
Abstract
Diffuse axonal injury (DAI) is characterized by diffuse white matter (WM) disruption caused by shearing forces acting on the brain. Cortical atrophy can be accompanied by WM disruption, which is assumed to reflect the loss of neuron cell bodies in gray matter (GM) regions adjacent to disrupted WM. It remains unclear whether WM disruption leads to regional GM alteration in DAI. The aim of the present study was to assess WM disruption and corresponding GM alterations in patients with DAI using a connectome-based approach. Twenty-four patients and 24 healthy controls underwent magnetic resonance imaging with diffusion tensor imaging (DTI). Deterministic fiber tracking was conducted to investigate structural connectivity between the corpus callosum (CC) and each pre-defined regional cortical area. We calculated 85 × 85 connectivity matrices for fractional anisotropy (FA). Group comparisons were conducted to identify abnormal connectivity in patients. Further, the regional cortical volume of each connectivity matrix was compared between patients and controls. Finally, correlation analyses between the matrices and regional cortical volumes were performed within the patient group. Connectome analyses revealed that, compared with controls, patients exhibited a FA reduction in connectivity via CC to 32 cortical regions including the frontal, parietal, and occipital cortices. Among these regions, GM volume was reduced in 19 of 32 regions. There were no significant correlations between WM disruption in which abnormal connectivity was identified and the corresponding GM alterations. These results suggest that GM pathology is, at least in part, independent of the corresponding WM damage in DAI.
Introduction
The pathology of diffuse axonal injury (DAI), a major form of traumatic brain injury (TBI), is characterized by diffuse white matter (WM) disruption caused by shearing forces associated with sudden acceleration, deceleration, or rotation of the brain. 1 Primary axotomy may occur within minutes to an hour after injury as an initial response to trauma. Axonal degeneration progresses over time after injury, and WM pathology, including damage of brain structural connectivity, becomes evident as secondary axotomy over weeks or months after trauma. Secondary axotomy may persist for years, affecting functional outcomes for individuals with DAI. 2
As axons wither and begin to degenerate, the accumulative loss of axons results in reduced WM volume. 3 WM volume reduction measured by high-resolution magnetic resonance imaging (MRI)-based morphometric analysis has been reported in the corpus callosum (CC), brainstem, longitudinal fasciculus, and fornix 4 –9 in DAI.
In addition to volume reduction in the WM, microstructural alterations, measured with diffusion tensor imaging (DTI) parameters such as fractional anisotropy (FA), have been reported in patients with DAI. The reduction of FA in DAI is considered to reflect primary and secondary axonal injury, 5,10,11 and has been reported in several WM regions, including the CC, cingulum, superior and inferior longitudinal fasciculus, uncinated fasciculus, and brainstem fiber tracts. 9,12
Among these WM regions, the CC is one of the most commonly affected regions of WM in DAI. 13 –16 We recently reported that robust reductions in volume and FA occurred in the CC of patients with DAI. Further, in our previous study, among various WM regions, only the CC showed significant structural alterations after correcting for multiple comparisons. Further, we reported that structural alterations of the CC in patients were correlated with impaired processing speed, 9 a core deficit following TBI including DAI. 17 Thus, the CC appears to be an important region for DAI from a clinical perspective.
In addition to WM disruption, gray matter (GM) alteration is also common among individuals with TBI. GM volume reduction in TBI has been reported in subcortical regions such as the insula, thalamus, amygdala, and nucleus basalis. 7,12,18,19 Regarding the cortical GM, reduced cortical volume and thickness have been reported in the frontal gyrus and temporal gyrus. 6 –8,12,18,20 These significant losses of cerebral GM volume were found to occur even in those without focal lesions, suggesting that volume reduction may result from DAI with secondary Wallerian degeneration leading to delayed neuronal cell death, rather than direct damage to neuronal cell bodies. 6,19,21
However, experimental model studies have shown that traumatic axonal injury does not necessarily result in death of the corresponding cell body in rats. 8,22 In addition, as highlighted in a review by Buki and Povlishock, because the progress of traumatic axonal alteration is slow, neuronal cell bodies can reorganize and survive even with progressive changes evoked by DAI. 23 These findings conflict with the notion that secondary Wallerian degeneration always leads to delayed neuronal cell loss, mentioned previously. Therefore, the relationship between WM injury and volume loss in corresponding GM in DAI remains unclear. 19 Although both WM disruption and cortical GM alteration have been reported in patients with DAI, no previous study has comprehensively investigated whether WM disruption leads to corresponding regional cortical GM alteration in the brains of patients with DAI.
The aim of the present study was to assess WM disruption and its direct relationship with corresponding GM alteration in patients with DAI in detail using a connectome-based approach. Based on the results of previous studies, 9,13 –15,24 including our own, we focused on structural damage to transcallosal fibers.
Methods
Participants
Participants were recruited from the outpatient clinic of the neuropsychology unit at the Department of Psychiatry, and at the Department of Neurosurgery, Kyoto University Hospital. Inclusion criteria for patients were: (1) an injury sustained through significant trauma, (2) brain MRI showing possible diffuse pathology without large focal lesions (> 10 mm 3 ), (3) being older than 18 years of age, and (4) the injury having occurred at least 5 months before the study. Exclusion criteria were: (1) visual or visuoperceptual deficits, (2) history of another TBI, (3) history of drug abuse, or (4) history of neurological or psychiatric disorders before TBI onset.
Twenty-four patients with TBI (17 males, mean age of 40.2 years, standard deviation [SD] 12.5) participated in the study. Eight of the 24 patients had participated in our previous study. 9 Table 1 shows patient demographic and clinical information. Four patients (16.7%) had mild TBI, 1 (4.1%) had moderate TBI, and 19 (79.2%) had severe TBI, according to the Glasgow Coma Scale (GCS) or Japan Coma Scale (JCS), a measure of the severity of impaired consciousness used in Japan. The relationship of the JCS score to severity of injury has been explored previously. 25 The comparison group comprised 24 healthy individuals (17 males, mean age of 39.1 years, SD 10.1) matched to the TBI group for age and sex.
Demographic and Clinical Characteristics
DAI, diffuse axonal injury; HC, healthy controls.
This study was approved by the Committee on Medical Ethics of Kyoto University and was conducted in accordance with the Code of Ethics of the World Medical Association. Written informed consent was obtained after participants had been given a complete description of the study.
Procedures: MRI acquisition and pre-processing
All participants underwent MRI scans with a 3T whole-body scanner with a 40 mT/m gradient and a receiver-only 32 channel phased-array head coil (MAGNETOM Tim Trio, Siemens, Erlangen, Germany). The scanning parameters of the T1-weighted three-dimensional magnetization-prepared rapid gradient-echo (3D-MPRAGE) sequence were as follows: repetition time (TR) = 2000 ms; echo time (TE) = 4.38 ms; inversion time (TI) = 990 ms; field of view (FOV) = 225 × 240 mm; matrix = 240 × 256 mm; resolution = 0.9375 × 0.9375 × 1.0 mm 3 ; and there were 208 total axial sections without intersection gaps. DTI scanning parameters were as follows: TE = 96 ms; TR = 10,500 ms; 96 × 96 matrix; FOV = 192 × 192 mm; there were 70 continuous axial slices of 2.0 mm thickness, 64 non-collinear volumes with b = 1500 s/mm 2 , and a volume with b = 0 images, with a field map.
Data processing and statistical analysis
Data pre-processing
3D-MPRAGE data were processed using SPM8 (

Examples of fiber tracking for a patient with diffuse axonal injury (DAI) as well as for a healthy subject. GCC, genu of the corpus callosum (CC); BCC, body of the CC; SCC, splenium of the CC. Color image is available online.
Connectivity matrices
From the 90 regions of the Automated Anatomical Labeling (AAL) atlas, 31 we selected 82 cortical regions of interest (ROIs) excluding subcortical nuclei. In addition, we selected three ROIs (genu, body, and splenium of the CC) from the Johns Hopkins University (JHU) white-matter atlas. 32
For each pair of brain regions i and j, deterministic fiber tracking was calculated using the command line version of the Diffusion Toolkit. It was then determined whether they were structurally connected by examining if one or more streamlines were included with two-end points in brain regions i and j. If two regions were structurally connected, FAij of a connection was defined as the mean value of FA across all voxels of all connection fibers. If no streamline was found between brain regions i and j, FAij was defined by 0. These procedures were performed using an in-house MATLAB script. In this way, we obtained symmetric 85 × 85 connectivity matrices for FA.
Network analysis
Statistical analyses were performed using the network-based statistic (NBS; Melbourne Neuropsychiatry Center, the University of Melbourne and Melbourne Health, Australia) 33,34 with a t-statistic exceeding a threshold of t = 3.1 and a familywise error (FWE)-corrected p value <0.05 for the size of each resulting component using 5000 permutation tests. Group comparisons were conducted to identify abnormal connectivity in patients with DAI relative to controls. The effects of age and gender were excluded from the group comparisons as nuisance covariates. The results were visualized using an in-house connectome viewer written in C++.
Regional GM volume analysis
GM volumes in regions in which abnormal connectivity was identified were compared between DAI patients and the controls. To investigate the direct relationship between WM disruption and corresponding cortical GM alteration in the following correlation analysis, we calculated regional GM volume using same ROIs with 82 cortical regions based on the AAL atlas that were applied connectivity matrices. The voxel values of segmented and normalized GM images were multiplied (modulated) by the Jacobian determinants obtained from non-linear normalization steps. For each ROI, values from the modulated GM probability map were averaged over voxels. We conducted a series of one way analyses of variance (ANOVAs) with diagnosis as a between-subjects factor, using GM density as a dependent variable. P < 0.05 was considered statistically significant after Bonferroni correction for multiple comparisons.
Correlation analysis between WM and GM
To investigate the relationship between WM disruption and GM alterations, correlation analyses between the abnormal FA values and the corresponding regional GM volumes were performed in the DAI group. Bonferroni–Holm correction was performed for multiple comparisons. Further, partial correlation analyses between FA values and the corresponding regional GM volumes were performed to control for the effects of the time from injury, because there is wide range of time since from injury on our subjects. Statistical analyses were conducted using SPSS 22.0 software (IBM Corp., Armonk, NY) for GM volume analysis and correlation analysis.
Results
Group comparisons in connectivity analysis
Connectome analysis revealed a significant reduction in FA in the connections from the CC to 32 cortical regions, including the superior frontal gyrus, middle frontal regions, inferior frontal gyrus, Rolandic operculum, rectus gyrus, supplementary motor area, cingulate gyrus, calcarine, cuneus, superior occipital gyrus, postcentral gyrus, superior parietal gyrus, and precuneus in the DAI group relative to controls (Table 2 and Fig. 2). There were no connections that showed increased FA in the DAI group compared with controls.
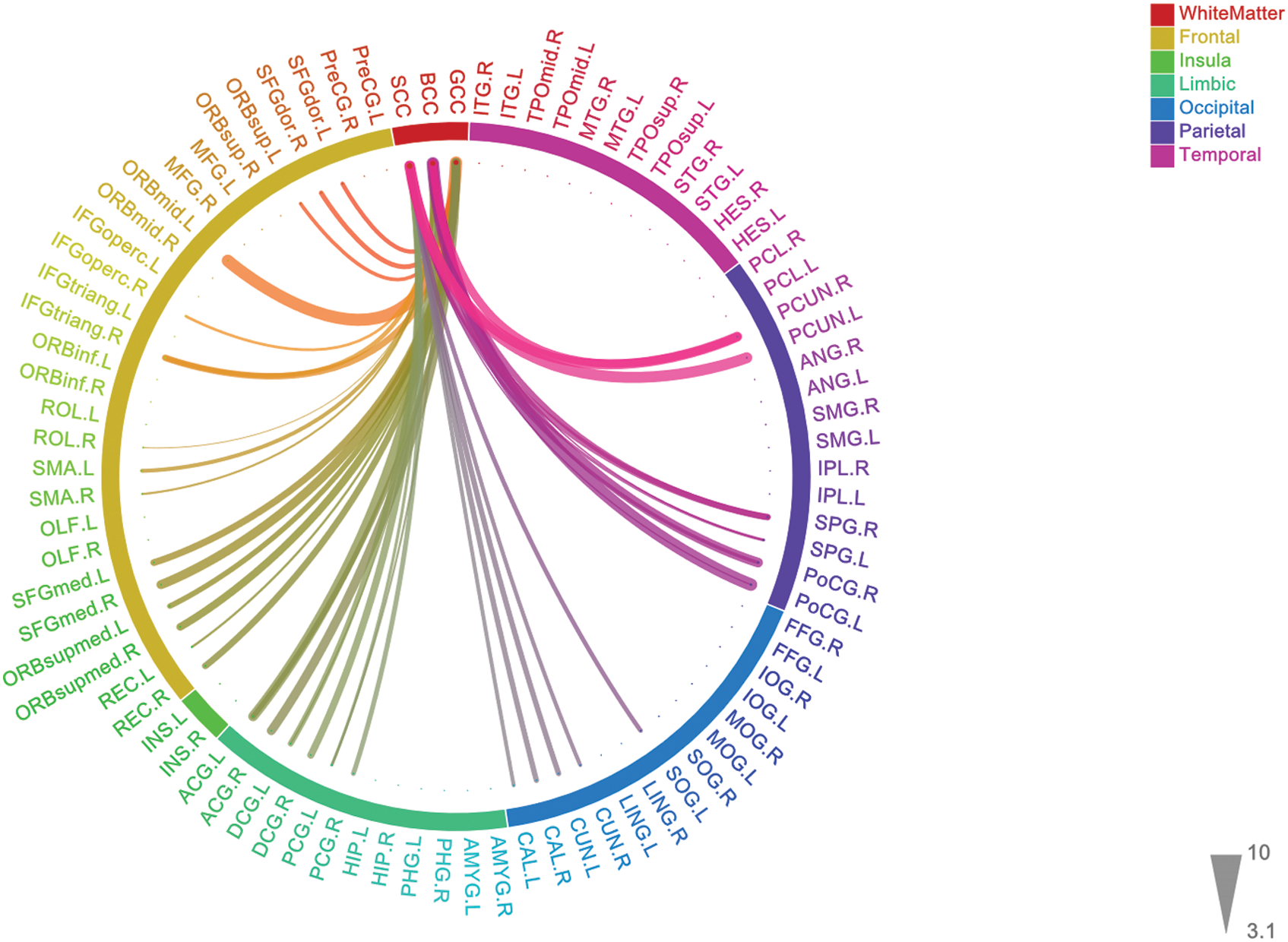
Group comparisons in the connectome analysis. Patients showed reduced FA between the CC and certain cortical areas, comprising frontal, limbic, occipital and parietal regions. A threshold of t = 3.1 and a family-wise error corrected p < 0.05, using 5000 permutation tests, were applied. The thickness of connections indicates the t-score. L, left; R, right; GCC, genu of the CC; BCC; body of the CC; SCC, splenium of the CC. PreCG, precentral gyrus; SFGdor, superior frontal gyrus, dorsolateral; ORBsup, superior frontal gyrus, orbital part; MFG, middle frontal gyrus; ORBmid, middle frontal gyrus, orbital part; IFGGoperc, inferior frontal gyrus, opercular part; IFGtriang, inferior frontal gyrus, pars triangular part; ORBinf, inferior frontal gyrus, orbital part; ROL, Rolandic operculum, SMA, supplementary motor area; OLF, olfactory cortex; SFGmed, superior frontal gyrus, medial; ORBsupmed, superior frontal gyrus, medial orbital; REC, gyrus rectus; INS, insula; ACG, anterior cingulate and paracingulate gyri; DCG, median cingulate and paracingulate gyri; PCG, posterior cingulate gyrus; HIP, hippocampus; PHG, parahippocampal gyrus; AMYG, amygdala; CAL, calcarine fissure and surrounding cortex; CUN, cuneus; LING, lingual gyrus; SOG, superior occipital gyrus, MOG, middle occipital gyrus; IOG, inferior occipital gyrus; FFG, fusiform gyrus; PoCG, postcentral gyrus, SPG, superior parietal gyrus; IPL, inferior parietal, but supramarginal and angular gyri; SMG, supramarginal gyrus; ANG, angular gyrus; PCUN, precuneus; PCL, paracentral lobule, HES, heschl gyrus; STG, superior temporal gyrus; TPOsup, temporal pole: superior temporal gyrus; MTG, middle temporal gyrus; TPOmid, temporal pole: middle temporal gyrus; ITG, inferior temporal gyrus. Color image is available online.
Group Comparisons in the Connectome Analysis
GCC, genu of the corpus callosum (CC); BCC, body of the CC; SCC, splenium of the CC.
Regional GM volume analysis
Among the 32 regions where abnormal connectivity was identified in the DAI patients, there was a significant reduction of GM volume in 19 regions, including the right supplementary motor area, bilateral medial superior frontal gyrus, bilateral left orbital part of the medial superior frontal gyrus, bilateral rectus, bilateral anterior and dorsal cingulate gyrus, right posterior cingulate gyrus, bilateral calcarine regions, bilateral cuneus, left superior occipital gyrus, and bilateral post-central gyrus (Table 3 and Fig. 3). The number of regions showing significant volume reduction was the same without multiple comparison correction. There was no region that showed increased GM volume in the DAI group compared with controls.
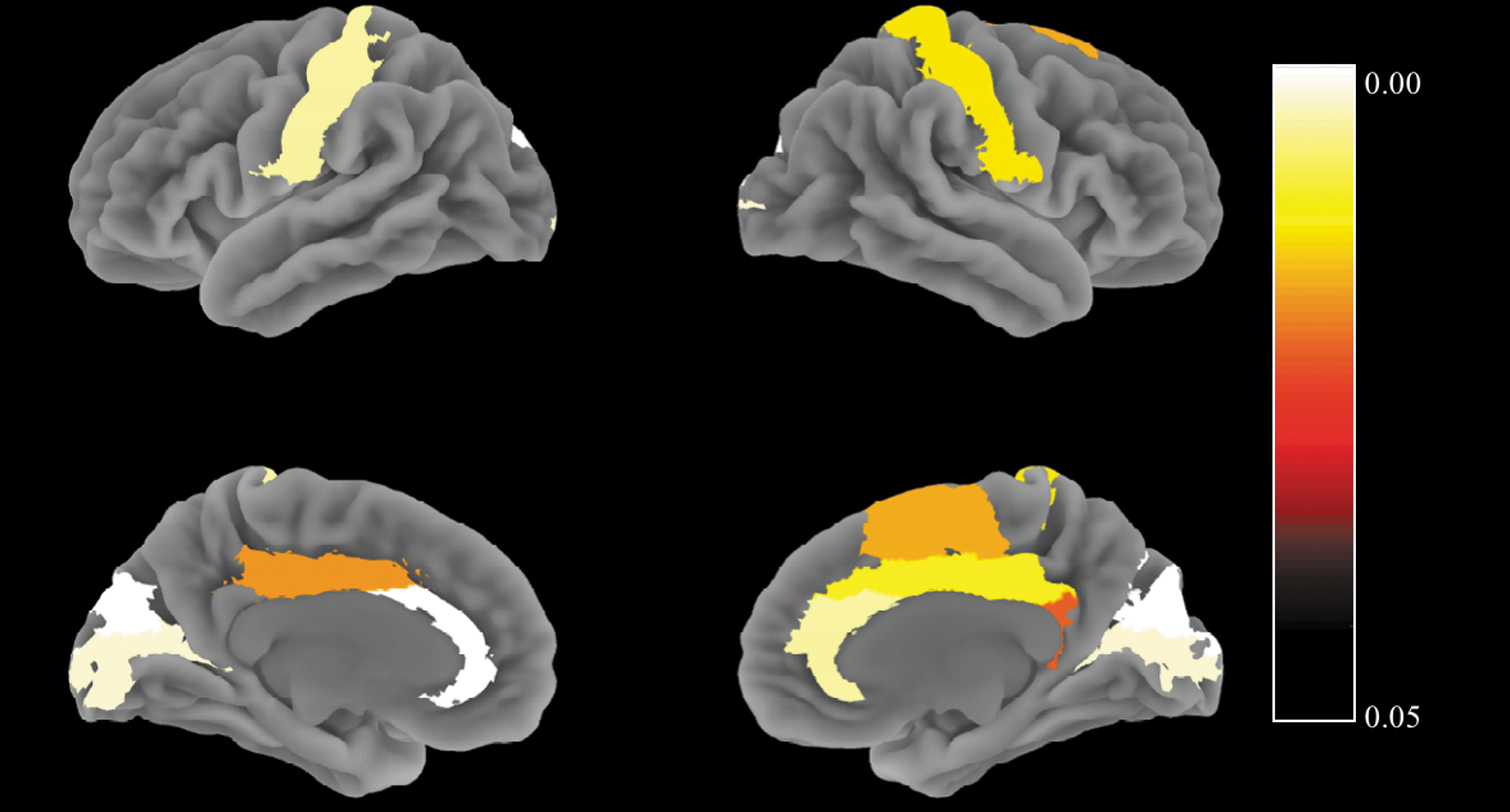
Results of group comparison in regional gray matter (GM) volume analysis. Patients showed GM volume reduction in the right supplementary motor area, bilateral medial superior frontal gyrus, bilateral orbital part of the medial superior frontal gyrus, bilateral rectus, bilateral anterior and dorsal cingulate gyrus, right posterior cingulate gyrus, bilateral calcarine regions, bilateral cuneus, left superior occipital gyrus, and bilateral post-central gyrus. Colored bar indicates the p value in the group comparison. Color image is available online.
Group Comparison of Regional Grey Matter Volumes
DAI, diffuse axonal injury.
Significant at p < 0.05 with Bonferroni correction.
Correlation analysis between WM and GM
There was no significant correlation between FA in connectivity and the corresponding GM volume in each of the 19 regions mentioned. The range of Pearson correlation coefficients was 0.05–0.53 (Table 4). There were weak or moderate correlations between FA in connectivity to bilateral medial superior frontal gyrus (left: r = 0.48, p = 0.09; right: r = 0.53, p = 0.007), right calcarine regions (r = 0.46, p = 0.02), and right cuneus (r = 0.52, p = 0.01) and the corresponding GM volume, but they did not survive correction for multiple comparisons. Significance level was adjusted by Bonferroni–Holm correction from 0.002 to 0.003 (0.05/19 to 18 respectively).
Pearson's Correlations between Fractional Anisotropy Values and Corresponding Gray Matter Volumes
GCC, genu of the corpus callosum; BCC, body of the corpus callosum; SCC, splenium of the corpus callosum;
L, left; R, right.
We also performed partial correlation analyses for FA in connectivity and the corresponding GM volume in each of 19 regions to control for the effects of time since injury. The correlations between the right medial superior frontal gyrus, right cuneus, and the corresponding GM volume were still significant after controlling for time since injury, but they did not survive correction for multiple comparison (r = 0.44, p = 0.04 and r = 0.44, p = 0.04, respectively). The correlation between the left medial superior frontal gyrus, right calcarine regions, and the corresponding GM volume was not significant when time since injury was included in to the controlling variables (r = 0.41, p = 0.06 and r = 0.35, p = 0.11, respectively).
Discussion
In the present study, our main aim was to determine which transcallosal fibers exhibited prominent structural damage in DAI patients using a connectome technique, and to examine whether GM alterations would be accompanied by WM alterations. Connectome analyses showed reduced FA in connectivity between the CC and specific cortical regions, including the middle frontal gyrus and precuneus, in patients with DAI. Mixed results were observed regarding regional GM volume where connectivity via the CC was altered; the corresponding GM volume was reduced in some regions, such as the medial superior frontal gyrus and cuneus, but remained intact in other regions, including the superior parietal gyrus and precuneus. Further, no correlation was found between the degree of FA reduction and the corresponding regional GM volume reduction in patients with DAI.
Our finding of FA reduction in connectivity via the CC is consistent with previous reports. 35 –37 The CC, the largest commissural WM pathway in the brain, is an important region in DAI pathology, because it is particularly vulnerable to shearing forces acting on the brain. 38 Additionally, alteration of the CC is reported to be related to functional outcomes in TBI. 39 Here, we revealed that CC connectivity in DAI was particularly disrupted in the connections to certain regions, including the frontal and occipital lobes, and precuneus. This suggests that altered connectivity via transcallosal fibers may differ depending on the cortical regions to which the fibers were connected. This regional difference may reflect the variable vulnerability of subcomponents of transcallosal fibers to the shearing forces involved in DAI.
Patients with DAI exhibited reduced GM volume in 19 of 32 regions where abnormal connectivity was identified. Regional GM volume reductions were evident in the superior frontal gyrus, anterior cingulate gyrus, calcarine regions, cuneus, and superior occipital gyrus. These findings are generally consistent with previous studies in patients with DAI. 12,19,40 Based on animal data, after primary axotomy, immediate mechanical damage to the axonal cytoskeleton along with axon swelling occurs in minutes to hours. In contrast, secondary axotomy; that is, progressive axonal degeneration, occurs days to months after injury. 41 This pathological change might cause GM volume reduction in the chronic stage in patients with DAI. Therefore, volume reductions, which were found in 19 of 32 cortical regions in the present study, may be caused by the consequences of traumatic axonal injury. In contrast, GM volume in another 12 regions remained intact even if the adjacent WM was disrupted. This may be attributable to compensatory mechanisms. Indeed, previous studies have reported that although traumatic axonal injury causes cell death and degeneration, it also induces growth-related events that enable remaining neurons near and distant to the lesion's locus to survive, repair, and form new connections. 42,43
One novel finding in the current study was the absence of significant relationships between WM disruption and corresponding cortical GM alteration. To the best of our knowledge, only one previous study has investigated the relationship between WM axonal integrity including the CC and regional GM volume. 44 In contrast to our results, the study's authors found a significant relationship between FA reduction in the CC and GM volume in several cortical regions, such as the parietal region, frontal lobule, and precuneus. This discrepancy might be the result of differences in methods between the two studies. We measured the FA of fibers connecting the CC and cortical regions, and assessed the relationships between FA values and regional cortical volumes. In contrast, Werner and coworkers measured average FA value of the whole CC, GCC, and SCC, and assessed the relationships between FA value and regional cortical volume selected based on their previous study. 19
The current study has several limitations that should be considered. First, our sample was restricted to patients without focal lesions, because it is technically difficult to process and analyze imaging data of individuals with focal lesions in an automated manner, which was employed in this study. However, the majority of patients with severe TBI have focal lesions. Therefore, we cannot generalize our findings to entire TBI population. Second, we focused on patients in the chronic phase. Consequently, we cannot generalize our findings to patients in the acute or subacute stage. However, our chronic sample is suitable for examining whether WM disruption leads to GM alterations. Third, although we focused on CC alterations in the current study, WM alterations have also been reported in other WM tracts, such as brainstem fiber tracts and longitudinal fasciculi. 1,45,46 The CC is the most affected WM region in DAI, but further research including of other WM tracts, such as longitudinal fibers, is warranted to achieve a better overview of WM-GM impairments in DAI. Fourth, in the analyses, we focused on FA and did not include other DTI measures such as median, radial, and axial diffusivity. Although these DTI measures have also been shown to be altered in TBI, 47 among these DTI measures, FA is reported to be used more frequently than other DTI measures in TBI. 48 Future studies investigating WM disruption and corresponding GM alterations measured by other DTI parameters in DAI would provide more detailed information on the relationships between GM and WM alterations in this population.
Footnotes
Acknowledgments
The authors thank all participants for their contribution to this project. This work was supported by an Industrial Disease Clinical Research Grant (150502-02), a Health Labour Sciences Research Grant, a Grant-in-Aid for Young Scientists B (15K19722) and C (17K10327) from the Japan Society for the Promotion of Science, and a research grant from the General Insurance Association of Japan.
Author Disclosure Statement
No competing financial interests exist.