
Abstract
Outcome prediction after spinal cord injury (SCI) is essential for early counseling and orientation of the rehabilitative intervention. Moreover, prognostication of outcome is crucial to achieving meaningful stratification when conceiving clinical trials. Neurophysiological examinations are commonly employed for prognostication after SCI, but whether neurophysiology could improve the functional prognosis based on clinical predictors remains an open question. Data of 224 patients included in the European Multicenter Study about Spinal Cord Injury were analyzed with bootstrapping analysis and multivariate logistical regression to derive prediction models of complete functional recovery in the chronic stage after traumatic cervical SCI. Within 40 days after SCI, we evaluated age, gender, the motor and sensory cumulative scores of the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), and neurophysiological variables (motor evoked potentials, sensory evoked potentials, nerve conduction study) as possible predictors. Positive outcome was defined by a Spinal Cord Independence Measure total score of 100. Analyzing clinical variables, we derived a prediction model based on the ISNCSCI total motor score and age: the area under the receiver operating curve (AUC) was 0.936 (95% confidence interval [CI]: 0.904–0.968). Adding neurophysiological variables to the model, the AUC increased significantly: 0.956 (95% CI: 0.930–0.982; p = 0.019). More patients could be correctly classified by adding the electrophysiological data. Our study demonstrates that neurophysiological assessment improves the prediction of functional prognosis after traumatic cervical SCI, and suggests the use of neurophysiology to optimize patient information, rehabilitation, and discharge planning and the design of future clinical trials.
Introduction
Prognostication of outcome following spinal cord injury (SCI) is as important to patients and their families as it is to the medical staff and to caregivers when planning rehabilitation. 1 Correct prognostication of outcome is also crucial to achieving meaningful early stratification when conceiving clinical trials. 2 However, because of the heterogeneity of lesion characteristics, the disability secondary to traumatic SCI is highly variable. Functional independence after rehabilitation typically depends on spinal lesion levels and severity. It also varies with the focal distribution of segmental spinal lesion pattern, resulting in a variable combination of central and peripheral neural lesion burden at any affected spinal segment. 3 Further, a multitude of secondary injury mechanisms with variable degrees of subsequent demyelination and axonal damage result from spinal trauma. 4 In this context, neurophysiological techniques have been suggested for prognostication because they are objective and available early after injury even if a patient is unable to cooperate. 5,6 In addition to clinical examination according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), neurophysiological evaluation allows for quantitative differentiation of gray and white matter injury at different spinal levels and for testing of distinct anatomic regions of the spinal cord. 4 A demyelination will typically result in slowing of conduction velocity and axonal damage results in amplitude reduction of evoked potentials or compound muscle action potentials.
We have shown in the past that neurophysiological evaluation can serve as an independent stratification tool in describing typical homogeneous cohorts among SCI patients, and that these cohorts can be used for prediction of functional outcome in paraplegic and tetraplegic patients. 3,7 –10 Neurophysiological evaluation can, therefore, provide an objective and quantitative measure of underlying spinal pathology. Although these aspects speak to a systematic use of neurophysiological evaluation in SCI, the significance for outcome prediction and relationship with function have not been systematically established. More specifically, given the high prognostic value of standardized clinical testing according to ISNCSCI examination, the additional cost and effort to obtain neurophysiological evaluation requires justification. 11 –13 Hence, it remains unclear what neurophysiological evaluation can add to improve prediction of functional outcome in traumatic SCI.
It was assumed that the complexity and extent of damage within the spinal cord would be reflected in the alteration pattern of combined sensory and motor evoked potential and nerve conduction study testing. Assuming that neural repair in the human central nervous system is minimal, we expected that permanent lesion burden would be reflected in the readout from neurophysiological evaluation very early on after spinal injury, thus relating to, and anticipating, functional outcome. We hypothesized that early neurophysiological evaluation assessment could enhance the predictive power of clinical examination for any severity and lesion level of cervical SCI in the assessment of functional prognosis.
Methods
Data were derived from the European Multicenter Study about Spinal Cord Injury (EMSCI) (
Clinical and functional assessments
Neurological examinations were performed according to the ISNCSCI. The scale provides a total motor score which ranges from 0 to 100, and a total light touch and pin prick score from 0 to 112 points, respectively. Severity of SCI was classified following the American Association of Spinal Cord Injury (ASIA)/ISNCSCI impairment scale (AIS) as A (motor–sensory complete), B (motor complete, sensory incomplete), C (motor–sensory incomplete), and D (motor–sensory incomplete, average of key muscles below the lesion show movement against gravity). 14,15 Examinations were performed by trained rehabilitation specialists with several years of experience in the field of SCI rehabilitation.
The functional assessments were scored by the team of physical and occupational therapists and nurses with several years of experience in the field of SCI and according to the validated Spinal Cord Independence Measure (SCIM) II/III protocol. 16,17 Both SCIM versions comprise different subscores relating to body function in self-care (20 points) and mobility (40 points), as well as bladder, bowel and breathing function (40 points). Different versions consist of minor adaptions in single scores, but no difference in subscores or total score (100 points).
Neurophysiological examination
Neurophysiological examinations were independently performed by trained technicians and experienced physicians according to common clinical standards. 18 All neurophysiological measurements were obtained on conventional clinically certified electromyography machines, and these examinations followed a strict measurement protocol throughout the EMSCI network. Recordings were obtained bilaterally for somatosensory evoked potentials (SEP) following stimulation of the ulnar and tibial nerves. For technical details of neurophysiological recordings see previous publications. 3,7,9,10 Motor evoked potentials (MEP) were obtained bilaterally following transcranial magnetic stimulation of the corresponding cortical motor area from anterior tibial and abductor digiti minimi muscles. For technical details of neurophysiological recordings see previous publications. 3,6,8 Nerve conduction studies were obtained from the ulnar and tibial nerves bilaterally. Distal latency, minimal F-wave latency, and amplitude of the compound muscle action potential from tibial anterior and abductor digiti minimi muscles were obtained. Readouts were transferred to the database and monitored by blinded raters before further evaluation.
Neurophysiological abnormalities from both sides were rated according to cutoff criteria in order to transform individual data into an ordinal scale.
Transformation to a score guided by clinical normative data was done for several reasons according to an earlier publication: 19 reduction of the number of variables (amplitude and latency of both SEP and MEP recordings, amplitude and F-wave persistence of nerve conduction studies each derived from four extremities allowed reduction from 24 to 3 variables), definition of robust pathological values to allow application in a clinical setting, reduction of variance, and an increased power (assuming that much larger numbers of patients would have to be included with an increasing number of variables). Criteria included amplitude, latency, and F-wave persistence. This resulted in an electrophysiological score. Within this score all neurophysiological examinations were rated as normal, impaired, or abolished, and scores were implemented as explained subsequently (Table 1).
Scoring of Electrophysiological Examinations
Electrophysiological examinations were scored according to the latency and amplitude in motor evoked potentials (MEP) and sensory evoked potentials (SEP), respectively. Nerve conduction studies (NCS) were scored according to amplitude of compound muscle action potentials and F-wave persistence as indicated.
UE, upper extremities; LE, lower extremities.
MEPs and SEPs were rated according to latency and amplitude of the collected potentials, respectively. Latency was normalized for body height. Limits were determined according to laboratory-determined reference values as follows.
Amplitude of MEP were scored with 2 points if they reached at least 0.1 mV, 1 point if clearly present but <0.1 mV, and no points if the potential was missing. Body height corrected latency for upper extremities and for lower extremities was scored with 1 point if it was <25 ms and <34 ms, respectively, otherwise it was scored with no points. A maximum score of 3 was achieved if latency and amplitude were within these defined normal limits, a score of 2 was achieved if either latency was delayed or amplitude was reduced, a score of 1 was achieved if both latency and amplitude were beyond limits, and a score of 0 was achieved if no potential could be obtained.
Amplitude of SEP was scored with 2 points if it reached at least 0.5 μV, 1 point if it was clearly present but <0.5 μV, and no points if the potential was abolished. Body height corrected latency <21.7 ms for upper extremities respectively <44.3 ms for lower extremities was scored with 1 point, otherwise it was scored with no points. A maximum score of 3 was achieved if latency and amplitude were within normal limits. A score of 2 indicated that either latency was delayed or amplitude was reduced, whereas a score value of 1 indicated that both latency and amplitude were beyond limits. A score value of 0 was attributed if no potential could be obtained.
The nerve conduction studies were scored according to compound motor action potential (cMAP) amplitude and F wave persistence. Amplitude was scored with 2 points if cMAP reached at least 5/4 mV in tibial/ulnar neurography, respectively, 1 point when it was below these limits, and no points when abolished. F-wave persistence was scored with 1 point if >50% in both studies, otherwise it was scored with no points. Therefore, a maximum score of 3 was achieved if all parameters were above limits, a score of 2 was achieved if cMAP amplitude or F- wave persistence was below limits, a score of 1 was achieved if cMAP and F wave persistence were below limits, and a score of no points if no cMAP, and therefore also no F-waves, could be collected.
Sum scores were calculated per modality (motor evoked potentials respectively sensory evoked potentials resp. nerve conduction study) with a maximum score of 12 each.
Patient selection
A whole database query was made on February 8, 2016, resulting in 3568 data sets of all included paraplegic and tetraplegic patients. Tetraplegic patients were identified according to the neurological level of injury (segments C1 to T1) in stage 2, if data were missing in stage 1. Patients who could not be classified at these time points because of missing clinical data or who were classified as paraplegic were excluded from the analysis. All AIS grades were included in the evaluation. For the analysis, we considered the baseline data collected between 16 and 40 days after SCI (stage 2) when available. When those data were missing, the stage 1 assessment (within 15 days from injury) was used for analysis. Measurements 6 months after SCI (stage 4) were used as outcome measures and if not available, the 12 month outcome (stage 5) was used.
Functional outcome
The functional outcome at 6 months (or at 12 months, if no data were available at 6 months) after SCI was assessed through SCIM II/III total score. A score of 100 (full score) was considered as a positive outcome. SCIM versions II and III within the EMSCI database were combined in the present evaluation, as total scores (maximum 100 points) do not differ between the two versions.
Statistical analysis
Candidate parameters for the prediction of a total SCIM score of 100 points, were identified using a stepwise augmentation procedure from the initial data set including age, sex, neurological level of injury, ISNCSCI total motor score, ISNCSCI total pin prick score, ISNCSCI total light touch score, MEP, SEP and nerve conduction study score. SCIM score was not included in the procedure as it was used as the outcome variable. The procedure was performed separately for the clinical and the electrophysiological parameters. We bootstrapped the stepwise augmentation procedure 100 times and counted how often each of the candidate variates remained in the final model. Parameters that were selected at least 60 out of 100 times were used in the analysis. 20 Using multivariate logistical regression models, where a presence of a SCIM score of 100 at 6/12 months was the dependent and the clinical or electrophysiological parameters within 40 days from injury were the independent variates, we estimated the probabilities for various combinations of predictors. Additionally, to test the discrimination capacity of each prediction model in the complete sample of 224 patients, a comparison of the prediction in both models was calculated in respect to a “rule in” threshold of >95% probability respectively “rule out” threshold of <5% probability reaching the outcome SCIM 100. We tested the predictions of the models with the χ2 test implemented in Stata's “roccomp” routine. We summarized continuous variates with means and standard deviations and dichotomous variates with percentages. A p value <5% was considered statistically significant. All statistical analyses were conducted using the Stata 14.2 statistics software package (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP).
Results
Study population
From a total of 3568 patients in the database, 317 could not be classified at stage 1 or 2 assessments because of lacking clinical data, and 1509 were classified as paraplegic and therefore excluded from further analysis. A total of 1742 data sets of tetraplegic patients were used for further analysis.
Although 1518 data sets were missing one or more baseline or outcome parameters, 224 data sets contained complete clinical and electrophysiological baseline data within 40 days after SCI and outcome data after 6 or 12 months (Fig. 1). Study population descriptive parameters are shown in Table 2. Thirty-one patients reached outcome SCIM 100 after 6–12 months after spinal cord injury. Detailed characteristics of these patients are shown in Table S1 (see online supplementary material at
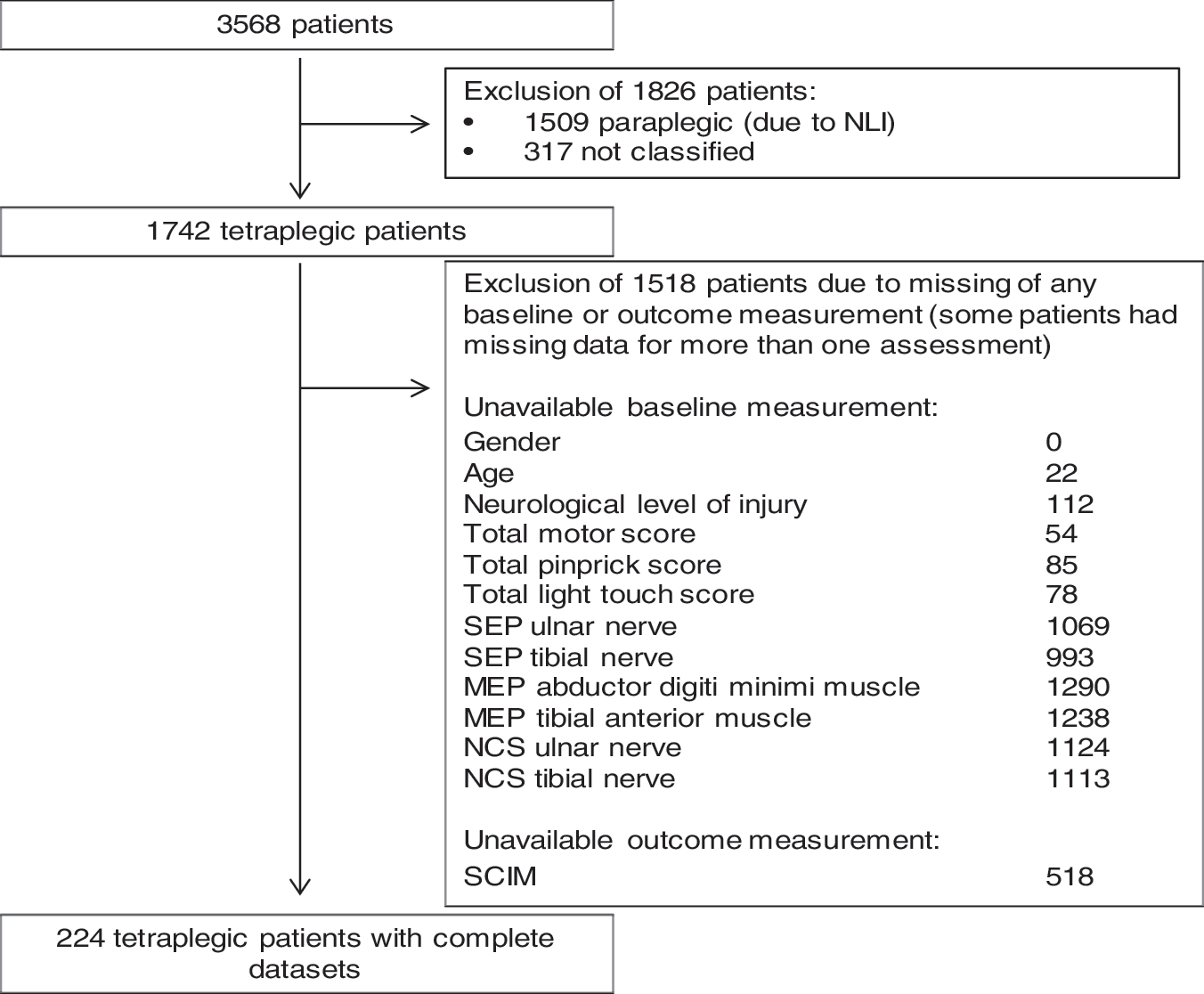
Identification of complete data sets of tetraplegic patients for statistical analysis. NLI, neurological level of injury; MEP, motor evoked potentials; SEP, sensory evoked potentials; NCS, nerve conduction study; SCIM, Spinal Cord Independence Measure.
Distribution of Baseline and Outcome Parameters
AIS, ASIA (American Spinal Injury Association) Impairment Scale; NT, not testable; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; MEP, motor evoked potentials; SEP, sensory evoked potentials; NCS, nerve conduction study; SCIM, Spinal Cord Independence Measure.
Identification of relevant baseline parameters for outcome prediction
The clinical parameters selected were patients' age at study entry and the total motor score. Performing 100 repeated prediction calculations with clinical parameters, ISNCSCI total motor score was included 100 times in the prediction model as the most important predictor and age was included 99 times. Sensory scores (total pin prick score, included 16 times, total light touch score, included 30 times), sex (included 8 times), and neurological level of injury (included 29 times) were by far less important in calculations (Table S2) (see online supplementary material at
The electrophysiological variables chosen were MEP, SEP, and nerve conduction study score, included to the same extent (MEP 97 times, SEP 86 times, nerve conduction study 99 times) in the prediction model.
Therefore, ISNCSCI total motor score, age, SEP, MEP, and nerve conduction study score could be identified as the most important baseline parameters and were therefore used for further receiver operating characteristic (ROC) analyses and multivariate logistical regression models.
Outcome prediction value of a single modality
ROC analysis revealed total motor score as the best single prediction parameter for the chosen outcome (total SCIM score 100) with an excellent AUC (0.909; 95% CI: 0.871–0.947). SEP score (AUC 0.829; 95% CI: 0.758–0.900) as well as MEP (AUC 0.868; 95% CI: 0.799–0.936) and nerve conduction study score (AUC 0.832; 95%CI: 0.770–0.895) alone also showed reasonable outcome prediction. Repeated analysis considering the 6 month outcome (available in 199 of 224 patients) and the 12 month outcome (available in 176 of 224 patients) showed corresponding results (Table S3) (see online supplementary material at
Electrophysiological examinations improve outcome prediction
To evaluate the additional benefit of electrophysiological examinations, multivariate logisticsl regression models for outcome SCIM score 100 were calculated (Table S4)(see online supplementary material at
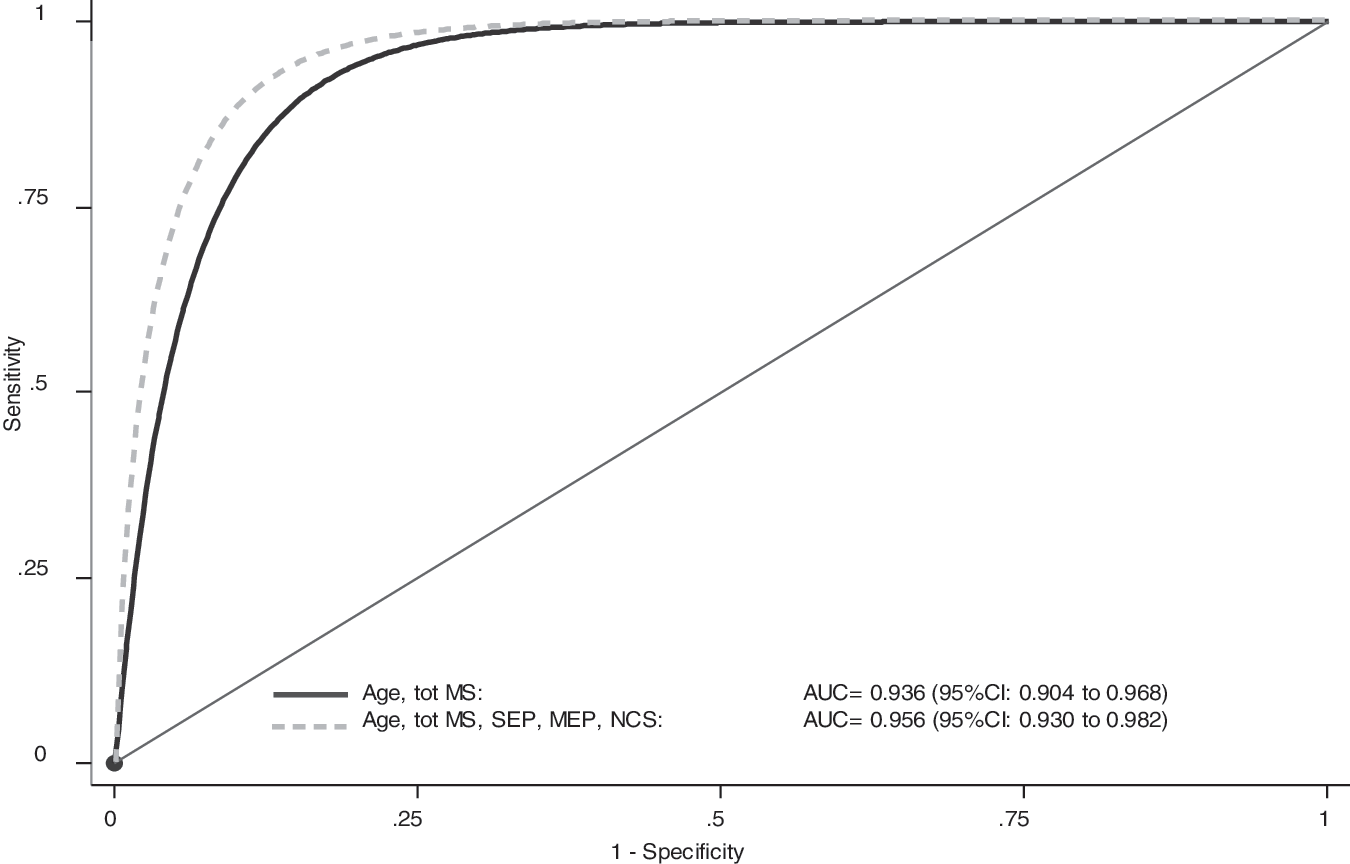
Electrophysiological examinations improve outcome prediction. Prediction of model 1 (black line), including only age and total motor score, could be significantly improved from an AUC of 0.936 (95% CI: 0.904–0.968) to 0.956 (95% CI: 0.930–0.982) with additional electrophysiological information in model 2 (dotted line, p = 0.019) including age, total motor score, and all neurophysiological variables. MS, motor score; MEP, motor evoked potentials; SEP, sensory evoked potentials; NCS, nerve conduction study; AUC, area under the receiver operating curve; CI, confidence interval.
The effect of the increased discrimination capacity of the model with electrophysiology can be translated into additional patients correctly classified given specific rule-in or rule-out probability thresholds (detailed information see Table S5)(see online supplementary material at
Comparing the two models within the group reaching SCIM 100 outcome, one more patient was classified correctly (“rule in”) when using the full rather than the simple model. On the other hand, when comparing the two models within the group not reaching SCIM 100 outcome, seven more patients were classified correctly (“rule out”) when using the full rather than the simple model. Only one false positive prediction was found when applying the simple model.
Discussion
In this analysis, we could show that early prediction of functional outcome can be achieved with high accuracy based on clinical assessment of ISNCSCI total motor score alone, as well as by neurophysiological examinations. However, accuracy could significantly be increased when combining both clinical examination and neurophysiology. The number of patients for whom a correct functional prediction could be achieved was increased in the full model with respect to neurophysiological information. This is highly relevant, given the potential reduction of numbers to treat when powering clinical trials and for the individual benefit of each additional correctly predicted patient, as accurate outcome prediction at an early stage after SCI is crucial for planning the rehabilitation course and long-term living modalities. Further, at an early stage, clinical examination can be less reliable because of the impaired ability of a patient to cooperate and, therefore, electrophysiological examinations could provide standardized additional predictive power early after injury. We will further discuss these results and why prediction precision remains difficult and why improving the accuracy of outcome prediction is essential.
The SCIM score provides reliable functional information on activities of daily living and is a routine assessment during SCI rehabilitation and treatment. 17 Moreover, the Spinal Cord Outcomes Partnership Endeavor (SCOPE) suggested SCIM III as primary outcome measure for pivotal phase III clinical trials. 21 SCIM score at 6/12 months has been chosen for outcome, as most clinical improvement is achieved at this time and rehabilitation in tetraplegic patients is usually accomplished after 9 months. 22 Predicting functional status at that time, therefore, is crucial for organizing assistance and devices after hospitalization. In previous studies, 11,23 the functional recovery assessed by SCIM at 6 months and 1 year has commonly been used for the derivation of clinical prediction rules of functional recovery after SCI
In this study, we intended to show the relevance of adding neurophysiological assessments to improve a prediction model in principal. We dichotomized patients' outcome based on SCIM II and III total score 6 months after SCI in I; “optimal functional recovery” when the SCIM total score was 100 and II. We coded “incomplete functional recovery” when the SCIM total score was <100, because we considered that the distinction of “optimal” versus “incomplete” recovery could be regarded as unambiguous. SCIM total score is a global score, derived from the sum of different subscores of functional domains. For that reason, any other cutoff value of SCIM total score would have been problematic, as values <100 can correspond to very different clinical conditions, with possible limitations in different domains (e.g., arm function, transfers, bladder and bowel management, respiration). By choosing 100 as cutoff, we could distinguish two distinct populations: those with a full functional recovery as assessed by SCIM and those with a variable degree of functional impairment. This is instrumental to our study, which was conceived as a proof of principle to evaluate the additional predictive value added from neurophysiological examinations to clinical predictors. This finding prepares the field for further studies assessing the potential contribution of neurophysiological examinations to the prediction of a particular functional outcome in SCIM domains.
ISNCSCI examination is a standardized, reliable clinical examination of SCI patients used commonly in the SCI community. Assessment of motor, as well as sensory, function by light touch and pinprick testing is implemented in the protocol and, therefore, provides information about motor and sensory system integrity. Therefore, it is not surprising to find the high predictive value of total motor score. However, neurophysiological examination can provide additional independent and objective information about spinal cord function. SEP reflects the dorsal column, MEP reflects the corticospinal tract and nerve conduction study reflects the anterior horn and peripheral nervous system function. Thus, additional anatomical and somatotopic information about the extent and localization of nervous system damage is reflected in neurophysiological data. A reliable quantification of the extent of the impairment of spinal cord function is available from these recordings. Neurophysiological techniques have been suggested for prognostication because they are objective and available early after injury, even if a patient is unable to cooperate. 5,6 The obtained potentials can be rated according to robust cutoffs for latency and amplitude as normal, impaired, and abolished. To simplify the use of electrophysiological examinations, a scoring was introduced in this study as mentioned (Table 1). Thereby the abundance of neurophysiological data can be reduced and scaled for use in the simplification of a prediction model.
Although 1742 of 3568 patients could be identified as tetraplegic, only 224 complete data sets could be used for our statistical analysis, because of missing baseline data or outcome assessments. In most cases, electrophysiological data were missing (Fig. 1). One reason is that not all SCI centers participating in the EMSCI network have implemented the complete electrophysiological protocol in the clinical workup within the rehabilitation course and, therefore, not all patients were tested with neurophysiological examinations. On the other hand, at baseline (up to 40 days after SCI), because of complications, some patients' status might have been such that some of the results of the clinical examinations could not be performed. Further, because of implementation of all electrophysiological modalities in our model, we observed a relatively high dropout rate of patients for whom incomplete neurophysiological examinations were performed. However, 224 data sets with >30 patients reaching the predicted outcome (SCIM score of 100) represent a reasonable sample for statistical analysis. Descriptive parameters (Table 2) of our tetraplegic study population were comparable with those of populations published before and, therefore, the evaluation of prediction can be assumed to be representative. 3
In a prediction model published earlier, age, motor score, and light touch sensation in the segment L3 and S1 had been identified as crucial parameters for prediction of walking ability. 11 The Lower Extremity Motor Score of ISNCSCI was identified as main predictor of bladder function recovery after SCI. 12,13 SEP, MEP, and nerve conduction study have been shown to provide important information for prediction of the outcome of walking ability as well as hand function. 3,5,6,9,10 So far, no combination of these modalities has been evaluated for prediction, and the additional value of electrophysiological examinations has not been shown.
In this study, total motor score and age, as well as SEP, MEP, and nerve conduction study score, but not sensory scores, were identified as useful parameters for outcome prediction using the bootstrapping procedure. A possible reason for this may be the fact that dermatomal sensory testing has little meaning for total function in activities of daily life as assessed by SCIM. Another reason may be the comparatively coarse scale of sensory rating distinguishing only the levels of impaired and loss of sensation, whereas motor rating is more elaborate. Further, inconsistencies of sensory scoring might be a reason for poor relevance for prediction in our analysis. On the other hand, SEP scores did show good reliability for outcome prediction, although both light touch sensory testing and SEP examinations reflect dorsal column function. This might be attributed to a variety of causes. SEPs objectively measure dorsal column conductivity and may, therefore, be more representative of the likelihood of preserved spinal integrity. This was shown earlier, as the initial presence of tibial SEPs after SCI was highly related to positive functional outcome in terms of the regaining of walking ability. 5 Similarly, presence and quality of ulnar SEPs were shown to indicate good hand function outcome. 10 Given the fact that SEPs are only preserved when a significant number of dorsal column fibers are excitable in a synchronized volley, it is conceivable that tibial or ulnar SEP represent a benchmark for preserved spinal conductivity, indicating good likelihood for preserved spinal transmission. This may be a better criterion than arbitrary sensory scores, which are dependent on patients' and raters' subjective judgment.
It should be pointed out as a limitation that subgroup analysis of AIS categories could not be performed because a full functional recovery as indicated by a total SCIM score of 100 was only found in patients who were SCI incomplete and initial AIS D. For technical reasons, we decided to use this unambiguous total SCIM value as target outcome in this proof of principle study to test the additional prediction value of electrophysiological examinations. From a clinical standpoint, the use of a variety of SCIM dichotomization limits and/or subscores would likely be more meaningful, and could provide analysis within AIS subgroups. However, given the notion that SCIM is a composite score, any other dichotomization limit would mean widely varying individual outcomes with respect to possible combinations of the sums of SCIM subscores for self-care, respiratory/bladder function, and mobility. Further, any analysis within SCIM subscores would not have allowed a general statement about the additional benefit of electrophysiological assessment for the prediction of global function in SCI recovery. As a consequence, the results of this analysis may not be generalized to all AIS grades. More detailed outcome analyses with respect to SCIM domains such as self-care and hand function are required, including electrophysiological data. This will allow clinically more meaningful dichotomizations and, therefore, will likely include all AIS groups. The overarching goal is clinically meaningful prediction of detailed function with best precision. According to the present analysis, neurophysiological examinations are good candidates to contribute significantly to prediction precision.
Conclusion
In a population of 224 tetraplegic patients, our study has shown excellent prediction of full functional recovery 6–12 months after traumatic SCI by use of ISNCSCI, age, SEP, MEP, and nerve conduction examinations.
The prediction model based on clinical variables could be significantly improved by combining it with electrophysiological multimodal parameters, reflecting better prediction precision because of the addition of neurophysiological data. Our analysis suggests the use of neurophysiology in the workup of patients with SCI, in order to provide the best possible outcome prediction for adequate patient information and future planning.
Footnotes
Acknowledgments
We thank the participating EMSCI network centers for providing data used for these analysis, in particular Norbert Weidner (Heidelberg, Germany), Henk van de Meent (Nijmegen, Netherlands), Rainer Abel (Bayreuth, Germany), Thomas Meiners (Bad Wildungen, Germany), Carl Hans Fürstenberg (Karlsbad Langensteinbach, Germany), Doris Maier (Murnau, Germany), Yorck-Bernhard Kalke (Ulm, Germany), Klaus Röhl (Halle, Germany), and Jesus Benito (Barcelona, Spain). Chiara Pavese is partially supported by an investigator fellowship from Centro Comunicazione e Ricerca, Collegio Ghislieri, Pavia, Italy.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.