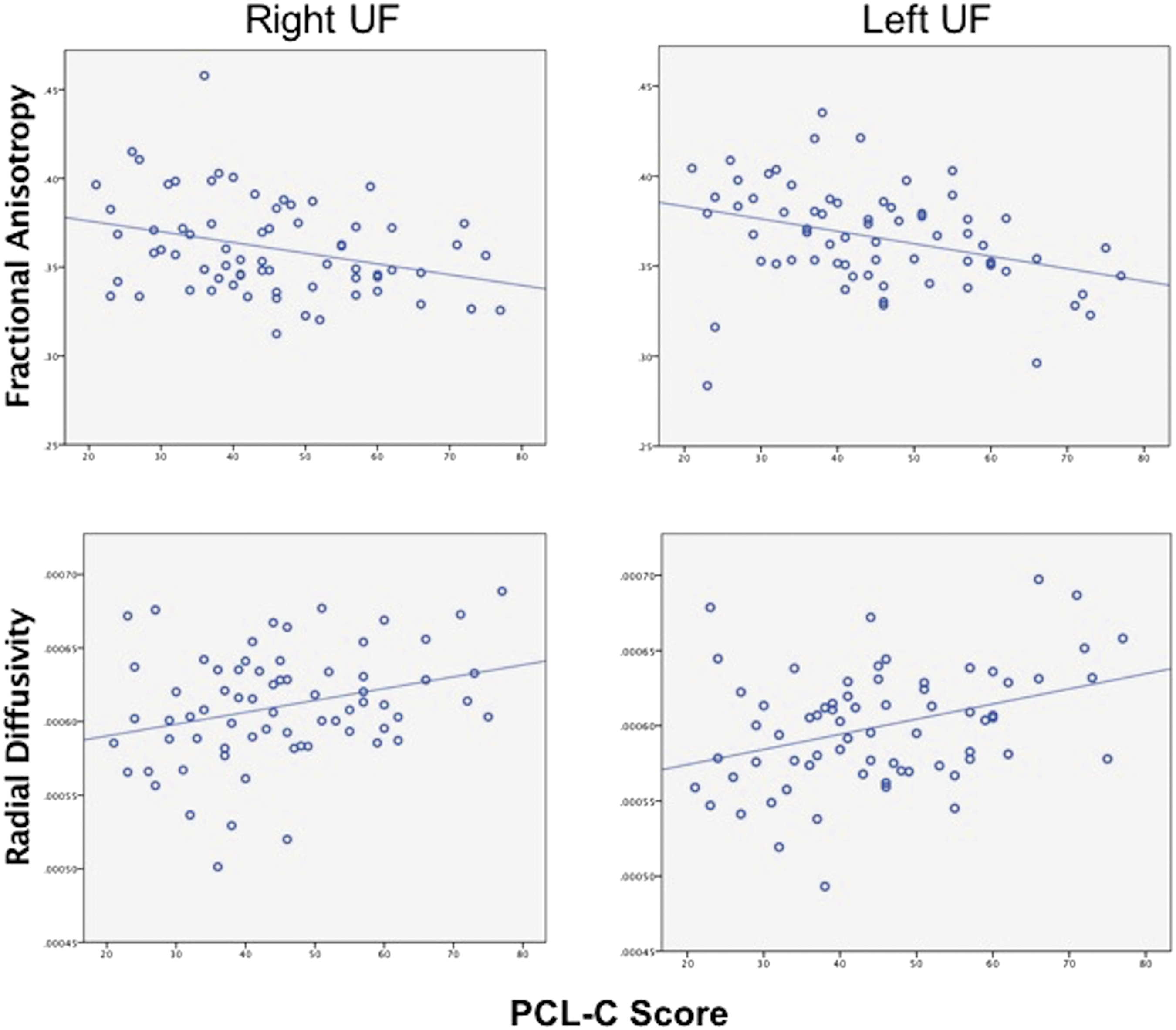
Scatterplots of diffusion-tensor imaging (DTI) measures and Post-Traumatic Stress Disorder Checklist Civilian version (PCL-C) total score for right and left uncinate fasciculi (UF). Adjusting for age, PCL-C score inversely correlated with fractional anisotropy (FA) across the right UF (r = −0.258, p = 0.0337) and left UF (r = −0.304, p = 0.0118), and positively correlated with radial diffusivity (RD) across the right UF (r = 0.276, p = 0.0228) and left UF (r = 0.348, p = 0.0037). Color image is available online.
Main Effects of PTSD on DTI Measures of the UF
p < 0.01, ** p < 0.05.
Mean and standard deviation are shown, with F-values and P-values derived from age-adjusted model. No significant PTSD by age interaction effects were found.
AD, axial diffusivity; DTI, diffusion-tensor imaging; FA, fractional anisotropy; MD, mean diffusivity; mTBI, mild traumatic brain injury; PTSD, post-traumatic stress disorder; RD, radial diffusivity; UF, uncinate fasciculi.
A breakdown of the PCL-C total score into sub-domains revealed the correlation with DTI measures was attributed to the avoidance and re-experiencing domains primarily. RD bilaterally and FA and MD for the left uncinate fasciculus correlated significantly with the avoidance sub-score (p < 0.005), whereas RD and FA bilaterally and MD for the left uncinate fasciculus significantly correlated with the re-experiencing sub-score (p < 0.05).
Discussion
This study examined neural correlates of PTSD within major white matter tracts in a military mTBI population. PTSD-related symptomology (i.e., anxiety and depression) was significantly higher in the mTBI+PTSD group as compared with mTBI only, and higher PCL-C total score was associated with lower white matter integrity in the uncinate fasciculus bilaterally. In addition, re-experiencing and avoidance sub-domains correlated with FA, MD, and RD values in the uncinate fasciculi. Lower FA and higher RD are both associated with disruption of white matter, specifically demyelination and axonal degeneration, 42 –45 which may result in reduced connectivity between regions of the ventro-limbic system. Several DTI studies have reported reduced FA and increased diffusivity with mild TBI, 24,26,46 –48 with Niogi 26 specifically reporting lower FA in the uncinate fasciculus following mTBI. It is possible that the uncinate fasciculi are more susceptible to traumatic injury in our PTSD population, or that its structural integrity is more closely associated with PTSD outcomes than other limbic tracts.
Screenings for depression and anxiety in our study reflected poorer mental health in the PTSD population. Consistent with our findings, co-morbid anxiety and depression are frequently noted by self-report or clinical diagnosis in other studies of mTBI and PTSD. 6,14 Post-concussive complaints can include (in addition to depression and anxiety) headache, sensitivity to light and sound, fatigue, cognitive/memory impairment, dizziness, and sleep disturbance. 11,49 However, these symptomologies can present with PTSD even in the absence of mTBI, and more study is needed to elucidate the relationships among these factors.
The main finding of poorer integrity of the uncinate fasciculi, and to a lesser extent the anterior thalamic radiations, in those with mTBI+PTSD is unsurprising given existing understanding of limbic system functioning and disruption in PTSD. 13,50,51 Williamson and colleagues 13 suggest an autonomic pathway model wherein dysfunction of the uncinate fasciculus specifically disrupts connectivity between the orbitofrontal cortex and amygdala, leading to altered feedback regulation of emotional reactivity. Further, the review suggests that arousal not naturally inhibited by a “relaxed state” is a hallmark of PTSD and considered maladaptive behavior. It is possible our mTBI+PTSD cohort is affected in this way, especially given the correspondence between degree of tract alterations and PTSD symptoms.
The uncinate fasciculus plays a known role in memory encoding and retrieval in healthy persons. 52 –54 Alterations to the uncinate fasciculus have been noted in clinical populations with emotion and memory problems, including schizophrenia, bipolar disorder, and Alzheimer's disease. 55 –57 In this study, the re-experiencing sub-domain of PTSD symptoms was particularly correlated with anisotropy and RD of the uncinate fasciculus. It is possible disrupted connectivity within the uncinate fasciculus may be responsible for abnormal emotional-memory preservation in this population in addition to post-traumatic symptoms. FA was additionally associated with avoidance, which could be the result of functional inhibition to the limbic pathway signals. 13 Closer examination of functional connectivity of the uncinate fasciculus in individuals with mTBI and PTSD would be needed to confirm such a dysfunction of the limbic network.
A few mTBI studies have related the number of injuries to severity of white matter effects. 58 –60 The group with PTSD outcomes was exposed to more blasts on average in our study, suggesting the possibility of multiple contributing factors to post-traumatic stress. That is, compounded brain injury could be contributing to PTSD either independently or in conjunction with emotional trauma from multi-blast exposure. Further study of emotional regulation mechanisms (i.e., autonomic nervous system pathways) would be needed to determine any cause-and-effect relationships. 13
This study has a number of limitations. First, because TRACULA only identifies certain larger white matter tracts, our study did not include every tract involved in the limbic system, nor did it address white matter changes around predominantly crossing fibers. Second, as the study only includes participants with mTBI, the findings do not inform differences that may be evident in the non-injured population. Finally, a lack of pre-injury data, both in terms of imaging and neuropsychological evaluation, limits our ability to identify whether PTSD outcomes are the direct result of brain injury or a predisposition to PTSD, or a combination of these factors.
Conclusion
To our knowledge, this is the first study to directly correlate PTSD symptoms with the degree of white matter alteration in a military mTBI population. A number of factors could be contributing to PTSD in our population, including localized injury mechanisms, degree of blast exposure, war-related experiences, and predisposition. However, given the role of the uncinate fasciculus in limbic system emotion regulation, it is possible that reduced structural integrity in the uncinate fasciculus leads to increased susceptibility to PTSD outcomes. Further, this regional alteration might specifically be involved in emotional memory preservation and recall (or a lack thereof), as characterized by dominance of re-experiencing and avoidance symptoms. These findings elucidate the link between mTBI and PTSD outcomes, suggesting disruption to the fronto-limbic network circuitry that corresponds to the degree of damage.
Footnotes
Acknowledgments
This work is supported by the U.S. Army Medical Research and Materiel Command under Contract No. W81XWH-15-D-0039-0003. The views, opinions, and/or findings contained in this report are those of the author(s) and should not be construed as an official Department of the Army position, policy, or decision unless so designated by other documentation. In the conduct of research where humans are the subjects, the investigator(s) adhered to the policies regarding the protection of human subjects as prescribed by the Code of Federal Regulations (CFR) Title 45, Volume 1, Part 46; Title 32, Chapter 1, Part 219; and Title 21, Chapter 1, Part 50 (Protection of Human Subjects).
The authors acknowledge the following team members for their contributions to the study design and execution: from the National Intrepid Center of Excellence: Gerard Riedy, Jenni Pacheco, Alex Kubli, Joseph Hennessey; from the BIMA analysis team: William Orrison, Jeffrey Lewine, Darlene Harbour, Tom Perkins, Kayla Deru, Susan Churchill, Anne Lindblad, and Jigar Patel.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.