
Abstract
There is a need for better tools to objectively, reliably, and precisely assess neurological function after sport-related concussion (SRC). The aim of this study was to use a robotic device (Kinesiological Instrument for Normal and Altered Reaching Movements; KINARM) to quantify neurological impairments in athletes acutely and when clinically asymptomatic post-SRC. Robotic assessments included five KINARM standard tasks that evaluate aspects of motor, sensory, and cognitive function. We hypothesized that acutely concussed athletes would demonstrate significant rates of impairment on the robotic assessment, and that impairments would be associated with acute symptom severity. Pre-season assessments were conducted from 2011 to 2016 on 1051 athletes. Eighty-four athletes were reassessed acutely (≤10 days post-injury) and while symptomatic post-SRC and 89 when clinically asymptomatic. Forty-four parameters were measured from the KINARM assessment to characterize neurological function. Reliable change indices (80% confidence interval) identified impairments in healthy and concussed individuals for each parameter. In concussed individuals, impairment rate varied across parameters from 4% to 27% at the acute time point and from 2% to 18% when clinically asymptomatic. Healthy athlete impairment rates were between 2% and 16% across all testing time points. We identified relationships between acute symptom severity and task performance for only two parameters, both of which evaluated attributes of motor function. Overall, the KINARM identified impairments in motor, sensory, and cognitive function in athletes with SRC; however, impairment rates were low and largely did not relate to symptom severity. More complex tasks may be necessary to identify potentially subtle neurological impairments post-SRC.
Introduction
Concussion is now recognized as one of the most common injuries occurring in contact, collision, and high-speed sport. 1,2 Yet, the ability of healthcare professionals to effectively diagnose, prognosticate, and manage concussions remains limited by the lack of a gold-standard assessment. 3 An ideal assessment approach needs to be objective, precise, reliable, and multi-dimensional, with a level of efficiency that allows it to be clinically feasible. However, many of the neurological assessments currently used in sport-related concussion (SRC) are dependent on patient symptom reporting, subjective interpretation, and grossly abnormal clinical signs (e.g., forgets instructions, answers questions slowly, and visibly unsteady gait). As a result, the identification of deficits is easily obscured by patient factors and examiner bias related to previous training and experiences. Nevertheless, the development of better assessment tools is hampered by the variable symptoms and often subtle deficits that can be experienced after SRC. 3
Robotic technology can provide a means for developing neurological assessments that are objective, reliable, efficient, and precise. 4 –10 The Kinesiological Instrument for Normal and Altered Reaching Movements (KINARM) 11 is a robotic device on which a set of brief (∼2–4 min) standard tasks have been developed to evaluate upper-extremity motor and sensory control, as well as aspects of cognitive function. KINARM tasks that have been examined in previous clinical work include: Visually Guided Reaching (VGR) 7,12,13 to evaluate upper extremity visuomotor capability; Position Matching (PM) 9,12,14,15 to evaluate upper extremity proprioceptive capability (i.e., position sense); Object Hit (OH) 8,12 to examine rapid bimanual motor control; Object Hit and Avoid (OHA) 10,12 to examine attention, rapid motor selection and response inhibition; and Trail Making B (TMB) 5,12,16,17 to evaluate task-switching. The neurological domains tested by these robotic tasks overlap with those evaluated by many traditional assessments used after traumatic brain injury (TBI; e.g., Fugl–Meyer Assessment, Trail Making Tests, and Functional Independence Measure), 13,18 –21 and impaired performance on each of these KINARM tasks has been identified in individuals with mild, moderate, and severe non-sport-related TBI across varying stages of recovery. 12,13,18 Notably, Debert and colleagues reported impairments on the KINARM VGR and PM tasks in individuals with non-sport-related TBI who attained normal scores on traditional clinical assessments. 13 Other work found that performance on the KINARM task battery described above within 24 h of mild non-sport-related TBI was predictive of symptoms persisting for at least 3 weeks post-injury. 12
Less is known about the utility of the KINARM for neurological assessment, specifically after SRC. SRC is generally thought to represent a subtler subset of TBIs 22 and is commonly studied separately from other forms of TBI. Work investigating motor and sensory abilities in SRC has typically focused on postural stability 23 –26 and gait, 27 –30 yet given findings in other types of TBI, 12,13,18 it is plausible that the upper-extremity abilities evaluated by many of the KINARM standard tasks could also be impacted by SRC. Moreover, cognitive testing is considered an essential component of SRC assessments, 31 and the KINARM device allows incorporation of cognitive testing (e.g., TMB task) into a multi-dimensional neurological assessment battery. To date, only one previous study has utilized the KINARM in SRC. 17 When compared to normative values, pediatric ice-hockey players with a remote history of concussion displayed nearly no deficits in the KINARM standard task battery described above. 17 Nevertheless, no previous work has considered the potential of the KINARM to identify neurological deficits acutely, or to predict and/or track recovery after SRC.
In the present study, we baseline tested athletes on a KINARM standard task battery during the pre-season and reassessed within 10 days of sustaining an SRC, and then again when the athlete was clinically asymptomatic. We identified SRC-related impairments on an individual basis through application of reliable change indices (RCIs), which account for test-retest variance to determine whether change in performance from one assessment to another is abnormal. 32 This baseline testing and RCI approach is in contrast to previous clinical work with the KINARM, which has typically involved comparing an individual's performance on a single post-injury test to healthy normative values, 7 –10,13,17,18 but it is in accord with other work in SRC studying cognition 33 –35 and balance. 24 To our understanding, the baseline testing approach is commonly used in SRC research to account for athletes' unique abilities (i.e., because of different sport demands, position, skillsets, experience, etc.) and to improve statistical power for detection of potentially subtle deficits, issues that are not as problematic in other clinical populations that we have studied with the KINARM (e.g., non-sport-related TBI, stroke). Further, athletes participating in contact, collision, or high-speed sports represent a specific, identifiable group in which a large number of concussions are expected to occur in a given period of time. 36,37 As a result, a baseline testing approach is much more logistically plausible for this population than most other neurological conditions. We expected that athletes would demonstrate significant rates of impairment on robotic tasks both acutely post-concussion and when clinically asymptomatic, and that those impairments would be associated with higher acute symptom severity. Overall, this study was designed to add new knowledge about the potential utility of the KINARM for identifying acute neurological deficits and tracking recovery after SRC.
Methods
Participants
Baseline robotic assessments were conducted from 2011 to 2016 during the pre-season on elite athletes ranging in age from 15–40 years old and participating in contact/collision/high-speed sports. Study participants were recruited through and tested at the WinSport Medicine Clinic (now Group23 Sports Medicine) and the University of Calgary Sport Medicine Centre in Calgary, Canada. A subset of athletes returned on one to two occasions within their first study season to participate in repeat testing after the initial baseline assessment. Athletes enrolled in the study over multiple seasons participated in annual baseline testing and, as a result, completed more than one baseline assessment. Data from participants who completed repeated assessments in a healthy, uninjured state, both within a single season and across multiple seasons, were used to determine RCIs for each robotic measure (see Statistical analyses section). Athletes were considered to be in a “healthy state” and their data used in these analyses if they self-reported as free of any post-concussion–like symptoms related to previous injuries, were participating fully in sport, and did not sustain any injuries that could impact robot performance between assessments.
All athletes enrolled in the study were asked to return for assessment as soon as possible (within 10 days) after SRC. Athletes reported to the clinic after sustaining a suspected concussion on the recommendation of their team certified athletic therapist or physiotherapist, and all SRCs were diagnosed and managed by a sport medicine physician (B.W.B.). Athletes were monitored during recovery and asked to complete a final robotic assessment when clinically asymptomatic. Athletes were deemed clinically asymptomatic by a sport medicine physician (B.W.B.) when their subjective self-report of symptoms (Sport Concussion Assessment Tool v3, Post-Concussion Symptom Scale; SCAT PCSS) returned to baseline levels or lower (i.e., subjectively 100%) and they passed standard clinical assessments (i.e., clinically asymptomatic). While we collected baseline, post-concussion, and clinically asymptomatic assessments in the majority of our sample, in some cases, our ability to assess athletes at the acute post-concussion time point was precluded by extenuating circumstances (e.g., athlete in non-local competition). For these athletes, we collected only a baseline and a clinically asymptomatic assessment. In other cases, athletes were clinically asymptomatic at the time of initial post-concussion assessment (≤10 days) or completed the post-concussion assessment but did not return for the final clinically asymptomatic assessment.
All participants provided written, informed consent before commencing the study procedures. Procedures were approved by the University of Calgary Conjoint Health Research Ethics Board (Ethics ID: 23963) and conducted in accord with its guidelines.
Robotic assessment
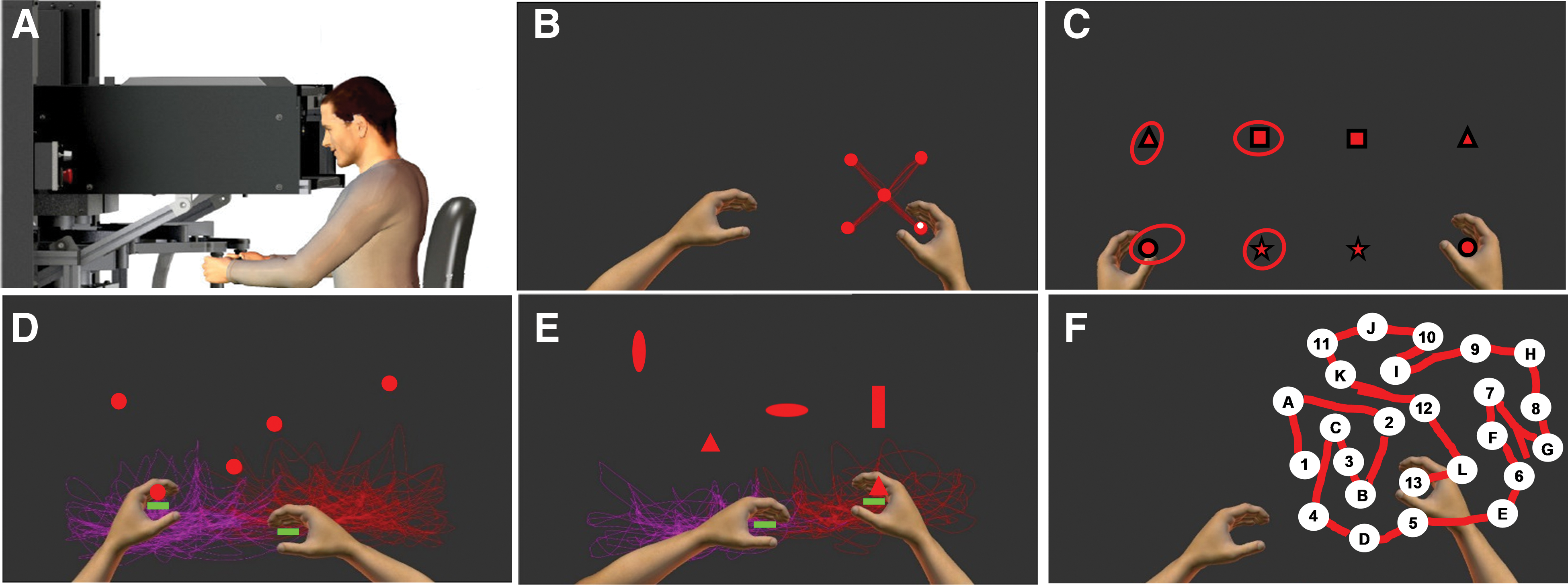
Robotic assessments were conducted with the KINARM end-point device (BKIN Technologies Ltd., Kingston, ON, Canada). Positioned in front of the KINARM and grasping the end-point handles, participants moved their arms in the horizontal plane to interact with an augmented reality system displayed in the same plane. Robot height was adjusted so participants' heads rested in the center of the visual field (Fig. 1A). From 2011 to 2013, all participants were assessed while seated in front of the KINARM. In 2014, the KINARM was modified to accommodate a standing posture, and all participants from then on were assessed while standing. Participants tested post-concussion and, when clinically asymptomatic, were always assessed in the same posture as their most recent baseline assessment.
The KINARM end-point robotic device (
A robotic assessment session was ∼20 min in duration and included the following tasks: Visually Guided Reaching, 7,13,14 Position Matching, 9,13,14 Object Hit, 8 Object Hit and Avoid, 10 and Trail Making B. 5,16,17
The Visually Guided Reaching (VGR; Fig. 1B) task evaluated upper-extremity visuomotor capability. The robot handle was displayed as a white circle (0.5-cm radius) and targets shown as red circles (1.0-cm radius). Participants used the dominant arm to reach as quickly and accurately as possible from the central target to one of four peripheral targets located 10 cm away and then back. Peripheral targets were presented in a pseudo-random order for a total of 20 out and 20 back reaching movements.
The Position Matching (PM; Fig. 1C) task assessed upper-extremity proprioception (position sense). With the participants' eyes closed to occlude visual feedback, the robot moved the dominant arm (passive arm) to one of four possible targets located at the corners of a 20 × 20 cm square grid. When the passive arm movement was complete, participants moved the non-dominant arm (active arm) to mirror-match the passive arm position, notifying the operator when they had matched. Twenty-four trials were completed with target locations presented in a pseudo-random order.
The Object Hit (OH; Fig. 1D) task examined rapid, bimanual upper-extremity motor ability and visuospatial attention. Robot handles were represented as 2-cm-wide green paddles. Objects (red circles with 2-cm radius) were “dropped” from 10 evenly spaced bins across the top of the screen. Participants used both hands to hit as many objects away as possible, receiving haptic feedback (i.e., small perturbation) when an object was hit. Over 105 sec, 30 objects were dropped at random from each bin (300 objects total). As the task progressed, object speed and frequency increased. The size of the paddles was smaller and the initial speed of the objects faster in this version of the task relative to the original task developed for the KINARM. 8
The Object Hit and Avoid (OHA; Fig. 1E) task evaluated similar attributes as the OH task, with added emphasis on attention, rapid motor selection, and inhibition. The task proceeded similarly to OH, except at the beginning participants were shown two of a possible eight object shapes that would be “dropped” from the bins at the top of the screen. Participants were instructed to hit those two “target” shapes, while avoiding the other six “distractor” shapes. Distractors passed through the participants' paddle if contacted. Two hundred targets and 100 distractors were dropped over 105 sec. As with OH, this version of OHA was modified to increase difficulty relative to the original task developed for the KINARM. 10
The Trail Making B (TMB; Fig. 1F) task is a robot-based version of the standard neuropsychological paper-and-pencil task designed to evaluate task-switching. 16 The robot handle was represented as a white circle (0.5 cm radius), and an array of 25 white circular targets labeled with letters (A–L) and numbers (1–13) was presented. Participants traced through the targets in an alpha-numeric sequence (i.e., 1-A-2-B-3-C…12-L-13) as quickly as possible. When a correct target was entered, the target turned green. If an incorrect target was entered, the target turned red and the participant was required to return to the previous correct target before continuing. Participants were familiarized to the task by completing a five-target version of the task before the full task. Participants were randomly presented with one of eight possible target patterns.
Robotic outcome measures
Forty-four parameters quantified performance on spatial and temporal aspects of the five tasks (Table 1). Parameter performance was quantified in each participant as a standardized z-score developed from an age-adjusted normative model of single-session baseline performance of healthy athletes between 18 and 40 years of age (BKIN Technologies Ltd.). 38 Seated and standing KINARM performance z-scores were developed separately, with the following sample sizes for the normative data sets: seated: VGR, n = 522; PM, n = 520; OH, OHA, n = 528; TMB, n = 528; standing: VGR, n = 147; PM, n = 147; OH, n = 147; OHA, n = 144; TMB, n = 148 (BKIN Technologies Ltd.). 38
Robotic Tasks and Outcome Measures
Data from the following parameters are not reported in the current study because it was non-normal and could not be converted to z-scores: VGR – ISR; OHA – TDH, DHD, DHND; TMB – EC.
“Task scores” were also derived from the normative data sets described above to capture overall performance on a task. 38,39 Briefly, z-scores for each parameter in a given task were transformed into zeta-scores, where the best performance was zero and higher values reflected poorer performance. The root mean square (RMS) distance of all parameter zeta-scores was then computed for each participant in the normative data set. Distribution of these RMS values was transformed into z-space and then into positive scores, such that zero denotes best performance and larger values indicate poorer performance. The units of the task score follow the same percentiles as ±1 standard deviation (SD) of a normal distribution (i.e., 1 = 68.3%, 2 = 95.4%, etc.). 38 –40
Normative models of KINARM standard task performance for athletes under 18 have not yet been developed. However, after determination of a negligible effect of age on task performance between 15- and 18-year-olds (see Supplementary File),(see online supplementary material at
Clinical variables
Self-reported history of concussion (including self-reported dates), migraines, attention-deficit hyperactivity disorder (ADHD), anxiety, and depression were collected from enrolled participants. Athletes with a history of concussion before the study were only included in the study if they self-reported that all symptoms had resolved since their previous SRC and they were participating fully in sport. The SCAT (v3) was administered by a qualified health professional (M.S.C., B.W.B.) at the post-concussion appointment. Only participants who continued to experience post-concussion symptoms at this assessment went on to complete the acute post-concussion robotic assessment. Last, the number of days between the concussion and symptom resolution (i.e., days to clinically asymptomatic) was recorded.
Statistical analyses
Before converting data to RCIs, we assessed whether the distribution of change in performance across sessions (tests 1 to 2, tests 2 to 3, and tests 1 to 3) in the healthy individuals differed based on: sex (male vs. female), history of concussion (yes vs. no), testing posture (seated vs. standing), and testing time frame (repeat testing within a single season vs. on an annual basis). These comparisons were made through visual inspection and objective evaluation of the data distributions with Kolmogorov–Smirnov Z tests for each parameter. For each of the above-mentioned variables (sex, history of concussion, posture, and time frame), there were a total of 147 comparisons of distributions to be conducted (44 parameters and five task scores, comparing change between tests 1 and 2, tests 2 and 3, and tests 1 and 3). In healthy athletes with a history of concussion, we also conducted multiple (147 total) bivariate Spearman's correlation analyses to evaluate the relationship between the self-reported time (months) since their last concussion with their change in performance across sessions for each parameter. Given that the vast majority of statistical tests examining these variables yielded non-significant results (see Results section), we collapsed all of the healthy athlete data into a single data set from which we derived the values needed to calculate RCIs for each robotic parameter.
The changes in robotic parameter z-scores between assessments were then converted to RCIs for the data from concussed athletes (e.g., baseline to post-concussion) and the healthy individuals (e.g., test 1 to test 2) that informed the RCI calculations. This allowed for comparison of rates of impairment identified in healthy and concussed groups. RCIs were calculated using the equations provided by Jacobson and Truax
32
and adjusted for practice effects. Calculated RCI values were interpreted against z-distribution critical values, such that ∼10% of the sample would be expected to be considered impaired on each parameter based on chance (80% confidence interval). The supplementary information (including Supplementary Table 1) (see online supplementary material at
Based on RCI calculations, the proportion of healthy athletes and athletes with concussion who were classified as impaired on each robotic parameter and task score was quantified. The number of impairments detected for each individual on each task was also quantified. Mann–Whitney U tests compared the median number of parameter impairments identified in each task in healthy versus concussed athletes. The number of impairments identified when considering tests 1 and 2 and tests 1 and 3 in healthy individuals were compared to the most recent baseline and the acute post-concussion assessment, and the most recent baseline and the clinically asymptomatic assessment, respectively, in the concussed athletes. Next, chi-square tests of association were conducted between SRC status (i.e., healthy or concussed) and impairment status (i.e., normal or impaired) for each parameter at each time point (i.e., tests 1 to 2/baseline to acute post-concussion and tests 1 to 3/baseline to clinically asymptomatic).
Further analyses were conducted on those parameters for which SRC was associated with impairment (based on chi-square tests above) to determine whether identification of impairment on these parameters was associated with other clinical measures. These analyses involved additional chi-square tests of association between impairment classification and history of concussion (yes or no), migraines (yes or no), and acute SCAT PCSS score. For the purpose of these analyses, acute SCAT PCSS score was broken into categories (0, 0–5; 1, 6–22; 2, 23–88; 3, 89–132) where higher values indicate greater symptom severity, similar to past work. 41 Too few participants presented with a history of ADHD (n = 6), anxiety (n = 3), and depression (n = 0) for these clinical variables to be considered. Spearman's correlation coefficients (rs) were also determined to evaluate relationships between the following variables: SCAT PCSS score, RCI values of KINARM parameters for which concussion was associated with impairment at the acute post-concussion time point, the number of days until clinically asymptomatic, and age.
In secondary analyses, we conducted Mann–Whitney U tests to compare the median number of parameter impairments identified in each task at the acute SRC time point in concussed athletes who were reassessed ≤3 days post-injury and those who were reassessed between 4 and 10 days post-injury. In these same individuals, chi-square tests of association were conducted between post-concussion assessment time frame (i.e., ≤3 days post-concussion or 4–10 days post-concussion) and impairment status (i.e., normal or impaired) for each parameter. Where associations between assessment time frame and impairment status were detected, relationships between KINARM parameters and clinical variables were further examined in the concussed athletes who were tested ≤3 days post-injury. Chi-square tests considered associations between KINARM parameter impairment status and categorical clinical variables, whereas Spearman's correlations were used to examine relationships between KINARM parameter RCI values and continuous clinical variables.
Given that this was the first study of the use of KINARM tasks to assess acute SRC, all analyses were considered exploratory with significance level set at p < 0.05, uncorrected. Data are reported as mean ± SD. All statistical analyses were performed in MATLAB 2016a (The MathWorks, Inc., Natick, MA) and SPSS software (SPSS 23.0; IBM Corporation, Armonk, NY).
Results
Participants
A total of 1051 athletes completed initial baseline assessments for the study. Of those, 105 athletes (age, 20.1 ± 4.7 years) completed two assessments in a healthy, uninjured state, and 81 (20.4 ± 4.5 years old) athletes on three occasions. Over the study period, 114 concussions were sustained in 105 athletes (age, 18.2 ± 3.3 years at concussion). Symptoms were resolved within the study period in all cases. Seven athletes sustained two concussions and 1 sustained three concussions. Only the first concussion was considered for the individuals who sustained recurrent injuries over the course of the study. Of the 105 concussions included in the analyses, 84 were assessed while still symptomatic and within 10 days post-injury (4.0 ± 2.4 days, ≤3 days, n = 40; 4–7 days, n = 35; 8–10 days, n = 9), and 89 were assessed when clinically asymptomatic. Five athletes tested at the acute post-concussion assessment, and 2 athletes at the clinically asymptomatic assessment could not complete all of the robotic tasks because of symptom exacerbation or reoccurrence. Figure 2 shows a flow chart depicting participant numbers at each phase of the study protocol, and Table 2 describes characteristics of healthy athletes who participated in repeat testing and those who sustained a concussion.
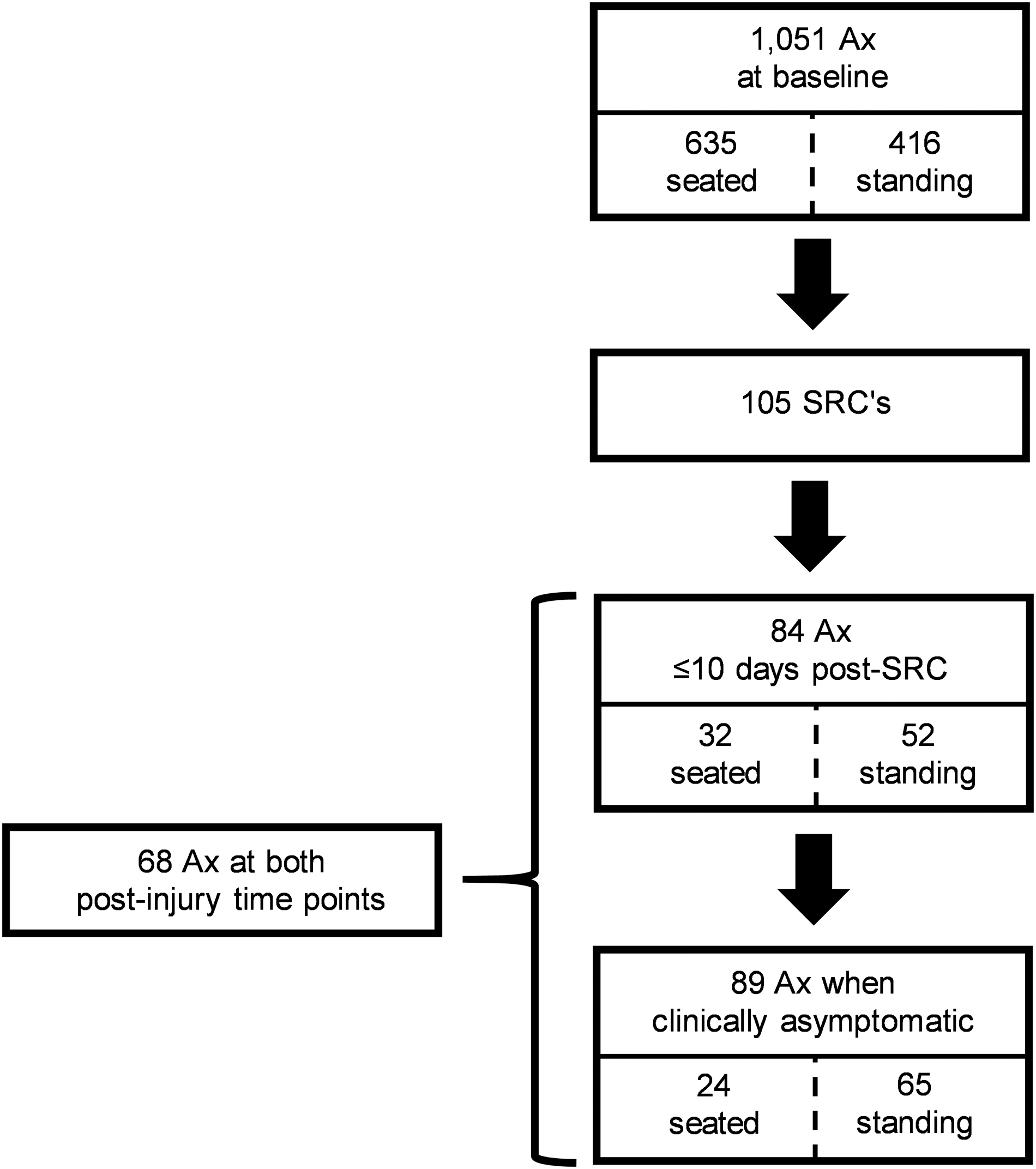
Flow chart depicting the number of athletes assessed at each study time point. One hundred fourteen concussions were sustained over the study period, but nine of those were recurrent concussions in athletes who had already sustained a concussion during the study period. These recurrent concussions were not included in the analyses. Sixteen individuals with SRC were assessed ≤10 days post-SRC, but did not return for reassessment when otherwise clinically asymptomatic. In 21 individuals, we were not able to conduct an assessment before symptom resolution (e.g., SRC sustained during nonlocal training or competition). Ax, assessment; SRC, sport-related concussion.
Characteristics of Athletes Who Completed Repeat Testing in a Healthy, Uninjured State and Athletes Who Sustained Concussions
Data are reported as mean ± standard deviation.
The approximate date of the last concussion was reported in only 24 of the 49 healthy athletes with a history of concussion.
The approximate date of the last concussion was reported in 52 of 67 concussed athletes with a previous history of concussion.
SRC, sport-related concussion; Ax, assessment; M, male; F, female; R, right; L, left; PC, post-concussion; CA, clinically asymptomatic; SCAT, Sport Concussion Assessment Tool; PCSS, post-concussion, symptom severity; Y, yes; N, no; n/a, not applicable.
Comparisons within the healthy athletes and reliable change index conversion
When comparing distributions of change in performance for all testing time points for each parameter in healthy athletes, Kolmogorov–Smirnov Z tests yielded significant differences (p < 0.05) between: male and female participants for 15 of 147 comparisons (10.2%), participants with and without a history of concussion for 6 of 147 comparisons (4.1%), seated and standing postures for 9 of 147 comparisons (6.1%), and testing time frames for 10 of 147 comparisons (6.8%). In the healthy athletes with a history of concussion for whom the approximate time since their last SRC was available (n = 24 of 49), Spearman's correlation analyses yielded significant (p < 0.05) relationships between self-reported time since previous concussion and change in performance in 7 of 147 variables (4.8%). All statistically significant findings detected with these tests are reported in Supplementary Table 2. (see online supplementary material at
Robotic Task Parameters with Significant Chi-Square Association (p < 0.05) between Concussion and Impairment at the Acute Post-Concussion (a) and Clinically Asymptomatic (b) Time Points
VGR, Visually Guided Reaching; RT, reaction time; IDR, initial distance ratio; TH, total hits; HND, hits nondominant; HSND, hand speed nondominant; PS, posture speed.
Impairment status in healthy and concussed athletes
Figure 3 shows box-and-whisker plots of the number of parameter impairments identified in healthy versus concussed participants at the acute post-concussion and clinically asymptomatic assessments for each task. At the group level, Mann–Whitney U tests indicated that the median number of parameters failed was significantly greater for athletes at the acute post-concussion time point than for healthy athletes in the VGR task (U = 606.5, Z = −2.28; p = 0.02) and TMB task (U = 3454.5, Z = −2.41; p = 0.02) and showed a trend for the same effect in the OH task (U = 3634.5, Z = −1.88; p = 0.06). In contrast, there was no difference in number of impairments between healthy controls and athletes at the acute post-concussion time point for the PM task (U = 4369, Z = −0.143; p = 0.89) and OHA task (U = 4159, Z = −0.118; p = 0.91; Fig. 3A). At the clinically asymptomatic time point, there were no differences in the median number of impairments identified between healthy and concussed athletes for any task (p ≥ 0.51; Fig. 3B).
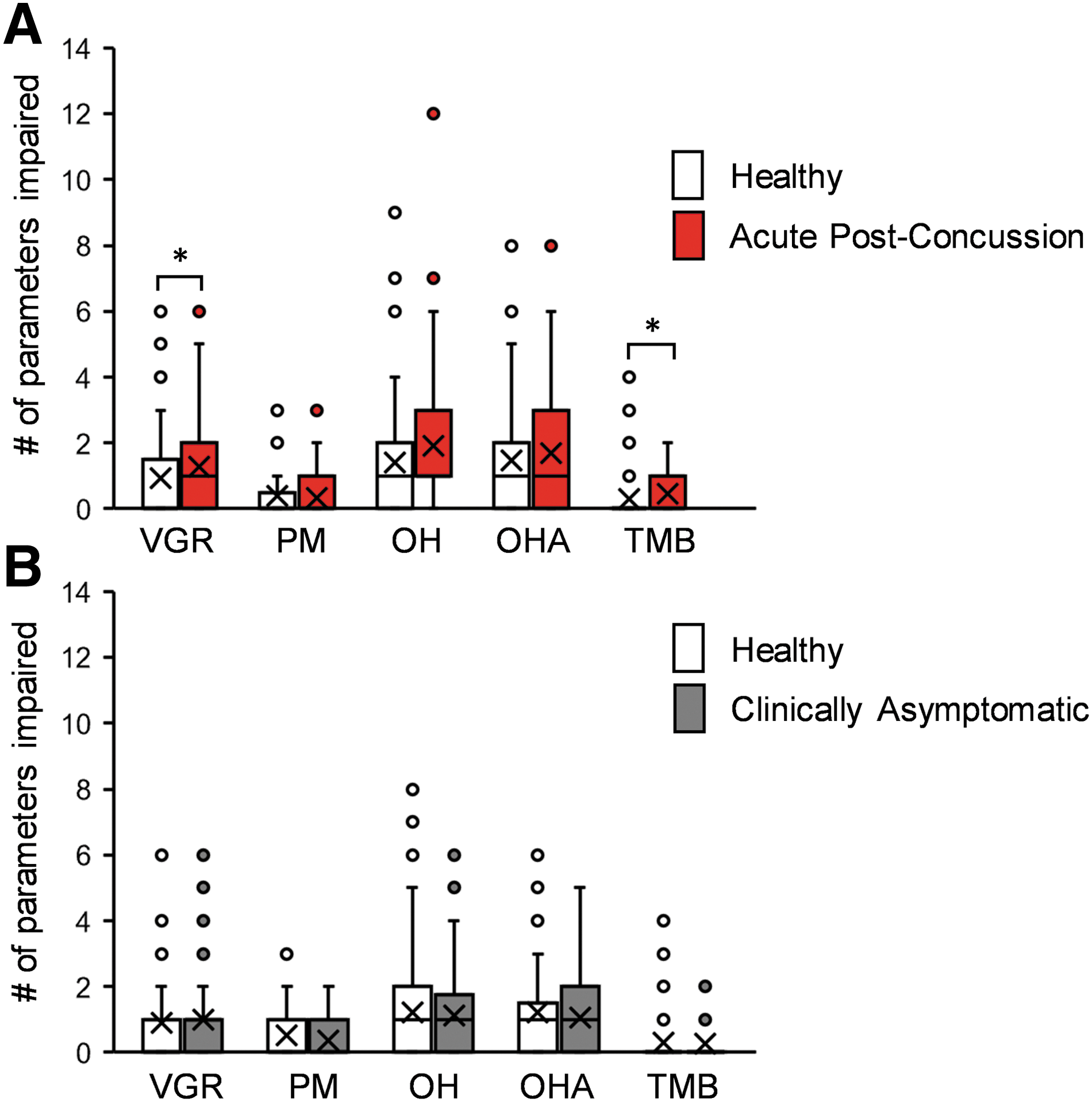
Number of parameters identified as impaired in healthy and concussed athletes. Healthy athletes' change in performance between a first and second assessment and between a first and third assessment was compared against concussed athletes' performance change between baseline and acute post-concussion, and baseline and clinically asymptomatic assessments. The number of parameters varies between tasks, such that VGR is scored out of a total of nine parameters, PM out of four, OH out of 14, OHA out of 14, and TMB out of three. Boxes represent the range between the first and third quartile. Medians are represented by horizontal lines within a box and means by “ × ” symbols. When a median is not depicted, it is overlapping with the lower quartile, with the exception of the clinically asymptomatic (gray box) VGR data, where it overlaps with the upper quartile. Whiskers extend to the 5th and 95th percentile. Circles represent single data points falling outside of the 5th and 95th percentile. Asterisks indicate significant differences (p < 0.05) between healthy and concussed athletes in the number of parameters identified as impaired. VGR, Visually Guided Reaching; PM, Position Matching; OH, Object Hit; OHA, Object Hit and Avoid; TMB, Trail Making B. Color image is available online at
Figure 4 depicts the proportion of participants with concussion classified as impaired based on the RCI cutoffs for each robotic parameter and task score. Parameters with statistically significant associations between sustaining a concussion and identification as impaired at the post-concussion and clinically asymptomatic time points are shown in Table 3. Significant associations were identified at the acute post-concussion time point for the following parameters: VGR task-Reaction Time (χ2 (1) = 5.09, p = 0.02, Cramer's V = 0.164); Initial Distance Ratio (χ2 (1) = 4.73, p = 0.03, Cramer's V = 0.158); PM task–ShiftXY (χ2 (1) = 6.97, p = 0.01, Cramer's V = 0.192); OH task–Total Hits (χ2 (1) = 8.47, p = 0.004, Cramer's V = 0.213); Hits with Non-Dominant Hand (χ2 (1) = 8.14, p = 0.004, Cramer's V = 0.209); and Non-Dominant Hand Speed (χ2 (1) = 9.01, p = 0.003, Cramer's V = 0.220). At the clinically asymptomatic assessment, a greater proportion of impairment in the concussion group relative to healthy athletes was found only for the VGR task Posture Speed parameter (χ2 (1) = 4.66, p = 0.03, Cramer's V = 0.166). There were no other parameters at either assessment for which sustaining a concussion and identification as impaired were associated (p ≥ 0.058, Cramer's V ≤ 0.146).
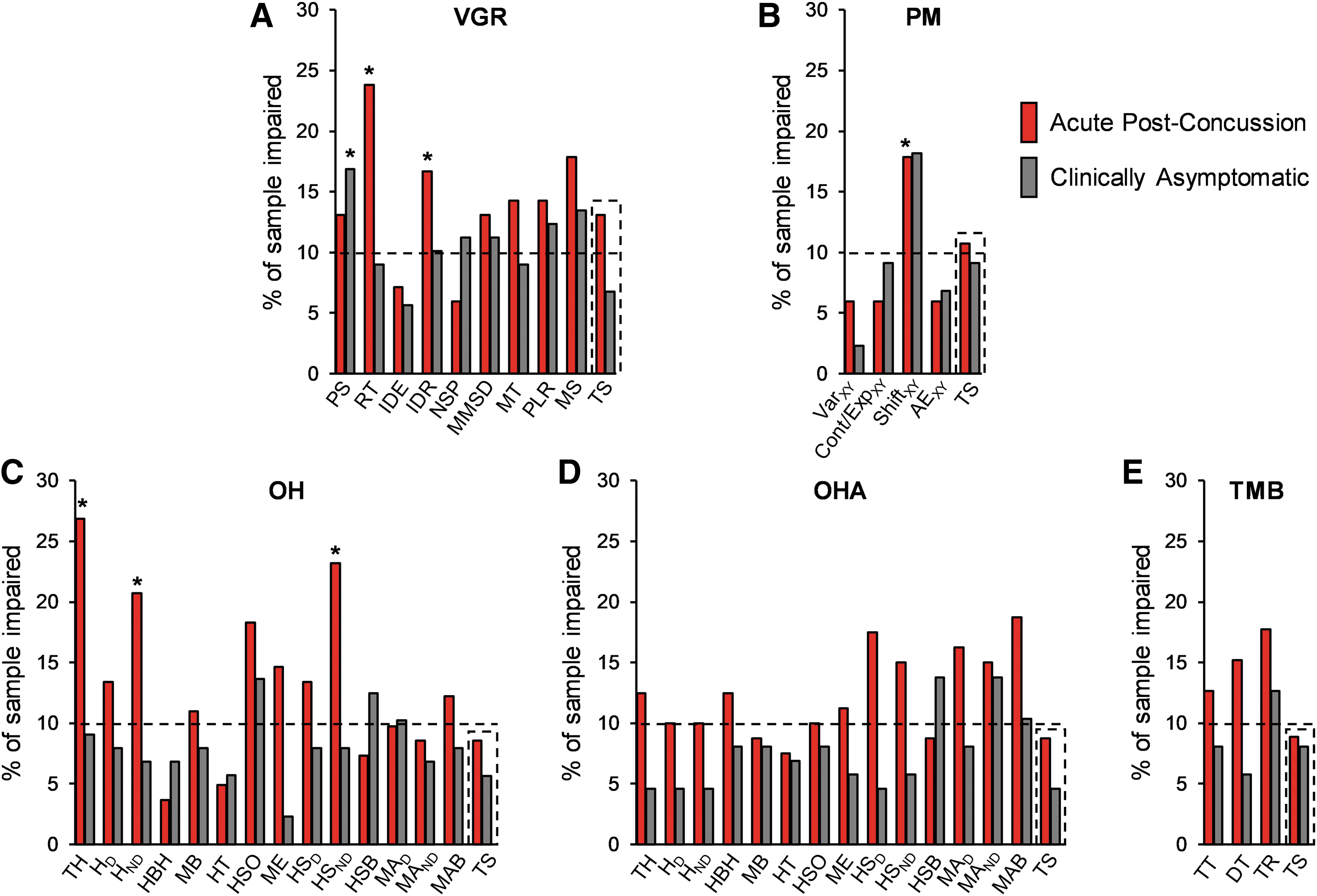
Percentage of sample identified as impaired on each parameter for each robotic task at the acute post-concussion and clinically asymptomatic time points. Asterisks identify parameters for which impairment was associated with concussion at the indicated assessment time point (p < 0.05). The horizontal dotted line indicates the percentage of the sample expected to be identified as impaired by chance alone. The dashed line box in each panel surrounds the overall task score (TS) for each task. RCI, Reliable change indices; PS, Posture Speed; RT, Reaction Time; IDE, Initial Direction Error; IDR, Initial Distance Ratio; NSP, Number of Speed Peaks; MMSD, Minimum Maximum Speed Difference; MT, Movement Time; PLR, Path Length Ratio; MS, Maximum Speed; VarXY, Variability XY; Cont/ExpXY, Contraction Expansion Ratio XY; ShiftXY, Shift XY; AEXY, Absolute Error XY; TH, Total Hits; HD, Hits Dominant; HND, Hits Non-Dominant; HBH, Hand Bias of Hits; MB, Miss Bias; HT, Hand Transition; HSO, Hand Selection Overlap; ME, Median Error; HSD, Hand Speed Dominant; HSND, Hand Speed Non-Dominant; HSB, Hand Speed Bias; MAD, Movement Area Dominant; MAND, Movement Area Non-Dominant; MAB, Movement Area Bias; TT, Test Time; DT, Dwell time; TR, Time Ratio; TS, Task Score; VGR, Visually Guided Reaching; PM, Position Matching; OH, Object Hit; OHA, Object Hit and Avoid; TMB, Trail Making B. Color image is available online at
Relationships to clinical variables
Additional chi-square tests were conducted on those parameters for which concussion was associated with impairment to evaluate associations between impairment and clinical variables. Impairment on VGR Reaction Time (χ2 (2) = 6.91, p = 0.03, Cramer's V = 0.294) and OH Total Hits (χ2 (2) = 6.72, p = 0.04, Cramer's V = 0.293) at the acute post-concussion time point were associated with acute SCAT PCSS category, where higher rates of impairment were found among individuals with greater symptom severity (Table 4). There was a trend for an association between OH Non-dominant Hand Speed and acute SCAT PCSS category (χ2 (2) = 5.35, p = 0.07, Cramer's V = 0.262). All other associations between impairments on robotic measures and clinical variables were non-significant (p ≥ 0.12, Cramer's V ≤ 0.344).
Relationship between SCAT PCSS Category and Proportion of Athletes Impaired at the Acute Post-Concussion Time Point for Parameters on Which Impairment Was Significantly Associated with Symptom Severity (Visually Guided Reaching-Reaction Time and Object Hit-Total Hits)
Sport Concussion Assessment Tool (SCAT) Post-Concussion Symptom Score (PCSS) was broken into categories from low- to high-severity scores (0, 0–5; 1, 6–22; 2, 23–88; 3, 89–132).
VGR, Visually Guided Reaching; RT, reaction time; PCSS, Post-Concussion Symptom Severity; OH, Object Hit; TH, Total Hits.
We detected some weak correlations when evaluating relationships between various demographic, clinical, and KINARM variables (Fig. 5A–C). Total acute SCAT PCSS score was correlated with the VGR Reaction Time RCI values (rs = 0.37, p = 0.001) and the OH Total Hits RCI values (rs = 0.32, p = 0.01) for the acute post-concussion test. There was also a trend for a correlation between total acute SCAT PCSS score and the days until clinically asymptomatic (rs = 0.23, p = 0.06). All other correlations evaluated were non-significant (rs ≤ |0.19|, p ≥ 0.22).
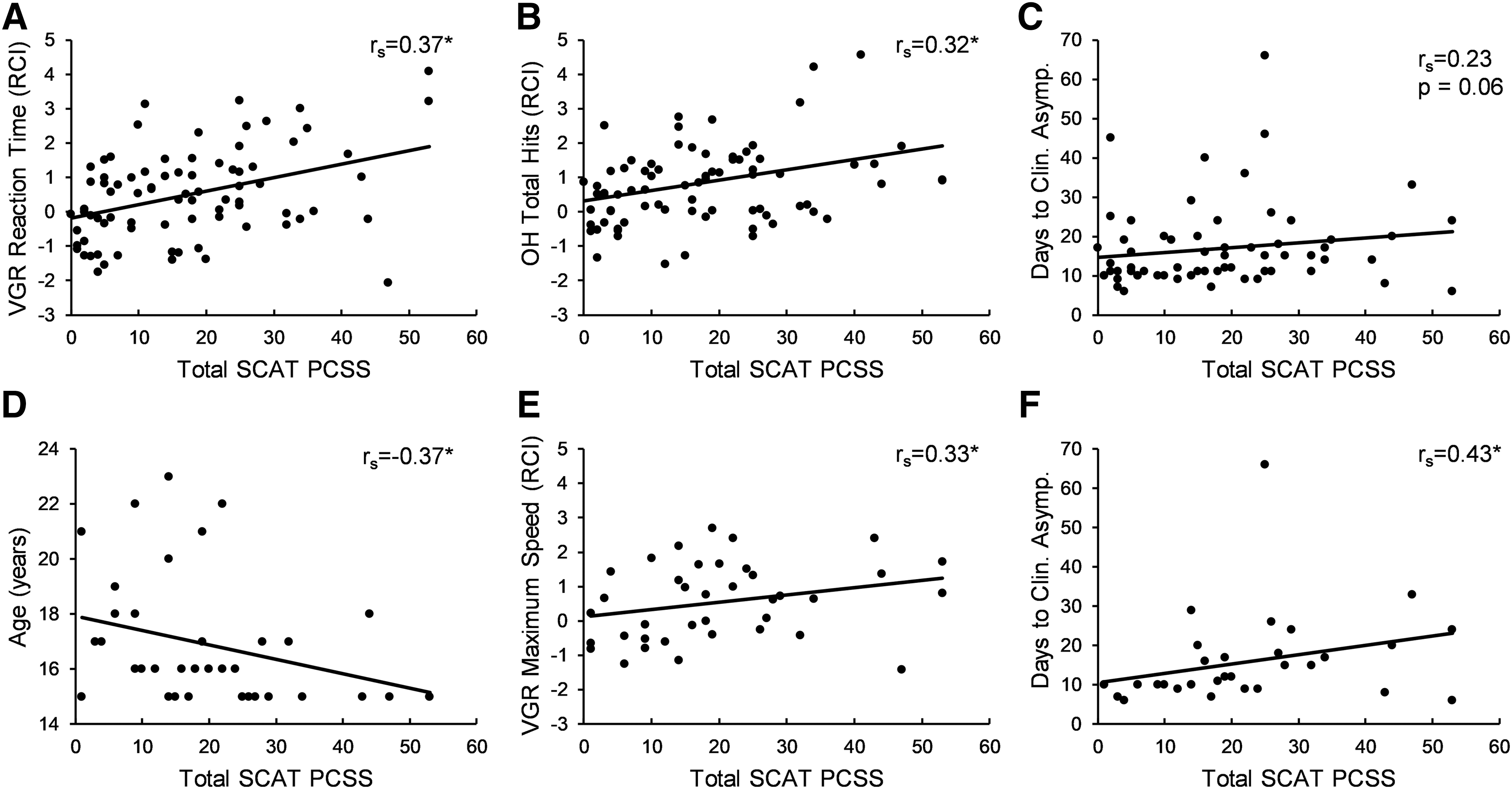
Significant and trending relationships between acute total SCAT PCSS score and other variables. (
Time frame of reassessment after sport-related concussion
Mann–Whitney U tests indicated that the median number of parameters identified as impaired at the acute post-SRC time point was not significantly different for any task when comparing individuals reassessed ≤3 days post-concussion with those assessed at 4–10 days post-concussion (p ≥ 0.29). However, chi-square tests indicated that a higher proportion of concussed athletes tested ≤3 days post-injury were identified as impaired than those tested 4–10 days post-injury on the VGR task Maximum Speed parameter (30.0% and 6.8%, respectively; χ2 (1) = 7.68, p = 0.01, Cramer's V = 0.302) and the OHA task Movement Area Bias parameter (27.5% and 7.7%, respectively; χ2 (1) = 5.31, p = 0.02, Cramer's V = 0.259). All other comparisons of parameter impairment rates between these groups were non-significant (χ2 (1) ≤ 3.80, p ≥ 0.05, Cramer's V ≤ 0.217). Additional chi-square tests examining associations between impairment on these parameters with clinical variables (acute SCAT PCSS category, history of concussion, and history of migraines) in the athletes tested ≤3 days post-concussion were non-significant (p ≥ 0.09, Cramer's V ≤ 0.276). However, Spearman correlations conducted in this participant subgroup indicated significant relationships between the acute SCAT PCSS score and: age (rs = −0.37, p = 0.02), the post-concussion RCI value for the VGR task Maximum Speed parameter (rs = 0.33, p = 0.04), and the number of days until clinically asymptomatic (rs = 0.43, p = 0.01). These relationships are depicted in Figure 5D–F. All other Spearman correlation tests were non-significant (rs ≤ |0.21|, p ≥ 0.20).
Discussion
In the present study, we derived and applied RCI cut-off values for a subset of KINARM standard task parameters to quantify motor, sensory, and cognitive performance in athletes with SRC. We observed a generally higher rate of impairment in acutely concussed (≤10 days) athletes than in healthy athletes; however, the rates of impairment after concussion were lower than expected based on previous KINARM studies of non-sport-related TBI. 12,13,18 Acute symptom severity was related to performance on two KINARM task parameters (VGR Reaction Time, OH Total Hits), and the acuteness of our reassessment (≤3 vs. 4–10 days) appeared to only slightly influence the observed patterns of impairment. As a group, KINARM task impairments were largely resolved at the clinically asymptomatic assessment time point.
Development of reliable change indices
We developed RCIs to allow for identification of individual impairments based on change in KINARM task performance from baseline to post-concussion, consistent with previous work studying cognition
33
–35
and balance
24
in SRC. Accounting for individuals' pre-injury level of function may be particularly useful in this clinical population, given that it should allow for increased detection of subtle deficits in athletes with unique physical and cognitive skillsets. Along these lines, previous work suggests that comparing cognitive performance after concussion to single test norms tends to underclassify impairments in individuals with above-average performance.
42
Thus, the RCI cut-off values reported in the supplementary information(see online supplementary material at
KINARM impairments identified in acute sport-related concussion
Visually Guided Reaching Task
In the VGR task, athletes with acute SRC were impaired on more parameters than healthy athletes. Also, a higher proportion of acutely concussed athletes compared to healthy athletes were impaired in the Reaction Time (RT) and Initial Distance Ratio (IDR) parameters. RT provides information about the processing time associated with initiating a movement, whereas IDR provides information about the initial, feed-forward movement that was generated as a result of that processing. Other work using the KINARM in study samples with a range of non-sport-related TBI severities also noted deficits in RT and measures of feed-forward control in the VGR task. 13,18 However, these previous studies concomitantly described high impairment rates in measures of feedback control and global aspects of reaching. 13,18 Thus, the current results are partly consistent with past findings in TBI, but suggest that acute SRC deficits may be less commonly reflected in VGR measures of feedback control and global reaching performance than other forms of TBI.
Position Matching Task
As a group, athletes with acute concussion did not demonstrate impairments on more PM parameters than healthy individuals. However, a higher proportion of acutely concussed athletes compared to heathy athletes were impaired on the PM task ShiftXY parameter, which quantifies a general shift in an individual's sense of their limb position. Little previous work has reported on specific PM parameter impairments in mild TBI, but interestingly the only participant with mild TBI in the study by Debert and colleagues also presented with a specific impairment in the ShiftXY parameter. 13 In contrast, participants with moderate-to-severe TBI were impaired on multiple PM task parameters. 13
Object Hit Task
There was a trend for athletes with acute SRC to be impaired on more OH parameters than healthy athletes. The OH task also yielded the highest rates of impairment in individual parameters compared to other tasks in our study. For example, OH Total Hits had the highest impairment rate (26.8%) of all KINARM parameters currently tested. The relatively high OH impairment rates are consistent with Logan and colleagues' 18 work in non-sport-related TBI and may reflect both the high motor demands required by the task and its reliance on bimanual coordination. For instance, neuroimaging studies in individuals with concussion demonstrated damaged white matter structure within the corpus callosum, 43 a brain region critical to such bimanual coordination. Notably, our results in acute SRC indicated higher rates of impairment in the non-dominant than the dominant hand. Whereas Logan and colleagues 18 reported similar OH impairment rates between hands in non-sport-related TBI, the degree of impairment appeared generally worse in the non-dominant versus dominant hand (cf. Fig. 4). Thus, TBI may more robustly impact OH performance involving the non-dominant versus dominant hand, possibly as a result of the higher challenge associated with motor control in the less-skilled non-dominant limb.
Object Hit and Avoid Task
Given that the OHA task is similar to OH but with added cognitive processing, we expected to find relatively high rates of impairment with it post-SRC. Nevertheless, there were no group differences in the number of impairments between healthy and post-SRC athletes, and impairments were not associated with having a concussion for any OHA parameters. Importantly, though, the overall motor demand in the OHA task is less than for OH because participants are only required to hit two of the objects and avoid the rest, rather than hit them all. Thus, the OHA task demands more cognitive processing (i.e., response inhibition), but substantially fewer rapid decisions on movement selection and execution, than the OH task. The divergence of impairment rates between these two tasks may then speak to which neurological domains are more commonly impacted specifically in acute SRC
Trail Making B Task
In the TMB task, concussed athletes showed impairment on a greater number of parameters than healthy individuals, but no specific parameter impairment was associated with having a concussion. Past work reported TMB deficits after concussion when considering overall test time, 44 and a study with the KINARM suggested that more than half of individuals with non-sport-related TBI demonstrated impairments on TMB task score. 18 Our findings suggest that impairments after acute SRC could be distributed across various aspects of TMB performance (e.g., Time Ratio, Dwell Time), but may not affect any specific parameter more commonly than another. These findings encourage delivery of the TMB test with methods that can quantify multiple aspects of performance, rather than pencil and paper tests that only consider global measures (e.g., total test time).
Clinical relationships
Presently, worse acute symptom severity was weakly associated with slowed RT on the VGR task and reduced Total Hits during the OH task post-SRC, but no other relationships between symptoms and KINARM performance were observed. The lack of stronger relationships suggests that the symptom reporting and KINARM assessment approaches are largely measuring different constructs. Past work reported multiple relationships between traditional clinical assessments and KINARM performance in non-sport-related TBI when the neurological domains tested were overlapping (e.g., Montreal Cognitive Assessment scores correlated with OHA and TMB task performance). 18 However, the PCSS used to measure symptom severity here is a composite measure of multiple symptoms, whereas the KINARM task measurements are highly domain specific. Thus, it is possible that a composite “neurological score” derived from consideration of performance across multiple KINARM tasks would be more likely to relate to symptom reports, but a valid method to create this has not yet been developed.
In acute (≤24 h) mild non-sport-related TBI presenting to the emergency department, performance on the same KINARM standard task battery used here was predictive of persistent symptoms (3 weeks post-injury). In contrast, we detected no relationships between KINARM task performance within 10 days of sustaining an SRC and the number of days until athletes were considered clinically asymptomatic. Although various methodological differences could contribute, the disparate findings are most simply explained by the difference in the time frame of the KINARM testing between studies. Neurological assessments conducted within the first 24 h compared to 10 days post-injury likely provide very different information. Further, it is plausible that the individuals with mild TBI in the previous work who presented to the emergency department on their own accord 45 may have sustained relatively more-severe TBIs compared to the athletes with suspected SRC in the current study who were referred to a sports medicine clinic by a team therapist.
Time frame of reassessment after sport-related concussion
Past work found diminishing effects of SRC on cognitive performance from 24 h to 8 days to 15 days post-injury. 45 Given the relatively large window of time in which our post-concussion assessment was conducted, we used secondary analyses to determine whether findings might differ based on the time frame of reassessment post-SRC. Individuals assessed ≤3 days post-injury showed higher impairment rates than those assessed 4–10 days post-SRC for the VGR Maximum Speed (i.e., maximum speed of the hand movement) and OHA Movement Area Bias (i.e., ratio of area occupied by the dominant and non-dominant hands) parameters. Impairments on these parameters were also detected at high rates in non-sport-related TBI. 13,18 In acute SRC, it is possible that these parameters are commonly impaired early post-injury, but resolve more quickly than other types of impairment (e.g., VGR RT).
Within the subgroup of athletes who were assessed ≤3 days post-injury, lower age was associated with higher acute symptom severity score (SCAT PCSS). Additionally, the relationship between symptom severity and the number of days until clinically asymptomatic was stronger in this subgroup than for the entire sample. Detection of these relationships in this particular subgroup may be connected to evidence that different types of symptoms predominate at different stages of recovery. 46 For example, physical symptoms (e.g., headache) are more common initially post-injury, with emotional symptoms (e.g., irritability) often developing later on. 46 Thus, symptoms contributing to the PCSS ≤3 days post-injury may be more tightly correlated with age and recovery time than others.
KINARM assessment when clinically asymptomatic following sport-related concussion
There were no differences between healthy and clinically asymptomatic athletes in the number of parameter impairments identified on each task. Likewise, at the clinically asymptomatic time point, impairment rate for only one parameter (VGR Posture Speed) was higher for concussed relative to healthy athletes. Posture Speed quantifies the mean hand speed when the hand should be at rest in a target, providing information about upper-limb postural control. In subacute non-sport-related TBI (average 56 ± 50 days post-injury), a similar impairment rate was detected for VGR Posture Speed (17.4% vs. 16.9% here). Yet, given the lower Posture Speed impairment rate acutely post-SRC and the lack of other significant findings at the clinically asymptomatic time point, further work is needed before its potential meaning can be elucidated. Overall, our results suggested that KINARM performance was largely normalized when individuals were clinically asymptomatic post-SRC and is in line with previous work indicating negligible impairment in KINARM standard tasks in asymptomatic pediatric athletes with a remote history of SRC. 17
Low KINARM standard task impairment rates in sport-related concussion
Studies of participants with mild non-sport-related TBI 12,18 have yielded markedly higher impairment rates than those observed in the current study of SRC. For example, the median proportion of parameters that were considered impaired in a study of acute (≤24 h) mild TBI presenting to the emergency department was more than double our current findings for the VGR, PM, OH, and TMB tasks. 12 As mentioned previously, a key difference contributing to contrasting results between our current study and this previous work is the time to assessment (≤24 h vs. ≤10 days). Nevertheless, it seems that deficits in neurological function post-SRC are often particularly subtle, and identification of such deficits remains a challenge in the field. Many factors could contribute to this challenge, such as intraindividual variability driven by changes in training state (i.e., pre-season to peak-season) and cases of malingering in the athlete population. Likewise, test-retest reliability of KINARM task parameters in healthy athletes 5,6 are slightly lower than for other populations. 7 –10 On the other hand, given that the KINARM has proven proficient in identifying deficits in other neurological conditions associated with subtle impairments (e.g., transient ischemic attack 40 ), it must also be considered that many individuals with suspected SRC may simply not have upper-extremity motor, sensory, and cognitive deficits and possibly no neurological injury at all. For instance, many symptoms evaluated on the SCAT (e.g., neck pain, balance problems, and irritability) could be explained by a musculoskeletal or vestibular injury, or psychological distress.
Limitations
The methodological approaches taken in the current study were chosen to maximize sample sizes for the healthy control group from which we derived RCIs and the SRC group. However, this approach also introduced limitations: 1) We collapsed data across sex, history of concussion, assessment posture, and testing time frame. Although there were minimal differences in KINARM performance across these variables, an ideal approach would involve determination of specific RCIs for each variation. Specifically regarding assessment posture, the proportion of participants tested while seated and standing was quite different between healthy controls and concussed athletes (see Table 2), and further study of the potential impact of testing posture on KINARM performance is merited; 2) There are not yet sufficient data to create normative models of KINARM performance specific to young athletes; by ascribing 18-year-old athlete z-scores to 15- to 17-year-old athletes, age effects were not fully accounted for in these participants; 3) Athletes underwent varying numbers of baseline assessments before their acute post-concussion assessment. Practice effects and reliability coefficients were applied to RCI calculations accordingly (see Supplementary File); (see online supplementary material at
Another limitation relates to the 5 individuals at the acute post-concussion assessment and 2 individuals at the clinically asymptomatic assessment who could not complete the KINARM test battery because of exacerbation or reoccurrence of symptoms. These athletes' impairments were not illustrated in the quantifiable results, and the clinical importance of the symptoms experienced must be acknowledged.
Future directions
Whereas the current set of KINARM standard tasks appears useful for assessment across varying stages of recovery after non-sport-related TBI, 12,13,18 refinement of KINARM assessments will be necessary to achieve appropriate sensitivity for detection of the subtle impairments common to SRC. Some improvement could be achieved through relatively simple modifications, such as by focusing on non-dominant limb performance, as suggested by the higher levels of impairment in the non-dominant limb during the OH task observed here. Other approaches may involve assessment of more-complex neurological functions, such as visuomotor rotations 49 or sensorimotor learning. Integration of additional technology (e.g., gaze tracking, force plates) could also allow evaluation of performance on tasks that utilize multiple neurologic systems concurrently. Yet, given that some participants were unable to complete the current KINARM test battery, it may be necessary to develop alternate KINARM protocols based on individual symptom burden and recovery stage. Past work has considered the potential of developing a hierarchical KINARM task order for assessment after stroke. 50 A similar approach could plausibly be developed that is specific to SRC, where athletes proceed through different KINARM tasks based on their symptoms, time post-injury, and level of performance on each task.
An ultimate aim of this line of study is to develop robotic assessments of neurological function that are useful for both diagnosis of SRC and monitoring of recovery over time. Size and expense of the KINARM are limiting factors for its implementation for sideline diagnostic testing. However, given that a previous feasibility study reported that the KINARM could be integrated into an emergency department, 51 its addition to athlete dressing rooms or central athletic facilities may be plausible in some cases. Alternatively, if a KINARM task is found to be particularly useful in SRC assessment, a modified version could potentially be developed with some other technological means that is more conducive to sideline testing (e.g., OH task on a tablet). A more pragmatic use of the KINARM for SRC may be in tracking recovery in a sport medicine clinical setting to inform return-to-play and return-to-learn judgements. However, given the generally low impairment rates at the clinically asymptomatic time point in the current study, the utility of the KINARM or other robotic technology to this end will be dependent on whether more sensitive assessments can be developed.
Conclusions
This study contributes toward the development of improved assessments of SRC. The results indicate that robotic tools can provide an efficient means of obtaining objective, quantitative information about motor, sensory, and cognitive function in this group. Nevertheless, the low impairment levels detected with the KINARM tasks used presently highlight the challenge of objectively quantifying neurological impairments in SRC at the individual level, and the potential need to design robotic tasks that assess more-complex abilities.
Footnotes
Acknowledgments
The authors acknowledge the participating athletes, coaches, and team therapists.
Author Disclosure Statement
This work was funded by Own the Podium Canada, the Canadian Academy of Sport and Exercise Medicine Research Fund, the Canadian Sport Institute Calgary, and Jim Smith of Calgary, Alberta. C.S.M. was funded by post-doctoral fellowships from the Canadian Institutes of Health Research and Alberta Innovates Health Solutions. T.A.W. was funded by a Mitacs fellowship in partnership with Own the Podium Canada. S.H.S. is cofounder and chief scientific officer of BKIN Technologies, Ltd., the company that commercializes the KINARM device used in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.