
Abstract
The aim of this study is to investigate glucose uptake on 18F-fluorodeoxyglucose positron emission tomography positron emission tomography (FDG-PET) in patients with chronic mental and cognitive symptoms following a single blunt mild traumatic brain injury (TBI) and without visible brain lesions on computed tomography (CT)/magnetic resonance imaging (MRI). Eighty-nine consecutive patients (mean age 43.8 ± 10.75 years) who had a single blunt mild TBI from a traffic accident and suffering from chronic mental and cognitive symptoms without visible brain lesions on CT/MRI were enrolled in the study. Patients underwent FDG-PET imaging, and the mean interval between the TBI and FDG-PET was 50.0 months. The Wechsler Adult Intelligence Scale version III (WAIS-III) testing was performed within 1 month of the FDG-PET. A control group consisting of 93 healthy adult volunteers (mean age 42.2 ± 14.3 years) also underwent FDG-PET. The glucose uptake pattern from FDG-PET in the patient group was compared with that from normal controls using statistical parametric mapping. Glucose uptake was significantly decreased in the bilateral prefrontal area and significantly increased around the limbic system in the patient group compared with normal controls. This topographical pattern of glucose uptake is different from that reported previously in patients with diffuse axonal injury (DAI), but may be similar to that seen in patients with major depression disorder. These results suggest that the pathological mechanism causing chronic mental and cognitive symptoms in patients with a single blunt mild TBI and without visible brain lesions might be different from that due to primary axonopathy in patients with DAI.
Introduction
The incidence of traumatic brain injury (TBI) has been estimated to be between 100–600/100,000 per year. 1 –5 In the United States, more than 2 million people experience TBI each year, and more than 1.5 million of these people do not require hospitalization because their injuries are considered “mild.” 6 Many clinical studies categorize the severity of TBI (mild, moderate, and severe) according to the classification established by the American Congress of Rehabilitation Medicine (ACRM) or World Health Organization (WHO) Collaborating Center Task Force. 7,8 These classifications are based on the Glasgow Coma Scale (GCS) score assessed in the acute phase, and are clinically useful in predicting prognosis roughly. However, especially in cases of mild TBI, a long-term prognosis cannot be estimated precisely using this classification in the acute phase. 9
In the United States, about 75% of patients with TBI correspond to mild TBI, and approximately 30% of mild TBI patients suffer chronic symptomatic sequelae for months to years, which is unexpected with respect to the GCS score from the acute phase. 10 Among such patients, there are a substantial number who did not receive any administrative welfare or medical services. 9 One possible reason for this lack of medical care is that the symptoms may be caused by the presence of minute traumatic brain lesions, which may be overlooked or underestimated over time. However, minute traumatic brain lesions have not been examined in patients with chronic symptoms following mild TBI. Thus, it is important to investigate the relationship between the presence of minute brain lesions and the severity of chronic clinical symptoms.
Generally, it is difficult to distinguish minute traumatic brain lesions on structural imaging modalities such as conventional magnetic resonance imaging (MRI) and computed tomography (CT) in the chronic phase. Alternatively, sophisticated acquisitions such as T2*-weighted imaging (T2*WI), susceptibility-weighted imaging (SWI), and fractional anisotropy images analyzed by statistical parametric mapping (FA-SPM imaging) derived from diffusion-weighted imaging are able to detect these lesions more easily. 11 –15 However, minute brain lesions are not always detectable even with such sophisticated imaging techniques. In the majority of patients with mild TBI, no brain lesions are detectable with CT or MRI. In metabolic investigations of the brains of patients with TBI, positron emission tomography (PET) and single photon emission computed tomography (SPECT) have played an important role as supplementary imaging to detect minute brain lesions. 16 –22 In particular, PET can assess glucose metabolic uptake in addition to blood flow, and provides more precise localized information and higher spatial resolution images than SPECT. 23
We identified only four previous reports of PET studies with 18F-fluorodeoxyglucose (FDG) in patients with blunt mild TBI using semi-quantitative image analysis. 24 –27 However, because these studies enrolled a relatively small number of patients, the reliability of the results may be reduced.
The aim of this study was to investigate glucose uptake on FDG-PET in a substantial number of patients with chronic mental and cognitive symptoms following a single blunt mild TBI without visible brain lesions on CT/MRI. In addition, we examined the relationship between FDG-PET uptake abnormalities and cognitive dysfunction.
Methods
Subjects
Eighty-nine consecutive patients (mean age, 43.8 ± 10.75 years; range, 22–69 years; 39 males and 50 females) with blunt mild TBI due to a single traffic accident, who were referred to Kizawa Memorial Hospital from March 2012 to February 2016 with the aim of neuropsychological testing and neuroimaging of their post-traumatic mental/cognitive sequelae, were enrolled in this study. All subjects had been diagnosed with mild TBI according to the criteria of ACRM 7 at a primary hospital during the acute phase, and had no history of intracranial or peripheral surgery, penetrating head injury, open skull fracture, neurological disease unassociated with injury, mental retardation, psychiatric disease, or alcohol or substance abuse prior to the TBI. An MRI, including T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), T2*WI, fluid attenuated inversion recovery imaging (FLAIR), SWI, and FA-SPM imaging, and an FDG-PET were performed at that time. The mean interval between the TBI and the neuroimaging was 50.0 months (range, 6.3–122.8 months). No visible brain lesions could be distinguished on MRI in any patient. Subjects underwent the Wechsler Adult Intelligence Scale version III (WAIS-III) including FIQ (Full Intelligence Quotient), VIQ (Verbal Intelligent Quotient), and PIQ (Performance Intelligence Quotient) 28 testing as a neurocognitive examination within 1 month of the FDG-PET. The chronic mental/cognitive symptoms that were described by the patients included disturbances in memory (94.4%), attention (96.6%), execution (87.6%), emotion (76.4%), and behavior (94.4%).
For the control group, 93 healthy adult volunteers (mean age, 42.2 ± 14.3 years; 52 males and 41 females) also underwent FDG-PET imaging. All patients and healthy volunteers had a minimum education level of graduation from high school.
The study was approved by the institutional research ethics committee of Kizawa Memorial Hospital and was in accordance with the Declaration of Helsinki. All subjects provided informed written consent.
FDG-PET
The PET scanner used in this study was an Eminence STARGATE (Shimadzu Corporation, Kyoto, Japan), which provides 99 transaxial images at 2.65-mm intervals. The in-plane spatial resolution (full width at half maximum) was 3.5 mm. The scan mode was the standard three-dimensional mode. Participants were placed in the PET scanner so that slices were parallel to the canthomeatal line. Participants fasted for at least 4 h prior to injection of FDG (3.5 MBq/kg injected intravenously through the cubital vein over 1 min). The participants were seated comfortably with eyes open and environmental noises were kept to a minimum for 45 min, after which a cesium-137 rotating pin source was used to obtain a 4-min transmission scan, followed by a 10-min acquisition scan. FDG-PET images were reconstructed with attenuation correction using data from the transmission scans, dead time, random, and scatter.
Statistical analysis
FDG-PET images were processed using MATLAB software (Mathworks, Inc., R2017a, Natick, MA) and SPM V.12 software (Wellcome Department of Imaging Neuroscience, London, UK;
When the difference of FDG uptake between the patient and normal control groups in a cluster was significant, receiver operating characteristic (ROC) analysis was performed for evaluating the sensitivity, specificity, accuracy, and area under the curve (AUC) in the peak voxel of the clusters using R software (version 3.4.0) for distinguishing the two groups.
Finally, multiple regressions were performed between PET data from patients and their WAIS scores with proportional scaling, a brain mask of 0.8 mean intensity, and significance thresholds of both the voxel (an uncorrected voxel-wise threshold of p < 0.001) and cluster level (extent threshold of 60 voxels). To visualize the SPM t-map, significant voxels in each analysis were projected on to the render file (render_spm96.mat) in three orthogonal projections implemented in SPM12.
Results
WAIS-III scores
Cognitive dysfunction of the patient group was measured by WAIS-III scores (85.7 ± 17.35 for the FIQ, 87.7 ± 15.63 for the VIQ, and 85.5 ± 18.72 for the PIQ; mean ± standard deviation).
FDG-PET uptake in patients
FDG uptake was significantly decreased in the whole bilateral prefrontal areas in the patient group compared with the normal control (Fig. 1). FGD uptake was significantly increased in the bilateral temporal lobes including bilateral parahippocampal gyri, bilateral cingulate gyri, and brainstem, which mostly correspond to the limbic system, in the patients group compared with the normal control (Fig. 2).
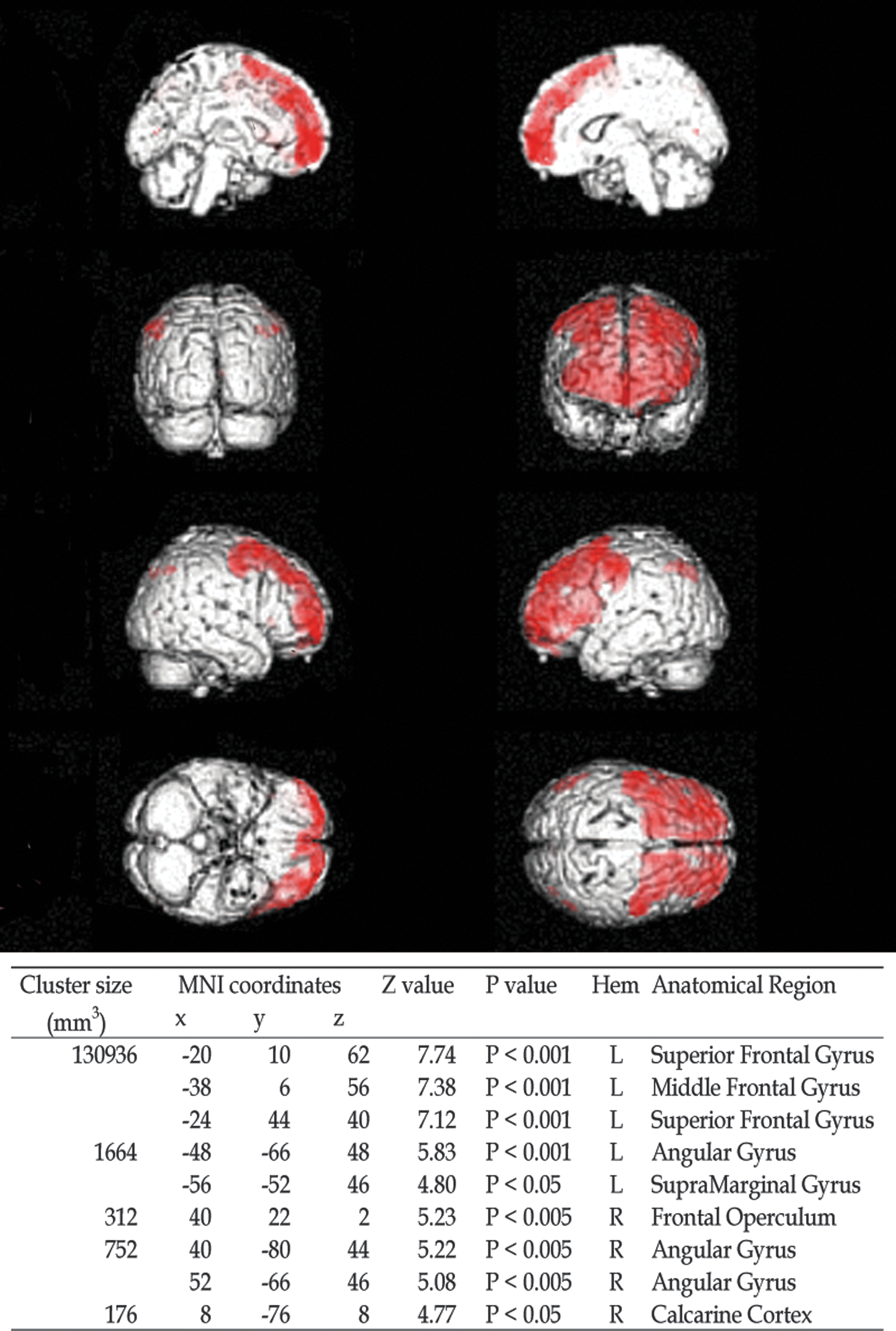
Brain regions (red) in which FDG uptake was decreased significantly in the patient group compared with the normal control are shown. These regions correspond to the whole bilateral prefrontal areas. There were 9 peak voxels in the clusters with significant decrease of FDG uptake. Hem, hemisphere; MNI, Montreal Neurological Institute.

Brain regions (red) in which FDG uptake was increased significantly in the patient group compared with the normal control are shown. These regions were the bilateral temporal lobes including bilateral parahippocampal gyri, bilateral cingulate gyri, and brainstem, which mostly correspond to the limbic system. There were 10 peak voxels in the clusters with significant increase of FDG uptake. Hem, hemisphere; MNI, Montreal Neurological Institute.
ROC analysis for differentiating patients from normal control
Table 1 shows the ROC curves for differentiating patients from the normal control. There were 9 peak voxels (2 voxels each in the left superior frontal gyrus and right angular gyrus, and 1 voxel each in the left middle frontal gyrus, left angular gyrus, left superior marginal gyrus, right frontal operculum, and right calcarine cortex) in the clusters in which FDG uptake was significantly decreased in the patient group compared with the normal control. The ranges were 0.652–0.924, 0.292–0.584, 0.597–0.635, and 0.578–0.623 in the sensitivity, specificity, accuracy, and AUC, respectively. There were 10 peak voxels (2 voxels in the right anterior cingulate gyrus, and 1 voxel each in the left parahippocampal gyrus, left brainstem, left posterior cingulate gyrus, right middle temporal gyrus, right posterior cingulate gyrus, right precuneus, right middle cingulate gyrus, and right caudate) in the clusters in which FDG uptake was significantly increased in the patient group compared with the normal control. The ranges were 0.270–0.438, 0.739–0.989, 0.580–0.652, and 0.540–0.597 in the sensitivity, specificity, accuracy, and AUC, respectively.
ROC Analysis in the Peak Voxels for Differentiating Patients from Normal Control
AUC, area under the curve; MNI, Montreal Neurological Institute; mTBI, mild traumatic brain injury.
Correlations between glucose uptakes and WAIS-III scores
The region with a significantly positive correlation between FDG uptakes and FIQ score was the left middle frontal gyrus, and that between FDG uptake and VIQ score was also the middle frontal gyrus (Fig. 3). There was no significant positive correlation between FDG uptake and PIQ score.

The region (red) with a significantly positive correlation between FDG uptakes and Full Intelligence Quotient (FIQ) score was the left middle frontal gyrus and that between FDG uptake and Verbal Intelligent Quotient (VIQ) score was also the middle frontal gyrus in the patient group. Hem, hemisphere; MNI, Montreal Neurological Institute.
The region with a significantly negative correlation between FDG uptake and PIQ score was the right parahippocampal gyrus (Fig. 4). There was no significant negative correlation between FDG-PET uptake and the FIQ or VIQ scores.

The region (red) with a significantly negative correlation between FDG uptake and Performance Intelligence Quotient (PIQ) score was the right parahippocampal gyrus in the patient group. Hem, hemisphere; MNI, Montreal Neurological Institute.
Discussion
The advancement and propagation of imaging technologies for CT and MRI have led to a recent rapid progress toward more precise evaluation of brain pathology after trauma. However, disappointingly, visible brain lesions are not apparent on CT or MRI in the majority of patients with a single blunt mild TBI suffering from chronic post-traumatic mental and cognitive symptoms. The pathology responsible for these chronic symptoms has not yet been identified, except for chronic traumatic encephalopathy (CTE), which is a progressive tauopathy seen in patients with repeated mild TBI. 29 The pathological mechanism of blunt mild TBI is regarded commonly as cerebral concussion, a mild type of diffuse brain injury (DBI), which is due to shearing stress in the brain from acceleration impact. As such, there should exist some type of organic brain lesion or axonopathy in the same regions as diffuse axonal injury (DAI), a severe type of DBI due to the same mechanism. 30 –32 However, we do not know why organic brain lesions are rarely visible on CT or MRI in patients with chronic mental and cognitive symptoms following a single blunt mild TBI.
In many previous brain FDG-PET studies in patients with chronic mental and cognitive symptoms and/or disturbance of consciousness from DAI, consistent lower uptake in the cingulum, medial prefrontal regions, frontal base, and medial thalamus has been demonstrated. 18,21,22,33 –35 These brain regions are thought to be the most vulnerable to DAI. However, according to the following studies, in a small number of patients with chronic mental and cognitive symptoms from TBI but without visible brain lesions on CT or MRI, the possibility that other brain regions may be responsible for the symptoms has been suggested.
There are three previous clinical studies using FDG-PET to assess patients with chronic mental and cognitive symptoms due to blunt mild TBI. One is the study by Chen and colleagues, 24 in which no significant differences in regional FDG uptake in the frontal and temporal regions of 5 mildly injured patients with chronic symptoms were revealed compared with controls. Ito and associates 26,27 studied cerebral glucose uptake in 40 patients with mild/moderate TBI, including 16 patients with mild TBI, without visible brain lesions on MRI, and the results were consistent with those reported by Chen and colleagues. A study by Mendez and co-workers, 25 indicated hypometabolism in the left inferior frontal or Broca's area, the left medial anterior temporal region, the inferolateral anterior temporal regions, the left posterior cingulate, and the left thalamus in 12 patients with blunt mild TBI compared with controls. These three studies were performed with a small number of patients and, therefore, the reliability may not be high. Nevertheless, the topographical pattern of brain hypometabolism of patients with mild TBI in these studies was somewhat different from that which has been reported in patients with DAI. However, the great majority of these DAI patients have visible brain lesions on CT or MRI even in the chronic phase.
In this study, we also investigated differences in FDG uptake in patients with chronic symptoms after a single blunt mild TBI without visible brain lesions on CT or MRI compared with normal controls. To obtain reliable results on statistical analysis of imaging, 89 patients were enrolled. Our results indicate that glucose uptake was significantly decreased primarily in the entire bilateral prefrontal area in patients compared with normal controls. This topographical pattern of decreased uptake is somewhat different from that reported in patients with DAI. 18,20,33 –35 These results complement the findings from the studies by Chen and colleagues, Mendez and co-workers, and Ito and associates, 24 –27 and suggest that there may be other pathological mechanisms that cause chronic post-traumatic mental and cognitive symptoms in patients with a single blunt mild TBI and without visible brain lesions that are different from DAI.
In DAI, visible lesions from axonal injury may cause disruptions in communication between the cerebral neocortex, basal ganglia, and the limbic system. In these cases, as mentioned above, the reported hypometabolic regions include the cingulum, the medial prefrontal regions, the medial inferior frontal regions, and the medial thalamus. 18,20,33 –35 These hypometabolic regions are thought to be secondary lesions of functional damage from the disruption of information transmission by injured axons rather than primary lesions, and are presumed to result in the chronic neurological symptoms.
On the other hand, the pattern of the hypometabolism in the entire prefrontal area, as observed in our symptomatic patients, is more similar topographically to the hypometabolism seen in patients with major depression disorder rather than that reported for DAI. 36 –38 Further, the finding that glucose uptake was increased around the limbic system in patients compared with controls may suggest a compensatory response to the hypometabolism of the prefrontal area, which is also similar to that recognized in major depression disorder. 39 This compensatory glucose uptake response is also similar to that found with other common neuropsychiatric diseases such as bipolar disorder and schizophrenia. 40 –46 From this perspective, the pathological mechanism responsible for mental and cognitive symptoms in our patients may be hypothesized as related to the monoamine hypothesis, which has been advocated classically as a cause of common neuropsychiatric diseases rather than axonopathy due to primary organic brain damage as seen in DAI. 47 –51 However, the hypothesized pathological mechanism for blunt mild TBI without visible brain lesions is likely to be a secondary pathology in the whole bilateral prefrontal areas led by the primary mechanical traumatic damage in other brain regions related to the monoamine activating system. This mechanism may be different from the pathological mechanism hypothesized for primary functional disorders of monoamine in the brain, which has been suggested in common neuropsychiatric diseases.
Further research is needed to elucidate the specific pathological mechanism leading to such metabolic malfunction in the brain of patients with a single mild TBI without visible brain lesions and having chronic mental and cognitive symptoms.
Conclusion
Glucose uptake on FDG-PET was decreased significantly primarily in the bilateral prefrontal area and increased significantly around the limbic system in patients with chronic mental and cognitive symptoms following a single blunt mild TBI without visible brain lesions on CT or MRI compared with normal controls. This topographical pattern of the FDG-PET uptake was different from that seen in patients with DAI, but was rather similar to that observed often in patients with major depression disorder. Our results suggest that the pathological mechanism causing mental and cognitive symptoms in such patients with blunt mild TBI may be different from that due to primary axonopathy in patients with DAI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Acknowledgments
The authors would like to thank Ms. Hibino and Ms. Nishibu for support with the neuropsychological examinations.