
Abstract
This study longitudinally assessed 10- to 14-year-old patients with sports and recreational concussion (n = 22) who remained symptomatic 3 to 4weeks post-injury compared with typically developing controls (n = 24). Examination by multi-modal magnetic resonance imaging (MRI) and multi-domain clinical outcome measures was completed at 1-month and 6-months post-injury. Concussion patients showed evidence of improvement by 6-month follow-up in domains of cognitive function, whereas measures of psychological health were less resolved with patients exhibiting sustained symptoms of depression, behavior impairment, and concussion symptoms. Quantitative neuroimaging measures identified measures indicative of chronic injury with regional reductions observed by both volumetric segmentation and white matter fractional anisotropy (FA) from diffusion tensor imaging (DTI). Volumetric reductions (p < 0.01) were observed in the middle anterior and posterior portions of the corpus callosum, and right caudal anterior cingulate cortex of patients, although none held after strict correction. Examination of the FA data identified significant reductions in the left middle frontal gyrus white matter (p = 0.0003). Linear regression analysis on the 6-month depression outcome variable using the initial clinical, demographic, and imaging measures identified the top predictive models to include concussion diagnosis, and initial symptoms of depression, concussion symptoms, and sleep impairment with additional contribution from other measures of mental health, behavior impairment, and quality of life depending on the model (adjusted r-squared = 0.69 indicating strong predictive ability). This study supports further inclusion of mental health rehabilitation and imaging supplementing traditional cognitive rehabilitation strategies employed in these young athletes.
Introduction
There has been a growing public health concern regarding the impact of concussion exposures on youth athletes with over 1 million new pediatric cases of sport and recreational concussion occurring each year. 1 Current imaging diagnostic techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) are often insensitive to the underlying pathophysiological changes following these concussion exposures, so much so that the explicit definition of these uncomplicated mild brain injuries includes the absence of traditional radiological findings. 2 More recent efforts suggest a role for quantitative neuroimaging techniques in elucidating the underlying brain changes associated with concussion. Caution is warranted however, as there is currently limited understanding of the clinical and biological relevance of these imaging findings 3 and how this relationship may evolve over time post-injury. There is an unmet need for longitudinal studies in the pediatric athletic population to help resolve the current knowledge gap.
Although efforts have begun to address this need, longitudinal quantitative neuroimaging and clinical evaluation of sports-related concussion has been mostly limited to the study of older adolescence and college-aged athletes. 4 –11 The majority of these studies only assessing participants weeks 4,11,12 to 1–3 months 5 –7, 12,13 post-injury. One study did examine college-aged athletes within the first week and then again 6 months later, reporting sustained changes in quantitative imaging metrics derived from diffusion tensor imaging (DTI), 8 but questions remain regarding the recovery trajectory and chronic outcome in younger athletes. Prior work suggests that this younger age group may be particularly susceptible to prolonged symptoms 14,15 and exhibit sustained quantitative neuroimaging changes out to 3 months, 13 but it is unclear what early clinical or imaging information would best predict symptom prolongation and longer-term outcome.
The objective of the current study was to longitudinally assess 10- to 14-year-old patients with sports and recreational concussion who remained symptomatic at 3–4 weeks post-injury and compare them with typically developing controls. Examination by both multi-modal MR imaging and multi-domain clinical outcome measures was completed at 1-month post-injury and 6 months later. This was done to test the hypothesis that the early outcome and imaging could be used to predict 6-month follow-up clinical presentation, thereby addressing some of the concern regarding clinical relevance of these quantitative neuroimaging techniques. We further hypothesized that we would identify evidence of recovery that could aide in informing more targeted rehabilitation in the future in this youth athlete population. To our knowledge this is the first longitudinal clinical and quantitative neuroimaging imaging study in 10- to 14-year-old sports concussion patients carried out to the early chronic outcome of 6 months.
Methods
This was a prospective, observational, longitudinal study of symptomatic pediatric sports and recreational concussion patients compared with typically developing controls. Cross-sectional findings from the initial study evaluation have been previously reported. 16 Inclusion criteria stipulated youth were 10 to 14 years of age, either gender, able to provide their own assent with parental consent, and willing and able to complete an MRI scan. Exclusion criteria for both groups specified no history of neurological disorders or psychiatric diagnoses, no contraindications to MRI scans, no claustrophobia, and no history of major head injury defined as any head injury exposure greater than a concussion. Of note, previous diagnosis of concussion was not a rule-out for the concussion group, whereas controls were excluded if they had any prior head injury diagnosis including concussion. Symptomatic concussion was defined as patients who had sustained a concussion during sports or recreational play that was diagnosed by a treating physician, whose symptoms had remained unresolved after a minimum of 4 weeks post-injury, and who had been seen in the Sports Medicine, Concussion, or Rehab Medicine specialty clinics at Seattle Children's Hospital. Study evaluations were completed at 4–6 weeks and 6–12 months post-injury.
Patients were identified by their concussion diagnosis code and scheduled appointments. Informational letters were sent to the families of prospective patients briefly explaining the study and inquiring about participation. Interested families followed up with the study team regarding participation. Typically developing youth, who comprised the control group, were identified through study flyers and advertisements posted through research networks at Seattle Children's Hospital and the University of Washington Institute of Translational Health Sciences. The study was approved by the Institutional Review Board at Seattle Children's Research Institute and all study procedures were conducted at the University of Washington School of Medicine in accordance with the approved protocol. Compensation for participation was provided in the form of gift cards. All concussion patients completed a suggested treatment course by their advising physicians between the two time-points of study evaluation. No intervention was provided for research purposes.
Clinical evaluations
At each study visit, neuropsychological evaluation consisted of the Immediate Post-Concussion Assessment and Cognitive Test 17 (ImPACT), a computer-based measure of verbal memory, visual memory, visual motor speed, reaction time, and impulse control in addition to overall symptom severity endorsement; the King Devick, 18 a measure of visual processing; the Weschler Intelligence Scale for Children, 5th Edition 19 -Digit Span, a measure of auditory working memory; the Delis-Kaplan Executive Function System Test 20 -Verbal Fluency Module, a measure of verbal fluency; the Symbol Digit Modalities Test, 21,22 a measure of oral and written processing speed; and the Grooved Peg Board Test (Lafayette Instrument, Inc.), a measure for fine motor speed and dexterity. Overall health behavior impairment and quality of life were measured by the Health Behavior Inventory-20 Item 23,24 (HBI) and the Pediatric Quality of Life Inventory 25 (PedsQL), respectively. Mental health symptoms and overall sleep impairment were measured by the Patient Health Questionnaire-9 item 26 (PHQ-9) for depression, the Generalized Anxiety Disorder-7 Item 27 (GAD-7), and the Adolescent Sleep-Wake Scale (ASWS). 28 Clinical evaluations were reviewed after each study visit by a neuropsychologist (D.C.) with expertise in sports psychology with follow-up evaluation by a pediatric psychiatrist (N.D.L.) to screen for any concerning mental health endorsements. Total time to complete evaluations and assessments was 1.5 h. Participants were allowed to take breaks as needed. All testing was completed in quiet, private, well-lighted rooms by study psychometrists trained to administer assessments. All assessments listed were collected for research purposes only and were not part of any patient's formal medical record.
MRI acquisition
At each study visit, participants also underwent an MRI scan. MRI scans were completed on a 3T Philips Achieva with a 32-channel head coil. Each imaging session lasted ∼40 min and included a 1-mm isotropic MPRAGE (repetition time [TR] = 7.6 msec, echo time [TE] = 3.5 msec, Matrix = 240 × 240, Slices = 180, 5:13), 1-mm isotropic three-dimensional [3D] T2-weighted (T2W) image (TR = 2500 msec, TE = 250 msec, Matrix = 240 × 240, Slices = 180, 5:22), 1 mm × 1 mm × 3 mm 3D T2-Star (TR = 45 msec, TE = 25 msec, Matrix 180 × 180, Slices = 54, 3:41), 2D fluid-attenuated inversion recovery (FLAIR) collected at an in-plane resolution of 1 × 1 mm with a slice thickness of 4 mm, no gaps (TR/inversion time [TI] = 11000/2800 msec, TE = 125 msec, Matrix = 280 × 186, Slices = 30, 2:56), 3-mm isotropic resting-state funtional MRI (fMRI) (TR = 2000, TE = 25 msec, Matrix = 64 × 62, Slices = 40,7:14) and a 32 direction 2-mm isotropic diffusion sequence acquired with reverse polarity (A-P, P-A), b = 1000 sec/mm2, and 6 non-diffusion weighted images collected together for DTI analysis (each TR = 7800 msec, TE = 69 msec, Matrix = 128 × 128, Slices = 72, 6:39). MRI scans were reviewed by a board-certified -ediatric neuroradiologist (J.W.) after each study visit.
Diffusion tensor imaging (DTI) post-processing and analysis
The DTI post-processing pipeline utilized for this study 29 employed the analytical methods constructed by Dr. Carlo Pierpaoli and colleagues at the National Institutes of Health (NIH) called TORTOISE: Tolerably Obsessive Registration and Tensor Optimization Indolent Software Ensemble. 30 For reverse polarity data, each DWI acquisition both A-P and P-A is initially run through DiffPrep 31,32 in TORTOISE for susceptibility distortion correction, motion correction, eddy current correction, and registration to a 3D high resolution structural image. For echo planar imaging (EPI) distortion correction, the diffusion images were registered to the 1-mm isotropic T2 image using non-linear b-splines. Eddy current and motion distortion were corrected using standard affine transformations, followed by re-orientation of the b-matrix for the rotational aspect of the rigid body motion. Following DiffPrep, the output images from both the A-P and P-A DWI acquisitions were then sent through Diffeomorphic Registration for Blip-Up Blip-Down Diffusion Imaging 33 (DR-BUDDI) in TORTOISE for further EPI distortion and eddy current correction that can be completed with diffusion data that has been collected with reverse polarity. This step combines the reverse polarity imaging data to create a single, cleaned, DWI data set that is then sent through DiffCalc 34 –41 in TORTOISE. This step completes the tensor estimation 42 using the robust estimation of tensors by outlier rejection (RESTORE) 39 approach. Following tensor estimation, a variety of DTI metrics can be derived. For this study, we specifically focused on fractional anisotropy (FA) as our main metric for analysis.
Following this post-processing in TORTOISE, 3D image stacks for mean diffusivity (MD) and FA were introduced into DTIstudio 43,44 for segmentation of the DTI atlas 45 onto each participants DTI data set in “patient space” through the Diffeomap program in DTIstudio using both linear and non-linear transformations. This is a semi-automated process that allows for the extraction of DTI metrics within each 3D-atlas-based region of interest providing a comprehensive sampling throughout the entire brain into 189 regions including ventricular space. Given that previous studies have reported an impact of head motion in particular in this youth population, 46 examination of noise parameters was completed following post-processing and compared between groups to confirm that the imaging data from the concussion group in particular was not falsely influenced by poor image quality due to head motion. Although collection of reverse polarity data collected at different points in the imaging protocol and processed with DR-BUDDI as noted above will greatly reduce this impact, examination of the noise values for the DTI scans comparing control with concussion patients at each time-point confirmed there were no differences (Time 1 Control noise mean ± standard deviation [sd] = 1.73 ± 0.74, Concussion noise mean ± sd = 1.74 ± 0.71, Control rms = 1.39, Concussion noise rms = 1.39, p = 0.40 and 0.75, respectively; Time 2 Control noise mean ± sd = 1.72 ± 0.90, Concussion noise mean ± sd = 1.70 ± 0.89, Control rms = 1.38, Concussion noise rms = 1.35, p = 0.21 and 0.16, respectively). For this study, selection of regions was limited to regions of white matter, as the main hypothesis regarding DTI was that there would be reductions in white matter integrity observed with FA related to concussion. This reduced the number of regions used for further analysis to 78. In an exploratory analysis, MD was also examined in these very same regions. To select only white matter, FA images were then thresholded at 0.2 or greater, and the data within each of the 78 regions of interest were extracted in ROI Editor on both the FA and MD image for further analysis.
Quantitative volumetric segmentation
Post-processing of the 3D T1-weighted high-resolution structural MPRAGE image was performed using Freesurfer 47 v5.3.0 for volumetric segmentation. Freesurfer is a semi-automatic segmentation program for observing volumetric data using a high-resolution structural T1-weighted image. This process is divided into two primary parts. The first part consists of sub-cortical/white matter surface creation and segmentation of the individual structures. The second part provides reconstruction of the cortical surface, created from the underlying white matter surface followed by parcellation of the cortical areas. Image processing steps include initial regression of extraneous, non-cortex/non-white matter tissue and motion correction before alignment with the MNI template. Spatial registration of the brain mask to the MNI space is completed prior to the elimination of topological defects. After this, generation of the “pial/cortical” and “white matter” tessellated surfaces is completed. Quality assurance (QA) of the image processing includes review of QA/quality control (QC) measures including noise values, null values, and fit measures. Additionally, complete visual inspection in each orthogonal plane of the segmentation is done with application of control points where needed to assure correct alignment of the automated Freesurfer program and to correct for small erroneous inclusions of other anatomy such as blood vessels, dura, and any white matter lesions. This is completed by a radiological technician who has been trained in neuroanatomy and is expert in using the Freesurfer processing software. The current study focused on primarily whole brain volume 48,49 and select sub-cortical region comparisons given previous literature on pediatric brain injury. 49 Segmentation of cortex into 68 cortical regions segmented by Freesurfer were evaluated in an exploratory fashion after they were inspected by an imaging scientist blinded to the clinical status of the participant, following control point correction and reprocessing where needed.
Statistical analysis
Differences in demographic information between the concussion and control group were assessed for statistical significance using Mann-Whitney and Fisher's exact tests as appropriate. Differences in neurospychological test performance and quality of life at 6 months between the two groups was evaluated with Mann-Whitney tests and Cohen's d. Improvement in clinical outcome measures are reported as Cohen's d; however, statistical significance of the group differences was assessed using mixed-effects linear regression on the actual scores. Cross-sectional comparisons in neuroimaging data were assessed using Mann-Whitney tests and Cohen's d, whereas evaluation of change in a neuroimaging measure over time was determined using mixed-effects linear regression. All of these models included a random-intercept for each subject and an unstructured correlation matrix, with significance determined using a group-by-time interaction effect. Adjustments for multiple comparisons were made using Bonferroni-Holm prediction models were constructed using a best-subset approach based on Akaike Information Criterion (AIC), 50 in which all possible combinations of a limited set of potential predictors are compared using a metric that accounts for both goodness-of-fit and parsimony.
For outcome, we conducted univariate analyses correlating the 6-month outcome parameter with data from the initial evaluation in those very same participants, which included concussion diagnosis, 6 demographic variables (age, height, weight, education, gender, handedness), 26 clinical outcome measures, 78 regions of FA, and the 15 primary volumetric regions adjusted for total brain volume. The top 12 most significant predictors by univariate analysis were then used for each outcome to determine the best models according to Akaike Information Criterion (AIC). Twelve predictors were chosen due primarily to computational convenience, but also to help guard against overfitting. The threshold for univariate significance was a p-value ≤0.025. Based on all possible combinations of univariate predictors, 4096 different multi-variate models were fit by linear regression, and the AIC statistic was calculated for each model. AIC is a likelihood-based measure of a model's information content. For these analyses we opted to use a slightly modified version, noted in the prediction tables as “AIC Corrected” that is recommended for modeling when using smaller sample sizes. 51 For each outcome, 10 prediction models with the lowest (best) AIC corrected values are reported, presenting them in columnar format to allow for easy comparison. Although there is no formal test to assess whether difference between models based on AIC is significant, a generally accepted rule of thumb is that models with AIC values within 2 of the lowest AIC are not substantially different in their predictive ability. 52 All 10 models for each outcome are within this range.
Results
We assessed 230 potential youth for eligibility in the study with the majority of participant exclusion resulting from resolution of symptoms in the concussion group (Fig. 1). In total, 52 youth were enrolled in the study: 27 controls and 25 symptomatic concussion patients; 46 completed both time-points of evaluation: 24 controls and 22 symptomatic concussion patients. Whereas the study did not follow a true match sample paradigm, comparison of participant characteristics confirmed excellent agreement on all primary demographic parameters including age, height, weight, education, gender, and handedness (Table 1). Both groups also showed comparable diversity across sports played (p = 0.96). As history of concussion was not an exclusion for concussion patients as it was for the controls, a small subset of study participants in the concussion group did report previous concussion diagnosis. In 6 of our concussion patients (24%), 5 reported 1 previous concussion diagnosis and 1 patient had 2 prior concussions with a mean time since previous concussion of 18 months. As the findings from the initial evaluation have been previous described, 16 the current study focused on the longitudinal results and comparison at 6-month follow-up evaluation. Mean time post-injury to this second evaluation was a minimum of 6 months (mean = 6.88 months, sd = 3.32 months) with a 6- to 12-month post-injury window of evaluation.
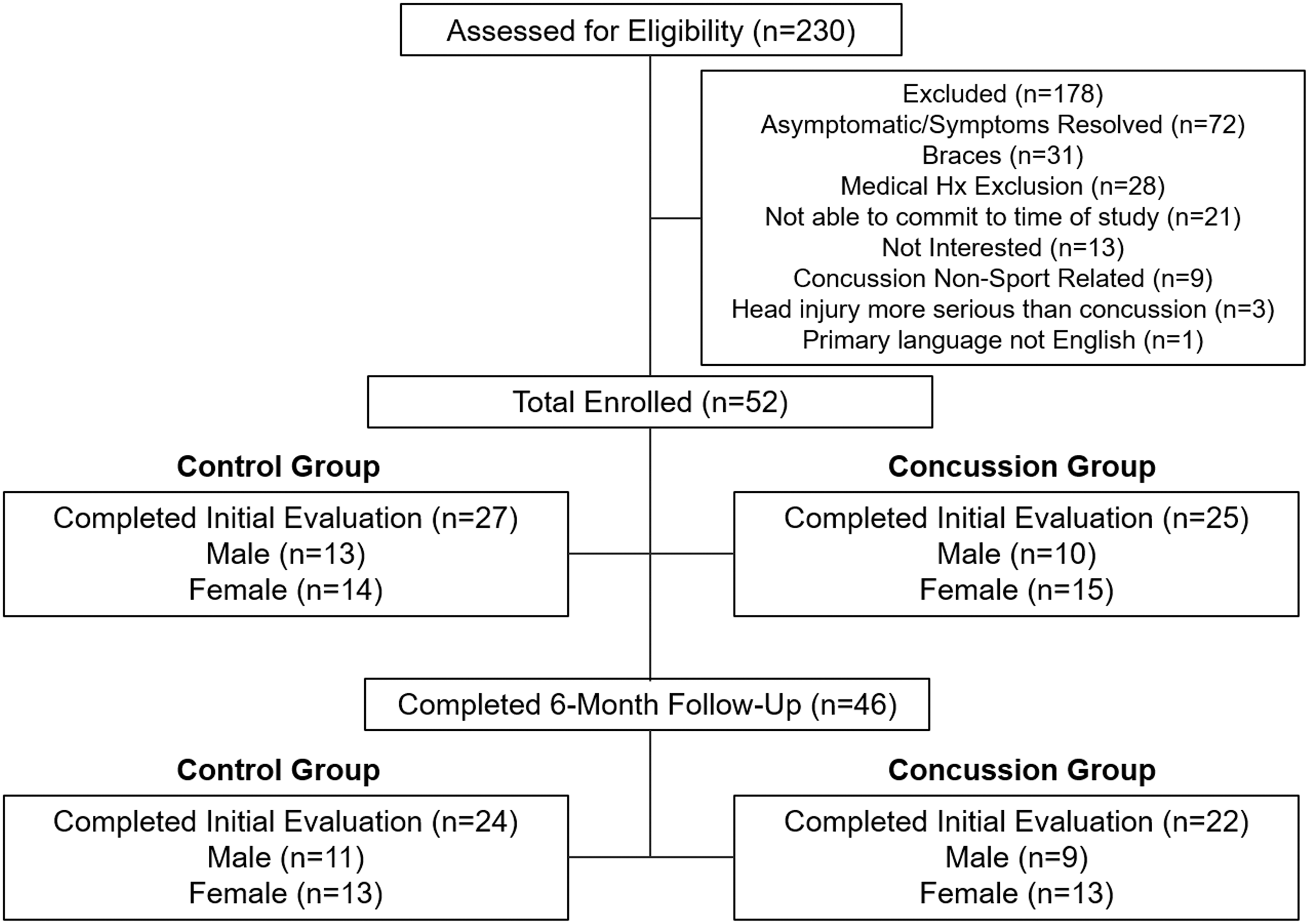
Consort diagram of enrollment and longitudinal evaluation.
Participant Characteristics at 6-Month Follow-Up
P-value reported from Fisher's exact test; all others Mann-Whitney U test.
sd, standard deviation.
Overall, neuropsychological test performance was comparable between controls and pediatric concussion patients at 6-month follow-up (Table 2). There were no significant differences in cognitive performance at this second time-point of evaluation and the domains (verbal memory, auditory working memory) in which concussion patients had poorer performance at the initial evaluation 16 appeared to have resolved. Interestingly, there were different patterns of significant improvement from initial evaluation when comparing the controls with the concussion patients (Table 2). The typically developing controls showed significant improvement on measures of visual motor speed, impulse control, oral and written processing speed, and motor speed and coordination, whereas the concussion patients showed significant improvement in verbal memory performance, visual motor speed, reaction time, and oral processing speed. The only domain in which an improvement was observed in the concussion patients that was significantly greater than that of the controls was on the symptom score derived from the ImPACT tool, which is a measure of concussion symptoms, not cognitive performance.
Neuropsychological Test Performance at 6-Month Follow-Up and Comparison to Initial Evaluation
Indicates significance after correction for multiple comparisons via Bonferroni-Holm (n = 15).
Indicates nominal significance (p < 0.01).
In contrast to the largely unremarkable cognitive test performance comparison, concussion patients did exhibit sustained impairment in domains of psychological health and health behavior at 6-month follow-up, which was significantly elevated in comparison which controls (Table 3). Concussion patients had significantly higher severity of symptoms of depression as well as greater frequency of health behavior impairment noted on the health behavior inventory at 1-month post-injury 16 and this remained the case at 6-month evaluation. This was particularly discouraging given that the concussion group did in fact show improvement on both of these measures from baseline and all concussion patients had been seen and treated by physicians specializing in concussion care management between the two time-points of evaluation. Additionally, 50% of the concussion patients met the criteria for depressive symptoms on the PHQ-9, but it should not be overlooked that 21% of the controls did as well even though both groups were carefully screened for any history of mental health conditions prior to enrollment. There was no difference in sleep performance as evidenced by the findings on the ASWS, or the GAD-7, which measures symptoms of anxiety. Overall measures of quality of life were also not distinguishing between groups at 6-month follow-up; however, this appears to be driven by the significant improvement in the concussion patients from initial evaluation, whereas the controls remained stable. To investigate the role of gender impact on all clinical measures of outcome, groups were dichotomized by sex and compared in a secondary analysis. No significant differences by gender were observed, which held after statistical correction on any clinical measure at either time-point examined by group (control p-value range: 0.01–0.87, concussion p-value range: 0.03–0.99).
Quality of Life, Sleep Impairment, Psychological Health, and Health Behavior: 6-Month Follow-Up and Comparison to Initial Evaluation
Indicates significance after correction for multiple comparisons via Bonferroni-Holm (n = 11).
Indicates nominal significance (p < 0.01).
Fisher's exact test employed for these two secondary outcome measures, all other p-values are from Mann-Whitney U test.
Conventional neuroimaging findings at 6-month follow-up were largely unremarkable and were no different from initial evaluation. Examination of the conventional images (MPRAGE, 3D-T2W, 3D-T2-Star, 2D-FLAIR, DWI) by a board-certified pediatric neuroradiologist (J.W.) revealed only incidental findings and were mostly unremarkable for pathoanatomical lesions consistent with brain injury. This is in line with the clinical definitions of uncomplicated mild traumatic brain injury or concussion, which can include absence of traditional radiographical findings as part of the description. Incidental findings included subarachnoid cyst formation (1 control, 1 concussion patient), asymmetric tonsillar ectopia without Chiari malformation (2 controls), and nonspecific T2 hyperintensities (2 controls, 2 concussion patients). These had been previously identified upon initial imaging evaluation and remained stable at 6-month follow-up. No participant, control, or concussion patient had more than one incidental finding.
Quantitative neuroimaging evaluation by both quantitative volumetric segmentation of the whole brain, cortical, and subcortical regions and by DTI did identify sustained abnormalities in the concussion patients at 6-month follow-up, although only minor after proper statistical correction for multiple comparisons via Bonferroni-Holm. Volumetric reductions (p < 0.01) were observed in concussion patients in the middle anterior (Control mean ± sd = 580 ± 173 mm3, Concussion mean ± sd = 478 ± 121 mm3, p = 0.01, Cohen's d = 0.73) and posterior portions of the corpus callosum (Control mean ± sd = 969 ± 166 mm3, Concussion mean ± sd = 862 ± 107 mm3, p = 0.009, Cohen's d = 0.76), and right caudal anterior cingulate cortex (Control mean ± sd = 2884 ± 390 mm3, Concussion mean ± sd = 2479 ± 0.007 mm3, p = 0.001, Cohen's d = 0.99), although none held after strict statistical correction by Bonferroni-Holm. Further, adjusting for total brain volume produced similar results for the middle anteriorportion of the corpus callosum (p = 0.017, Cohen's d = 0.70) and right anterior cingulate cortex (p = 0.02, Cohen's d = 0.63) with the posterior portion of the corpus callosum becoming less discriminating between groups (p = 0.07, Cohen's d = 0.46); again none held after Bonferroni-Holm correction. This was in contrast to the initial 1-month evaluation where left hippocampal volume (LHC) was reduced in concussion patients and an overall intracranial volume (ICV) in addition to total brain volume (TBV) was noted to be smaller than the typically developing controls. 16 By 6-month evaluation these differences had resolved due to the increase in volume in these regions in the concussion patients, whereas the controls remained relatively stable (change from initial evaluation comparing concussion with controls by mixed model regression; LHC = 153 mm3, p = 0.007, ICV = 43,380 mm3, p = 0.048, TBV = 13,751 mm3, p = 0.22). Linear mixed model regression was also employed to compare the change in the volumetric regions adjusted for age and TBV within each group from initial to 6-month evaluation, and no significant differences by group were identified (Control p = 0.08–0.99, Concussion p = 0.03–0.91).
Examination of the FA data extracted from the DTI scan did identify significant reductions in FA in the left middle frontal gyrus white matter in the concussion patients compared with controls (Control FA mean ± sd = 0.339 ± 0.01, Concussion mean ± sd 0.328 ± 0.007, p = 0.0003, Cohen's d = 1.18). Additional regions that showed reductions in FA trending toward significance at 6-month follow-up included the white matter of the left superior parietal gyrus (Control FA mean ± sd = 0.414 ± 0.01, Concussion mean ± sd = 0.406 ± 0.01, p = 0.02, Cohen's d = 0.67), left superior frontal gyrus (Control FA mean ± sd = 0.395 ± 0.01, Concussion mean ± sd = 0.388 ± 0.01, p = 0.02, Cohen's d = 0.66), and the left posterior portion of the middle frontal gyrus (Control FA mean ± sd = 0.374 ± 0.01, Concussion mean ± sd = 0.368 ± 0.008, p = 0.02, Cohen's d = 0.66), although these did not hold after statistical correction by Bonferroni-Holm. At the initial evaluation no region of FA survived correction by Bonferroni-Holm, although few regions trended toward significance including the left middle frontal gyrus white matter (Control FA mean ± sd = 0.338 ± 0.01, Concussion mean ± sd 0.331 ± 0.008, p = 0.006, Cohen's d = 0.72), right precuneus (Control FA mean ± sd = 0.314 ± 0.01, Concussion mean ± sd 0.304 ± 0.01, p = 0.006, Cohen's d = 0.72), and left fusiform gyrus (Control FA mean ± sd = 0.296 ± 0.01, Concussion mean ± sd 0.289 ± 0.007, p = 0.007, Cohen's d = 0.71).
Linear mixed model regression was also employed to compare the change in FA regions over time within each group from initial to 6-month evaluation. Controls were found to have a significant decrease in FA over time that held after Bonferroni-Holm correction in the genu, body, and splenium of the corpus callosum (all corrected p = 0.004) although cross-sectional comparison with concussion patients did not identify any significant group differences at either time-point in these regions. Concussion patients were found to have a significant decrease in FA over time that held after Bonferroni-Holm correction in the superior cerebellar peduncle (corrected p = 0.004), although cross-sectional comparison with controls did not identify any significant group differences at either time-point in this region. Neither group was found to have any significant increases in FA over time in the 78 white matter regions assessed. Exploratory examination of MD in these very same regions did not identify any statistically significant differences comparing concussion patients with typically developing controls at either the initial evaluation (p = 0.04–0.99 across all 78 regions) or the 6-month follow-up (p = 0.03–0.96 across all 78 regions). Linear mixed model regression was also employed to compare the change in MD regions over time within each group from initial to 6-month evaluation. Controls were found to have a significant increase in MD over time that held after Bonferroni-Holm correction in the splenium of the corpus callosum (corrected p = 0.004), right posterior limb of the internal capsule (corrected p = 0.004), and right external capsule (corrected p = 0.015) although cross-sectional comparison with concussion patients did not identify any significant group differences at either time-point in these regions. Concussion patients were not found to have significant change in any MD region that held after Bonferroni-Holm correction.
Leveraging the extensive battery of clinical outcomes and quantitative neuroimaging data previously collected at initial evaluation in these same participants allowed us to explore what early clinical, demographic, and imaging factors best predicted 6-month outcome for an overall measure of quality of life by PedsQL and 6-month depression symptom severity by PHQ-9, which was still significantly elevated in the concussion patients at this follow-up time-point. First univariate modeling was conducted for each 6-month outcome parameter (PedsQL or PHQ-9) correlating with the initial evaluation data in those very same participants, which included concussion diagnosis, 6 demographic variables (age, height, weight, education, gender, handedness), 26 clinical outcome measures, 78 regions of FA, and the 15 primary volumetric regions adjusted for TBV. The top 12 most significant predictors by univariate analysis were then used for each outcome parameter to determine the best model subset by AIC. The top 10 prediction models for each 6-month outcome parameter are reported. Prediction of 6-month overall quality of life across the 10 models consistently identified initial concussion symptoms from the ImPACT, pediatric quality-of-life school sub-domain, and severity of depressive symptoms from the PHQ-9 with additional contribution from other quality-of-life, mental health, and sleep measures depending on the model (Table 4).
Prediction of 6-Month Follow-Up Pediatric Quality of Life (PedsQL)
Model selection was limited to the 12 best univariate predictors.
Cells report B estimate and corresponding p-value for each effect in the model.
AIC Corrected is the AIC Corrected for the small group sizes.
Interestingly, none of the demographic, cognitive performance measures, or imaging measures contributed to the top models. Prediction of 6-month depression symptom severity across the 10 different models consistently identified concussion diagnosis, initial symptoms of depression by the PHQ-9, total concussion symptoms score from the ImPACT, and difficulty getting to sleep from the ASWS with additional contribution from other measures of mental health, sleep, behavior impairment, and quality of life depending on the model (Table 5). Again, none of the demographic, cognitive performance measures, or imaging measures contributed to the top models. It should be noted that given the relatively small sample size, these regression models are likely optimistic interpretations of the best predictors and require replication in a larger cohort before they are considered fully validated.
Prediction of 6-Month Depression Symptom Severity (PHQ-9)
Model selection was limited to the 12 best univariate predictors.
Cells report B estimate and corresponding p-value for each effect in the model.
AIC Corrected is the AIC Corrected for the small group sizes.
Discussion
Overall, 10- to 14-year-old pediatric concussion patients showed evidence of improvement by 6-month follow-up suggesting active recovery primarily in domains of cognitive function and overall quality of life. In contrast, measures of psychological health were less resolved with pediatric concussion patients exhibiting sustained symptoms of depression on PHQ-9, behavior impairment on HBI-20, and concussion symptoms evidenced by the ImPACT.. Quantitative neuroimaging measures also identified measures indicative of chronic injury with regional reductions observed by both quantitative volumetric segmentation and white matter FA from DTI data. Additionally, outcome prediction of 6-month follow-up overall quality of life using the PedsQL and 6-month follow-up depression severity using the PHQ-9 identified key parameters from the initial evaluation that if validated in a larger cohort, may provide important clinical parameters to consider when determining recovery trajectory.
Further, the middle frontal gyrus, 53 superior frontal gyrus, 54 anterior cingulate cortex, 55 and cingulum 56,57 have been previously implicated as important neuroanatomical regions associated with depression and even directly targeted for therapy 53 in young adult and adolescent patients. Given that the primary domain with sustained impairment at 6-month follow-up in our pediatric sports concussion patients was depression and that the middle frontal gyrus had the greatest reductions in FA with the superior frontal gyrus trending toward significance, in addition to volumetric reductions noted in the anterior cingulate cortex, we believe these initial findings potentially support the clinical and biological relevance of these imaging applications in this patient population.
Strengths of this study include the very well-matched groups of youth concussion patients and controls, the very tight age range of evaluation (10–14 years), longitudinal evaluation at two time-points 6 months apart, and the multi-faceted approach to evaluation using clinical measures across a variety of domains of function including neuropsychological performance, sleep, quality of life, psychological health, and health behavior in addition to the advanced neuroimaging collected at each time-point of the evaluation. Limitations of the study include a very modest group size, lack of statistical power to explore higher dimensional measures, lack of utilization of the longitudinal Freesurfer pipeline for volumetric segmentation, only cross-sectional segmentation at each time-point of evaluation, and lack of baseline evaluation data prior to exposure. Additionally, we were not able to also examine those youth who recovered quickly from concussion to understand the clinical outcome and neuroimaging trajectories in this group as well. Efforts are underway to replicate these findings in a larger cohort and to expand data collection to include more comprehensive evaluation of growth and development in both genders in an attempt to appreciate what role, if any, pre- and post-pubescence 58 would have in concussion recovery in particular in female youth athletes of this younger age range.
In conclusion, longitudinal evaluation of 10- to 14-year-old youth concussion revealed considerable recovery in cognitive domains and overall quality of life from initial evaluation to 6-month follow-up, although patients exhibited sustained symptoms of depression, behavior impairment, and to a lesser extent, sleep impairment and symptoms of anxiety. Whereas prolonged symptom progression has been previously reported, 14,15 this study provides further evidence for how these symptoms evolve out to 6 months post-injury. Quantitative neuroimaging collected at both time-points revealed abnormalities consistent with the pathophysiological changes associated with brain injury suggestive of a more extended impact of these types of exposures. These findings build upon a growing body of literature that supports the hypothesis of extended brain physiological changes following sports-related concussion 13 currently unappreciated by conventional neuroimaging methods expanding these findings out to early chronic outcome in youth athletes. Given the lack of pre-injury baseline information, it is unclear if there are pre-existing conditions contributing to patient trajectories following these concussive injuries. Predictive modeling of an overall measure of quality of life as well as a measure of depression at 6-month outcome were found to consistently identify predictors in the domains of quality of life, depression, concussion symptoms, concussion diagnosis, and to a lesser extent anxiety and sleep from initial evaluation and not in any of the cognitive performance domains, demographics, or imaging. Taken together, this study supports further focus and inclusion of mental health rehabilitation with the more traditional cognitive rehabilitation strategies employed in this young athlete population.
Footnotes
Acknowledgments
We would like to thank the families, patients, and participants without whom this study would not be possible. We are grateful for the assistance of the University of Washington Diagnostic Imaging Sciences team including Serena Bennett, Tim Wilbur, and Liza Young for their support with the imaging acquisition and logistical planning. Funding for this research was provided by the Seattle Pediatric Concussion Research Collaborative.
Authors Disclosure Statement
No competing financial interests exist.