
Abstract
Civilian firearm injury is an important public health concern in the United States. Gunshot wounds to the head (GSWH) remain in need of update and systematic characterization. We identify predictors of prolonged hospital length of stay (HLOS), intensive care unit length of stay (ICU LOS), medical complications, mortality, and discharge disposition from a population-based sample using the National Sample Program (NSP) of the National Trauma Data Bank (NTDB), years 2003–2012. Statistical significance was assessed at α < 0.001 to correct for multiple comparisons. In total, 8148 adult GSWH patients were included extrapolating to 32,439 national incidents. Age was 36.6 ± 16.4 years and 64.4% were severe traumatic brain injury (TBI; Glasgow Coma Scale [GCS] score 3–8). Assault (49.2%), handgun (50.3%), and residential injury (43.2%) were of highest incidence. HLOS and ICU LOS were 7.7 ± 14.2 and 5.7 ± 13.4 days, respectively. Overall mortality was 54.6%; suicide/self-injury was associated with the highest mortality rate (71.6%). GCS, Injury Severity Score, and hypotension were significant predictors for outcomes overall. Medicare/Medicaid patients had longer HLOS compared to private/commercial insured (mean increase, 4.4 days; 95% confidence interval [2.6–6.3]). Compared to the Midwest, the South had longer HLOS (mean increase, 3.7 days; [2.0–5.4]) and higher odds of complications (odds ratio [OR], 1.7 [1.4–2.0]); the West had lower odds of complications (OR, 0.6; [0.5–0.7]). Versus handgun, shotgun (OR, 0.3; [0.2–0.4]) and hunting rifle (OR, 0.5; [0.4–0.8]) resulted in lower mortality. Patients with government/other insurance had higher odds of discharging home compared to private/commercially insured (OR, 1.7; [1.3–2.3]). In comparison to level I trauma centers, level II trauma centers had lower odds of discharge to home (OR, 0.7; [0.5–0.8]). Our results support hypotension, injury severity, injury intent, firearm type, and U.S. geographical location as important prognostic variables in firearm-related TBI. Improved understanding of civilian GSWH is critical to promoting increased awareness of firearm injuries as a public health concern and reducing its debilitating injury burden to patients, families, and healthcare systems.
Introduction
Traumatic brain injury (TBI) is a major cause of public health and socioeconomic burden, with estimates by the U.S. Centers for Disease Control and Prevention at 2.5 million annual emergency department (ED) visits and 52,000 deaths. 1,2 Penetrating brain injury (PBI) accounts for 1.5% of TBI incidents and is the most lethal (42% of TBI deaths), in part because the majority of civilian cases are from high-velocity projectiles, for example, gunshot wounds to the head (GSWH). 3,4 Because of the highly destructive nature of ballistics to brain tissue, past studies on GSWH report the exceedingly high early-mortality rate of 71% on scene as well as an overall mortality rate of 88%. Roughly 97% of GSWH patients experience unfavorable outcome at hospital discharge (Glasgow Outcome Scale [GOS] = dead [GOS = 1], vegetative [GOS = 2], or severe disability [GOS = 3]). 5 –9
For patients who survive long enough to receive medical management, GSWH is a complex challenge and there is little literature describing the natural history of these injuries in a modern medical setting. Past investigations have suffered from small sample sizes, nonstandardized treatment algorithms, and incomplete data. As a result, there is a lack of robust substantiation for improved mortality subsequent to publication of the 2001 Guidelines for the Management of Penetrating Brain Injury. 10 To date, more civilians have died from gun violence since World War II than were casualties of the Korean and Vietnam conflicts combined, 8 yet the current body of research on PBI is mostly noncivilian. Put succinctly, the standardized guidelines include immediate restoration of circulating volume, blood pressure, oxygenation, and ventilation, aggressive antibiotic and seizure prophylaxis, and less-aggressive surgical debridement for deep-seated fragments. 11,12 Although these guidelines are widely utilized, overall patient outcomes have not been corroborated by large-scale studies. Given these factors and the increased scrutiny by the media on gun violence, an accurate characterization of GSWH on a national scale is critical.
Critical differences in setting, risk factors, and prognosis exist between the civilian and noncivilian GSWH. Civilian GSWH is typically caused by subsonic bullets, whereas noncivilian GSWH is largely a result of supersonic, military-grade bullets which transmit significantly more energy to brain tissue. As a result, noncivilian GSWH is most often fatal. The noncivilian PBI literature also has a high proportion of shell and shrapnel injuries, which are generally of lower velocity and irregularly shaped, thus imparting less kinetic energy and damage to brain tissue. This difference explains why, despite an average injury-to-hospital time of less than 45 min in the civilian setting, shell and shrapnel PBI common in the military arena has mortality rates of 10–30%, even with longer mean evacuation time of 2.3 h from battlefield to medical care. 13 –15 The impact of the weapon caliber in the civilian GSWH population remains to be analyzed to determine the significance of ballistics on functional outcome.
Predictors of outcome in civilian GSWH have been an important, and timely, topic of recent research. Consensus on outcome determinants includes age, hypotension, suicide attempt, bullet trajectory, and lesions on brain computed tomography (CT) scan, Glasgow Coma Scale (GCS) score at admission, and abnormal pupillary response. 12,16,17 Other regional reports have found localized firearm-related injury patterns driven by market trends for pistols, semiautomatic weapons, and other forms of handguns. 18 –20 These fluctuations may be specific to demographics, socioeconomic status, and geographical region. To our knowledge, no standardized reports have characterized the details of civilian GSWH on a national scale to account for shifting demographics, inter-regional discrepancies, and evolving firearm technology. Epidemiological surveillance of firearm-related injuries at the turn of the century demonstrated the healthcare burden from firearms, 21 –24 but the 10–11% of patients presenting with GSWH insofar have yet to be examined on the granular level in the firearm literature. Given the lack of standardized national reporting of patients presenting with GSWH, we provide an epidemiological update of U.S. firearm TBI over the past decade. We hypothesize that clinical assessment during triage, including hypotension and injury severity measures, along with the injury intention, type of firearm, and geographical region, may be associated with worse outcomes post-GSWH. The aim of this study is to provide an update of this subset of patients in the United States.
We use the National Sample Program (NSP) of the National Trauma Data Bank (NTDB), a prospective, curated trauma registry with the purpose of tracking and providing information about trauma care and outcomes. We performed a retrospective analysis of demographic data, risk factors, management strategies, complications, disposition, and mortality in the PBI population specifically wounded by firearms who were treated nonoperatively and operatively. It is our objective to update the epidemiology and clinical history of U.S. firearm TBI over the past decade, as well as prognosis and outcome to inform acute management of this critically injured population. Notably, we characterize our patient sample by firearm cohort and U.S. geographical locale, with implications on management and outcome.
Methods
In this study, we used the NSP of the NTDB from arrival years 2003–2012. The NSP for each year consists of a stratified sample of 100 NTDB participating hospitals based on U.S. Census region, trauma care designation, and NTDB reporting status. 25 Hospitals were drawn by the NTDB from the sampling universe of 453 level I or II trauma centers, and the sample size of 100 hospitals was determined by past review indicating it can be extrapolated to represent the national patient distribution. 26 Detailed data qualification, selection, cleaning, and standardization algorithms have been previously reported. 26 Because the NSP of the NTDB is a fully de-identified data set without the 18 federal Health Insurance Portability and Accountability Act (HIPAA) identifiers, the current study was classified as exempt from institutional review board review.
A total of 410,101 incidents sustaining TBI were extracted from NSP years 2003–2012 using the International Classification of Diseases, Ninth Revision (ICD-9) codes 800-801.99, 803-804.99, and 850-854.19 as previously described. 27 –29 Adult patients (variable name “age” ≥18; n = 355,388) with known penetrating TBI (ICD-9 codes E922.0-922.9, E955.0-955.4, E965.0-065.4, E970, and E985.0-985.3 [Table 1]) and sex (variable name “gender”; n = 8148) were extracted for analysis (Fig. 1). Patients with nonmissing data in our five targeted outcomes variables (mortality, inpatient medical and surgical complications, hospital length of stay [HLOS] of patients alive at discharge, intensive care unit length of stay [ICU LOS] of patients alive at discharge, and discharge destination were included in the final sample).

Flow chart identifying firearm-related TBI patients for analysis from the NSP of the NTDB, 2003–2012. NSP, National Sample Program; NTDB, National Trauma Data Bank; TBI, traumatic brain injury.
Summary of Extracted Firearm-Related ICD-9 E-Codes
ICD-9, International Classification of Diseases, Ninth Revision.
Demographic and clinical variables of interest were extracted for multi-variable analysis to include age, sex, race, health insurance status, medical history, U.S. geographical region, site of incident, intention of injury, type of firearm, isolated TBI, American College of Surgeons (ACS) trauma center designation, hypotension in the ED (systolic blood pressure [SBP] <90 mm Hg), GCS score, stratified Injury Severity Score (ISS), and ED disposition. The Charlson Comorbidity Index (CCI) was utilized as a summative score of overall comorbidity burden, calculated using the standard comorbidity weights as previously described in large, retrospective TBI studies. 30 –34 Demographic and clinical variables that were missing and/or marked as not known/not recorded from the NSP were coded as “unknown.”
Statistical analysis
Descriptive variables are presented using proportions for categorical variables and means and standard errors (SEs) for continuous variables. Group differences were assessed using Pearson's chi-squared test (X 2 ) for categorical variables and analysis of variance for continuous variables. For analyses with individual cell counts <5, Fisher's exact test was used in place of X 2 . Categorical outcome variables (e.g., mortality, complications, and discharge destination) were assessed using binary logistic regression. Continuous outcome variables (e.g., HLOS, ICU LOS) were assessed using linear regression. Multi-variable analyses were adjusted for demographic and clinical variables (age, sex, race, CCI score, health insurance status, U.S. geographical region, site of incident, intention of injury, type of firearm, isolated TBI, ACS trauma center designation, hypotension in the ED, GCS score, and ISS). Odds ratios (ORs) and associated 95% confidence intervals (CIs) were reported for logistic regressions, and mean differences (B), SEs, and 95% CI were reported for linear regressions. Statistical significance was assessed at α = 0.001. All analyses were performed using the Statistical Package for Social Sciences (SPSS; version 23; IBM Corporation, Chicago, IL).
Results
Demographics and clinical characteristics
From admission years 2003–2012, the NSP recorded 355,388 adult TBI incidents. Firearm-related injuries accounted for 8148 events (Table 2), which corresponded to 32,439 events in the U.S. population nationally, or roughly 2.2% of adult TBIs presenting to U.S. trauma centers. Incidence by year showed increased data following standardization of the trauma registry in 2008, with a stable trend in incidence over time since 2008 (Fig. 2). Patients were aged 36.6 ± 16.4 years of age, 86.5% male, and 52.9% Caucasian. Age 18–29 years (45.5%) was of greatest incidence, with few medical comorbidities as evidenced by a mean CCI score of 0.15 ± 0.59 (Table 2). Identifiable insurance statuses were self-pay/unbilled (31.3%), Medicare/Medicaid (15.2%), private/commercial (14.8%), and government/other (10.4%).

Left panel: the number of patient events included. Middle panel: proportions of patients with complications, discharge to home, and deaths. Right panel: the hospital LOS and ICU LOS of hospitalized patients alive at discharge (mean ± SE). *Year in which the National Trauma Data Standard was implemented. ICU, intensive care unit; LOS, length of stay; SE, standard error; TBI, traumatic brain injury. Color image is available online at
Demographic Data and Injury Characteristics of 8148 Adults With Firearm-Related TBI a
The age range of the patients was 18–89.
Data represent number of patients (%), unless indicated otherwise.
The range of the CCI score is 0–8.
TBI, traumatic brain injury; SD, standard deviation; M/F, male/female; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score; ICU, intensive care unit; OR, operating room.
Injury intentions were assault (49.2%), suicide/self-inflicted (41.9%), accident (3.5%), and legal intervention (1.7%). African Americans accounted for the greatest proportion of GSWH by assault mechanism (52.1%). Assault was the most common mechanism in age 18–49 years (57.3%); suicide/self-inflicted was most common in age ≥50 years (72.5%; Fig. 3). Handgun (50.3%) was more often the weapon of injury, and residential area was the most frequent scene of injury (43.2%). The majority of GSWH victims presented with additional trauma not limited to the head and face (69.0%). Median initial GCS score was 3 (interquartile range, [IQR], 3–14); mean GCS was 6.8 ± 5.8. Median ISS was 21 (IQR, 16–25); mean ISS was 20.7 ± 13.9. Most patients had severe TBI (GCS, <8; 64.4%), followed by mild TBI (GCS, 13–15; 28.1%) and moderate TBI (GCS, 9–12; 4.1%). Thirty-one percent of patients were hypotensive (SBP, <90 mm Hg). ED dispositions of highest incidence were ICU (49.6%), death (20.3%), and operating room (15.4%).
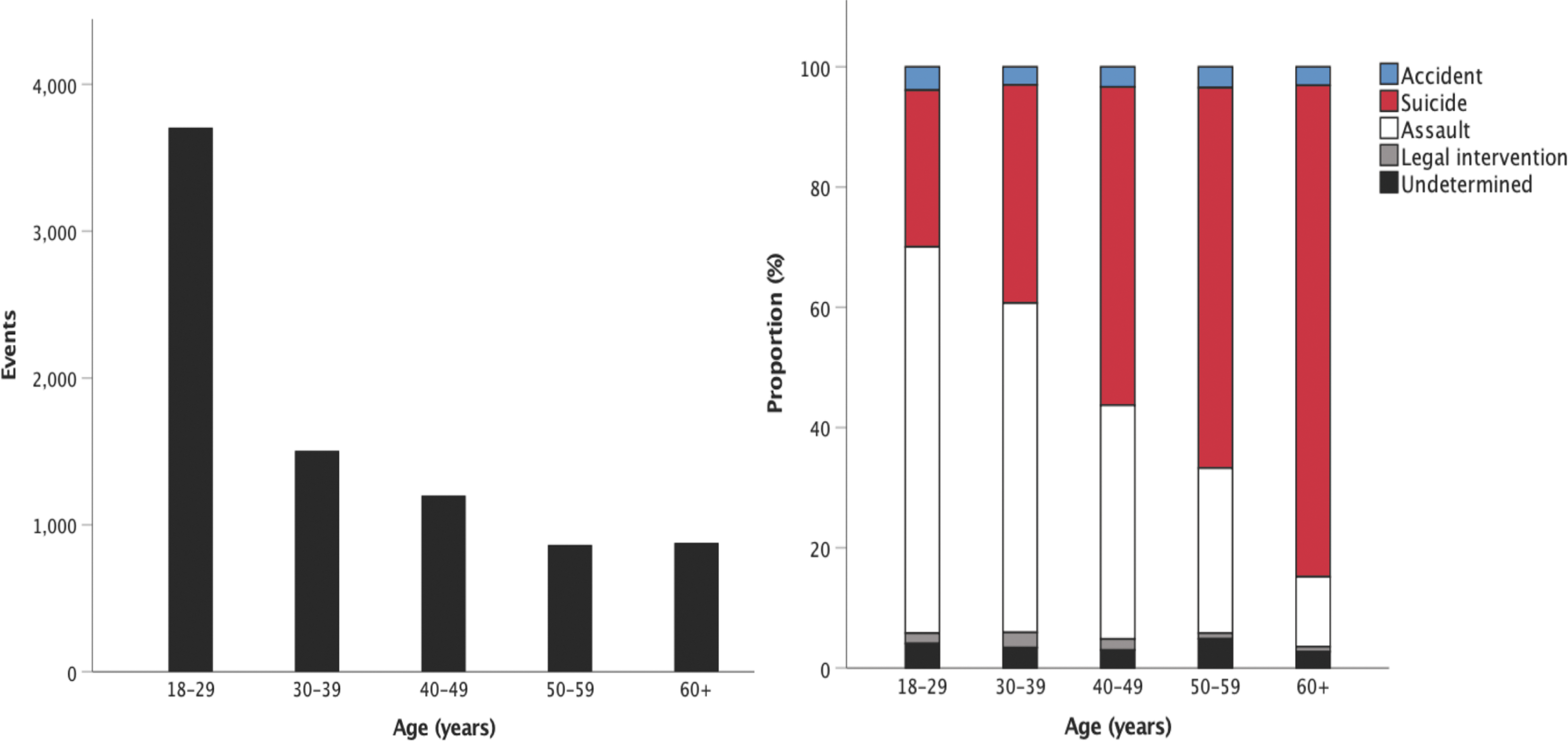
Left panel: the number of firearm-related TBI events in each adult age group. Right panel: proportions of firearm-related TBI attributed to accident, suicide/self-inflicted, assault, legal intervention, and undetermined intent in each age group. TBI, traumatic brain injury. Color image is available online at
Regional characteristics and trauma center level
Across U.S. regions, most injuries occurred in the South (39.5%), followed by West (19.7%), Midwest (16.0%), Northeast (4.8%), and unknown (19.9%). Univariate analyses indicated high incidence of suicide/self-inflicted in the Midwest (47.8%) and the South (45.1%), compared with the high rates of assault in the Northeast (61.6%), the West (53.7%), and unknown (60.6%; Fig. 4). A smaller proportion of Caucasian patients was observed in the West (47.5%) and Northeast (37.9%) compared to other races. A higher proportion of African Americans was observed in the Northeast (45.5%) and South (37.3%); the category of “other races” was highest comparatively in the West (33.3%; Fig. 5). Handgun injuries were particularly frequent in the Northeast (74.2%; Fig. 6). Fifty-two percent of GSWH patients were admitted to level I trauma centers, 18.1% to level II, and the remainder were undetermined. Admission to level I trauma centers was most common in the Midwest (68.1%) followed by Northeast (64.7%); admission to level II was most common in the West (32.4%) followed by Northeast (27.6%); and undetermined trauma center level was greatest in the South (42.1%).

Injury intention and geographical region by U.S. Census. Color image is available online at

Patient race and geographical region by U.S. Census. Color image is available online at
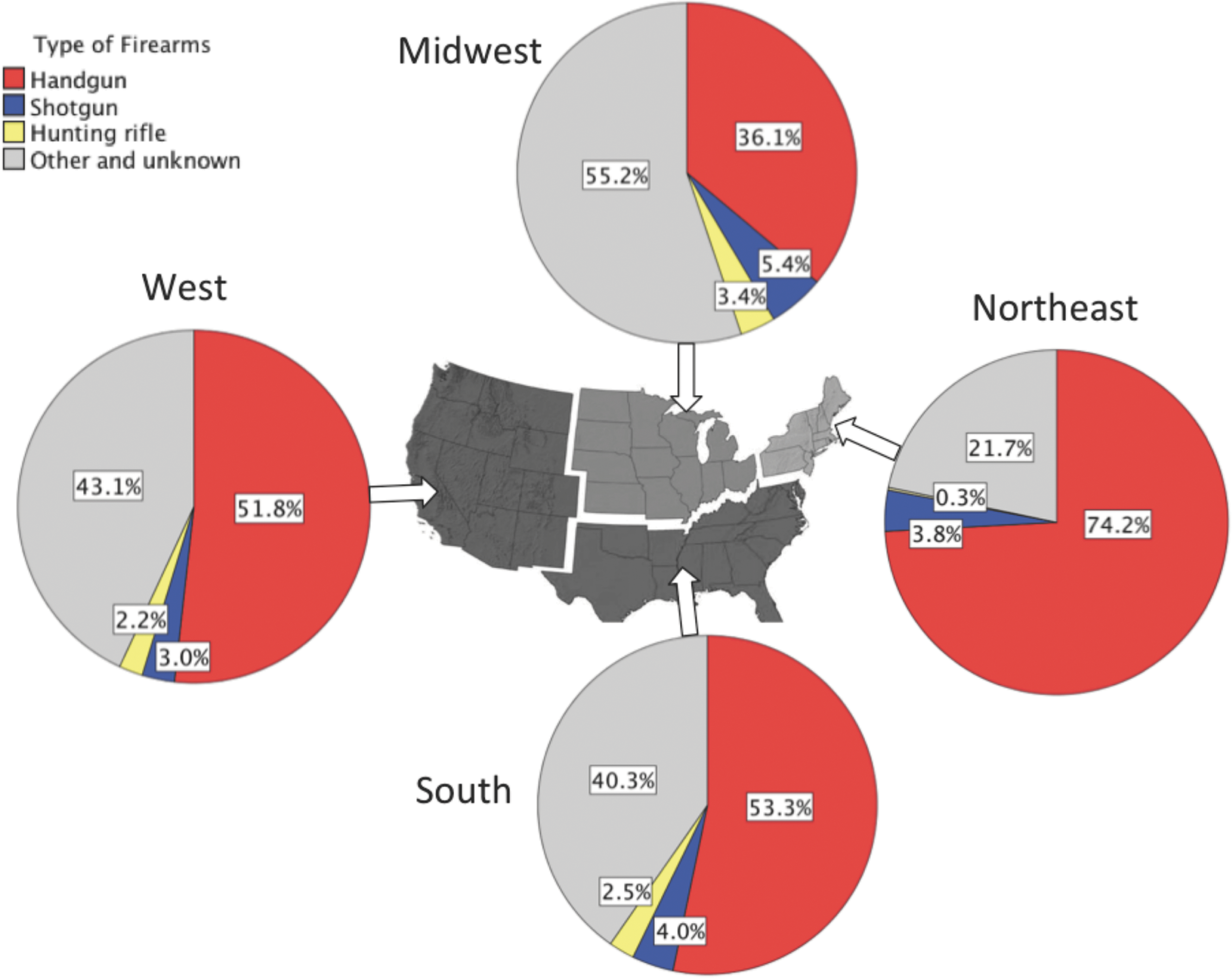
Type of firearm and geographical region by U.S. Census. Color image is available online at
Mortality
In total, 4446 deaths occurred in the cohort, which corresponded to an overall mortality rate of 54.6%. By location, 37.2% of deaths occurred in the ED, whereas the remainder occurred following triage and during inpatient hospitalization. Mortality rates by motive were highest for suicide/self-inflicted (71.6%) followed by legal intervention (45.3%), assault (41.1%), and accidents (36.7%). Regarding weapon of choice, handguns were associated with the highest relative mortality (57.8%), followed by hunting rifle (48.7%) and shotgun (31.9%), with mortality from other/unspecified at 53.3%. By age, the elderly (60+ years) fared worst with a 73.3% mortality rate, followed by age 50–59 years (63.3%), 40–49 years (54.6%), 18–29 years (50.2%), and 30–39 years (49.3%). Mortality rates by geographical region, and by trauma center, were largely comparable; by geographical region: the Northeast (58.8%), Midwest (57.4%), South (55.0%), West (53.0%), and unknown (52%); by trauma center: level II (58.7%), level I (55.0%), and undetermined (51.3%). Mortality rate did not vary by year of admission (Fig. 2). Low GCS associated with increased mortality rate (Fig. 7).
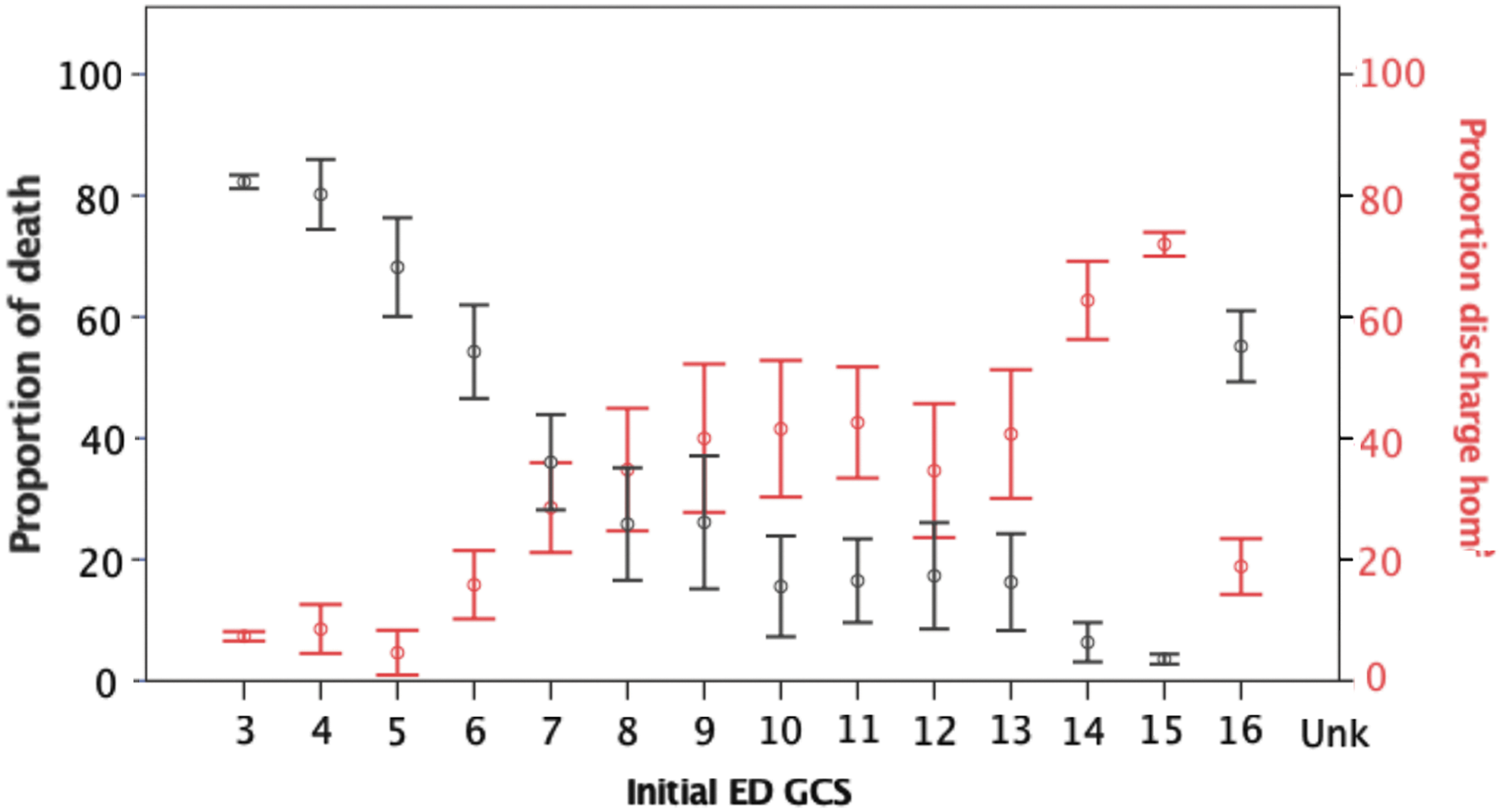
Overall rates of mortality and discharge to home by the TBI severity as assessed by initial GCS in the ED (mean % ± SE). ED, emergency department; GCS, Glasgow Coma Scale; SE, standard error; UNK, unknown. Color image is available online at
Multi-variable analysis indicated that intent of injury, type of firearm, site of incident, age, health insurance, isolated TBI, ED hypotension, TBI severity, and ISS of 25–75 or unknown were statistically significant predictors of death (Table 6). GCS score 3–8 was associated with greatest risk of death (OR, 39.4; [31.4–49.5]; p < 0.001), followed by unknown GCS (OR, 10.6; [7.4–15.2]; p < 0.001), ISS 25–75 (OR, 8.1; [4.5–14.7]; p < 0.001), and ED hypotension (OR, 5.1; [4.3–6.2]; p < 0.001). Of note, after multiple comparisons correction (threshold, p = 0.001), suicide/self-inflicted was marginally associated with higher odds of death (OR, 1.7; [1.2–2.6]; p = 0.004) compared to accidental injury. Relative to handgun injuries, shotgun (OR, 0.3; [CI, 0.2–0.4]; p < 0.001) and hunting rifle (OR, 0.5; [0.4–0.8]; p < 0.001) showed lower odds of mortality. Patients who were self-pay/unbilled (OR, 2.0; [1.6–2.5]; p < 0.001) or with unknown insurance (OR, 1.7; [1.4–2.1]; p < 0.001) were less likely to survive their injuries compared to private/commercially insured.
Hospital and intensive care unit lengths of stay
Mean HLOS was 13.9 ± 17.9 days for those who survived their injuries; when ICU admits were analyzed separately, mean ICU LOS was 8.6 ± 17.4 days. Patients who died during hospitalization had mean HLOS of 2.2 ± 5.7 days and mean ICU LOS of 2.5 ± 4.8 days. Multi-variable linear regression analysis indicated the following predictors for prolonged HLOS in survivors: suicide/self-inflicted, Medicare/Medicaid, the South geographical region, hypotensive status unknown, TBI severity, and ISS of 16–24, 25–75, or unknown; GCS of 3–8 was the only significant predictor for prolonged ICU LOS (Tables 3 and 4). ISS 22–75 (mean increase, 11.8 days; [9.4–14.3]; p < 0.001), GCS score 3–8 (mean increase, 11.0 days; [9.7–12.3]; p < 0.001), GCS score 9–12 (mean increase, 9.3 days; [7.3–11.4]; p < 0.001), ISS unknown (mean increase, 8.8 days; [6.0–11.5]; p < 0.001), GCS unknown (mean increase, 6.3 days; [3.2–9.3]; p < 0.001), ISS 16–24 (mean increase, 5.9 days; [3.6–8.2]; p < 0.001), and unknown hypotensive status (mean increase, 5.0 days; [2.4–7.7]; p < 0.001) were the greatest drivers of prolonged HLOS. Beginning in 2008, hospital LOS and ICU LOS did not vary with admission year (Fig. 2).
Multi-variate Analysis of LOS in the Hospital After Adult Firearm-Related TBI
The statistical significance threshold was set at p = 0.001 to account for multiple comparisons.
LOS, length of stay; TBI, traumatic brain injury; SEM, standard error of the mean; CI, confidence interval; NA, not applicable; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Multi-variate Analysis of LOS in the ICU After Adult Firearm-Related TBI
The statistical significance threshold was set at p = 0.001 to account for multiple comparisons.
LOS, length of stay; ICU, intensive care unit; TBI, traumatic brain injury; SEM, standard error of the mean; CI, confidence interval; NA, not applicable; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Injuries from suicide/self-inflicted mechanism demonstrated longer HLOS (mean increase, 4.4 days; [1.8–7.1]; p < 0.001) relative to unintentional injuries. In comparison to patients with private/commercial insurance, Medicare/Medicaid insurance was associated with prolonged HLOS (mean increase, 4.4 days; [2.6–6.3]; p < 0.001). By regional classification, patients treated in the South had prolonged HLOS (mean increase, 3.7 days; [2.0–5.4]; p < 0.001) compared to the Midwest. Multi-variate analysis of ICU LOS of patients who survived their injuries found GCS score 3–8 as the only significant predictor of longer ICU LOS (mean increase, 5.0 days; [3.5–6.5]; p < 0.001) relative to GCS score 13–15.
Medical complications
In total, 1412 patients (17.3%) suffered medical complications during hospitalization, which included pneumonia, acute respiratory distress syndrome (ARDS), cardiac arrest, deep venous thrombosis (DVT), coagulopathy, acute kidney injury or renal failure, pulmonary embolism, myocardial infarction, cerebrovascular complication, decubitus ulceration, and urinary tract infection. Pneumonia (5.2%), ARDS (5.0%), cardiac arrest (5.0%), and DVT (1.7%) were most common. Multi-variable analysis indicated that geographical region, TBI severity, and ISS were significant predictors for medical complications (Table 5). Compared to ISS 0–8, unknown ISS was associated with the greatest odds of complications (OR, 14.2; [4.5–45.2]; p < 0.001), followed by ISS 25–75 (OR, 10.9; [3.4–34.4]; p < 0.001) and ISS 16–24 (OR, 10.1; [3.2–31.9]; p < 0.001). Multiple comparisons correction (threshold, p = 0.001) indicated that, relative to handgun, other/unspecified weapon of injury had higher risk of complications (OR, 1.3; [1.1–1.5]; p < 0.001). Compared to the Midwest, the South had higher odds of complications (OR, 1.7; [1.4–2.0]; p < 0.001), and the West had lower odds of complications (OR, 0.6; [0.5–0.7]; p < 0.001). Complication rate did not vary by year of admission (Fig. 2).
Multi-variate Analysis of Predictors of Complications After Adult Firearm-Related TBI
The statistical significance threshold was set at p = 0.001 to account for multiple comparisons.
TBI, traumatic brain injury; CI, confidence interval; NA, not applicable; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Multi-variate Analysis of Predictors of Death After Adult Firearm-Related TBI
The statistical significance threshold was set at p = 0.001 to account for multiple comparisons.
TBI, traumatic brain injury; CI, confidence interval; NA, not applicable; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Hospital discharge disposition
Among patients who survived their injuries, 2240 (27.5%) were discharged to home and 1462 (17.9%) to rehabilitation or skilled nursing facilities. By mechanism of intent, rates of return to home were: assault (70.5%), accident (64.6%), undetermined (59.5%), legal intervention (57.9%), and a much lower return-home rate for suicide/self-inflicted (35.8%). Patients with suicide/self-inflicted mechanism of intent had the lowest odds of return to home (OR, 0.5; [0.3–0.7]; p < 0.001) compared to accidental injury. Discharge rates were comparable across firearm type and site of incident. Return to home rates were, on average, higher for younger patients: 18–29 years (66.1%), 30–39 years (62.9%), 40–49 years (59.6%), and lower for 50–59 years (46.7%) and 60+ years (29.9%). Return to home rates were comparable across the geographical regions: the South (64.4%), Northeast (62.7%), West (61.6%), and Midwest (58.0%); region of unknown (53.5%) was lower than the South and West. Patients at level II trauma centers were less likely to return home than those at level I trauma centers (53.8% vs. 62.1%). By insurance category, self-pay/unbilled patients were most likely to go home (66.9%) followed by government/other (64.7%) and unknown (64.0%), whereas Medicare/Medicaid (51.1%) and private/commercial (50.2%) patients had the lowest rates of return to home. Rate of discharge to home did not vary by year of admission (Fig. 2). Low GCS associated with decreased rate of discharge to home (Fig. 7).
Multi-variable analysis indicated that mechanism of intent of injury, age, health insurance, trauma center level, ED hypotension, TBI severity, and ISS were significant predictors of return to home (Table 7). In comparison to GCS score 13–15, GCS scores 9–12 (OR, 0.4; [0.3–0.6]; p < 0.001), 3–8 (OR, 0.4; [0.3–0.4]; p < 0.001), and unknown (OR, 0.4; [0.2–0.6]; p < 0.001) were the strongest drivers of decreased odds of returning home, followed by government/other insurance (OR, 1.7; [1.3–2.3]; p < 0.001). After multiple comparisons correction (threshold, p = 0.001), suicide/self-inflicted injuries were associated with lower odds of returning home (OR, 0.5; [0.3–0.7]; p < 0.001) compared to accidental injury. Patients with government/other insurance had higher odds of returning home (OR, 1.7; [1.3–2.3]; p < 0.001) compared to those who were privately or commercially insured. Relative to patients from level I trauma centers, level II patients were less likely to return home (OR, 0.7; [0.5–0.8]; p < 0.001).
Multi-variate Analysis of Predictors of Hospital Discharge Disposition After Adult Firearm-Related TBI
The statistical significance threshold was set at p = 0.001 to account for multiple comparisons.
TBI, traumatic brain injury; CI, confidence interval; NA, not applicable; CCI, controlled cortical impact; ACS, American College of Surgeons; ED, emergency department; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; ISS, Injury Severity Score.
Discussion
Civilian firearm-related TBI is an important public health concern with growing recognition from both the medical community and the public. Previous studies have documented the incidence of GSWH in various urban and rural communities. 8,35 –38 However, the absence of a single data set that incorporates weapon characteristics, patient demographics, inpatient course, and acute outcome has precluded large-scale analyses of specific risk factors for prolonged LOS, increased complications, and acuity of discharge destination after GSWH. The present study utilized the NSP of the NTDB to characterize the epidemiology and clinical history of U.S. firearm TBI over the past decade with a targeted interest on firearm cohort, U.S. geographical locale, and acute management strategies. To our knowledge, this study is the first to define predictors of poor outcome after GSWH across regional centers to reflect national trends of care.
Demographics and mortality
The difference in incidence between years 2003–2007 and 2008–2012 likely reflects a limitation of data acquisition during the early years and more standardized data collection with implementation of the National Trauma Data Standard (NTDS) beginning 2008. 39,40 In our analysis of 8148 adult GSWH patients triaged to a level I or II trauma center, over 60% were classified as severe TBI by GCS score, over 50% were assaults, and over 30% of patients were hypotensive (SBP, <90 mm Hg). Handgun was the most prevalent firearm type, causing half of all injuries. These findings are largely consistent with previous reports that small firearms cause approximately half of 50,000 TBI deaths each year in the United States with high rates of early mortality. 38,41 Overall mortality without accounting for out-of-hospital deaths in the current study was slightly more than half, and over 60% of these deaths occurred during inpatient hospitalization, conforming to national reports that less than half of patients arriving alive to the ED with GSWH ultimately survive their injuries at hospital discharge. 5,7,9,42 In the literature, age, CT findings of basal cistern obliteration and intraventricular hemorrhage, and GCS score at admission are consistent predictors of mortality after GSWH. 8,9,43 –47
Not surprisingly, the majority of GSWH patients were ages 18–29 years. In contrast to the higher incidence of interpersonal violence in patients <40 years of age (62%), suicide/self-inflicted injuries were more frequently observed in patients >40 years of age (65%). We found that mortality rate increased with age, and older patients were less likely to be discharged home. Severe TBI by GCS score conferred the greatest odds of death, followed by unknown GCS, ISS 25–75, ED hypotension, unknown ISS, insurance type, injury intention, and firearm type. Patients categorized as “unknown” likely include those who expired before completing their injury severity assessment in the ED, and thus an “unknown” GCS or ISS can be a marker of mortality. Similarly, patients who were self-pay/unbilled or with unknown insurance had higher rates of mortality than those with identifiable insurance. Suicide/self-inflicted GSWH conferred greater odds of death compared to unintentional injury; by firearm type, shotgun and hunting rifle were associated with lower odds of mortality compared to handgun. Shotgun wounds carry a wide severity spectrum owing to the fact that pellets scatter and behave as individual low-velocity projectiles, even at the range of a few meters. 48,49 Whereas shotgun GSWH carries lower mortality, our analysis showed that shotgun-injured patients experienced longer stays in both the ICU (mean increase, 3.5 days) and hospital (mean increase, 4.2 days). High-energy rifle bullets carry high lethality and these patients rarely survive to be admitted, unless GSWH from rifle shots are accidental hits from long range or ricocheted striking at low velocity. 50,51
Length of stay and discharge disposition
Not surprisingly, lower GCS score, increasing ISS, ED hypotension, and increasing age were also negative predictors for discharge to home; relative to patients of unintentional injury, suicide/self-inflicted injury patients were half as likely to return home. Patients admitted at level II trauma centers had an OR of 0.7 for being discharged home compared to level I trauma centers, a finding consistent with previous studies. 52 Several explanations regarding this gap in functional outcome have been proposed, including higher volume and higher acuity of patients observed in level I centers, more experienced medical personnel, in-house neurosurgeons, and the immediate availability of the operating room. 53 –56
Patients with Medicare/Medicaid had longer stays in both the hospital and ICU compared to private/commercial insurance. Medicare/Medicaid patients are often more health burdened at baseline, constituting a higher health-risk bracket and may require longer monitoring during their hospitalization. Patients who were self-pay/unbilled had shorter HLOS stay (mean decrease, 2.4 days) compared to those who were privately/commercially insured, which can be explained by both the high mortality rate of unbilled individuals and also by the gap in medical access for uninsured patients. 57 –60 Interestingly, relative to private/commercial insurance, patients with government-sponsored insurance were more likely to be discharged home. Although the reason for this finding is unclear, it is possible that patients insured by government agencies have set care standards before a patient is deemed ready for discharge, as well as an organized network of referrals and/or placement to low-acuity residential facilities, in-home health services and social/community services.
Isolated gunshot wounds to the head versus polytrauma
The majority of patients suffered additional trauma not limited to the head and face. A higher proportion of polytraumatic injuries were from assault, whereas a majority of isolated TBI and face injuries were suicide/self-inflicted. In the past several decades, demand for pistols has increased in part because of their increased capacity (vs. the six-round capacity of revolvers); accordingly, the number of patients with multiple GSWs in assaults increased as well. 61 A recent study found that in urban communities of low socioeconomic status, multiple GSWs was associated with higher mortality and longer ICU stay. 62 National data indicate that approximately one in four Americans shot during interpersonal violence do not survive. 63 For assaultive GSWH, we report a mortality rate of 41%. In the context of all GSWH events, isolated TBIs have higher mortality than nonisolated (74% vs. 52%), partly attributed to the close-range lethality by suicide/self-inflicted injury compared with being shot multiple times at farther range. We observed no difference in HLOS and ICU LOS in isolated versus polytraumatic injuries for patients surviving to hospital discharge.
Medical complications
Similar to the other outcomes assessed in this study, GCS and ISS scores were the strongest predictors of medical complications. Pneumonia (5%), ARDS (5%), cardiac arrest (5%), and DVT (2%) were most frequently observed, which aligns with the fact that severe brain injury, mechanical ventilation, depressed consciousness, aspiration, and secondary cerebral insults are prominent risk factors for pulmonary complications when the central nervous system/respiratory axis is altered after severe TBI. 64 –67 Previous evidence recommended that the prevention or reversal of such complications should be prioritized during critical care to improve outcome. 68 In comparison to handgun, other/unspecified firearms had a higher complication rate; differences in ballistics may play a role and deserve additional investigation in future studies. Inherent missile characteristics (mass, shape, and construction), velocity (longitudinal and rotational), and fragmentation tendency during impact (hollow point or soft point) confer differing injury patterns that alter clinical course and risk for complications. 69,70
Distinctions by U.S. region and trauma center designation
This study demonstrated a few regional differences of interest. Compared with patients treated in the Midwest, those in the South had a higher complication rate whereas the West had a lower complication rate. The South also had a prolonged HLOS (mean increase, 3.7 days) relative to the Midwest; a higher complication rate would naturally result in longer hospitalization. Although mortality rates did not vary across the United States as was expected, the discrepancies in regional complication rate and hospitalization length are worth noting. Although great efforts at standardization have been made since the Guidelines for the Management of Penetrating Brain Injury was published in 2001, GSWH represent a unique subset of TBIs in need of evidence-based-guidelines on optimal management. 71 –73 Recently, there is a trend toward less-aggressive debridement of bone and missile fragments and more-aggressive antibiotic prophylaxis. Whether the best surgical approach is craniectomy or craniotomy and the survival benefit from intracranial pressure (ICP) monitoring are still under debate, with varied reports on morbidity and mortality. 12,74 –76 Other explanations previously put forth include differences in trauma center distribution and services expenditure, varied stages of regionalization for trauma-care delivery, and urban-rural pre-hospital care. 77 –80
Cost of gunshot injuries
Firearm ownership policies worldwide correlate, and often are commensurate with, national firearm-related injury rates. The correlation between gun ownership and homicide/suicide rates has been previously affirmed by the International Crime Survey in 14 countries including the United States. 81 Other studies showed similar findings, with the highest comparative rate of firearm-related injuries in the United States. 82,83 On the other hand, lower gun availability has not been shown to spur an increase in other methods of homicide and suicide. Whereas rates of both homicide and suicide by firearm rise with gun ownership, it has a stronger impact on suicides than homicides, and, given the particularly high mortality associated with a suicidal intent, reducing gun availability may decrease risk of firearm-related deaths. 84
Cook and colleagues estimated the national cost of acute-care and follow-up treatment to be $17,000 per gunshot injury, which in 1994 alone produced $2.3 billion in lifetime costs; assaults accounted for 74% of the aggregate cost. 85 Considering that U.S. taxpayers paid nearly $1.1 billion (49%) of these costs, firearm injuries create a substantial burden to the healthcare system. 86 –88 Further, the financial burden per injury is substantially greater for gunshot trauma to the head, with the mean cost of treatment in these patients totaling $117,338 per individual. 89 Firearms rank second only to motor vehicles among all consumer products in their consumption of public healthcare funds.
Limitations of the study
This study is not without limitations. First, it only included data submitted by level I and II trauma centers participating in the NTDB, and therefore does not capture GSWH at non-ACS-designated trauma centers, and injuries without sufficient severity to triage to higher-acuity care. GSWH patients who expire at the scene, or en route to the hospital, are likewise not captured by the NTDB. Therefore, the true incidence and prevalence of GSWH in U.S. trauma centers are likely several times higher than recorded in the current analysis, on both extremes of the injury severity spectrum. The increased incidence from 2007 to 2008 was attributed to improved standardization and uniformity of information collection by the trauma registry, which limited the potential to accurately compare the periods 2003–2007 with 2008–2012. Specifics of the hospital management course, such as critical care management, are not recorded in the NTDB and represent a significant limitation to the understanding of the optimal management course for distinct GSWH injury profiles, as well as protocol differences relating to U.S. regions. It is known that significant practice variation exists among even trauma centers of the same region and acuity, which is another shortcoming of retrospective analyses, given that comparative effectiveness cannot be readily determined.
For the current analysis, we focused on the demographic and clinical injury effects on acute outcome after GWSH, and did not delve into the myriad of surgical interventions appropriate for various GWSH etiologies and severities, which should be the subject of future studies of similar scale. Associations between the type of neurosurgical intervention and outcomes, such as length of stay, complications, disposition, and mortality, constitute topics of ongoing study to improve management, prognosis, and recovery post-GSWH. In addition, the sequelae of medical complications, and subsequent interventions, are not recorded by the NTDB and represent a gap in our understanding of GSWH outcome in the United States. We are also limited to 30-day outcomes in the NTDB and are unable to determine the long-term outcome of patients contained in this study nor improvement or decompensation in their trajectory of recovery.
Another limitation of the national database, particularly for a patient population with high injury severity and mortality at initial triage, may be the lack of complete data reporting. Although we perform multi-variable regressions to identify predictors for poor outcome, we are limited by the data submitted to the NSP of the NTDB. Improved quality assurance to minimize unknown data would aid future studies in the GSWH population. Gunshot injuries characterized as separate entities (i.e., homicide vs. suicide) can often comprise interconnecting crimes (i.e., homicides-suicides). 83 Such a distinction does not exist in the NTDB nor the majority of retrospective studies to date; hence, improved characterization of interconnecting crimes would provide a more accurate understanding of firearm epidemiology in the United States and possibly provide evidence for formulating effective policies at reducing GSWH.
Conclusions
Older age, hypotension, and injury severity (GCS and ISS) are associated with poor prognosis after firearm-related TBI. Isolated GSWH and handgun injuries are associated with higher mortality. Suicide/self-inflicted GSWHs are more likely to suffer prolonged hospitalization and decreased odds of returning home. Compared with level I trauma centers, GSWH patients treated at level II trauma centers have lower odds of being discharged home. Patients with Medicare/Medicaid insurance show longer hospitalizations than those with private/commercial insurance, patients of self-pay/unbilled insurance have higher mortality, and patients of government/other insurance are more likely to be discharged home. Practice differences for GSWH management likely exist among U.S. geographical locales and warrant further investigation. Improved understanding of civilian GSWH is critical to promoting increased awareness of firearm injuries as a public health concern and reducing its injury burden to patients, families, and healthcare systems.
Footnotes
Acknowledgments
Committee on Trauma, American College of Surgeons, NTDB NSP 2003-12, Chicago, IL. The content reproduced from the NTDB NSP remains the full and exclusive copyrighted property of the American College of Surgeons. The American College of Surgeons is not responsible for any claims arising from works based on the original data, text, tables, or figures.
Author Disclosure Statement
No competing financial interests exist.