
Abstract
Neurostimulant medications are commonly prescribed following traumatic brain injury (TBI) in adults; little is known about their use in children with TBI. Our objective was to analyze neurostimulant prescribing practices from 2005 to 2015 in children admitted to the intensive care unit (ICU) with TBI. We hypothesized that neurostimulant prescriptions have increased over time and are associated with older age and injury severity. A retrospective cohort study of patients age 1 month to 18 years with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis code for TBI admitted to the ICU between 2005 and 2015 in 37 pediatric hospitals included in the Pediatric Health Information System was conducted. Variables examined include patient and injury characteristics and neurostimulant medication use. Descriptive statistics and multi-variable logistic regression testing were used to determine variables associated with neurostimulant prescription. Of 30,881 patients with TBI, most were male (64%) and age 0–4 years (43%). In patients with mechanism of injury reported (n = 21,998), TBI was most frequently due to falls (36%) and motor vehicle collisions (36%). One thousand sixty-four neurostimulants were prescribed to 878 (3%) patients with 41% of prescriptions for amantadine and 38% for methylphenidate. Neurostimulants were prescribed a median (interquartile range) of 17 (8–35) days post-injury and increased over the study decade (R2 = 0.806). In a multi-variable analysis, variables most strongly associated with receipt of a neurostimulant were age 14–18 years (odds ratio 5.8, 95% confidence interval [4.3,7.8]), motor vehicle collision (3.1, [2.4,4.2]), intracranial pressure (ICP) monitor (3.8, [3.1,4.5]), and mechanical ventilation (3.4, [2.7,4.3]). Use of neurostimulants following pediatric TBI is uncommon, has increased over time, and is associated with indicators of higher severity of illness. Knowledge of prescribing practices may assist in optimizing the design of efficacy and outcome studies that will inform clinical guidelines.
Introduction
Traumatic brain injury (TBI) is a leading cause of pediatric morbidity and mortality. 1 Children with severe TBI (Glasgow Coma Scale [GCS] score <9) are estimated to have a 20% mortality rate and 50% morbidity rate. 2 Longer durations of intensive care and hospital admission until inpatient rehabilitation admission after TBI is associated with worse functional outcomes. 3,4 This period thus represents a crucial opportunity for clinicians to implement interventions that may facilitate recovery and timelier transfer of care.
Guidelines for the medical management of severe TBI in infants, children, and adolescents focus on acute stabilization following injury. 5 There are no guidelines and little data to support the optimal timing of rehabilitation interventions such as physical therapy, rehabilitation consultation, or neurostimulant trials for children with low arousal states while hospitalized post-injury. Neurostimulant medications such as amantadine are thought to enhance awakening and thus promote participation in rehabilitation and combat adverse functional outcomes resulting from TBI. 6,7 Studies in adults suggest amantadine may facilitate recovery in patients with disorders of consciousness following TBI. 8 The evidence in children is less robust, 9,10 however, with study design focused primarily on chronic behavioral and neuropsychological outcomes rather than the subacute recovery period. 11,12 Thus, physicians use clinical judgment with regard to whether and how to prescribe neurostimulant medications for their patients, likely leading to wide practice variation and effectiveness. 13
The objective of this study was to evaluate neurostimulant prescribing practices over the past decade and identify factors associated with prescribing after pediatric TBI to inform prospective study design. Our hypothesis was two-fold: neurostimulants would be (1) prescribed more frequently for older versus infant and toddler-age children, and (2) would be prescribed more often for children with more severe TBI.
Methods
A retrospective cohort study was performed of patients aged 1 month to 18 years with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) discharge diagnosis code for TBI who were admitted to a pediatric ICU between 2005 and 2015 in pediatric hospitals included in the Pediatric Health Information System (PHIS) database.
The PHIS database is an administrative database containing inpatient, emergency department, ambulatory surgery and observation encounter-level data from most not-for-profit, tertiary care pediatric hospitals throughout the United States. These hospitals are affiliated with the Children's Hospital Association based in Overland Park, KS. Data quality and reliability are assured through a joint effort between the Children's Hospital Association and participating hospitals. Portions of the data submission and data quality processes for the PHIS database are managed by Truven Health Analytics (Ann Arbor, MI). For the purposes of external benchmarking, participating hospitals provide discharge/encounter data including demographics, diagnoses, and procedures. Nearly all hospitals also submit resource utilization data (e.g., pharmaceuticals, imaging, and laboratory) into PHIS. Data are de-identified at the time of data submission, and data are subjected to a number of reliability and validity checks before being included in the database. On entry into the database, patients are given an unblinded hospital ID for identification and tracking of diagnoses or billing within the database. Individual hospital results were blinded for the study in accordance with PHIS policies.
We included patients admitted to the intensive care unit (ICU) of a hospital reporting data to the PHIS database who received an ICD-9-CM discharge diagnosis code for TBI between January 1, 2005 and October 1, 2015 (refer to Supplementary Tables S1–S5; see online supplementary material at
We included only the first patient admission with TBI as a diagnostic code; subsequent admissions by the same patient are not represented. We excluded patients who were not admitted to the ICU to target a more severely ill patient population. Other exclusion criteria included admission to a hospital that did not report pharmacy or clinical data for all or part of the study period, and age less than 1 month to avoid trauma associated with birth. Overall, 30,881 patients from 37 hospitals met the criteria for inclusion (Fig. 1).
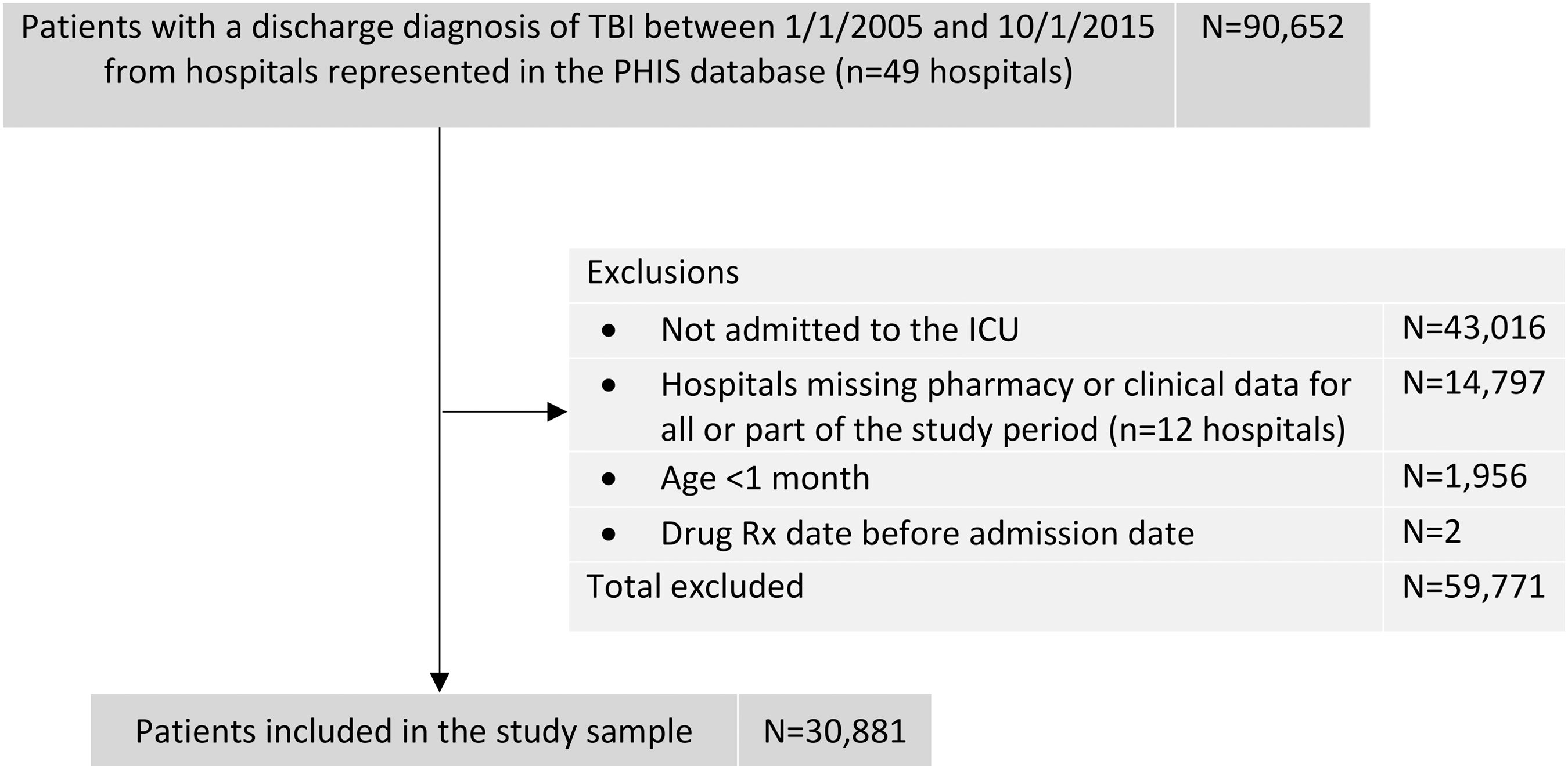
Selection criteria for patients <18 years of age requiring critical care after traumatic brain injury (TBI) between January 2005 and October 2015. ICU, intensive care unit; PHIS, Pediatric Health Information System.
Our primary outcome was an analysis of prescribing frequency over the study period. A secondary outcome was to identify factors predictive for receipt of a neurostimulant prescription. Variables examined included patient characteristics (age, gender, race/ethnicity, insurance status, 5-year discharge epoch: 2005–10, 2010–15), injury characteristics (mechanism of injury, traumatic shock), interventions (mechanical ventilation, intracranial pressure [ICP] monitoring, craniotomy/craniectomy), and outcomes (hospital length of stay; ICU days; physical, occupational, and speech/language therapy evaluations; mortality; discharge disposition). We recorded the days between injury and when a medication (amantadine, methylphenidate, dexmethylphenidate, bromocriptine, levodopa/carbidopa, modafinil, and donepezil) was ordered, the number of days for which a medication was ordered, and the presence of a co-morbid diagnosis of attention deficit hyperactivity disorder (ADHD). Mechanism of injury was determined using a subset of ICD-9-CM codes called external causes of injury codes (E-Codes) corresponding to those used by the Centers for Disease Control and Prevention (CDC) to track mechanisms of injury for pediatric TBI
14
(refer to Supplementary Tables S1–S5; see online supplementary material at
Statistical analysis
Categorical data were reported as frequencies and percentages, whereas continuous data were reported as medians with interquartile ranges. Statistical analyses were performed using Stata, 16 and included chi-squared and proportion tests for categorical variables and Wilcoxon signed rank sum tests for continuous variables. A multi-variate logistic regression analysis was performed to identify factors associated with receipt of a neurostimulant prescription. Statistical significance was set at a p-value of <0.05. We included pre-injury variables with significance of p < 0.1 on univariate analysis with a neurostimulant prescription in the multi-variable logistic regression. Missing data were not imputed. The study was deemed exempt from review by the University of Pittsburgh Institutional Review Board.
Results
The records of 30,881 TBI patients were included in the analysis. Patients were majority male (63.8%), Caucasian (53.2%), and on public insurance (53.0%) (Table 1). After stratifying patients into four age groups, most were 1 month to 4 years old (42.9%). The most common etiology of TBI was fall (36.0%) or motor vehicle collision (35.7%) of patients with reported mechanisms of injury. Overall, mortality was 6.7%, and differed such that mortality was lower among patients who received neurostimulants (3 [0.3%] vs. 2053 [6.8%] for the non-stimulant group, p < 0.001).
Patient Characteristics by Neurostimulant Prescription Status
Portion of study population had missing data for the identified categories, reflected by “n” value next to category heading.
Overall, 878 (3%) received at least one neurostimulant prescription while admitted to the hospital (Table 1). Of patients with a length of stay of 14 days or greater (5054 patients), 711 (14.1%) received a neurostimulant. Compared with the non-neurostimulant group, the neurostimulant group was disproportionately older, with 286 (32.6%) patients between the age of 14 and 18 compared with 4508 (12.0%) patients in the non-neurostimulant group (p < 0.001). Patients who received a neurostimulant prescription had significantly longer hospital stays, with a median (interquartile range) of 36 (18–64) days compared with 3 (2–8) days for the non-neurostimulant group (p < 0.001) (Table 2). The neurostimulant group also had significantly more ICU days (11 [4–19] vs. 2 [1–3] days, p < 0.001). The patients in the neurostimulant group were more frequently mechanically ventilated (82.1% vs. 42.5%), were more likely to have invasive intracranial pressure (ICP) monitoring (42.3% vs. 10.0%), and craniotomy or craniectomy (13.0% vs. 7.3%) versus those in the non-neurostimulant group (all p < 0.001). Physical therapy evaluations were more frequently obtained for the neurostimulant group compared with the non-neurostimulant group (90.4% vs. 38.4%, p < 0.001). Finally, of the 20,925 (67.8%) patients included in Version 2 of the PHIS database, 58 of 673 (8.6%) patients who received a neurostimulant were discharged to a rehabilitation center, compared with 544 of 20,252 (2.7%) patients who did not receive a neurostimulant prescription (p < 0.001).
Injury Characteristics, Management, and Outcomes
Reflects subset of study population with reported mechanism of injury.
Wilcoxon rank-sum test; **Only reflected in Version 2.
ICU, intensive care unit; IQR, interquartile range; MVC, motor vehicle collision; OT, occupational therapy; PT, physical therapy.
A total of 878 (3%) patients received 1064 prescriptions for neurostimulant medications. The most commonly prescribed medication was amantadine (41.1%) followed by methylphenidate (38.1%) (Table 3). Overall, neurostimulants were started at a median of 17 (8–35) days following admission and continued during in-hospital care for a median of 11 (5–25) days. Dexmethylphenidate was given earliest at 9 (3–37) days post-injury for a median of 3 (1–9) days, followed by amantadine at 15 (9–28) days for 16 (8–31) days. Of patients who received a neurostimulant, 164 (18.7%) had a co-morbid diagnosis of ADHD. One hundred seventy-nine (16.8%) prescriptions were given to these patients, of which most were for methylphenidate (65.4%). Neurostimulant prescriptions per number of patients significantly increased over the study period (R 2 = 0.806, p < 0.05) accounted for by the rise in amantadine prescriptions (R 2 = 0.851, p < 0.05) (Fig. 2).
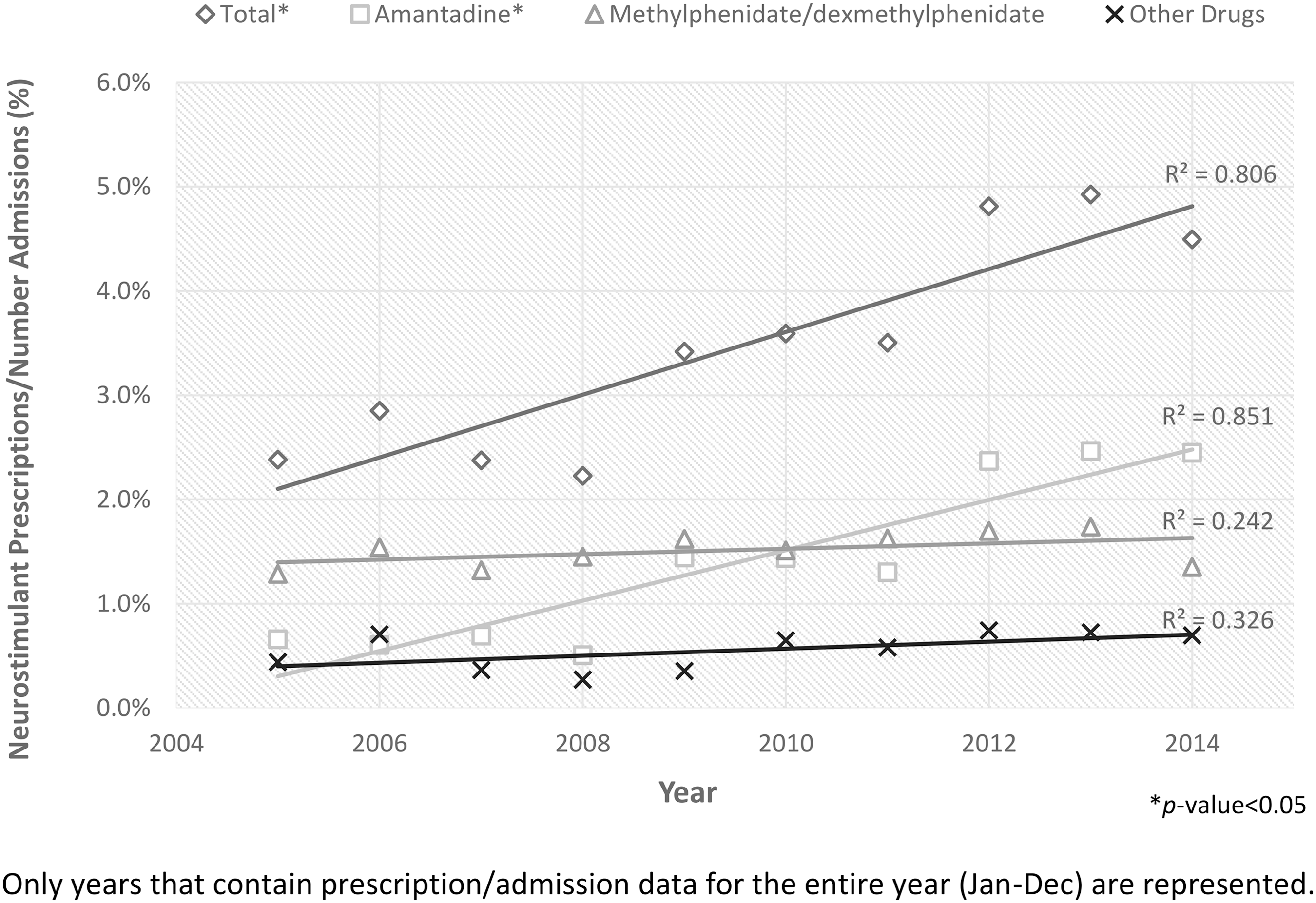
Neurostimulant prescribing trends over the course of the study period. Amantadine prescriptions and overall neurostimulant prescription frequency rose significantly between 2005 and 2014.
Neurostimulant Prescription Details
Refers to number of prescriptions; total patients: 878; 164 had ADHD.
ADHD, attention deficit hyperactivity disorder; IQR, interquartile range; LOS, length of stay.
The multi-variable logistic regression found a significant relationship between older age and neurostimulant prescription: ages 4–9 (adjusted odds ratio 2.8, 95% confidence interval [2.1,3.8]), ages 9–14 (4.0 [2.9,5.4]), and ages 14–18 (5.8 [4.3,7.8]) (all p < 0.001) (Table 4). Additionally, ICP monitoring (3.8 [3.1,4.5]), mechanical ventilation (3.4 [2.7,4.3]), motor vehicle collision mechanism of injury (3.1 [2.4,4.2]) (all p < 0.001), and craniotomy/craniectomy (1.3 [1.0,1.8]) (p = 0.04) were associated with neurostimulant prescription. Female participants in the study were less likely to receive a neurostimulant prescription (0.8 [0.7,0.99]) (p = 0.04).
Multivariable Logistic Regression for Neurostimulant Prescription
aOR, adjusted odds ratio; CI, confidence interval; ICP, intracranial pressure; MVC, motor vehicle collision.
Discussion
This study is the largest to date to analyze neurostimulant use in critically ill children with TBI, providing a scope of current prescribing practices. The results of this study show that neurostimulants were infrequently prescribed in the hospital setting compared with a recent observational study in adults (25% frequency). 13 Although information on the indication for neurostimulants was not available in the PHIS database, these drugs are typically prescribed to facilitate awakening from minimally conscious or vegetative states to enhance recovery and facilitate participation in rehabilitation. 17
Amantadine, the most commonly prescribed neurostimulant in this study, enhances synaptic dopaminergic transmission and antagonizes N-methyl-D-aspartate (NMDA) receptors. 18 –20 The pronounced rise in frequency of amantadine prescriptions over the study period may parallel the publication of an adult Phase III trial suggesting an improved rate of recovery with the use of amantadine after TBI. 8 This study was the first to show beneficial effects of a pharmacological agent on patient outcomes, and represented a key step in determining efficacy and safety data for use of amantadine. We found that neurostimulants in our study were prescribed with a bias toward teenaged children, unsurprising given that this age group is closest to randomized trials performed in adults. However, inpatient rehabilitation following pediatric TBI promotes independent ambulation and expressive language in children following abusive or non-abusive head trauma of all ages. 21 –25 Additionally, clinicians prescribed neurostimulants on average 2 weeks earlier than in the adult trial protocol, perhaps representing an interest in earlier rehabilitation interventions.
In children, amantadine has demonstrated a favorable safety profile after TBI and other acquired brain injury. 9,10 Pilot data also support improved symptomology and outcomes following neurostimulant prescription after concussion. 26,27 Two small prospective trials suggest improved elements of recovery with use of dopaminergic agents following severe TBI. 28,29
Female sex was associated with non-receipt of a neurostimulant prescription despite accounting for severity of illness markers. Following TBI, females have better survival and morbidity compared with males with similarly severe injuries, with protective hormonal effects postulated as a potential mechanism. 30,31 The PHIS database lacks information on duration of coma, preventing further analysis of whether the sex differences in our study were due to females having less of a coma burden that would otherwise prompt neurostimulant prescription. Other studies have not found sex to be a significant predictive factor in functional outcome after TBI, though disposition following a hospital stay and predictors of outcomes following injury may differ based on sex. 32,33 Although potentially less likely in children than adults to represent a key variable in determining outcome after injury, sex remains an important variable to explore in pediatric TBI, particularly because innate sex differences in the response of neurons to injury are well known in both pre-clinical and clinical studies. 34,35 Differences in response to neurostimulants after TBI are unknown, but there are sex differences in dopamine transmission after experimental TBI that may affect response to neurostimulants. 36
Twice as many children with severe TBI and neurostimulant prescription had physical therapy consultation than children without neurostimulant prescription, and less than 10% of children in this study overall were discharged to inpatient rehabilitation. Together with early allied health interventions in the ICU, 37 prescription of neurostimulants when indicated, and assessment by physical medicine and rehabilitation teams in a protocolized way may lead to improved outcomes for children with severe TBI. 4,38,39
In summary, lack of high-quality efficacy data and optimal administration of neurostimulants to improve arousal and facilitate rehabilitation for children with TBI suggests the need for robust research programs to positively impact patient outcomes. 5,10 –12,28,29,40
Limitations
We were not able to make conclusions regarding efficacy of neurostimulants on recovery following TBI. Because of the nature of billing/administrative coding data, the PHIS database does not contain information on drug indication, tolerance, efficacy, or drug dosage. Important clinical parameters such as GCS scores and other measures of neurological state were not reported; for injury severity, we used surrogate markers such as ICU admission and the need for mechanical ventilation. We were also unable to elucidate pre- versus post-injury ADHD diagnoses that may have impacted choice or administration of neurostimulant medications. Notably, we chose not to exclude patients with ADHD diagnoses from the study sample due to the mutually influential relationship of ADHD and TBI. 41 The database lacks post-ICU inpatient rehabilitation prescribing data, when more children may have been prescribed neurostimulants. Finally, caution must be exercised when forming conclusions based on statistically significant findings and their translation into clinical significance in a study of this size.
Conclusion
Neurostimulants have been shown to hasten recovery for adult patients with severe TBI, but use has been limited in pediatrics, and prospective data to support efficacy and best practices are limited. Prospective data are needed to inform guidelines for the use of neurostimulants and other aspects of rehabilitation throughout the continuum of care that coordinate many aspects of therapy and ultimately improve outcomes.
Footnotes
Acknowledgments
University of Pittsburgh School of Medicine, Dean's Summer Research Program and Scholarly Project.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.