
Abstract
Traumatic brain injury (TBI) is common; however, effective treatments of the secondary brain injury are scarce. Melatonin is a potent, nonselective neuroprotective and anti-inflammatory agent that is showing promising results in neonatal brain injury. The aim of this study was to systematically evaluate the pre-clinical and clinical literature on the effectiveness of melatonin in improving outcome after TBI. Using the systematic review protocol for animal intervention studies (SYRCLE) and Cochrane methodology for clinical studies, a search of English-language articles was performed. Eligible studies were identified and data were extracted. Quality assessment was performed using the SYRCLE risk of bias tool. Meta-analyses were performed using standardized mean differences (SMD). Seventeen studies (15 pre-clinical, 2 clinical) met inclusion criteria. There was heterogeneity in the studies, and all had moderate-to-low risk of bias. Meta-analysis of pre-clinical data revealed an overall positive effect on neurobehavioural outcome with SMD of 1.51 (95% CI: 1.06–1.96). Melatonin treatment had a favorable effect on neurological status, by an SMD of 1.35 (95% CI: 0.83–1.88), and on cognition by an SMD of 1.16 (95% CI: 0.4–1.92). Melatonin decreased the size of the contusion by an SMD of 2.22 (95% CI: 0.8–-3.59) and of cerebral edema by an SMD of 1.91 (95% CI: 1.08–2.74). Only two clinical studies were identified. They were of low quality, were used for symptom management, and were of uncertain significance. In conclusion, there is evidence that melatonin treatment after TBI significantly improves both behavioral outcomes and pathological outcomes; however, significant research gaps exist, especially in clinical populations.
Introduction
Traumatic brain injury (TBI) is one of the commonest causes of neurological morbidity and death worldwide. 1 Recent estimations suggests an incidence of 790/100,000 person years. 2 Despite being common, evidence supporting its management and specific treatments are lacking. 3 After the acute injury, a torrent of complex and varied pathophysiological processes ensue that unfortunately result in further significant secondary brain injury, but that also potentially offers a therapeutic window. 4 Part of the problem in making treatment advances is that the injuries themselves are diverse, and they occur in markedly varied biopsychosocial settings, which influences outcome. As many treatments that have focused on a specific pathway or symptom have failed to show efficacy in human studies, it becomes attractive to consider a nonselective agent as a therapeutic candidate. 5,6
Melatonin (MEL) could be a promising neuroprotective agent in TBI. Although MEL's role in the chronoregulation of major physiological processes (e.g., the sleep–wake cycle) is well accepted, 7,8 more recently its therapeutic potential is being explored in acquired brain injury, most notably neonatal hypoxic-ischemic encephalopathy. 9 –11 MEL has pluripotent antioxidant and anti-inflammatory properties, 12 –15 which are both receptor mediated (at physiological levels) and non-receptor mediated (especially at supra-physiological levels). 16 –19 Further, its lipophilic properties allow it to cross cell membranes easily and reach subcellular compartments. 20 The latter is a useful property, considering that TBI results in widespread cellular process disruption such as metabolic cascades, indiscriminate neurotransmitter release, oxidative stress, and mitochondrial dysfunction. Indeed, a recent Neurotrauma Pharmacology working group identified a need for pharmacotherapies that promote neurorepair, neuroregeneration, and neuroprotection. 6
MEL affords neuroprotection through a wide variety of mechanisms, 18 including acting as a direct free radical scavenger and antioxidant 21 through reduction in oxidative stress by decreasing oxidative/nitrosative species and by increasing antioxidant enzymes. 22 –25 MEL also improves mitochondrial function by increasing electron transport and the function of complexes I and IV and by decreasing direct mitochondrial oxidative damage. 26 –28 As an indirect and direct consequence of these actions, MEL has also been shown to inhibit programmed cell death (apoptosis). 29 –31
In addition to providing protection from toxic metabolic intermediaries, MEL has also been shown to modulate neurotransmitter effects in TBI and other neurological conditions. Excessive release of the excitatory neurotransmitter glutamate occurs immediately after TBI. 32 MEL has the potential to “balance” this because of its action at inhibitory gamma-aminobutyric acid (GABA) receptors, especially GABAA receptors. 33 –36 It has been also shown to decrease the neurotoxicity associated with beta-amyloid, which accumulates in several neurodegenerative diseases including chronic traumatic encephalopathy (CTE). 37 Neuroinflammation is also thought to play a role in TBI and CTE. 38 Although inflammation and glial cell activation after TBI can be beneficial, if it is excessive, it can lead to significant damage and impaired function. MEL is a potent anti-inflammatory agent. 13,39,40 It achieves this partly through cytokine signaling and also indirectly by decreasing the inflammatory mediators nitric oxide and malondialdehyde production. 41
Not only is MEL attractive because of its neuroprotective properties, it also offers therapeutic potential for many of the common post-TBI symptoms such as sleep disruption, pain, mood disturbance and increased anxiety. 42 –47 MEL can help the initiation of sleep via its action on MEL receptors, 48 and can also decrease pain both at the tissue level and by modulating the opioid and GABAergic systems. 49,50 MEL may be useful in migraine, 51,52 and has efficacy in disorders of chronic pain and anxiety. 53,54 Importantly, MEL has an excellent side effect profile, with good tolerability in high does and even in children. 55 –57
In summary, MEL may offer safe nonselective neuroprotection and symptomatic treatment following TBI. The aim of this study was determine the effect of treatment with MEL (or other melatonergic agent) on the outcome (anatomical, cognitive, physical, or behavioral) after TBI compared with control or usual care in either humans or animals.
Methods
The following databases were comprehensively searched between July and December 2017 by investigator K.M.B.: The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library), PubMed (1951 to December 2017), CINAHL (1982 to December 2017), PsycINFO (1966 to December 2017), MEDLINE® (Ovid) (1948 to December 2017), Embase (1988 to December 2017), and the National Institute of Health Clinical Trials Database, 2017. The following search strategy was used using the MeSH headings or keywords: (1)
Selection criteria
Studies had to meet the following selection criteria for inclusion. (1) The study had to be a randomized controlled trial (RCT) or comparative trials using a control group or case series (> 10 participants) satisfying inclusion criteria for types of participants, interventions, and outcomes. (2) The study population included adults and children (0–19 years of age, including neonates) or animals with a TBI. (3) Treatment with MEL or N-acetyl-5-methoxytryptamine or MEL analog or melatonergic agent. The intervention group had to have been compared with a group receiving sham, placebo, or other nonexperimental control in animal studies. In human studies, in order to be inclusive, the same criteria were used as for animal studies, and also included case series. (4) Treatment could begin either before the injury or at any time point post-injury and could be provided in the laboratory, at home, or in hospital. (5) There could be any validated outcome measure assessing anatomical, physical, cognitive, and/or behavioral outcomes. A wide variety of measures tend to be employed across studies; therefore, we did not require that each one had been validated in the TBI population, as this was anticipated to limit the number of studies that could be included. Functional outcome assessed by objective, validated, reliable scales were included. Studies using global outcome scores such as the Glasgow Outcome Score (GOS), and mortality and morbidity rates were also included. (6) There had to be full text available within a peer-reviewed journal, published in English. Articles that reported on the same sample were treated as a single study.
Two of the authors independently (K.M.B. and M.V.) assessed the eligibility of studies for inclusion in the review by first reviewing articles by title and abstract to exclude those not meeting inclusion criteria. Articles that appeared to meet the inclusion criteria were further evaluated by reading the full text. Consensus for article inclusion was reached by discussion among the authors (K.M.B., M.V., and M.J.E.).
Data extraction
Details about the study design and population demographics were extracted from the included studies (Table 1). The theoretical structure, content, and dosage of the intervention programs were tabulated (Table 2). Relevant data from the studies were extracted by the first author, including outcome measures (Table 3).
TBI Model, Study Design, and Quality Assessment of Included Studies
Animal species: aAlbino Wistar rat; bNew Zealand rabbit; cSabra mouse; dCD1 mouse; eAlbino N-Mary rat; fICR mouse; gSprague-Dawley rat; hSwiss mouse.
Traumatic brain injury (TBI) models: Controlled cortical impact (CCI); closed head injury (CHI); Marmarou method (diffuse injury); fluid percussion; acceleration/deceleration model (accel/decl).
Study designs: Randomized controlled trial (RCT); controlled trial (CT).
Quality assessment (QA) SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) risk of bias tool; iDowns and Black criteria
Details of Intervention
MEL, melatonin; HCl, hydrogen chloride; PEG, polyethylene glycol; AMT, amitriptyline; IP, intraperitoneal.
Details of Outcome Measures
Reported.
Data synthesis
Quantitative analysis was conducted using Review Manager (RevMan) version 5.3 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Treatment effects were first calculated separately for each study outcome. Treatment effects for pooled data were then calculated across trials, where possible, for specific outcomes and domains. For all analyses, a random effect, inverse variance model was used to calculate standardized mean differences (SMD) and 95% confidence intervals (CI). The effect of heterogeneity (I 2 ) was used to measure the degree of inconsistency across pooled studies caused by variability rather than chance, with larger values indicative of high heterogeneity.
Data quality
Two independent reviewers (K.M.B. and M.V.) assessed the risk of bias and the methodological quality using the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) Risk of Bias tool 58 for animal studies and Downs and Black Criteria 59 for human studies (Tables 2 and 4). The SYRCLE scale has demonstrated reliability and consists of 10 items each with a score of “high,” “unclear,” or “low” risk of bias. Where no mention of treatment randomization was made, the study was awarded a “high” risk of bias, but randomization without mention of the process was given a score of “unclear.” A “low” risk of bias was awarded when baseline characteristics of weight, sex, age, and strain of the animals were provided. When animals were euthanized immediately without being returned to housing, this category of study was ranked as “low” risk. If outcome was objectively assessed using computerized methods only, this category of study was awarded “low” risk of bias. Otherwise, studies with blinding of outcome assessors were categorized as “high” risk when no specific mention of blinding was made. Selective outcome reporting was not scored, as most animal protocols are not yet published/registered. The quality of human studies was evaluated using the Downs and Black quality assessment tool, which assigns an individual score calculated out of 29 total points for each study. Discrepancies were resolved by discussion. The protocol for this systematic review and meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number PROSPERO 2017 CRD4201707302).
Methodology Quality Assessment of Included Studies Using SYRCLE Risk of Bias Tool 58
Results
The selection process for included studies is shown in Figure 1. After removing duplicates, 213 studies were screened by title and abstract review. Twenty-two studies were identified for detailed review and a further three studies were identified from reference lists of review articles. Fifteen pre-clinical studies with unique data examining the neuroprotective effects of MEL and two clinical studies examining its use for symptom management after TBI were included (see Tables 1 and 2). Sample sizes were small in all studies: 4–16 in experimental pre-clinical groups, and 7 and 12 in clinical studies. Sixteen studies were controlled trials; one study was a retrospective controlled cohort study.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of included and excluded studies.
Pre-clinical studies
TBI model and severity of injury
A variety of animals were used: nine studies used rats, five used mice, and one used rabbits, (see Table 1). 30,40,46,60 –73 Most were young adults, although two models were juvenile rat models: postnatal day 7 and 30. 70,72 In keeping with the influence of sex on outcome following animal and human TBI, adult animals were all male, except for the rabbit model. 61 Several different mechanistic models of TBI were employed; more focal injuries were obtained using closed head injury (CHI), controlled cortical impact (CCI), or fluid percussion models (FPI). 30,40,60,61,64,66 –71,74 and diffuse injuries were obtained either by the Marmarou method 63,65 or the acceleration/deceleration model 72 The resultant injuries were moderate to severe in all cases except for one mild TBI model. 72 Although Bayir and coworkers report their TBI model as mild, the injuries on MRI would suggest moderate/severe TBI. 61
Interventions
The range of MEL doses is shown in Table 2 and ranged from 0.625 mg/kg to 200 mg/kg, although the most frequent dose was 5 mg/kg. The intervention was given once in six studies 60,61,66,69,70,74 and in nine studies the dose was repeated up to 14 times. 72 The total MEL dose was between 0.625 and 300 mg/kg. The control intervention was the agent or vehicle used to dissolve and administer the MEL (usually ethanol and saline). All interventions were given by intraperitoneal (IP) injection except in one study, in which it was administered orally. 72 The interventions were commenced 20 min before the injury, 69 within 5 min of the injury, 30,60,64,65,66, 67 –71 or at 1 h 63,74 or 4 h post-injury. 61 No adverse events caused by the interventions were reported in the pre-clinical studies.
Qualitative analysis
None of the pre-clinical studies had published protocols nor were registered with Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES). Therefore, the selective outcome reporting item on the SYRCLE tool was not scored. There was insufficient information reported for many (41%) of the remaining nine questions, which were scored as “unclear.” Overall, all studies had significant risks of bias (see Table 4). The average SYRCLE score was 15.3 (95% CI: 14.4, 16.1). Although four studies 60,65,68,69 scored above the 95% CI, they were not sufficiently remarkable as to be excluded from any analyses. Nine studies reported any randomization, although details were not given. Only 30% reported any blinding, either of investigators, animal handlers, or outcome assessors (see Fig. 2). None of the studies reported sample size calculations. Indeed, nine studies (60%) had sample sizes of six per group or less.
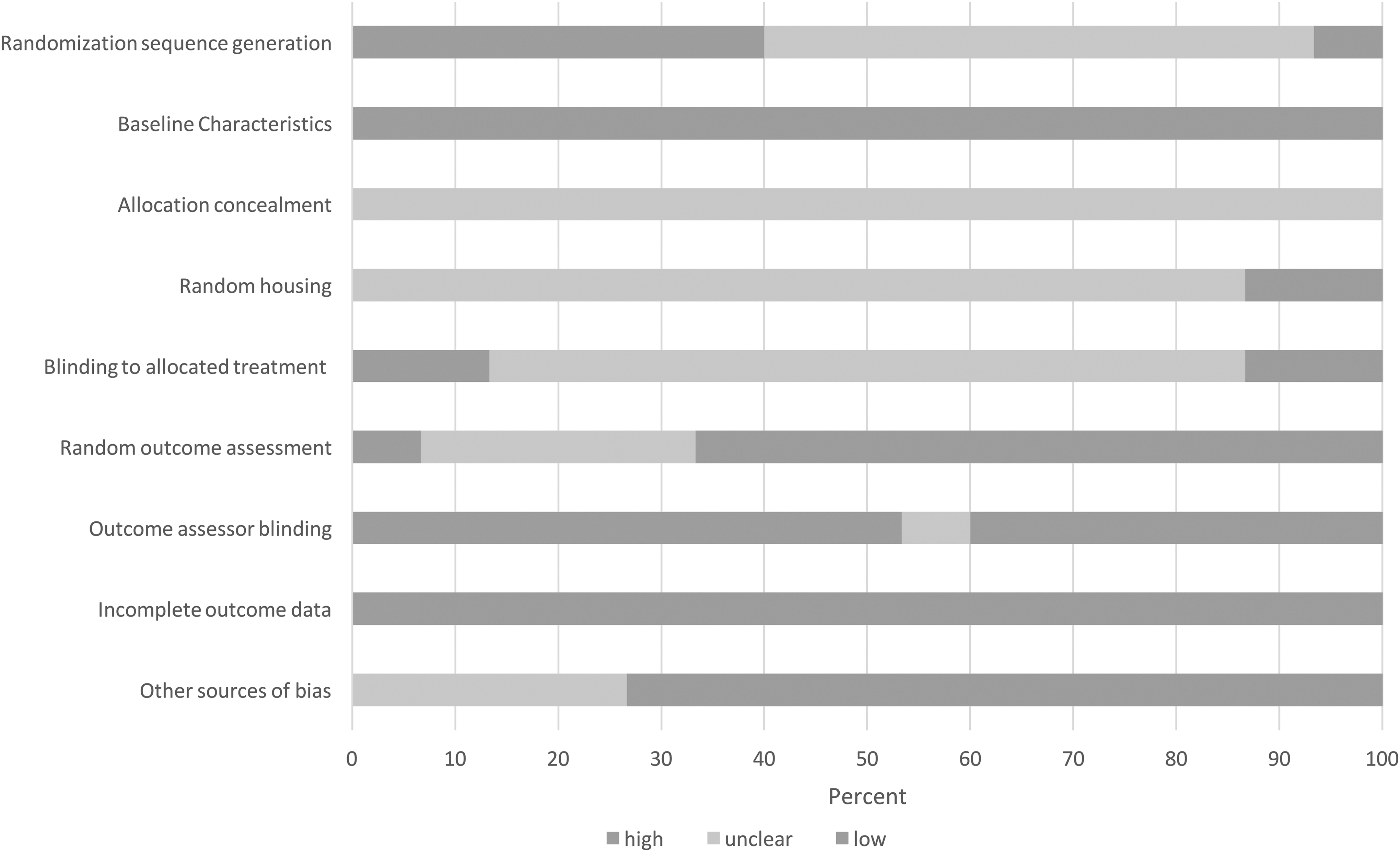
Assessment of bias in 15 animal studies evaluating the efficacy of melatonin to improve traumatic brain injury (TBI) outcome using the SYstematic Review Centre for Laboratory animal Experimentation (SYRCLE) risk of bias tool.
Outcome
A variety of outcome measures were used (see Table 3). The commonest were (1) brain water content as a marker for cerebral edema (eight studies) reported between 8 and 72 h post- injury, (2) lesion/contusion volume (seven studies) measured between 8 h and 14 days post-injury, (3) Neurological Symptom Scores (NSS) or variant (five studies), and (4) the Morris Water Maze test (MWM) (escape latency; used in four studies). The NSS, when used, was measured repeatedly between 1 h and 7 days post-injury (see Table 3). Similarly, the MWM test was measured repeatedly between day 1 and 4 post-injury except in one study. 68 These measures were used in meta-analyses of the pre-clinical studies. All motor outcomes differed in each of the four studies (see Table 3). Some motor outcomes required more balance and coordination (e.g., Rotarod test) than others (e.g., Grip test). Correct effect sizes and significance levels are reported in Table 5.
Mean, Standard Deviation, Effect Sizes, and 95% Confidence Intervals for Individual Pre-Clinical Study Results
Higher score = more favorable outcome.
Bold indicates statistical significance.
NSS, Neurological Severity Score; mNSS, modified mNSS; VCS, vetinary coma score; MWM, Morris Water Maze; NCM, Novel Context Mismatch, OF, Open Field; EPM, Elevated Plus Maze; FS, Forced Swim; BW, Beam Walking; MR, Motorod; BB, Balance Beam; ICP, intracranial pressure.
Stratified meta-analyses
There was a significant effect of treatment with MEL on both pathological outcome measures (Fig. 2), and behavioral measures (Fig 3).
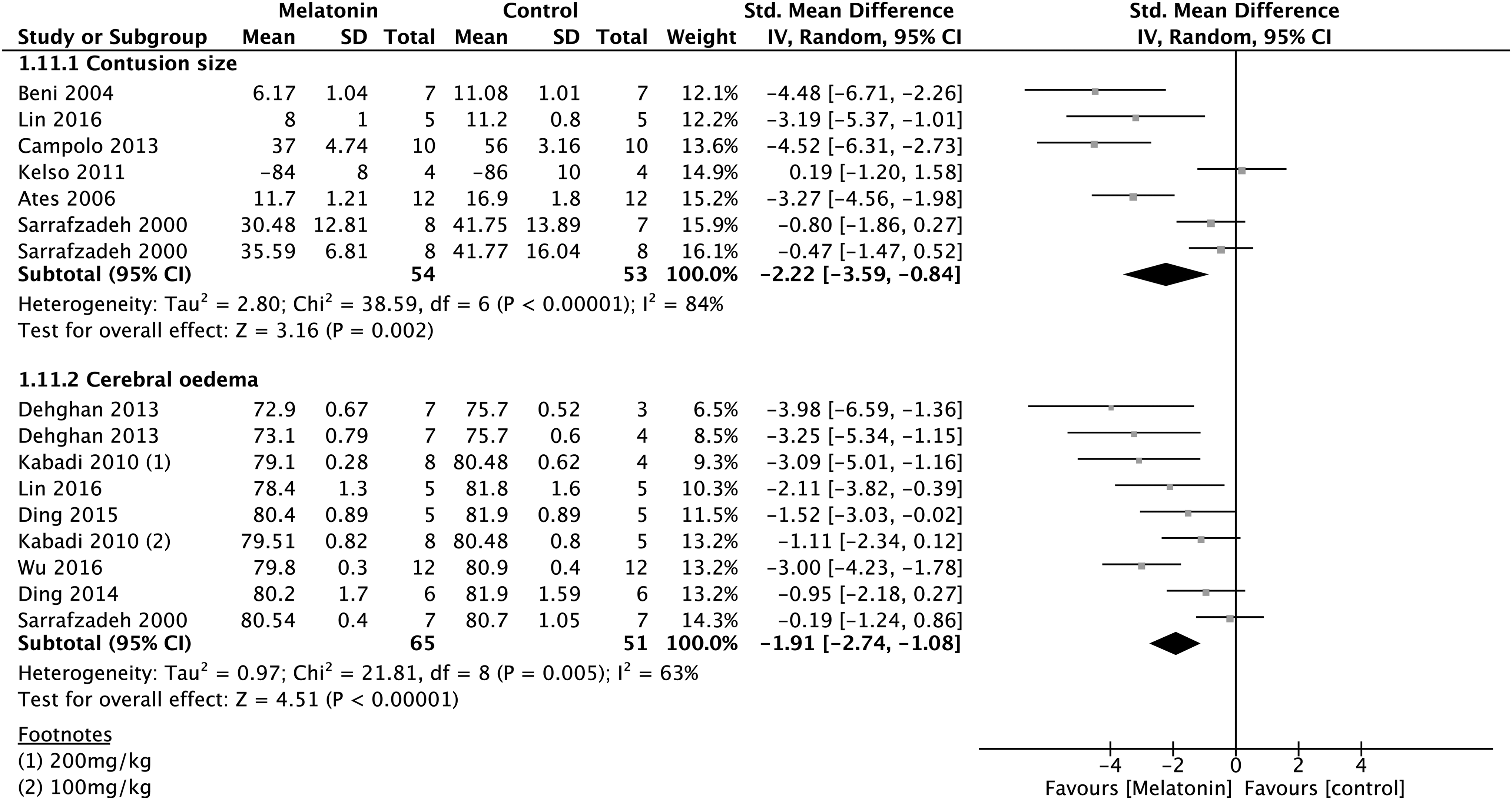
A Forest plot demonstrating the effect of melatonin in comparison with control (vehicle) on pathological outcome measures in pre-clinical studies of traumatic brain injury.
Pathological outcomes
MEL decreased the size of the contusion by an SMD of 2.22 (95% CI: 0.84, 3.59; six studies, seven comparisons). The effect size was large, being >3.0 for four of the six studies, with the largest being 4.5. 40 MEL decreased cerebral edema by an SMD of 1.91 (95% CI: 1.08, 2.74; six studies, nine comparisons). Six of nine studies reported significantly large effect sizes ranging from 1.5 to 3.9. There was significant heterogeneity among the studies (I 2 : 84%). However, this finding was supported by two studies not included in the meta-analysis. One reported a decrease in intracranial pressure (ICP) in association with MEL treatment. 63 In another study, MEL had a similar effect on brain protrusion (a marker of increased ICP) as 20% mannitol, 61 a first-tier therapy for increased ICP following TBI. 76
Behavioral outcomes
MEL treatment had a favorable effect on the neurological status (see Fig. 3), by an SMD of 1.35 (95% CI: 0.83, 1.88; five studies, eight comparisons). The outcome closest to 24 h post-injury was compared in the meta-analysis. Five of the eight experiments reported significantly large effect sizes associated with MEL treatment, ranging from 1.0 to 3.5. Meta-analysis demonstrated that overall, MEL improved the performance on a memory-based cognitive task by an SMD of 1.16 (95% CIs: 0.4, 1.92). There was a large effect size ranging from 1.1 to 2.4. Only one study examined the effect of MEL on mood and anxiety. 72 This was done between days 7 and 13 post-injury, and showed no effect of treatment. Motor outcomes were also improved by MEL (SMD 0.93; 95% CI:0.69, 1.93).
Overall effect
When all studies and comparisons were combined, the overall outcome was improved by an SMD of 1.51 (95% CI, 1.06, 1.96; 15 studies, 20 comparisons, see Fig. 4). One outcome measure from each study was included in the following order of priority: neurological status, cognitive function, contusion size, and cerebral edema. As expected, the heterogeneity was moderately high (I 2 58%). Nine comparisons had effect sizes >1.5.

Forest plot demonstrating the effect of melatonin in comparison with control (vehicle) on behavioral outcome in pre-clinical studies of traumatic brain injury.
Dose, timing of intervention, and frequency
Four studies examined the effect of differing doses on outcome. 63,66, 69,74 The dose, timing, and frequency of interventions varied greatly, making it difficult to draw conclusions. The effects of frequency of dose regimes and timing of interventions were analyzed in ad hoc subgroup analyses of the overall outcome. Interventions were considered to be “early” if given before 30 min and late if given after 60 min (see Fig. 5). There was no significant effect of single versus multiple dosing (χ2 2.26, df 1; p = 0.13) or of “early” or “late” treatment subgroups (χ2 0.2, df 1; p = 0.66, see Fig. 5).

Subgroup meta-analysis: efficacy of intervention versus control (vehicle) in pre-clinical studies examining single versus multiple dose and early (within 30 min) versus late treatment (≥ 1 h). Random effects assumed; 95% confidence intervals; effect of heterogeneity, I2; 200 mg/kg (1, 12), 5mg/kg (2, 10, 11, 13, 19, 21), 20 mg /kg (3, 5, 14, 15), 100 mg/kg (4, 16), 1 mg/kg (6), nighttime administration (7,17), 10 mg/kg (8, 20), daytime administration (9,18).
Clinical studies
Two clinical studies were identified. There was no placebo-controlled study. Kemp and coworkers examined the effectiveness of MEL in seven male adults with sleep disturbance and the study was of good methodological quality except for being significantly underpowered. 76 The TBIs ranged from mild to severe and had occurred 36 months (range: 9 − 73) previously. A double-blind randomized crossover study was performed using 5 mg of oral MEL in comparison with 25 mg amitriptyline for 4 weeks. 76 There was no effect of MEL treatment on sleep or neuropsychological parameters compared with the active comparator, amitriptyline. No adverse events were reported.
Kuczynski and coworkers reported an open-label retrospective cohort study of children (mean age 14 years, SD 3.1) with post-concussion syndrome and post-traumatic headaches 8 months following mild TBI. 46 Although a beneficial effect of MEL was reported – 75% (95% CI: 49, 88) had >50% improvement in the number of headaches – the study was uncontrolled. The effect on sleep was not reported. No adverse events were reported. Caution should be observed when drawing any conclusion from this study, because of its low methodological quality.
Discussion
The goal of this review was to systematically evaluate the literature for the efficacy of MEL as a potential treatment to improve outcome after TBI. Pre-clinical intervention studies, although often focused on a biological construct, ideally have either a pathological or a behavioral outcome consistent with clinical realities in order to add validity and allow clinical correlation. By necessity, pre-clinical studies often have small sample sizes. A systematic review combined with meta-analysis allow the data to be methodologically and objectively assessed. This is the first systematic review of the evidence supporting the use of MEL in animal models and humans with TBI. Based on the results of our meta-analysis in pre-clinical studies, there is potential for treatment with MEL to improve functional outcome.
MEL significantly improved neurobehavioral outcome in neurological, cognitive, and motor domains, as well as in histopathological domains (contusion size and cerebral edema). There was an overall positive standardized mean difference of 1.51 (95% CI, 1.06, 1.96). This is similar to its effect in a systematic review of pre-clinical stroke models 77 and meta-analysis of MEL as a treatment for pain in adults. 78 Although the results of this meta-analysis are strengthened by the effect seen across multiple species (mouse, rat, and rabbit), it is significantly weakened by the significant methodological differences, especially dose and timing of treatments.
After injury, MEL was administered within minutes or up to several hours later, and was used as a single treatment in some and as repeated treatment in other studies. Timing theoretically could target different mechanisms; for example, early administration affecting glutamate toxicity and free radical formation; and later doses targeting neuroinflammation. 13,21 As secondary brain injury is a rapidly progressive process, especially in the first few days, timing of drug administration is likely to be important. 4 In humans, MEL achieves maximum concentrations at ∼45 min when given orally (2 h if given intravenously), except when slow-release preparations are used (2 h), and its half-life is ∼2 h. 57 Here, although earlier treatment was found to be beneficial in one larger study, 69 we did not find an effect of single versus multiple dosing regimens or of early versus late initiation of treatment in subgroup meta-regression analysis. However, the variability of drug dosage (total dose: 2.5–300 mg) make these assessments less reliable. This is especially relevant as larger doses of MEL result in greater serum concentrations, at which supraphysiological non-receptor-mediated effects occur (e.g., direct free radical scavenging, enhancement of mitochondrial function). 27 For example, two studies found MEL 5 mg/kg was more effective than 1 mg/kg or 2.5 mg/kg. 69,74
Most pre-clinical studies had moderate or unclear risks of bias. A key factor in this was the lack of reporting detail to allow satisfactory experimental evaluation. Further, many investigators failed to either randomize or blind assessors and animal carers to the treatment condition. No studies provided sample size estimation or published protocols. This emphasizes the need for more rigor in applying reporting standards and for the publishing of experimental protocols.
In clinical studies, there was a lack of well-designed and adequately powered trials, and the two studies identified in the review evaluated the use of MEL in the chronic phase of TBI recovery for specific symptoms, headache, 46 and sleep. 76 These were of low quality. The randomized controlled crossover trial was significantly underpowered, and was unlikely to detect difference from an active comparator (amitriptyline). 76 The other clinical study was retrospective. 46 Overall, although MEL was well tolerated, there was a lack of data to support the use of MEL as a neuroprotective agent or for specific symptom management in clinical populations.
This current study has many strengths. First, it is a systematic review of the current evidence and followed a published protocol method to ensure a diligent and rigorous review process. By conducting a meta-analysis, studies were combined to increase overall sample size and statistical precision. Finally, included studies had functional neurological outcomes across the many domains of neurological impairment seen after TBI, and, therefore, clinical inferences can be easily made.
Although we attempted to be comprehensive, this review may have failed to identify studies and also may be subject to publication bias. We did not include unpublished data, and this may have skewed our results. All the studies in this review had small sample sizes and when combined with a relative paucity of studies, the meta-analysis is limited by a small data set. This systematic review has not investigated dosage or length of treatment beyond the first few days. It was not possible to examine the effects of MEL in specific TBI populations such as youth and the elderly, who may have different responses to the treatment. Nor were there sufficient studies to allow the evaluation of its use in different TBI pathologies; for example, diffuse versus focal injury.
Conclusions
There is evidence from pre-clinical studies that MEL treatment after TBI significantly improves both behavioral and pathological outcomes; however, significant research gaps exist. There are insufficient clinical data to support routine use following TBI, but further clinical research is warranted to evaluate whether MEL is a viable and safe adjunctive treatment to improve outcome after traumatic brain injury.
Footnotes
Acknowledgments
This work was supported by the Alberta Children's Hospital Foundation Neurotrauma Grant (RT34396). Dr. Barlow was supported in part by a tuition scholarship from the University of Queensland.
Author Disclosure Statement
No competing financial interests exist.