
Abstract
Characterizing psychological factors that contribute to persistent symptoms after mild traumatic brain injury (MTBI) can inform early intervention. To determine whether fear avoidance, a known risk factor for chronic disability after musculoskeletal injury, is associated with worse clinical outcomes from MTBI, adults were recruited from four outpatient MTBI clinics and assessed at their first clinic visit (mean = 2.7, standard deviation = 1.5 weeks post-injury) and again four to five months later. Of 273 patients screened, 102 completed the initial assessment, and 87 returned for the outcome assessment. The initial assessment included a battery of questionnaires that measure activity avoidance and associated fears. Endurance, an opposite behavior pattern, was measured with the Behavioral Response to Illness Questionnaire. The multi-dimensional outcome assessment included measures of post-concussion symptoms (British Columbia Postconcussion Symptom Inventory), functional disability (World Health Organization Disability Assessment Schedule-12 2.0), return to work status, and psychiatric complications (MINI Neuropsychiatric Interview). A single component was retained from principal components analysis of the six avoidance subscales. In generalized linear modeling, the avoidance composite score predicted symptom severity (95% confidence interval [CI] for B = 1.22–6.33) and disability (95% CI for B = 2.16–5.48), but not return to work (95% CI for B = −0.68–0.24). The avoidance composite was also associated with an increased risk for depression (odds ratio [OR] = 1.76, 95% CI = 1.02–3.02) and anxiety disorders (OR = 1.89, 95% CI = 1.16–3.19). Endurance behavior predicted the same outcomes, except for depression. In summary, avoidance and endurance behavior were associated with a range of adverse clinical outcomes from MTBI. These may represent early intervention targets.
Introduction
A
Cognitive-behavioral models have been developed for chronic pain after musculoskeletal injury, 19 daily headache, 20 chronic fatigue syndrome, 21 chronic subjective dizziness, 22 and medically unexplained symptoms 23,24 — all health conditions with clinical features that resemble chronic MTBI. Integral to each of these models is the role of fear-based activity avoidance. Patients tend to restrict what they do or modify how they do it to prevent physical or psychological discomfort. This fear avoidance predicts chronic disability. 25 –27
Little is known about the role of avoidance behavior in recovery from MTBI. A few studies have administered generic stress coping scales and reported inconsistent associations between avoidant coping and MTBI outcome. 14,28 –30 One previous study 31 reported that “limiting behavior” (a low level of activity after injury) in the first two weeks post-MTBI was not predictive of post-concussion symptom status three or six months later. Borrowing from the concept of “cogniphobia” in the chronic daily headache literature, 32 we found recently that fear of mental exertion inducing headaches after MTBI is associated with reduced memory performance and other forms of avoidance behavior. 33
Endurance behavior, characterized by a cycle of persisting with activities despite symptom exacerbation and then “crashing” with recuperative rest, 31 may also be problematic. This coping style can be considered the polar opposite of fear avoidance. Endurance behavior represents another pathway to chronic disability in contemporary models of chronic pain 34 –37 and fatigue. 38 Psychometric measures of avoidance and endurance behavior tend to be minimally or negatively correlated. 35,37,39 In one MTBI study, endurance behavior predicted chronic symptoms at follow-up. 39 This finding has not been replicated, nor have other potential consequences of endurance behavior been examined.
The primary aim of the present study is to characterize fear avoidance after MTBI and examine its relationship with a panel of clinical outcomes. Because there is no established measure of fear avoidance in MTBI, we administered several avoidance scales developed for other health conditions and attempted to extract a unidimensional composite score. We hypothesized that fear avoidance would be associated with later disability and work status, and an increased risk of psychiatric complications. It is less clear whether avoidance should be expected to predict post-concussion symptoms. If activity avoidance is effective for keeping symptoms at bay, patients who are inactive may experience fewer post-concussion symptoms. Avoidance might actually worsen symptoms through mechanisms such as deconditioning, however. 40 We also measured endurance behavior and hypothesized that it would not be associated with fear avoidance, but would independently predict clinical outcomes.
The present study reports on a sample of individuals seeking care for MTBI in outpatient clinics. Patients seen in this setting are more likely to have adverse psychological risk profiles in comparison with patients recruited from consecutive emergency department visits. 41
Methods
Participants were recruited from four outpatient MTBI clinics in the greater Vancouver (Canada) area between March 2015 and February 2017. Consecutive participants were approached in person by clinic staff and asked if they would be willing to be contacted by the research team. Those who agreed to be contacted were screened for eligibility. Eligibility criteria were: (1) 18–65 years old, (2) sustained an MTBI by the World Health Organization Neurotrauma Task Force operational definition 42 within the past six months, (3) fluent in English, and (4) employed before injury. The University of British Columbia Behavioral Research Ethics Board, the Vancouver Coastal Health Research Institute, and the Fraser Health Research Institute all provided ethics approval for this study.
Participants were recruited at the time they presented to the clinic and invited to complete an in-person assessment that included a structured interview of demographics (e.g., education level) and the index injury (e.g., loss of consciousness and co-occurring orthopedic injury). The predictor variables were also obtained in the initial in-person assessment. Participants were then asked to complete a follow-up outcome assessment by telephone four to five months later. Figure 1 shows a summary of participant flow through the study.
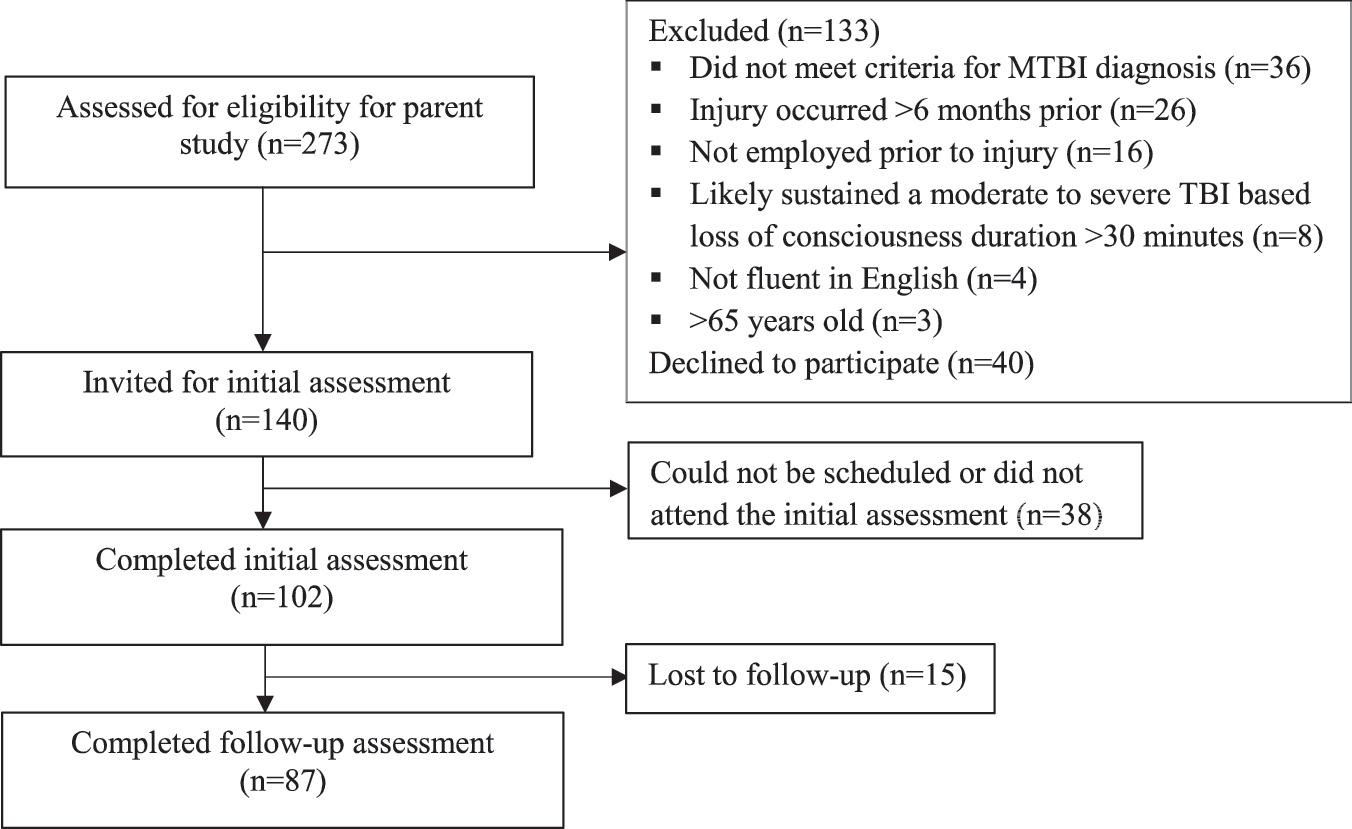
Participant flow through the study.
Predictors
Fear Avoidance Behavior Questionnaire (FABQ)
The FABQ was developed originally for workers with low back pain. 43 We modified this questionnaire for MTBI by replacing “back” with “brain” and “pain” with “symptoms.” A two-factor solution (“physical” and “work”) best fit the derivation sample, but some studies have supported a three-factor solution, 44 –46 that comprised “physical activity avoidance” (items 2–5), “work as a cause” of current symptoms (items 6, 7, 10, and 11), and “return to work readiness/prognosis” (items 12–16). The item content of the FABQ-Physical activities and FABQ-Work readiness subscales reflect the construct of interest in this study. Cronbach alpha was 0.713 for FABQ-Physical activities and 0.866 for FABQ-Work readiness in the present sample.
Behavioral Responses to Illness Questionnaire (BRIQ)
This multi-dimensional questionnaire measures illness coping behaviors associated with the development of persistent medically unexplained symptoms. 47 Two subscales from the BRIQ were administered in this study. The BRIQ-Limiting scale measures a tendency to rest excessively to facilitate recovery (Cronbach alpha = 0.821). The BRIQ All-or-nothing scale measures endurance behavior—i.e., a pattern of overdoing things to the point of feeling worse, after a period of recuperative rest (Cronbach alpha = 0.850 in the present sample).
Cogniphobia Scale
The 19-item cogniphobia scale modified by Suhr and Pickard 32 consists of two subscales that measure avoidance of mental exertion to prevent headaches (Cogniphobia-Avoidance) and beliefs that mental effort/headaches are dangerous (Cogniphobia-Dangerousness). Cronbach alpha for these subscales in the present sample were 0.888 and 0.860, respectively.
PTSD Checklist-5 (PCL-5)
The PCL-5 elicits severity ratings for symptoms of Post-traumatic Stress Disorder. 48 A two-item subscale within the PCL-5 (Cronbach alpha of 0.768 in the present sample) queries avoidance of thinking or being reminded of the stressful experience.
Medical Symptom Validity Test (MSVT) 49
The MSVT was designed to be sensitive to motivational factors but not the effects of traumatic brain injury (TBI) or genuine memory impairment. 50 –52 The “easy” subtests (Immediate Recognition, Delayed Recognition, and Consistency) have evidenced-based cutoffs for identifying cases with probable invalid responding.
This battery yielded a total of six avoidance-related measures and one measure of endurance behavior (BRIQ All-or-nothing). These measures were then used to predict future clinical outcomes, described below.
Outcomes
British Columbia Postconcussion Symptom Inventory (BC-PSI) 53
The BC-PSI measures post-concussion symptoms. Participants rated the frequency and intensity with which they have experienced the physical, cognitive, and emotional symptoms that comprise the International Classification of Disease-10 diagnostic criteria for Postconcussional Syndrome. The BC-PSI has strong psychometric properties in MTBI. 54 –56
World Health Organization Disability Assessment Schedule (WHODAS) 2.0
The WHODAS is a disease nonspecific measure of functional disability that covers the activity and participation domains including cognition, mobility, self-care, interpersonal functioning, life activities, and participation. 57 The WHODAS has been used widely in health research 58 and validated recently in mild TBI (mTBI), with an overlapping sample with the present study. 59 We administered the 12-item interview version and calculated a total score using the simple scoring method (sum of item scores).
Return to work (RTW)
Based on a structured interview, participants were determined to have a full RTW if they reported returning to the same job, with the same work hours and responsibilities. Participants who were not working were asked whether their work leave was primarily because of problems associated with the mTBI or other factors.
Psychiatric complications
A trained research assistant administered a structured psychodiagnostic interview based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders—the mood, anxiety, and substance modules of the MINI Neuropsychiatric Interview 60,61 version 6.0—under the supervision of a licensed psychologist. Major Depressive Disorder was coded as present for participants who met criteria for a current Major Depressive Episode. Participants who met criteria for PTSD, Generalized Anxiety Disorder, Panic Disorder, Social Anxiety Disorder, or Obsessive-Compulsive Disorder were coded as present for any anxiety disorder.
Analysis
Group differences were assessed with independent samples t tests (for continuous variables) or chi square tests (for proportions), and correlations with Pearson r. Continuous variables analyzed with t tests or Pearson r were approximately normally distributed. A principal components analysis (PCA) reduced the six avoidance measures into a composite score. Preliminary screening for missing data revealed that of the 102 participants who completed the initial assessment, four were missing data for at least one entire questionnaire and six were missing exactly one item from one questionnaire. These six missing item values were imputed with the mean of that participant's other item scores from the particular subscale. PCA was therefore performed on 98 cases.
The prognostic analyses were conducted with generalized linear modeling. A response family (with canonical link function) was chosen for each model based on the distribution of the outcome variable. We checked for improved model fit, operationalized by the Bayesian Information Criterion, by considering alternative response families or link functions. In an initial step (unadjusted modeling), the two main predictors of interest (PCA-derived composite score of fear avoidance and BRIQ All-or-nothing scale total score) were entered into each model as covariates. In a second step (adjusted modeling), additional covariates were entered into each model to control for potential confounding.
Of the 87 cases with outcome data, PCA composites were available for 84. Of those 84, one participant did not complete the BC-PSI. There were no missing data for the other outcomes. RTW was initially coded dichotomously as return to the same job, with the same hours and responsibilities (n = 37) versus incomplete (i.e., partial or no) RTW (n = 50). We then created an ordinal RTW variable by (1) separating out cases with partial RTW (n = 13; i.e., reduced hours or responsibilities) from no RTW cases into a third (middle) category, (2) re-categorizing participants who reported a full RTW but ongoing productivity loss (total score >10 on the Lam Employment Absence and Productivity Scale, 62 n = 9) into the partial RTW group based on our previous research with this sample illustrating that participants with full RTW after mTBI often have reduced productivity at work, 63 and (3) excluding participants who had not returned to work for reasons other than mTBI (n = 11). This yielded full (n = 28), partial (n = 25), and no RTW (n = 23) groups.
Results
Sample characteristics
The initial evaluation occurred at mean (M) = 2.7 (standard deviation [SD] = 1.5) months post-injury (at clinic intake), and outcomes were assessed at M = 7.3 (SD = 1.4) months post-injury. Participant characteristics are presented in Table 1.
M, mean; SD, standard deviation; FABQ, Fear Avoidance Behavior Questionnaire; BRIQ, Behavioral Responses to Illness Questionnaire; PCL, PTSD Checklist; MSVT, Medical Symptom Validity Test; BC-PSI, British Columbia Postconcussion Symptom Inventory; WHODAS, World Health Organization Disability Assessment Schedule.
N = 102 for baseline variables and N = 87 for outcomes.
N = 84.
“Indigenous” refers to Indigenous ancestry, including First Nations (North American Indian), Métis, and Inuit.
Participants who were lost to follow-up (n = 15) did not differ from participants who completed follow-up (n = 87) with respect to age, sex, education, ethnicity, or any of the predictor variables (p > 0.05).
Derivation of an Avoidance Composite Score
We derived a composite avoidance score by submitting the six avoidance scales (FABQ-Physical activities, FABQ-Work readiness, BRIQ Limiting, and Cogniphobia-Avoidance, Cogniphobia-Dangerousness, and PCL-5 Avoidance) to PCA and retaining one component. There was sufficient common variance among the avoidance scales for PCA (Kaiser-Meyer-Olkin = 0.767; Bartlett test, chi square [15] = 161.99, p < 0.001). All communalities were greater than 0.40 except for FABQ-Work Readiness (0.38) and PCL-5 Avoidance (0.36). The one extracted component (Eigenvalue = 2.91) explained 48.5% of the variance in the six avoidance scales, with item loadings ranging from 0.597 to 0.850. A second component (Eigenvalue = 0.94) could explain an additional 15.6% of variance but was difficult to interpret even with (Direct Oblimin) rotation and had high cross-loadings with the first component, and so was not retained. Further supporting a unidimensional structure, Cronbach alpha for the first component score was 0.750 and could not be improved by deleting any contributing scale.
The avoidance composite and measure of endurance behavior (BRIQ All-nothing scale) were not significantly correlated, r(98) = 0.156, p = 0.126. The avoidance composite score was not associated with age (r[98] = −0.05, p = 0.655) or sex (t[96] = −1.08, p = 0.281), but was significantly correlated with lower education (r[98] = −0.31, p = 0.002). Compared with participants who denied loss of consciousness, participants with witnessed (t[65] = 0.701, p = 0.486), suspected (unwitnessed) (t[68] = −0.392, p = 0.696), or unknown loss of consciousness (t[56] = 0.250, p = 0.803) scored similarly on the avoidance composite. The avoidance composite was also not related to post-traumatic amnesia (p > 0.05 for all comparisons). Sustaining a comorbid orthopedic injury was not significantly associated with greater avoidance (t[96] = 1.62, p = 0108). Participants with suspected symptom invalidity (performed below evidence-based cutoffs on the MSVT) had higher scores on the avoidance composite (t[96] = −4.04, p < 0.001, Cohen d = 0.96).
Prediction modeling
We fit a generalized linear model for each outcome, with two predictors, the avoidance composite and the BRIQ All-or-nothing scale. The omnibus model test and parameter estimates for each model are presented in Table 2.
BC-PSI, British Columbia Postconcussion Symptom Inventory; WHODAS, World Health Organization Disability Assessment Schedule; MINI, MINI psychiatric interview.
The avoidance composite predicted post-concussion symptom severity (BC-PSI) and disability (WHODAS). Participants scoring high on the avoidance composite were also more likely to meet diagnostic criteria for major depression and an anxiety disorder at follow-up. The associated ORs for these psychiatric complications were 1.76 (95% CI = 1.02–3.02) and 1.89 (95% CI = 1.16–3.19), respectively. Avoidance did not significantly predict RTW status, whether RTW was operationalized as a binary or ordinal variable. Endurance behavior (BRIQ All-or-nothing scale) similarly predicted post-concussion symptoms and disability, but was somewhat less strongly predictive of psychiatric complications.
To control for the potential confound of symptom overreporting explaining high scores on both the predictors and outcomes, we added a binary measure of symptom validity to these models (passed vs. failed the MSVT). Education level was also included in these models because it was associated with avoidance behavior in the present sample (see above) and with clinical outcome in previous mTBI prognostic studies, 11,14 and so may be another confound. The results of the confound-adjusted generalized linear modeling are also presented in Table 2. Performance validity predicted disability (WHODAS) but no other outcomes. Education level was not independently associated with any outcome. The coefficients for avoidance and endurance are modestly attenuated but still significant in most adjusted models. There was one exception. Avoidance predicted depression in the unadjusted model, but was a nonsignificant predictor in the adjusted model (p = 0.206), where there was a trend for education to predict depression (p = 0.078).
Development of a Brief Avoidance Scale for future research
It would be impractical to administer six avoidance scales (total = 44 items) in future research. We therefore created a short form avoidance scale by selecting all items that correlated >0.5 with the composite score and recoding them on the same 0–4 response scale. The BRIQ Limiting scale and PCL-5 already use a five-point rating scale, but item levels had to be collapsed for the other avoidance scales. The FABQ is rated on a seven-point scale; ratings of 0–1 were recoded as 0 and ratings of 5–6 were coded as 4. Cogniphobia Scale items are rated on a four-point scale. Ratings of 1, 2, 3, and 4 were assigned values of 0, 1, 3, and 4, respectively.
The 12 items shown in Table 3 correlated most strongly with the PCA-derived composite score (i.e., met the r > 0.5 criterion for selection). The summed score for these 12 items (M = 25.2, SD = 9.5, range = 5–48) had high internal consistency (Cronbach alpha 0.862) and a very strong correlation with the composite score (r = 0.91). Item characteristics are reported in Table 3.
FABQ, Fear Avoidance Behavior Questionnaire; BRIQ, Behavioral Responses to Illness Questionnaire; PCL, PTSD Checklist.
Note: Original response options were aCompletely disagree (0) to Completely agree (6), bNot at all (1) to Every day (5), cStrongly disagree (1) to strongly agree (4), and dNot at all bothered (0) to Extremely bothered (4). Recoded responses range from 0 to 4 for all scales.
Discussion
Fear avoidance has been established as a maladaptive form of coping with body pain, 19 headaches, 20 fatigue, 21 dizziness, 22 and anxiety, 64 but has scarcely been studied in mTBI. Endurance behavior, a cycle of overexertion and recuperation, may represent an alternative pathway to chronic disability after injury 34 –38 and has been shown previously to have prognostic value for chronic symptoms after mTBI. 31 We comprehensively assessed fear avoidance in a treatment-seeking mTBI cohort and examined its associations with a panel of clinical outcomes.
Fear avoidance and endurance behavior assessed at outpatient clinic intake predicted both symptoms and disability months later. These maladaptive coping styles were also associated with increased risk for having an anxiety disorder at follow-up. Fear avoidance heightened the risk for depression at follow-up, but not after controlling for potential confounds (level of education and symptom invalidity). Neither fear avoidance nor endurance behavior predicted RTW status, even when we reclassified participants who reported fully returning to work but had evidence of reduced work productivity. The influence of factors separate from mTBI (e.g., availability of workplace accommodations) may have weakened the association between symptom coping variables and RTW.
Avoiding strenuous activity in the 48 h after mTBI is probably adaptive, after which point gradual activity resumption is advised. 40,65,66 The present findings suggest that patients who do not follow the usual transition from avoidance to approach behavior are at risk for adverse outcomes. There are several possible mechanisms through which ongoing activity avoidance might perpetuate so-called post-concussion symptoms. Avoiding headache triggers may eventually result in sensitization such that triggers more easily provoke headaches. 67 Avoiding movement limits opportunities to habituate the vestibular system in patients with dizziness. 22 Inactivity may result in physiological deconditioning and, in turn, fatigue and other concussion-like symptoms. 19,40 Avoiding aversive thoughts or emotions can contribute to psychopathology. 64,68
The origins of fear avoidance after mTBI are unclear. Fear avoidance is rooted in cause-effect beliefs about the unpleasantness or dangerousness of engaging in certain activities or exposure to certain stimuli, and can emerge through classic conditioning. 69 The conditioned response (escape or avoidance) occurs in anticipation of an unconditioned stimulus. 69 In chronic pain, for example, fear of pain or reinjury is typically the unconditioned stimulus. 27 The unconditioned stimulus in mTBI may be analogous. Soon after mTBI, symptoms can worsen with physical or mental exertion. 70 Activity-related symptom exacerbations have been illustrated in observational clinical studies 71,72 and laboratory settings. 73 –76 It is therefore not difficult to imagine how early attempts to increase activity might reinforce avoidance behavior. Other unconditioned stimuli are possible. For example, patients may fear re-injury and unduly restrict their activities to mitigate this possibility. Cognitive failures may elicit another type of unconditioned stimulus, the social embarrassment or threat to one's ego induced by a cognitive failure, leading to hyperawareness of reduced competency, anxiety, and avoidance of cognitively demanding activities. 77 –79
In summary, avoidance behavior after mTBI may be motivated by fear of post-concussion symptoms themselves and/or a host of other feared anticipated consequences of resuming usual pre-injury activities. Interestingly, fear avoidance was associated with lower education in this study, raising the possibility that low health literacy may facilitate maladaptive illness beliefs and coping.
Endurance behavior independently predicted post-concussion symptom severity at follow-up, consistent with one previous study. 31 Endurance behavior also predicted disability outcomes and anxiety disorder diagnosis in our study. Endurance behavior was not significantly correlated with the avoidance composite (r = 0.16), consistent with the Avoidance-Endurance Model in chronic pain, 34 –37 which posits that there is a subgroup of fear avoidant patients and a distinct subgroup of patients who repeatedly “overdo it,” where both of these subgroups are at elevated risk for chronic disability. Chronic pain researchers advocate different treatment approaches for avoidance and endurance subtypes. 80 –84 Exposure-based treatment that targets fear of movement is best suited to the avoidance subtype, whereas pacing is appropriate for the endurance subtype. 83,85 –87 This treatment-matching principle may represent an important direction for future research in mTBI.
Limitations
The study design does not allow us to draw conclusions about causality. It is possible that some patients restricted their activities to a greater degree because their condition was more severe. We found, however, that avoidance behavior was unrelated to indicators of brain injury severity or comorbid orthopedic injury. Second, with only one early time point, we could not uncover the inflection point at which avoidance becomes maladaptive (“too much” for “too long”). Interestingly, one previous study 31 assessed activity restriction (with the BRIQ Limiting scale) soon after mTBI (“within two weeks”) and found no association with symptom status months later, whereas another recent study measured these same variables at an average of three years post-MTBI and found a significant association. 88 This pattern of findings is consistent with our theory-driven hypothesis that fear avoidance may be adaptive initially but become maladaptive if it persists.
Third, we found evidence for unidimensionality, but exploratory factor analysis with questionnaire items (vs. subscales) in a larger sample might reveal distinct dimensions of avoidance that differentially relate to outcome. Fourth, the present study relied on retrospective structured interviewing to confirm mTBI diagnosis and obtain injury characteristics. Acute medical records were typically not available. Fifth, selection bias was likely because we recruited from an outpatient specialty clinic and less than half of screened patients enrolled. Study participants may have been more likely to exhibit a maladaptive behavioral coping style. It should also be highlighted that participants who were not working at the time of injury were excluded from this study, further limiting generalizability. Sixth, administering six questionnaires to measure avoidance in future research may be burdensome. To address this, we created a 12-item short form avoidance scale that had favorable psychometric properties. Validation of this short form scale is required.
Conclusions
Patients who engage in fear avoidance or its antithetical coping style, endurance behavior, in the weeks to months after mTBI appear to be at increased risk for chronic symptoms, disability, and adverse mental health outcomes. Biopsychosocial models of mTBI outcome should tentatively incorporate these two pathways to chronicity. Future research is needed to assess the unique prognostic value of illness coping styles and their modifiability with early intervention.
Footnotes
Acknowledgments
The authors wish to thank research assistants Mary Ellen Johnson and Sabrina Khan as well as the clinical staff at our recruitment sites, including Kelsey Davies, Jennifer Loffree, Grace Boutilier, and Trish Mahoney (GF Strong Rehab Centre), Deanna Yells, Heather MacNeil, and Rod Macdonald (Fraser Health Concussion Clinic), Denise Silva and Lesley Norris (Back in Motion), and Karilyn Lao, Wayne Tang, and Cyrus Huang (LifeMark).
This study was funded by a Specific Priorities Research Grant from WorkSafeBC (#RS2014-SP03). NDS receives salary support from a Clinician-Scientist Career Development Award from the Vancouver Coastal Health Research Institute and a Health Professional Investigator Award from the Michael Smith Foundation for Health Research.
Author Disclosure Statement
Noah Silverberg has a private practice in neuropsychology that includes consultation roles with professional sport organizations and disability insurance providers, including WorkSafeBC. William Panenka has a clinical practice in forensic neuropsychiatry involving individuals who have sustained TBIs. Grant Iverson has been reimbursed by the government, professional scientific bodies, and commercial organizations for discussing or presenting research relating to mTBI and sport-related concussion at meetings, scientific conferences, and symposiums. He has a clinical practice in forensic neuropsychology involving individuals who have sustained mTBIs. He is a co-investigator, collaborator, or consultant on grants relating to mTBI funded by several organizations. He acknowledges unrestricted philanthropic support from ImPACT Applications, Inc.