
Abstract
Special Weapons and Tactics (SWAT) personnel who conduct breacher exercises are at risk for blast-related head trauma. We aimed to investigate the potential impact of low-level blast exposure during breacher training on the neural functioning of working memory and auditory network connectivity. We also aimed to evaluate the effects of a jugular vein compression collar, designed to internally mitigate slosh energy absorption, preserving neural functioning and connectivity, following blast exposure. A total of 23 SWAT personnel were recruited and randomly assigned to a non-collar (n = 11) and collar group (n = 12). All participants completed a 1-day breacher training with multiple blast exposure. Prior to and following training, 18 participants (non-collar, n = 8; collar, n = 10) completed functional magnetic resonance imaging (fMRI) of working memory using N-Back task; 20 participants (non-collar, n = 10; collar, n = 12) completed resting-state fMRI. Key findings from the working memory analysis include significantly increased fMRI brain activation in the right insular, right superior temporal pole, right inferior frontal gyrus, and pars orbitalis post-training for the non-collar group (p < 0.05, threshold-free cluster enhancement corrected), but no changes were noted for the collar group. The elevation in fMRI activation in the non-collar group was found to correlate significantly (n = 7, r = 0.943, p = 0.001) with average peak impulse amplitude experienced during the training. In the resting-state fMRI analysis, significant pre- to post-training increase in connectivity between the auditory network and two discrete regions (left middle frontal gyrus and left superior lateral occipital/angular gyri) was found in the non-collar group, while no change was observed in the collar group. These data provided initial evidence of the impact of low-level blast on working memory and auditory network connectivity as well as the protective effect of collar on brain function following blast exposure, and is congruent with previous collar findings in sport-related traumatic brain injury.
Introduction
B
Blast-related mTBI is primarily caused by energy transmitted to brain tissues when the explosive's pressure wave passes through the skull, tissues, and/or blood vessels due to the direct compression of the skull or thorax. Thus, the injuries are characterized by anatomical and physiological changes from the initial over-pressurized force hitting the body. The results may include rupture of the tympanic membrane and middle ear damage, and concussion. The concussion is likely to be caused by the brain bouncing or twisting inside the skull. This could cause damage to neurons and glial cells. Blast-related mTBI also can be caused by flying debris (secondary mechanism) or by hitting the ground, wall, or other objects in the environment (tertiary mechanism). Due to the multi-faceted nature of the injury in military environments, it is difficult to differentiate the effect of the primary cause of blast-related mTBI on brain function and structure from other effects potentially caused by secondary and tertiary mechanisms of injury. While extensive resources have been devoted to investigating the neurological and pathological sequela of blast-related mTBI in humans, unpredictable combat settings make replicating and isolating blast-related mTBI in research settings challenging.
While mTBI has received considerable attention in the media and scientific literature, the potential of receiving a brain injury from a blast is likely dependent on the magnitude and proximity of the blast and the timing and frequency of the blast exposure. The forces themselves range from exposures to innumerable small weapons fire to that of higher explosives, such as grenades, joint direct attack munitions, or much larger ordinance air blasts. An improvised explosive device can produce a blast overpressure of nearly 60 psi, 6 and brain injury resulting from the blast waves can have deleterious neurological effects. 7 –9
One group who may be particularly vulnerable to blast-related brain injuries are military personnel and non-military law enforcement who conduct breacher exercises. 10,11 During training, Special Weapons and Tactics (SWAT) and military personnel position themselves at the edge of a “safe exposure distance” before placing and detonating a low-level explosive charge on either a doorway or wall. This allows personnel to avoid debris and minimize room entry time while creating a blast capable of disorienting and disabling a perpetrator. Therefore, SWAT breaching personnel constitute a unique population for studying repeated low-level blast-related head trauma from the primary mechanism (i.e, the blast wave), as trainees are exposed to explosive blasts in a controlled minimized manner that, by design, limits potential injury resulted from the secondary and tertiary injury mechanisms. However, it is unclear whether this positioning fully protects them from indirect exposure to blast waves.
In order to teach and maintain skills associated with breaching, SWAT and military personnel are exposed to repeated low-level blasts during participation in breacher training. While these low-level explosions are classified as sub-concussive and may not lead to immediate brain injury or neurocognitive functional impairment that may warrant immediate clinical care, repetitive exposure to these blasts over time may have potential cumulative neurocognitive sequela. Recent studies have reported symptoms in breacher teams similar to those of soldiers who experienced stronger explosive blasts. 10,11 Multiple prospective studies have attempted to evaluate the sequelae of primary blast injury exposure and have found significant functional and structural alterations in the brain networks based on examination of war veterans. 12 –14 Such findings have been mirrored in prospective studies involving military personnel who participated in breacher and heavy weapons training. 15 –17 For example, Rhea and colleagues 15 found that some military personnel who were repeatedly exposed to low-level blasts in a single heavy weapons training session (exposure to two to nine blasts, all sub-concussive) showed neuromotor and neurocognitive performance decline after the low-level blasts exposure. Similar results were found in a 2-week long breacher training program with participants experiencing neurocognitive deficits and changes in biomarker loading following course completion. 16
In the present study, in addition to investigating the potential impact of exposure to repetitive low-level explosive blasts, a jugular vein compression collar, designed to slightly take up the reserve volume of the cranial spinal space and mitigate slosh by reducing the absorption of mechanical energy and reducing cavitation (vapor cavity bubble formation), 18 –22 was tested for its potential in mitigating the effect of blast exposure. Previous sporting impact neuroimaging data showed that young athletes who wore the collar demonstrated a significantly lower degree of pre- to post-season changes, both functionally and structurally, in comparison to those who did not wear the collar. 23,24 We predicted that the jugular vein compression collar would provide similar protection for breacher trainees as has been demonstrated in animal models and recently in athletic populations. 18,23 –26
In the present study, we studied a cohort of SWAT team members from local law enforcement who underwent a 1-day breacher training that included multiple controlled explosions. We compared the pre- to post-training functional magnetic resonance imaging (fMRI) of working memory using an N-Back task as well as changes in auditory network functional connectivity during a resting-state paradigm, and quantified the group difference between those who wore the collar versus those who did not wear the collar. Based on the data from our recent neuroimaging studies of sub-concussive head impacts in high school athletes, 23,24 we hypothesized a significant post-training increase in the blood oxygen–level dependent (BOLD) signal response and hyperconnectivity in association with exposure to explosion (for those who did not wear the collar), and significantly less changes in BOLD signal for those who wore the collar.
Methods
Participants
Twenty-three male participants (age range, 31.4 to 68.7 years, mean ± standard deviation [SD] = 43.5 ± 6.8 years) from a local SWAT team were enrolled for this study. Participants were randomly assigned to one of the two study groups: non-collar group (n = 11) and collar group (n = 12). All subjects provided informed consent prior to participation in the study. Primary exclusion criteria included history of neurological deficits, previous cerebral infarction, previous severe head trauma, known increased intracranial pressure, metabolic acidosis or alkalosis, glaucoma (narrow angle or normal tension), hydrocephalus, penetrating brain trauma (within 6 months), known carotid hypersensitivity, central vein thrombosis, known airway obstruction, or seizure disorder.
In the analysis of fMRI of working memory, five of the 23 participants were excluded from final analysis for the following reasons: missing the post-BLAST training scan due to scheduling issue (n = 1, non-collar group), claustrophobia (n = 1, collar group), or not following fMRI task instructions (n = 3, two from the non-collar group, one from the collar group). The final analysis included 18 participants (non-collar group, n = 8; collar group, n = 10). The demographic information, including age, body weight, and body mass index (BMI), are presented in Table 1. No statistically significant difference was found in any of these variables between the two study groups. For the resting-state fMRI analysis, only one participant was excluded (in the non-collar group, due to a scheduling issue). The demographic variables are presented in Table 1.
SD, standard deviation; fMRI, functional magnetic resonance imaging; BMI, body mass index; rs-fMRI, resting-state functional magnetic resonance imaging.
One-day breacher training
All participants participated in a 1-day training (including a morning session and an afternoon session) of breacher training and blast exposure. The morning session involved exposures to three large composition explosions-4 (C4) with a stand-off distance of 25 yards in an open field at an outdoor police shooting range. The afternoon session involved a more complex indoor environment at an abandoned bank with shorter stand-off distances and many walls and irregular surfaces interposed between the officers. The initial sensing of blast wave energies, done before the onset of officer exposure, yielded a higher reflective cumulative blast wave (thought to be greater than expected due to the heavy walls and steel within the bank itself). Thus, the stand-off distance from the C4 explosive charges for the afternoon session was increased from 8 to 22 feet. Eleven C4 explosions in various rooms and hallways were carried out on doors and the walls themselves and 25 flashbangs were detonated in rooms and within the bank vault itself, all with SWAT team members in attendance.
Instrumentation and procedures
Testing sessions were completed within 48 h to the day of breaching training at both the pre- and post-training time-points. The testing sessions consisted of the MRI testing sequence, electroencephalography (EEG), audiological testing, electrophysiological testing, and anthropometric measurement. A separate audiological testing session also was performed on the same day immediately following completion of the blast exposure. On the day of the breacher training, subjects were outfitted with accelerometers and blast over-pressure gauges, and those in the collar group were fitted with the appropriately sized collar device. The results derived from EEG data will be reported separately and will not be included in the present study.
Neck ultrasound evaluation and collar fitting
At the initial fitting of the collar before the breacher training session, a registered vascular technologist utilized ultrasound to ensure that the proper collar and internal jugular vein (IJV) responses (e.g., visual evidence of IJV dilation superior to collar) occurred as prescribed. The participants in the collar group wore the collar for approximately 7 h on the day of the breacher training. All measurements, images, and video clips were acquired using a LOGIQ e-unit (General Electric Inc., Fairfield CT) with an ultra-high frequency L8-18i-RS linear transducer.
Head acceleration and BLAST wave monitoring and quantification
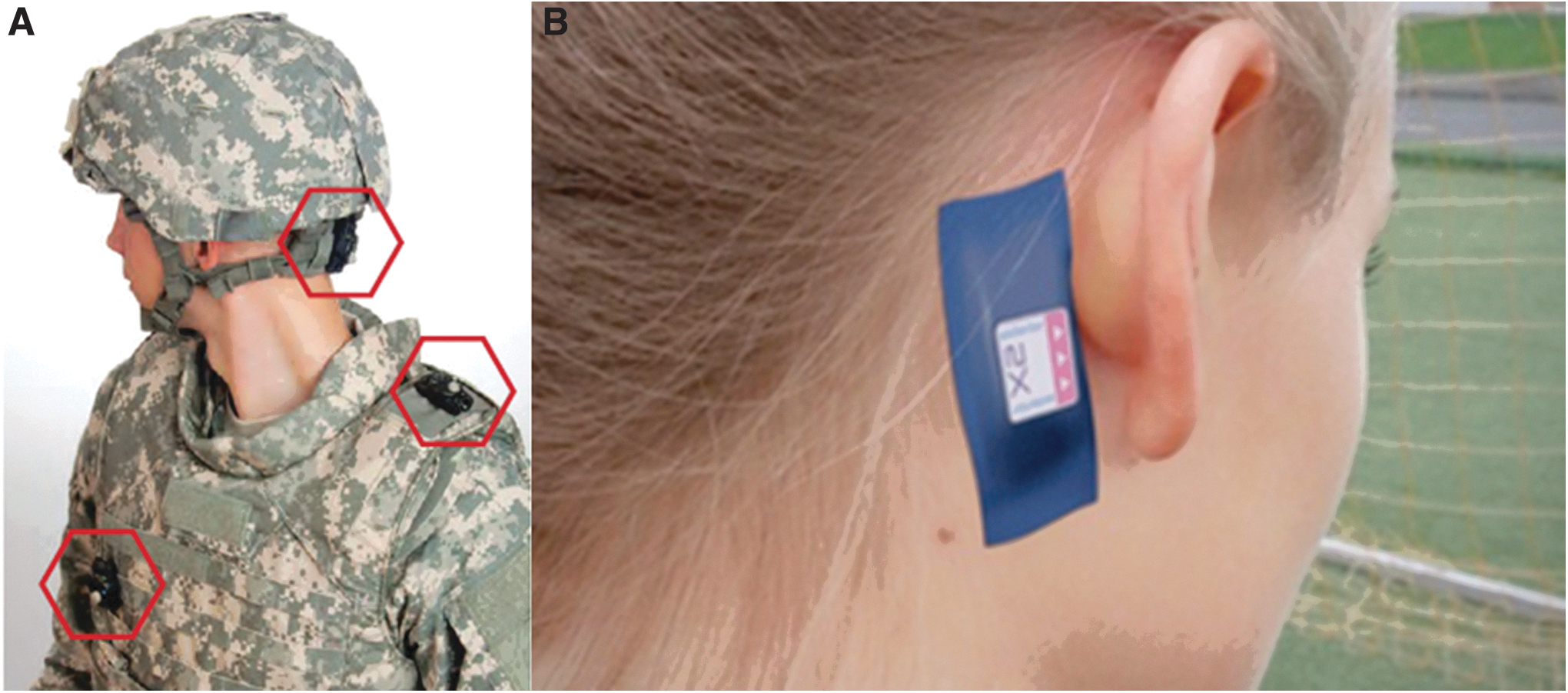
Each participant was outfitted with a Blast Gauge System (BlackBox Biometrics, Inc., Rochester, NY) to monitor blast pressure exposure (Fig. 1A). The Blast Gauge System consists of three wireless pressure gauges mounted on the chest, shoulder, and head, and is designed to capture the peak over and under pressure and impulse (area under the pressure-time curve) of explosive blasts. In addition, each participant was outfitted with an X Patch accelerometer (X2 Biosystems, Seattle, WA). The accelerometer adheres to the head just behind the ear using an adhesive patch (Fig. 1B). It assesses the severity of impacts by measuring three axes of linear acceleration and angular rotation, respectively, and converting this data to estimate the G-forces exposure to the head.
Audiological testing and electrophysiological measurement
Each participant underwent audiological testing and electrophysiological measurement, both pre- and post-training. The following testing was included in the study and quantified to evaluate the potential impact blast exposure as well as the efficacy of collar usage.
Pure tone audiometry (PTA)
A subjective measure of auditory acuity and is the standard used to determine hearing threshold levels for different frequencies. PTA determines the type, degree, and configuration of a hearing loss. It is a critical tool in determining any temporary threshold shifts after a high intensity blast or evidence of noise-induced hearing loss. 27,28
Distortion Product Otoacoustic Emission Testing (DPOAE)
This type of Otoacoustic Emission (OAE) test is an objective measure of the integrity of the outer hair cell function. 29 A normal cochlea does not just receive sound; it also produces low-intensity sounds called OAEs. DPOAEs are comprised of sounds emitted from the ear in response to two simultaneous tones of different frequencies. The response arises from the cochlea, but the outer and middle ear must be intact to transmit the sound back to the recording microphone to pass. Repeated high intensity noise exposure can compromise the outer hair cells, eventually resulting in cochlear dysfunction and hearing loss. DPOAEs provide early “warning signs” of these compromised hair cells, even when PTA reports normal hearing. 28
Auditory Brainstem Response (ABR)
An objective measurement of synchronous neural function in response to auditory (click and tone pip) stimuli. An ABR is not a hearing test; rather, it is an electrophysiological measurement used in conjunction with audiologic measures to identify any neurological abnormalities along the auditory nerve through the brainstem. 30,31
MRI data acquisition
Magnetic resonance scanning was conducted on either a Phillips 3T Achieva scanner or a Phillips 3T Ingenia scanner (Philips Medical Systems, Best, the Netherlands). The Achieva 3T and the Ingenia 3T scanner were equipped with a SENSE 32 channel head coil and dStream 32 channel head coil, respectively. The number of participants scanned on the two scanners 3T scanner is presented in Table 1. Each participant was scanned on the same scanner for both MRI sessions.
A single shot echo-planar imaging sequence was used for N-Back fMRI data acquisition with the following specifications: repetition time/echo time = 2000/35 msec; flip angle = 90°; 160 dynamic scans; field of view = 240 × 240 mm; image acquisition and reconstruction matrix = 64 × 64; 36 axial slices; resolution = 3.75 × 3.75 × 5.0 mm. Similar acquisition parameters were used in the resting-state fMRI data acquisition except that the number of dynamic scans was set to 150 and the scan was repeated twice. A high resolution (1 mm isotropic) three-dimensional (3D) T1 weighted sequence was used to for image registration. In addition, the susceptibility weighted imaging (SWI), diffusion tensor imaging (DTI), and high angular resolution diffusion imaging (HARDI) were also included in the magnetic resonance protocol. A board-certified neuro-radiologist evaluated the 3D T1-weighted images and the SWI data for potential incidental findings. The DTI and HARDI data will be analyzed and reported separately.
N-Back working memory fMRI paradigm
All participants performed a verbal working memory N-Back task at both the pre- and post-training fMRI sessions. The N-Back task was for N = 0 and N = 2. The fMRI paradigm consisted of five cycles of fixation (12 sec), 0-Back (26 sec), and 2-Back (26 sec) periods. During the 0-Back period, a series of letters, including A, B, C, D, and O, was presented successively in a random order. Participants were instructed to press a hand-held button when the letter “O” was presented. During the 2-Back task period, a series of letters, including A, B, C, and D, were presented successively in a random order. The participants were instructed to press a button when a letter shown was the same as the letter presented two trials back. The details of the fMRI experimental paradigm have been described elsewhere. 32
Resting-state fMRI paradigm
Each scan session included two sequential 5-min acquisitions of resting-state fMRI during which a fixed white cross (+) was displayed on a black background. Participants were instructed to lie still with their eyes open and looking at the cross but were not instructed to focus their thoughts on anything in particular.
Statistical analysis
Analysis of fMRI of working memory was performed using the FSL (fMRI of the Brain Software Library;
The second level analysis included generating the group activation map for the N-Back task, testing the pre- to post-training change in the brain activation, testing the group difference of the longitudinal change, as well as correlation analysis with blast exposure and working memory task performance. The group activation map for the 2-Back versus 0-Back contrast across all participants from both study groups at baseline was calculated using FSL's FLAME mixed effect model (model 1) based on the contrast and variance images from individual subjects. A gray matter mask based on FSL's standard space population gray matter tissue prior image (avg152T1_gray.nii) was created using an intensity threshold of 50 and used to limit the regions of brain activation to gray matter. The threshold-free cluster enhancement (TFCE) was used with 5000 permutations to account for multiple comparisons. 34 The within-group longitudinal fMRI changes between pre- and post-training sessions and the group difference of this longitudinal change also were processed and analyzed in FSL using FLAME with multiple comparisons corrected (TFCE with 5000 permutations).
Several variables, including age, BMI, body weight, and scanners, were individually tested for potential confounding effect in the group comparison analysis. None of these variables, however, showed significant effect in the initial test and were thus not included in subsequent analyses. For the correlation analysis, we first calculated the difference in the pre- and post-training Z maps from the brain areas that presented significant within-group difference in fMRI brain activations in the non-collar group. The pre- to post-training difference in Z-statistics were then extracted and used to correlate with blast exposure based on Pearson correlation analysis.
Analysis of resting-state fMRI was performed using Statistical Parametric Mapping (
Results
Participants characteristics
As shown in Table 1, the age of the 18 participants who were included in the final N-Back fMRI analyses ranged from 31.36 to 68.70 years (median: 40.13 years, mean ± standard deviation [SD]: 42.43 ± 8.47 years) at pre-training. No significant group difference in age at pre-training imaging was noted between the non-collar group (46.09 ± 9.54 years) and the collar group (39.50 ± 16.59 years, p = 0.102). The two study groups also were comparable in body weight and BMI. Blood pressure readings obtained with an automatic digital read-out forearm cuff showed no significant pre- to post-training change at p < 0.05 in systolic pressure, diastolic pressure, or pulse pressure in either the non-collar or collar group. For the resting-state fMRI analyses, 22 participants were included (median: 40.83 years, mean ± SD: 43.85 ± 9.57 years). The non-collar group (n = 10) was older than the collar group, with statistical significance (p = 0.02, Table 1). Similarly, no significant pre- to post-training blood pressure change at p < 0.05 was observed in either study group.
Exposure to the blast explosive waves during the breacher training
The number of blast explosive waves recorded for each participant ranged from one to 12 (Table 2). No significant differences were observed for the number of blast explosions, stand-off distance, the average peak pressure, or the total impulse between the two groups (all p > 0.05).
SD, standard deviation; fMRI, functional magnetic resonance imaging; rs-fMRI, resting-state functional magnetic resonance imaging.
Audiological testing results
The dB difference between the distortion product emission and the noise floor amplitudes (DP-NF) at both pre and post-training was calculated at a series of frequency (including 2000, 3000, 4000, 6000, and 8000 Hz) for each participant. The descriptive statistics of the pre- to post-training changes for each group and the statistical significance of the group difference are summarized in Table 3. There was a significant group difference in the pre- to post-training change in DP-NF at 4000 Hz in the right ear (p = 0.01). This group difference did not remain statistically significant after controlling for multiple comparisons. There was no significant group difference in the change in DP-NF at any other frequency level.
DP-NF, distortion product emission-noise floor amplitude; SD, standard deviation; R, right; ns, non-significant; L, left.
The two study groups also were comparable in the pre- to post-training change in the PTA and ABR testing (all p > 0.05). A more detailed analysis of the pre- and post-audiological and electrophysiological testing will be reported in a separate article.
fMRI N-Back task performance
The two study groups were comparable in fMRI task performance during both fMRI sessions (all p > 0.05; Table 4). No significant longitudinal pre- to post-change was found in accuracy or response time in either study group (all p > 0.05).
fMRI, functional magnetic resonance imaging; SD, standard deviation.
fMRI brain activation of N-Back working memory
Figure 2 presents the brain regions where the fMRI BOLD signal was significantly higher during the performance of the N-Back tasks (composite Z-score map, 2-Back >0 Back) in the entire cohort (n = 18) at the pre-BLAST training fMRI session. The significant activation (increased BOLD signal during 2-Back when compared with 0-Back) were found in a series of bilateral or unilateral anatomical loci that are known to be involved in the fMRI of working memory using N-Back task. No significant differences in fMRI BOLD signal at baseline were found between the non-collar and collar groups (p > 0.05, TFCE corrected).
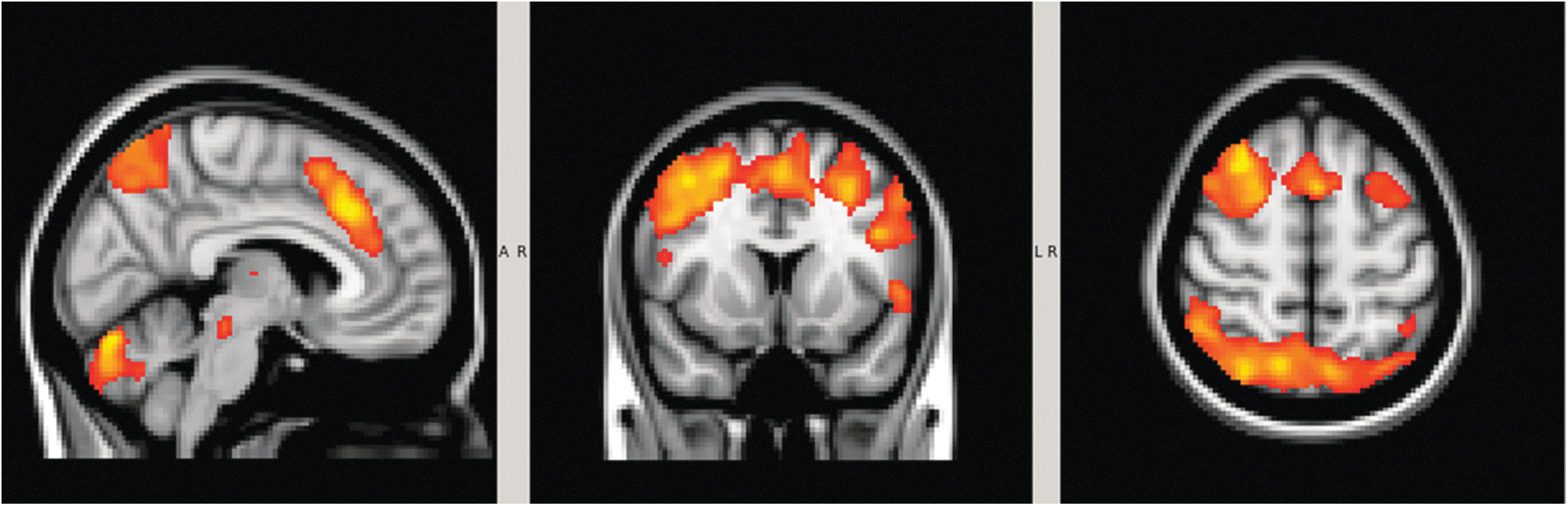
Composite Z-score maps of brain activation during the pre-blast training N-Back functional magnetic resonance imaging in the entire sample (n = 18, Z > 3, p < 0.01, corrected). Color image is available online.
Longitudinal pre- to post-training change and the group d + 9ifference of the change in fMRI brain activation of N-Back working memory
Figure 3 presents the composite p value map for brain regions within the non-collar group that showed significantly stronger activation (p < 0.05, TFCE corrected) for the 2-Back >0-Back contrast at the post-BLAST training fMRI session compared with the pre-BLAST training. The significant regions included the right insular, right superior temporal pole, right inferior frontal gyrus, and pars orbitalis. No significant pre- to post-BLAST training change was found in the collar group. Using the collar group as the reference, significantly larger pre- to post-BLAST training increase in brain activation also was found in the right insular, right superior temporal pole, right inferior frontal gyrus, and pars orbitalis (Fig. 4). The total volume of brain regions with significant group difference was 3648 mm 3 , equivalent to approximately 52 voxels at the original resolution of data acquisition.
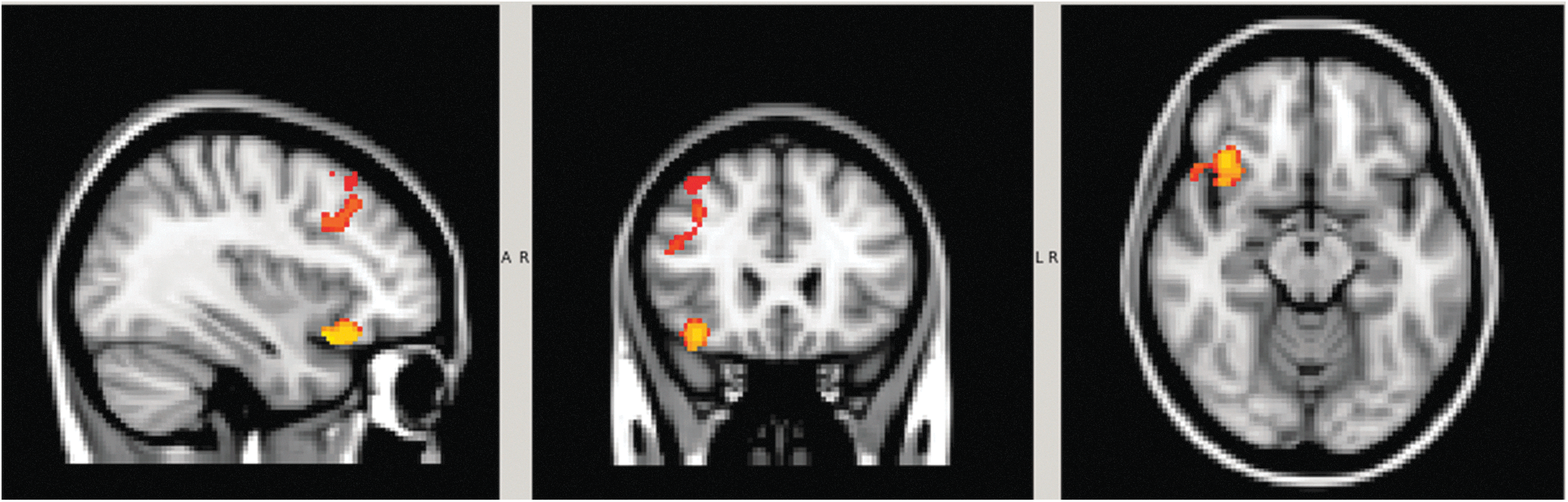
Brain regions with statistically significant pre- to post-blast training increase N-Back working memory brain activation in the non-collar group (n = 8; p < 0.05, corrected). No statistically significant change between pre- and post-blast training was found in any brain regions in the collar group (n = 10). Color image is available online.

Brain regions with significantly greater pre- to post-blast training increase in activation in the non-collar group (n = 8) than collar group (n = 10; p < 0.05, corrected). The volume of the brain regions with significant group difference was 3648 mm 3 , which is equivalent to approximately 52 voxels at the original resolution of data acquisition (3.75 mm × 3.75 mm × 5 mm). Color image is available online.
Association between the longitudinal change in brain activation of N-Back working memory and BLAST exposure
A significant correlation was found between the change in brain activation and the average peak pressure recorded from the head sensor in the participants in the non-collar group (r = 0.943, n = 7, p = 0.001; Fig. 5A). No statistically significant association was found between the average peak pressure and the pre- to post-BLAST training change in brain activation in the collar group (r = 0.380, n = 9, p = 0.37; Fig. 5B). No significant correlations were found between the number of blast explosions or the total impulse and the pre- to post-BLAST training change in brain activation in either of the two study groups (all p > 0.05).

Significant correlation between pre- to post-blast training change in blood oxygen–level dependent activation and the average peak impulse recorded at the head location in the non-collar group (r = 0.943, n = 7, p = 0.001).
Auditory network connectivity change and audiological testing outcomes
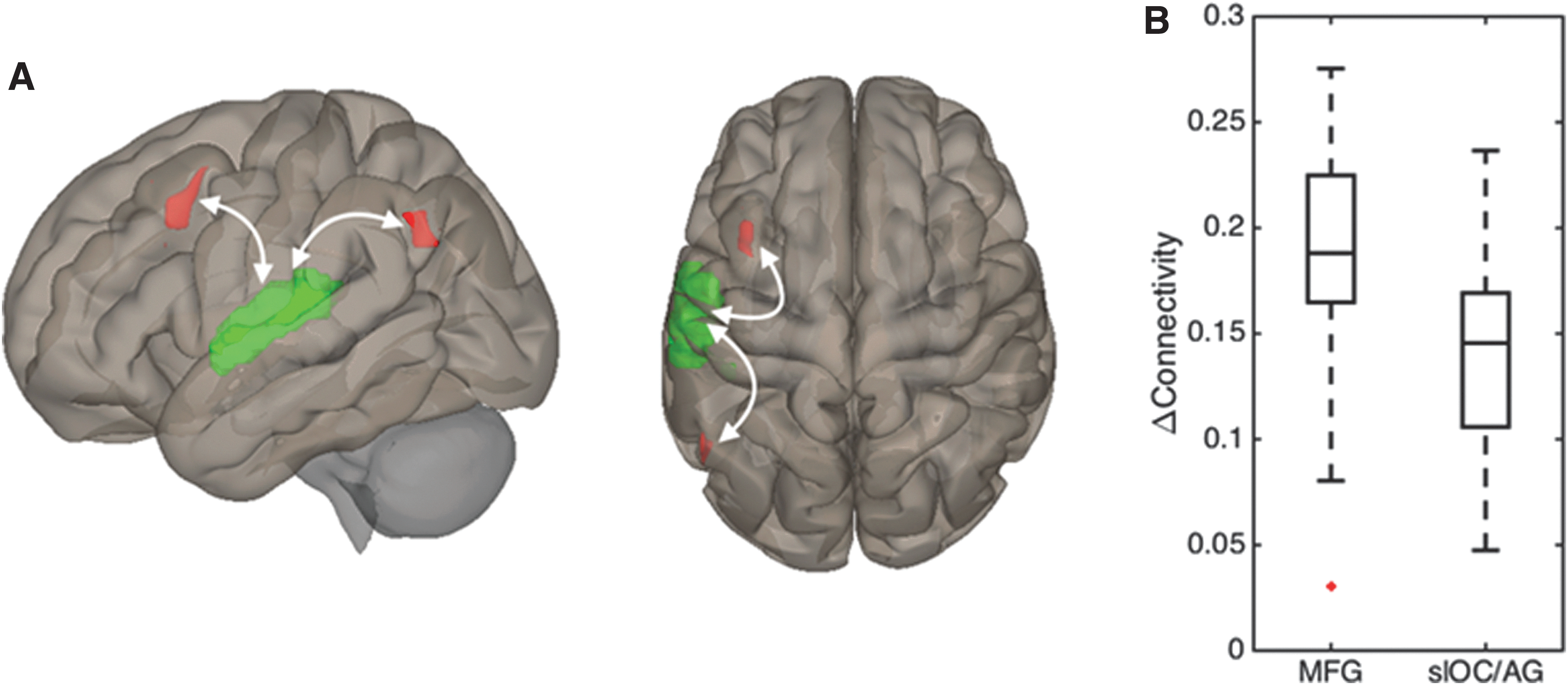
Prior to blast exposure, seed-to-voxel connectivity patterns showed no differences between the two groups for either the left or right primary auditory cortex. Following blast exposure, we observed hyperconnectivity (relative to baseline) in the non-collar group (n = 10) between the left primary auditory cortex and two discrete clusters in the left middle frontal gyrus (cluster p = 0.008 [FDR corrected], Δβ = 0.19, 1.54 cm 3 in volume) and left superior lateral occipital/angular gyri (cluster p = 0.019 [FDR corrected], Δβ = 0.15, 1.05 cm 3 in volume), respectively (Fig. 6). No significant pre- to post-training changes in connectivity were observed in the collar group between either the left or right auditory network and any other region of the brain. When comparing the group difference, there were no significant differences in changes of connectivity between the two study groups.
To exclude the potential confounding effect of age difference between the two groups, we tested and found that there is no correlation in the non-collar group between age and the observed changes in connectivity of either cluster (these correlations have r 2 values of almost 0 and p values of ∼0.6–0.7). Age also was tested as a covariate of no interest in the second-level seed-to-voxel analysis; the only effect is a small shrinkage in the size of our significant clusters (due to the loss of a degree of freedom). Therefore, all the results related to resting-state fMRI connectivity were based on analysis without age as a covariate.
We performed post hoc testing to evaluate associations between audiological and electrophysiological testing outcomes and the non-collar group's significant clusters of hyperconnectivity. Controlling for multiple comparisons, linear regression analyses revealed no significant association for either cluster with pre- to post-exposure changes in DPOAE, PTA, or ABR, although the latter of these measures showed some consistency in their correlations with connectivity changes based on uncorrected statistical significance values (Supplementary Table 1; see online supplementary material at
Association between the auditory network connectivity change and blast exposure
In the non-collar group, peak pressure was positively correlated with changes in connectivity between the right primary auditory cortex and the right pre- and post-central gyrus (Fig. 7A, 7B). In the collar group, total impulse was negatively correlated with changes in connectivity between the left primary auditory cortex and the medial frontal pole/paracingulate gyrus (Fig. 7C, 7D). Total impulse also was negatively correlated with changes in connectivity between the right primary auditory cortex and two clusters in the paracingulate gyrus and posterior corpus callosum (not shown in figure). No significant group difference was found in associations between auditory network connectivity change and blast exposure.

Seed-to-voxel analyses were used to test associations between blast exposure and changes in connectivity.
Discussion
In the present investigation, we studied a cohort of SWAT personnel who underwent a 1-day training of breacher exercises with low-level blast exposure in a controlled environment. We aimed to investigate the potential impact of low-level blast exposure on the neural functioning of working memory and auditory network connectivity. We also aimed to test whether a jugular vein compression neck collar device can help ameliorate the potential changes in response to the blast exposure. As hypothesized, significant pre- to post-training elevation in fMRI brain activation of working memory and increase in connectivity to the auditory network based on resting-state fMRI were found in the non-collar group but were not in the collar group. In addition, we also found significant correlation between the increase in the BOLD signal of working memory and the blast exposure.
Functional MRI of working memory using the N-Back task has been applied frequently in studying the functional integrity of brain networks in patients with traumatic brain injury varying in injury severity, 38 –44 as well as in athletes in contact sports with concussive 45 –48 or repetitive sub-concussive head impacts. 32,49 –52 With a few exceptions, most studies demonstrated stronger BOLD signal in response to working memory task after the TBI. 32,38,39,43,44,46 –48,53 To our knowledge, the application of fMRI for blast-related head trauma is emerging, but still limited. 54 Several studies have investigated patients with chronic blast-related mTBI focusing on different functional domains, including executive function, visual spatial functions, or emotional processing. 55 –58 However, we are aware of only one recent neuroimaging study that used fMRI of working memory based on N-Back task in conjunction with head trauma from repeated low-level blast exposure. 59 Carr and colleagues 59 investigated the change in activation during an N-Back task in acute or semi-acute stage (all within 1 week) in military personnel who underwent a 2-week breacher training. A significant increase in brain activation after the training was found in the instructor group but not in the student group, despite the comparable “dosage” of blast exposure during the study. Carr and colleagues 59 interpreted the elevated brain activation as being necessary to compensate for the potentially affected neurons in order to maintain the level of task performance. Carr and colleagues further attributed group differences to the higher level of exposure in the instructors who underwent the same type of breaching training (as instructors) multiple times every year prior to the participation of the study. The findings of increased BOLD signal post-training in the instructor group were congruent with previous studies of patients with TBI and athletes with concussion and/or sub-concussive head impacts. 20,44,46,59,60
Contrary to the negative findings in the student group in Carr's study, the non-collar group in the present study demonstrated elevation with statistical significance in brain activation after only one day of breaching training. One explanation for this this difference is blast type and frequency. The non-collar group in the present study experienced two to seven explosion blasts, with peak pressure ranging from 1.51 to 2.53 psi. For comparison, the participants in Carr and colleagues study all experienced 40 blasts, with peak pressure ranging from 0.1 to 13.0 psi (61% <1 psi, 4%> 4 psi). It is not clear whether these differences contributed to the discrepancy in fMRI findings. Other potential factors, including the difference in the length of training and the interval between the training and imaging, also may contribute to our differing findings.
Functional connectivity analyses using resting-state fMRI presents a double-edged sword: Measuring the correlation of BOLD signals from any two brain regions over time enables a granular interrogation of functional networks, but that same quality markedly increases the number of null hypotheses available for testing. Consequently, in order to retain statistical power, we limited our connectivity analyses to seed-to-voxel changes related to the primary auditory network. We chose this network due to the nature of the blast exposure to which our participants were subjected and the associated audiological testing data we acquired. The hyperconnectivity exhibited by the non-collar group is consistent with findings from numerous resting-state fMRI studies of TBI. 61 –66 A recent review by Hillary and Grafman 67 posits that such hyperconnectivity reflects a re-establishment of network communication via the recruitment of “detour” paths. 68 Our findings of positive correlations between connectivity changes and blast exposure in the non-collar group can be similarly explained by this mechanism; greater exposure would tend to result in a greater degree of injury and promote hyperconnectivity. However, the negative correlations between connectivity changes and blast exposure observed in the collar group cannot be understood within this framework. Notably, within the collar group, these associations were primarily driven by those with the lowest exposure exhibiting hyperconnectivity rather than those with the most exposure exhibiting decreased connectivity.
While the lack of overall hyperconnectivity and lack of positive associations in the collar group may be taken as evidence of a protective effect of the device, the negative correlations present a curious anomaly that warrants further investigation. In addition, it is noted that the working memory changes based on N-Back fMRI are in the right hemisphere whereas the findings based on changes derived from resting-state fMRI are in the left hemisphere. It may be attributed to the possibility that the lack of an acoustic component to any subvocal rehearsal effected by the participants would be expected to rule out observation of changes in activity associated with possible peripheral auditory pathway alterations. The resting-state fMRI network connectivity analysis is more likely to detect alterations in spontaneous rate of the peripheral system, whereas the working memory tasks should not differentially affect this activity.
In the present study, we term “low-level” to describe blasts that are sub-concussive in nature. Our study was designed to standardize and normalize exposures to explosive blasts while keeping the SWAT teams at a safe distance to ethically minimize damage, as blast overpressure can rupture eardrums, induce lung damage, and potentially be fatal. 69,70 The measured blast over pressure in the present study was in the range of 0.87–2.53 psi (1.51–2.53 psi in the non-collar group)—well under the safety protocol developed in United States military which requires any single blast event in a controlled training environment to be under 4 psi. 71,72 Therefore, despite being well below the threshold of the maximum blast pressure that could ethically be induced on our participants, we still found significantly increased brain activation in the non-collar group. Further, the pre- to post-training increase in brain activation was highly correlated with the peak pressure from the explosive blast, albeit the participants only experienced two to seven blasts with a range of 1.51 to 2.53 psi.
In this study, we also demonstrated that brain-level changes occurred from the repeated low-level blasts that were not observable with a common neurocognitive performance test based on accuracy or response time. Comparable task performance along with significant alteration in fMRI BOLD signal has been reported in some previous neuroimaging studies of TBI or sports related concussion. 40,73 –75 It is unclear whether ceiling effect from the 2-Back task selected in the present fMRI study contributed to the absence of performance change. The relation between the fMRI BOLD signal change and the task performance remains to be further investigated in future studies of the influence of exposure to low-level blast in breacher training.
The jugular compression collar is a novel approach designed to mitigate hydrodynamic energy absorption (coined by NASA in the 1960s as “slosh”) and thus the change in brain function and structure against insults from repetitive sub-threshold head impacts. The mechanical energy imparted by blast waves should be similar to concussive impacts that cause linear, rotational, and angular movement in the cranial fluids and the brains of contact sport athletes (i.e., slosh). Elastic collisions (as opposed to in-elastic collisions) are those in which there is no net loss in kinetic energy in the system as a result of the collision. Both momentum and kinetic energy are conserved quantities in elastic collisions. Colliding conditions that promote the end result of elastic-type collisions include 1) hard, non-distensible surfaces (as opposed to freely moving liquids) and 2) cross-bridging. Tissues of differing densities and molecular bonding would be expected to absorb mechanical forces (blast) at different rates.
Macroscopically, inhibition of fluid movement and thus mitigation of vapor cavities by “taking up the reserve compliance” of the cranium, would be expected to reduce any mechanical force absorption in a similar manner to airbags and seat-belts. In turn, microscopically, energy absorption into chemical bonds, electrostatic forces, and even Van der Waals forces could all be reduced by providing for an environment that promotes elastic collisions. Since both injuries are derived from a comparable category of mechanical energy, we expect that both injuries could potentially be mitigated in a similar fashion (slosh abatement). The collar produces a gentle back-filling of the intracranial compensatory reserve volume (“expandable space”) in the venous cerebrovascular tree by impeding low resistance jugular vein flow and diverting flow to the many alternative higher resistance venous drainage pathways (e.g., venous capacitance vessels). This may limit differing density cranial contents from accelerating and decelerating at different rates and directions (i.e., slosh). Further, as a possible mechanism, we postulate that if cavitation events are present during blast exposure, 20 –22 then confining the space that fluids can move away from each other (i.e., slosh reduction) should reduce the ability of vapor cavities from forming and imploding.
With regard to the potential safety concerns for the jugular compression effects on intracranial pressure, it is noted that the jugular compression has been studied for more than 100 years since 1916 when Queckenstedt first compressed the jugulars on the battlefield while a spinal needle was in place and the measured mild rise in intracranial pressure (ICP) gave forth to the maneuver that carries his name. 76 Common fashion neckties 77 raise ICP as do cervical collars, 78 and the mere act of lying down raises ICP to a greater level than jugular compression is known to. In a previous study of rats 79 subjected to the Marmarou Protocol, intracranial bolts measured a mild (1–3 mm Hg) rise in ICP of the rats as expected with the internal jugular vein compression. Further our study of swine 80 includes ICP monitoring as well with the same general mild rise. We have never observed the ICP to rise out of the normal physiological range (that occurs throughout a person's normal day) and in fact, activities of cough, sneeze, and Valsalva raise the ICP far in excess of jugular compression achieved with the collar device employed in the current investigation and it appears that in any given subject. As in any study of a newly discovered physiology, we have monitored closely for adverse events of long-term collar wear. To date we have not noted adverse responses to extended collar wear.
Initially assessed in contact sports, the collar device has demonstrated a potential protective effect in athletes, as evidenced by studies evaluating pre- to post-season changes in fMRI BOLD signal of working memory and DTI measures 23,24,32 While the exact mechanism of the protective effect of the jugular compression collar is not completely understood, it is presumed to cause changes in relative intracranial CSF and cerebral venous volumes, alter brain stiffness, and subsequently decrease relative brain movement (slosh) with head impacts. 6,13,15 In the current study, we hypothesized a similar mechanism for mitigation of blast wave impacts to which our military and tactical service members are exposed. In line with the observations in the fMRI studies of working memory using N-Back task in high school athletes in both male football and female soccer, 32,81 the jugular vein compression collar device showed a similar effect in ameliorating the pre- to post-training changes in brain activation.
While no prior study has been conducted based on resting-state fMRI of auditory network connectivity to investigate the collar device's mitigating effect in hearing impairment after blast exposure, the potential for hearing impairment within the repetitive head impacts arena and the natural world is well known, as reflected in the literature in as early as 1923, and beyond that is associated with falls and deafness. 82,83 Jugular compression redirects the flow from the high volume, low-resistance jugular system to the higher resistance paravertebral veins, causing them to dilate with a presumed secondary effect on pressure and volume in the cranial venous sinuses. This increase in intracranial volume can be transmitted from the intracranial space to the inner ear 84 that should result in a slight increase in inner ear pressure and volume. Adding more fluid volume into an enclosed space should affect the amount of relative movement for the structures within that volume and thus can potentially generate a protective effect preventing the fragile haircells from damage resulted from blasts.
The small sample size is a major limitation in the current study. Although the results are in line with our working hypotheses, the findings from the present study should be regarded as preliminary in nature. The lack of longitudinal follow-up after the post-training testing is also a limitation. The post-training testing was performed within 2 days after the 1-day breacher training, which can be considered as an acute stage. Based on both literature and our own studies, the temporal profile of abnormality based on fMRI and/or DTI may vary between acute, subacute, and chronic stages. It would be important in future studies to investigate the temporal progression of the changes observed at acute stages and test whether it is just a transient change, or whether it will persist for a long period and lead to symptoms that require clinical attention.
The lack of detailed history of blast exposure is another limitation. The two study groups were comparable at baseline in body weight, BMI, fMRI brain activation, and the N-Back task performance, with all these variables potentially associated with the history of blast exposure. However, the non-significant differences between the two groups in these measures helped to minimize systemic bias before the training started. The significant group difference in age at baseline in the analysis of auditory network connectivity is another limitation although the effect of age was tested and ruled out analytically as a significant confounder. It is unknown if the history of blast exposure predisposed the brain networks to be more vulnerable for future insults (such as the explosive blasts occurred during the training), which may have influenced our comparisons.
In addition, although there was a DPOAE difference at 4k Hz in the right ear, in the absence of evidence that most of the blasts occurred to the right of the participants and in the presence of positive evidence that the non-collar group was older (and thus likely to have reduced lability of the basilar membrane), attributing the preclusion of hearing impairment to the protective effect in the context of resting-state fMRI need further supporting evidences from future studies. In summary, the preliminary findings in the present study need to be replicated and verified in future large-scale studies with more comprehensive consideration in the controlling of potential confounding factors.
Conclusion
In conclusion, these data represent the first known efforts to mitigate the damaging effects of low-level repeated blast overpressures on brain function for working memory and auditory network connectivity. Despite relatively sparse number of explosive exposures (and a small average peak psi magnitude), we were able to demonstrate alterations of the brain that were statistically significant in the non-collared group but were absent when wearing the collar. We believe this lends support to previous studies using jugular compression to stave off the potential damaging effects of sport TBI and indicates that further study into this novel mechanism to help our warfighters is warranted.
Footnotes
Acknowledgments
The authors would like to thank Hamilton County Police Association (HCPA) SWAT. We appreciate their patience with the testing scheduling, follow-ups, and equipment additions. Their enthusiastic support made this study possible. We would like to thank Chief David Schaefer, SWAT Commander; Sheriff Jim Neil, Hamilton County Sheriff; and Chief Charles R. Lindsey, HCPA president for their help in obtaining approval for the study; we would also like to thank Interim SWAT Commander Tim Chin for helping to coordinate the entire study protocol. Special acknowledgement goes to SWAT Medical Directors, Dustin J. Calhoun, MD, and Edward Otten, MD, and Hamilton County Medical Director Lakshmi Kode Sammarco, MD. Without their time, commitment, and passion for the health and well-being of their team members, this study would not have been possible. We also thank Chief Jim Puthoff, Liaison to HCPA, who supported and presented the research ideas to the SWAT that allowed for the initial discussions to medical directors. We would also like to thank James P. Bailey, Evans Demolition/Excavation Division, who helped secure the bank for explosive breach training. We also thank the Bomb Explosive Ordnance Disposal Technicians Brad Justice and Steve Luensman who coordinated the explosive training and helped ensure the safety of both SWAT members and the research team. Lastly, the authors would like to thank Lacey Haas, Brynne Williams, Kaley Bridgewater, and Matt Lanier in the Imagine Research Center as their support made this study possible. The authors acknowledge funding support from Q30 Sports Innovations, LLC.
Author Disclosure Statement
David Smith is the inventor of the Q-Collar approach and has financial interest in the results of the current research. For the other authors, no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.