
Abstract
Recent data demonstrate improved locomotion with high-intensity locomotor training (LT) in individuals with incomplete spinal cord injury (iSCI), although concerns remain regarding reinforcement of abnormal motor strategies. The present study evaluated the effects of LT intensity on kinematic and neuromuscular coordination in individuals with iSCI. Using a randomized, crossover design, participants with iSCI received up to 20 sessions of high-intensity LT, with attempts to achieve 70–85% of age-predicted maximum heart rate (HRmax), or low-intensity LT (50–65% HRmax), following which the other intervention was performed. Specific measures included spatiotemporal variables, sagittal-plane gait kinematics, and neuromuscular synergies from electromyographic (EMG) recordings. Correlation analyses were conducted to evaluate associations between variables. Significant improvements in sagittal-plane joint excursions and intralimb hip-knee coordination were observed following high- but not low-intensity LT when comparing peak treadmill (TM) speed before and after LT. Neuromuscular complexity (i.e., number of synergies to explain >90% of EMG variance) was also increased following high- but not low-intensity LT. Comparison of speed-matched trials confirmed significant improvements in the knee excursion of the less impaired limb and intralimb hip-knee coordination, as well as improvements in neuromuscular complexity following high-intensity LT. These findings suggest greater neuromuscular complexity may be due to LT and not necessarily differences in speeds. Only selected kinematic changes (i.e., weak hip excursion) was correlated to improvements in treadmill speed. In conclusion, LT intensity can facilitate gains in kinematic variables and neuromuscular synergies in individuals with iSCI.
Introduction
Rehabilitation strategies for individuals with incomplete spinal cord injury (iSCI) are often directed toward ameliorating neuromuscular impairments, 1 although their efficacy on walking outcomes is not clear. Recent studies have suggested specific training parameters may facilitate locomotor outcomes following neurological injury. 2,3 Studies in animal models 4 –7 and humans with SCI suggest that repeated locomotor (i.e., walking) training (LT) may improve walking function as compared with non-walking practice, 8,9 although the efficacy of different LT strategies vary. For example, despite previous literature regarding the potential utility of treadmill (TM) stepping with body-weight support and physical assistance, the efficacy of this strategy as compared with other overground training is uncertain and varies between studies. 10 –13 The available data suggest additional training parameters beyond task-specific practice alone may contribute to improved locomotor outcomes.
More recent data suggest that the intensity of LT, defined as power output and estimated indirectly with heart rate (HR) or oxygen consumption, 14 may be a potentially critical variable that can facilitate walking function in patients with neurological injury. Selected studies 15,16 indicate greater improvements in locomotor function following LT at moderate to vigorous (hard) intensities as compared with lower-intensity LT. In individuals with iSCI, the potential role of LT intensity is not often assessed, 17,20 as achieving higher intensities is often not an explicit goal. 11,13 A recent pilot investigation evaluating high- versus low-intensity LT in iSCI revealed greater improvements in maximum TM and overground speed, as well as peak aerobic capacity and gait efficiency (i.e., reduced oxygen consumption at similar speeds), using the former strategy. 21 Although these gains are promising, concerns remain regarding changes in underlying motor control strategies in response to high-intensity LT. More directly, traditional rehabilitation theories suggest higher-intensity activities promote abnormal muscle activation strategies, 22,23 which may be reinforced with repeated training. Indeed, abnormal intralimb muscle co-activation strategies and their contributions to walking recovery following neurological injury continues to be an area of injury research. 24 –26 Regardless, previous studies have demonstrated that increased walking capacity and efficiency may also be attributable to changes in kinematic or neuromuscular strategies, 27 –29 possibly due to greater magnitude or rate of neuromuscular activation. However, multiple studies suggest minimal changes in co-activation or timing of neuromuscular strategies associated with locomotor recovery. 30 –32
Emerging literature suggests use of other computational strategies may provide greater insight into muscle coordination patterns. More directly, various techniques such as principle component analyses (PCA) or non-negative matrix factorization (NNMF) may provide insight into the organization of specific patterns of muscle coordination (or motor synergies) that can be combined to generate specific motor behaviors. 33 Previous work suggests these synergies can be flexibly reorganized to accomplish various biomechanical tasks, 34,35 although the capability of such reorganization may be limited following neurological injury. 36 –38 Determination of specific muscle synergies may facilitate understanding of potential mechanisms underlying various rehabilitation strategies, including following high-intensity training. More directly, changes in the magnitude or combination of muscle coordination patterns may reflect plastic changes in neural commands to successfully accomplish various functional tasks, whereas limited changes may reflect reinforcement of aberrant motor strategies, as suggested by traditional theories of rehabilitation.
The goal of the present study was to evaluate changes in kinematic and neuromuscular strategies following high- versus low-intensity LT in individuals with iSCI. Using a randomized, crossover design, functional gains between these protocols have been described previously, 21 although underlying patterns of kinematic and neuromuscular coordination utilized to accomplish these gains were not presented. Here, we evaluate changes in lower-extremity joint kinematics (joint excursion and coordination) and neuromuscular patterns (synergistic activation of muscles) prior to and following high- versus low-intensity to evaluate whether high-intensity LT may improve locomotor biomechanics, or whether aberrant motor patterns are reinforced with such training. Subsequent correlation and regression analyses were used to evaluate potential associations between these changes and improvements in locomotor function (i.e., walking speed). These data may provide insight into selected mechanisms underlying improved locomotor function with specific training interventions.
Methods
Patient population
Participants with chronic (>1 year) iSCI, classified as C or D using the American Spinal Injury Association (ASIA) Impairment Scale, with a neurological injury level of T10 or above were screened. Eligible participants were between 18 and 75 years old, demonstrated intact quadriceps or plantar flexor tendon reflexes, and were capable of overground walking without physical assistance with walking speeds <1.0 m/sec, with assistive devices (e.g., walker or cane) and below-knee braces as needed. Exclusion criteria consisted of the following: severe lower-extremity contractures; history of osteoporosis; cardiovascular or metabolic instability; unhealed decubiti; existing infection; active heterotrophic ossification; previous history of other central nervous system injury; or inability to adhere to study requirements. Participants were restricted from participating in other physical therapy during the study. All research procedures were approved by the Northwestern University Institutional Review Board, and participants provided written informed consent. All subjects underwent complete motor evaluation using Lower Extremity Motor Scores (LEMS) to determine their weaker and stronger limb. 17
Intervention
In this pilot investigation, we utilized a randomized crossover design to evaluate the preliminary efficacy of high- versus low-intensity LT on walking outcomes in iSCI. Participants received up to 20 1-h sessions of either a high- or low-intensity LT within 4 to 6 weeks, followed by a 4-week washout, 19,43 after which participants received the other LT paradigm. The washout period was adopted from previous literature. Goals of the training sessions were to achieve up to 40 min of stepping practice in variable contexts (tasks and environments 43 ), while achieving the desired intensity ranges. Training intensity was evaluated primarily by HR, with high-intensity LT targeting 70–85% of age-predicted maximum HR (HRmax; calculated as 208 − [0.7*age]), and low-intensity targeting at 50–65% HRmax. The former range has been utilized in previous studies evaluating the effects of high-intensity LT, 21 with lower ranges approximating HRs achieved during conventional physical therapy. 44,45 If targeted HRs could not be achieved, the rating of perceived exertion (RPE) scale was utilized, with high-intensity LT targeting “hard” to “very hard” and low-intensity targeting (< “somewhat hard”). 17,21
The primary training goals during both high- and low-intensity LT have been articulated previously 42,43 and included: (1) maximizing the amount of successful stepping practice in a specific direction; (2) achieving specific HR intensities; and (3) increasing difficulty of skilled walking tasks as tolerated. Each training session was composed of four different intervention subcomponents, namely (i) speed-dependent, (ii) skill-dependent, (iii) stair, and (iv) overground training, each practiced for 10 min per training session. Speed-dependent TM training focused on walking forward on a TM while maintaining targeted HRs. Limb-swing assistance, body-weight support, and nylon straps stabilizing the pelvis were provided as needed to ensure successful stepping, characterized by positive step lengths, lack of stance-phase limb collapse, and sagittal/frontal plane stability. Skill-dependent TM training was designed to challenge postural stability, propulsion, and limb swing by altering the biomechanical demands of stepping tasks. Skill training consisted of walking in multiple directions, over inclines and over obstacles, with and without ankle weights, with limited handrail use as tolerated. Selected tasks were intermittently practiced within the 10-min time frame allocated to skill training, with specific tasks selected by the treating therapists based on patients-specific gait deficits. Overground training focused on speed- or skill-dependent locomotor activities similar to those described above, with use of a gait belt or overhead suspension system for safety. Additional stepping activities included walking over uneven or narrow surfaces and stepping around obstacles. Stair climbing was also performed for 10 min over static or rotating stairs (Stairmaster, Vancouver, WA) with attempts to use reciprocal gait patterns and progression to higher speeds and reduced handrail use as able.
Training sessions were administered and supervised with licensed physical therapists, with documentation of total stepping duration, types of practiced tasks, HR, and RPE. Patients were provided as many rest breaks as needed, but were encouraged to achieve as much stepping practice as possible (up to 40 min) during the 1-h sessions while achieving the targeted HR range. Approximately one to eight rest breaks were provided as needed, with a reduced number of resting episodes during low-intensity LT. Amount of stepping per session was measured using accelerometers on the ankle of the more impaired limb (StepWatch, Modus, Washington, DC). Patients' HR was continuously monitored using pulse oximeters with forehead sensors (Masimo, Inc., CA).
Data collection
Each patient completed four separate gait assessments, including immediately prior to and following completion of 6 weeks (20 sessions) of high- and low-intensity LT paradigms. 44 Collection of gait kinematics and electromyographs (EMGs) were performed during a graded TM test performed on a split-belt TM with embedded force plates surrounded by an eight-camera motion capture system (Motion Analysis Corp., Santa Rosa, CA). Initial TM speed was 0.1 m/sec with increases of 0.1 m/sec every minute until the participant experienced significant gait instability, could not continue walking at that speed, or requested to stop. All participants wore a safety harness to minimize fall risk and were not provided any body-weight support. The highest TM speed that participants could achieve for 1 min was recorded as peak TM speed. During testing, 32 reflective markers were placed bilaterally on pelvis, thighs, shank, and foot (modified Cleveland Clinic 6 degrees of freedom [DOF] model), 45 and 12 EMG electrodes (Ag/AgCl Noraxon USA Inc., Scottsdale, AZ), were placed bilaterally on the following lower extremity muscles: medial gastrocnemius (MG), medial hamstring (MH), vastus lateralis (VL), rectus femoris (RF), tibialis anterior (TA), and soleus (SOL). A total of 30 sec of data were collected at each speed. Participants could hold onto bilateral handrails, which were instrumented with 6 DOF load cells (JR3 Inc., Woodland, CA). Kinematic data were sampled at 100 Hz, with analog EMG and load cell data sampled at 1000 Hz.
Data analysis
Kinematic data were processed using Cortex software (Motion Analysis Corp., Santa Rosa, CA), and further analyzed using custom pipelines in Visual3D (C-Motion Inc., Germantown, MD) and MATLAB (Mathworks, Inc., Natick, MA). Marker and force data for all walking trials were filtered using a low-pass, second-order Butterworth filter (10 Hz). Joint excursion and spatiotemporal measurements were calculated from the transformation between the respective model segments. A full stride was identified as the period when the vertical ground reaction force exceeded 25 N and confirmed with the most anterior position of the calcaneal marker and most posterior position of the metatarsal marker. Kinematic measures were normalized to percentage of the gait cycle and average step cycle profiles were created. Additional kinetic variables could not be accurately analyzed due to participant's inability to place each limb on separate TM belts.
Kinematic variables of interest included bilateral sagittal hip, knee, and ankle joint angles, sagittal joint excursions, and hip-knee joint coordination characterized using a cyclogram of sagittal hip versus knee angles. This cyclogram was quantified in terms of its stride-to-stride consistency (i.e., “consistency”) and its shape skewness (SKW). Consistency was calculated as the angular component of the coefficient of correspondence (ACC), 17,46 whereas SKW was quantified as the ratio of hip to knee joint excursion during a gait cycle. The ACC ranges between 0 and 1, with values closer to 1 indicating further stride-to-stride variability to accommodate stepping demands. SKW is an uni-dimensional variable with values between 0.60 and 0.80 representing healthy individuals. 47
EMG signals were band-pass filtered with a finite impulse response filter (Lancosh type 79-point window filtering, band-pass range from 30 to 450 Hz), rectified, and smoothed using root mean square calculations over a 50-msec window.
48
All EMG waveforms were visually inspected, with removal of gait cycles with substantial movement artifact or low signal-to-noise ratio, with at least 20 gait cycles included for each participant. EMGs were amplitude-normalized to the corresponding average of their peak values across all available cycles. Specific analyses of EMG activity were performed using NNMF, a computational technique that extracts the underlying principals from interdependent, often redundant, EMG signals.
33
NNMF is widely used to factorize the experimental EMG signals into a reduced number of independent activation signals (namely neural commands) and groups of muscles that are activated together in response to a neural command, namely synergy coordination.
36,37
Of note, factorized activation signals, referred as neural command, are fabricated computationally and do not represent the actual neural commands from the central nervous system. However, the terminology is well-accepted across the literature and is adopted for the rest of this study. Mathematically, normalized EMG signals, arranged as a (100 × 6) matrix, was split into two matrices; synergy activation or neural command (H) and synergy coordination (W) such that:
where “n” refers to the size of factorization. An example of inputs and outputs of NNMF is presented in Figure 1. Considering the redundancy of the neuromuscular system, size of factorization (n) can vary between one (i.e., assuming that all muscles were activated simultaneously through a single neural command) and six (i.e., assuming that each muscle is activated with a separate neural command). NNMF determines the smallest size of factorization (n) to minimize the Euclidian distance between experimental EMG and W × H such that the latter explains at least 90% of the variance in experimental EMG:
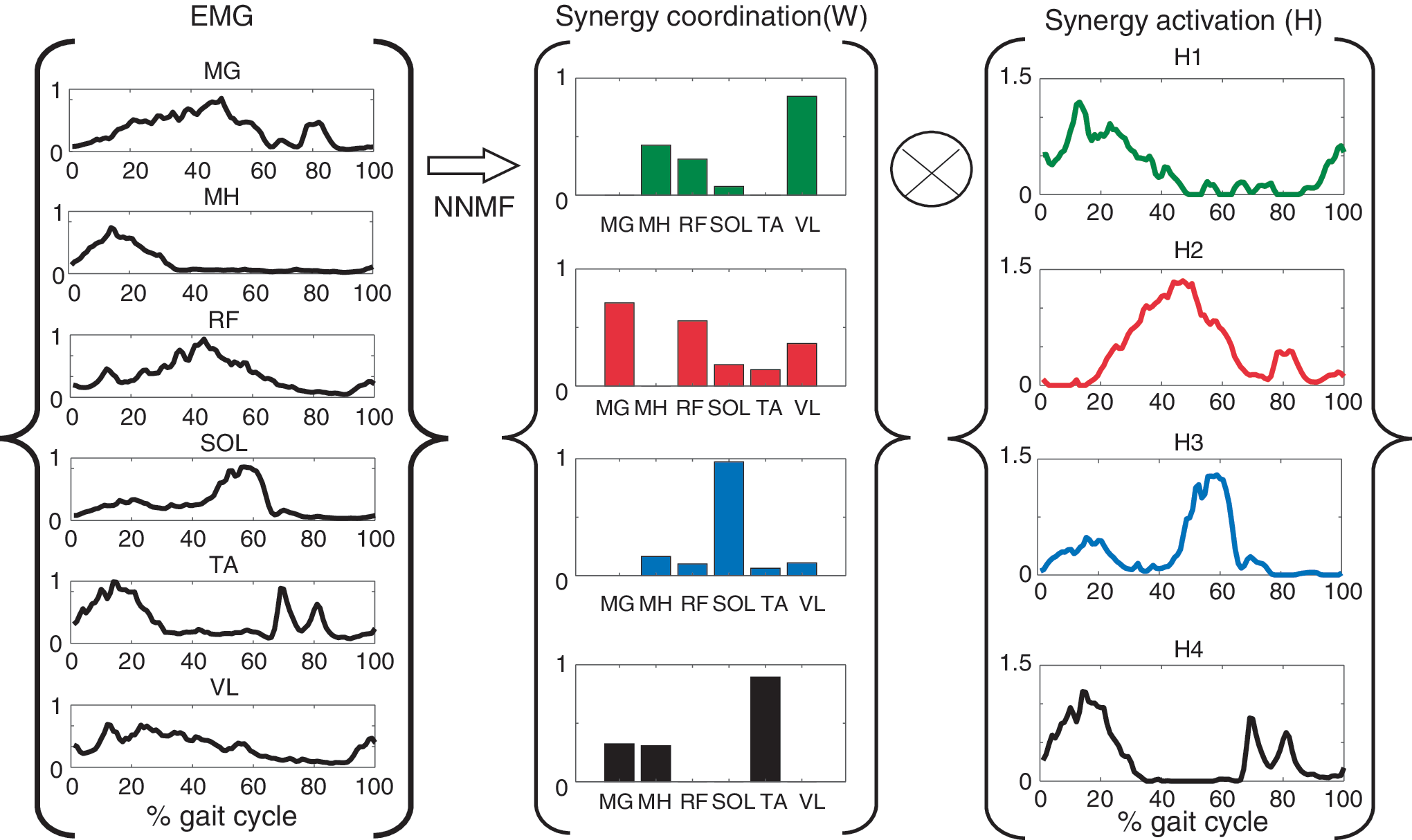
Schematic representation of neuromuscular synergy analysis. Six normalized electromyographic (EMG) envelopes were arranged in a matrix (100 × 6) and imported into non-negative matrix factorization (NNMF). This iterative optimization algorithm seeks the smallest number of activation profiles (Synergy activation: H), which suffice to regenerate the original EMG signals with at least 90% accuracy. Synergy activation profiles (H) and synergy coordination (W) are then determined so as to minimize the error between original EMG measurements and reconstructed EMG signals (W × H). In this schematic diagram, the optimization algorithm of NNMF has been solved for four synergies leading to H (4 × 100) and W (6 × 4). MG, medial gastrocnemius; MH, hamstring; RF, rectus femoris; SOL, soleus; TA, tibialis anterior; VL, vastus lateralis. Color image is available online.
where VAF represents the variance accounted for and i refers to every 1% increment in normalized gait cycle. The quality of NNMF is determined by the accuracy of reconstructed EMG (VAF > 90%). The VAF may be calculated for each individual EMG signal, the entire EMG matrix, or for various portions of gait cycle (stance and swing). Presented in this study, n was determined such that VAF > 90% was achieved for every and all EMG signals. Size of factorization, n, was then chosen as the variable of interest. According to previous literature, a higher n value in NNMF indicates the existence of independently timed muscle activations to accommodate specific biomechanical demands (weight transfer, limb swing, etc.) within a gait cycle, whereas lower values of n indicate over-lapping (i.e., non-discrete) synergies and co-activation of multiple muscles. 41 Accordingly, the variable n is often interpreted as neuromuscular complexity and higher complexities (i.e., large n) repeatedly reported to associate with higher function and better coordination in patients with neurological injuries. 36,37 To maintain consistent terminology with previous literature n (i.e., the smallest number of independently timed synergy activations necessary to reconstruct the experimental EMG signals with at least 90% accuracy 37 ) is referred as “neuromuscular complexity” for the rest of this study. Neuromuscular complexity was calculated separately for weak and strong limbs of each participant.
Statistical analysis
Repeated-measures analyses of variance (ANOVA) were used to compare the outcomes before enrolling in high- versus low-intensity LT to ensure that a participant's locomotor performance was equivalent prior to each training strategy. With the possibility of differences in participants' walking speed before enrolling, speed was used as a covariate in the repeated-measure ANOVA.
Paired t tests evaluated differences in changes in performance, or post-training (POST) minus baseline (BSL) following high- versus low-intensity LT. With this pilot evaluation, Bonferroni corrections were not performed to identify any differences with such training. Two separate paired tests were conducted for each LT paradigm, including changes in measured variables before and following the 6-week period (BSL vs. POST) at peak TM speeds achieved, as well as measures at BSL to similar measures at POST with speeds matched to participants' BSL peak TM speed (BSL vs. POST-MATCH). These latter comparisons allowed for evaluation of potential changes while adjusting for changes due to higher speeds. In addition, paired t tests also evaluated potential changes within each training paradigm (BSL to POST or POST-MATCH).
Step-wise multiple-linear regression models were used to investigate any potential relationships between changes in the participants' peak TM speed during high- or low-intensity LT and changes in gait kinematics or neuromuscular synergies observed. In addition, correlation and regression analyses were employed to investigate what kinematic variables were associated with improvements in peak TM speed. All statistical analyses were conducted using SPSS (v22, IBM, Armonk, NY).
Results
Twelve of the 17 participants with viable EMG recordings and kinematic data at all assessments (prior to and following each training paradigm) were included. Demographic characteristics for the sample were as follows: 10/2 male/female, average (± standard deviation [SD]) age of 50 ± 8.7 years, duration post-iSCI of 7.6 ± 8.5 years, and lower-extremity motor scores of 39 ± 6.1. Repeated-measure comparisons confirmed that patients received significantly higher aerobic intensities at high- versus low-intensity LT paradigms, measured in terms of average peak %HRmax (high: 127 ± 23 vs. low: 107 ± 19; p < 0.001) and peak RPE (16 ± 1.3 vs. 13 ± 1.1; p < 0.001). There were no differences in number of sessions (19 ± 2.6 vs. 19 ± 2.7; p = 0.24) or steps/session between training conditions (1750 ± 994 vs. 1716 ± 673; p = 0.91). The total duration of stepping practice documented by therapists ranged from 16 to 40 min across all subjects, with trends for greater minutes in low-intensity LT, and more breaks during high-intensity LT. Six individuals enrolled in high-intensity rehabilitation first. Our previous study showed that changes in peak TM speed are not affected by the order of training paradigms. 21
Changes in spatiotemporal and joint kinematics
Following high-intensity LT (BSL to POST), significant gains in TM speed (0.75 ± 0.38 to 1.0 ± 0.40 m/sec, p < 0.01) and non-significant increases in both cadence (88 ± 43 to 98 ± 33 steps/min, p = 0.52) and stride length (1.07 + 0.30 to 1.12 + 0.26 m, p = 0.83) were observed. Following low-intensity training, participants showed no changes in TM speed (0.70 ± 0.21 to 0.75 ± 0.38 m/sec, p = 0.15), cadence (86 ± 32 to 88 ± 46 steps/min, p = 0.34), or stride length (1.20 ± 0.33 to 1.29 ± 0.34 m, p = 0.37).
Following high-intensity LT (BSL to POST), specific improvements were observed in joint kinematics including significant increases at bilateral hip joint excursions (strong: p = 0.04; weak: p = 0.01) and strong limb knee excursion (p = 0.02). More specifically, significant increases at bilateral hip (strong: p = 0.02; weak: p = 0.03) and knee (strong: p = 0.03; weak: p = 0.04) flexion angles were observed following high-intensity training. Hip-knee flexion coordination (i.e., ACC) also improved bilaterally with changes reaching statistical significance only at weaker limb (p = 0.04; Fig. 2), with reductions in ankle dorsiflexion approaching significance (p = 0.05). In contrast to high-intensity LT, limited kinematic changes were observed following low-intensity LT (BSL to POST) including significant reduction of bilateral hip extension (strong limb: p = 0.02; weak limb: p = 0.03) and significant increases at bilateral hip flexion (strong limb: p = 0.03; weak limb: p = 0.04). Despite the changes within each training group, there were no significant differences in observed changes between high- and low-intensity LT (Table 1).
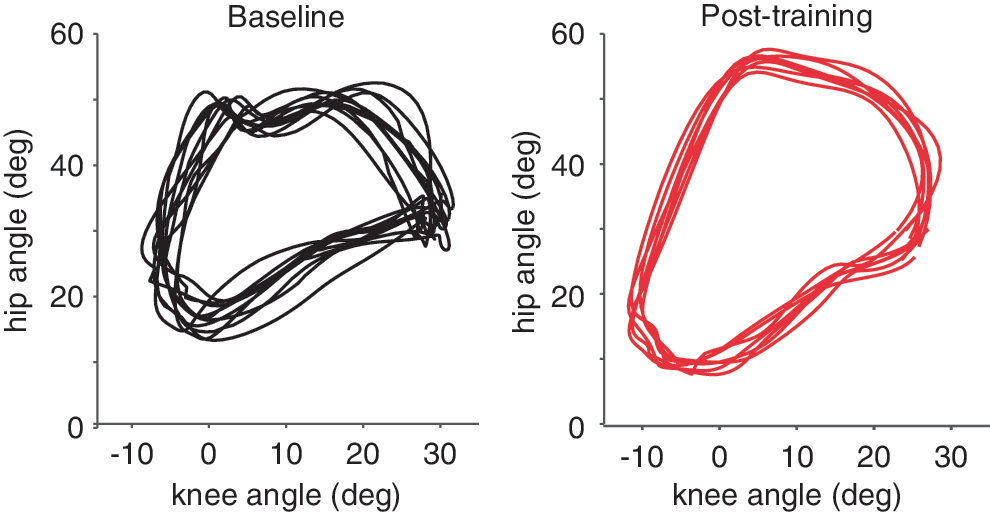
Comparison of intralimb coordination before (BSL) and after (POST) high-intensity training. Angular component of the coefficient of correspondence (ACC) and skewness (SKW) were quantified from the hip-knee cyclogram. Color image is available online.
Paired t Test Comparison of the Gait Kinematic Variables in BSL and POST for Stronger and Weaker Limbs following High and Low-Intensity Training
Peak angles and excursions are in degrees. Angular component of the ACC and SKW are in arbitrary units. P-values indicate between training-group differences. Asterisks indicate within training-group differences from BSL to POST (p < 0.05).
ACC, angular component of the coefficient of correspondence of intralimb hip-knee flexion cyclogram; BSL, baseline; Std, standard deviation; POST, post-training; SKW, skewness of intralimb hip-knee flexion cyclogram (i.e., the ratio of hip to knee range of motion) during a gait cycle.
Evaluation of kinematic changes at matched speeds (POST-MATCH vs. BSL) confirmed significant improvements in knee excursion of the weaker limb (p = 0.02) as well as intralimb hip-knee SKW (strong: p = 0.04l; weak: p = 0.04) with values approaching normal following high-intensity LT (0.60–0.80; Supplementary Appendix Table 1; see online supplementary material at
Changes in neuromuscular coordination
Indices of neuromuscular modules (synergy activation and coordination) were extracted from the EMG signals using NNMF. Neuromuscular complexity (i.e., number of synergies accounting for >90% variance) ranged from three to five synergies (Table 2). Prior to high-intensity LT, the majority of strong (66%) and weak (41%) limbs demonstrated a complexity of four modules. Among these participants, we observed two general distinct patterns of modular organization. For four patients, the first synergy occurred in the initial loading/early stance phase of the gait cycle, which was consisted primarily of RF, VL, and MH activity to support the body weight during initial loading. The second synergy consisted primarily of MG, RF, and VL activity during the mid- to terminal stance phase. During this phase, MG likely assists with propulsion, whereas RF/VL can assist with body-weight support and swing initiation. The third synergy at terminal stance to early swing included SOL activity associated with propulsion. Finally, the fourth synergy consisted of TA, MG, and MH activity with TA assisting with dorsiflexion during swing. In three individuals, a different organization of modules was observed in which the first module (initial loading/early stance phase) consisted of co-activation between MH and MG, and the third module (terminal stance/pre-swing) consisted of co-activation between SOL and RF/VL.
Comparison of Neuromuscular Complexity (i.e., number of synergies with variance inflation factors >90%), High- versus Low-Intensity Training
H/L: received high-intensity LT first, followed by low-intensity LT.
L/H: received low-intensity LT first, followed by high-intensity LT.
Synergies are reported at peak treadmill speed and BSL and POST. Participants presented with fewer synergies on their weaker limb prior to high vs. low-intensity training. POST results revealed greater neuromuscular complexity following high-intensity training.
BSL, baseline; LT, locomotor training; POST, post-training.
Synergy analyses of peak speed trials demonstrated increased neuromuscular complexity from BSL to POST following high-intensity LT (weak limb: 4.3 ± 0.75 to 4.9 ± 0.66, p = 0.01; strong limb: 4.0 ± 0.60 to 4.5 ± 0.52, p = 0.02; Table 2). More specifically, 6/12 and 5/12 participants demonstrated an increase of at least one synergy at their weaker and stronger limbs respectively following high-intensity LT. Increased complexity manifested as greater temporal distinction between synergy 1 (loading response) and synergy 2 (mid-stance), indicating reduced TA and RF co-activation at initial contact and reduced MG and SOL co-activation at mid-stance (see Fig 3). Of those six participants who specifically showed increased synergies at their weaker limb, two demonstrated additional changes; participant 6 (Table 2) demonstrated greater temporal distinction (reduced co-activity) between MH and VL at terminal swing and initial contact, whereas participant 9 demonstrated greater temporal distinction between SOL and TA at terminal stance and initial swing.
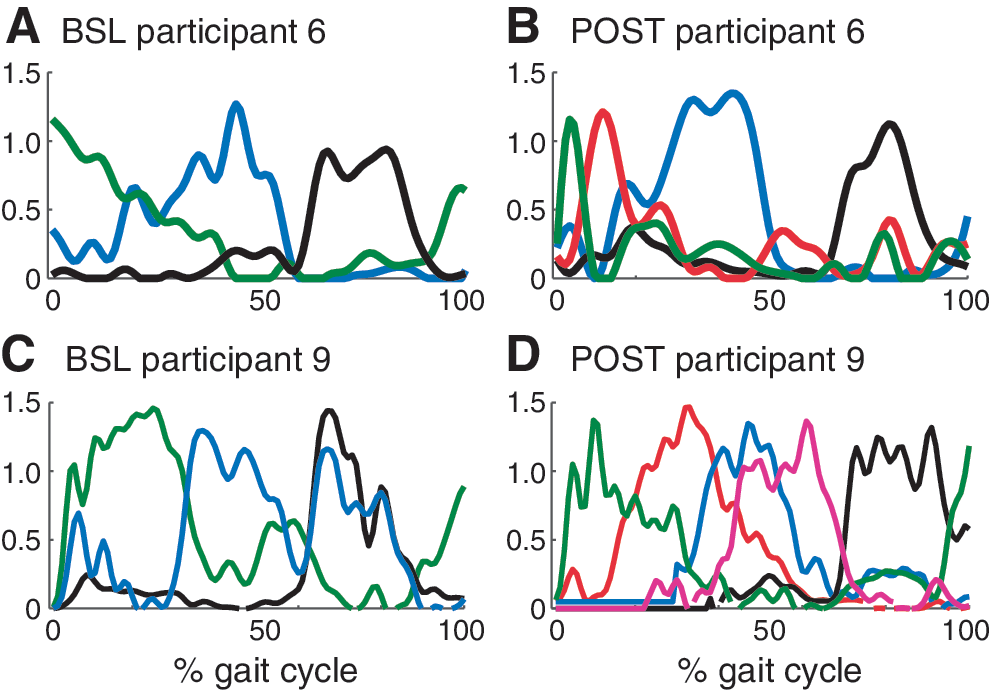
Two representative examples of additional synergy modules formed following high-intensity training.
Prior to low-intensity training, 75% of weaker limbs and 58% of stronger limbs demonstrated a complexity of five synergies. In these cases, a non-significant but potentially important effect of order was observed in neuromuscular complexity. More directly, in 2/6 participants (Subject 4 and 6 in Table 2), who received high-intensity LT first, at least one additional synergy was observed in their weaker limb that was preserved after the washout period. Moreover, 2/6 participants who received low-intensity LT first demonstrated a reduced number of synergies at their stronger limbs following the intervention, which did not recover prior to high-intensity LT (Subject 8 and 10 in Table 2). This residual effect led participants to start high-intensity LT with significantly fewer synergies at their weaker limbs (4.3 ± 0.75) compared with low-intensity LT (4.9 ± 0.51, p = 0.01). Nonetheless, neuromuscular complexity did not change (from BSL to POST) following low-intensity LT at either the weaker (4.9 ± 0.51 to 4.6 ± 0.51, p = 0.10) or stronger limb (4.5 ± 0.67 to 4.6 ± 0.51, p = 0.72).
Synergy analyses at matched-speed trials (POST-MATCH vs. BSL) showed that only 5/12 (instead of 6/12) participants demonstrated increased complexity at their weaker limbs following high-intensity LT. Despite, findings were similar; that is, neuromuscular complexity was increased following high-intensity LT (weak limb: 4.3 ± 0.75 to 4.8 ± 0.57, p = 0.04; strong limb: 4.0 ± 0.60 to 4.4 ± 0.52, p = 0.03) but remained unchanged following low-intensity LT (weak limb: 4.8 ± 0.57 to 4.6 ± 0.51, p = 0.25; strong limb: 4.5 ± 0.67 to 4.6 ± 0.51, p = 0.31).
Association between changes in peak locomotor speed and kinematic measures
Relationships between changes in kinematics and neuromuscular coordination with improved locomotor speed were identified using correlation analyses and multiple linear regressions. Changes in peak TM speed was correlated to changes in hip joint excursion (r = 0.64, p < 0.01), ACC (r = 0.46, p = 0.02) and SKW (r = 0.56, p < 0.01) of the weaker limb as well as knee joint excursion of stronger limb (r = 0.38, p = 0.05). Using multiple linear regression, changes in the weaker hip joint excursion was the only significant predictor of changes in peak speed (r 2 = 0.41, p < 0.001). Changes in the neuromuscular complexity were not directly correlated to the changes in peak TM speed.
Discussion
The present study revealed selected improvements in spatiotemporal and sagittal joint kinematics, as well as neuromuscular synergies, following high-intensity LT in participants with motor iSCI, with limited changes following low-intensity LT. Specific gains in bilateral hip excursion, bilateral hip and knee flexion, weaker limb ACCs, and stronger knee excursion were observed following high-intensity LT. In contrast, bilateral hip extension reduced following low-intensity LT. The complexity of neuromuscular synergies also increased following high- but not low-intensity LT. Specific changes in hip and knee excursion and intralimb coordination, but not neuromuscular complexity, were associated with gains in peak TM speed.
Our previous data suggest higher intensity LT can improve walking speed and metabolic capacity in patients with iSCI, whereas low-intensity LT did not elicit meaningful improvements in locomotor function. 21 High-intensity LT requires greater neuromuscular activation to achieve higher workloads (i.e., power output), 19,20 and potentially facilitates neuroplastic changes, which may contribute to enhanced locomotor performance. 17,18 Subjects in the high-intensity LT achieved higher HRs and RPEs, although total stepping amount was not different from low-intensity LT, potentially due to greater number of rest breaks. During testing, however, to achieve faster speeds, significant gains in joint excursions were observed, and improved kinematic consistency may also suggest improved motor coordination. 46 These results refute the notion that abnormal changes in kinematic strategies would be observed 22,23 ; rather, opposite findings were revealed in the present study (see also Leech and Hornby 17 ).
One particular kinematic finding that may be of interest was related to some of the initial deficits observed and compensations provided during testing and training. Namely, selected participants required an ankle foot orthosis (AFO) to safely ambulate. For these participants, restriction of ankle motion and reduced propulsive forces likely required increased motion from other joints to achieve higher speeds with training. Accordingly, bilateral hip joint excursions and selected changes in knee flexion-extension likely accommodated for these restrictions in ankle function, and allowed some individuals to achieve faster walking speeds following high-intensity LT. 42 We purposely allowed AFO use during training and testing to ensure safety and minimize risk of injury during stepping tasks, although future studies with larger sample sizes should investigate the potential role of AFO use and neuromuscular and kinematic changes with training following neurological injury.
In addition to changes in joint kinematics, the observed changes in neuromuscular synergies are particularly noteworthy, as there is limited information available regarding alterations in the modular organization of neuromuscular strategies following specific training regimens in patients with neurological injury. In the current data, significant increases in neuromuscular complexity were observed following high-intensity training at the fastest speeds achieved at POST, and after controlling for the confounding effect of speed (i.e., POST-MATCH). The latter finding could indicate that the observed gains in neuromuscular synergies may be due to the training effects rather than increasing speeds that were not achievable at BSL testing. Increased neuromuscular complexity in turn may suggest distinctive changes in neuromuscular strategies throughout the gait cycle. The data suggest the potential ability to discretely activate selected motor pools to accomplish various biomechanical demands of the gait cycle, which may contribute to improved speed or kinematic patterns.
Overall, our synergy analyses were partially consistent with previous literature. Similar to published studies, fewer muscle synergies were observed in weaker versus stronger limbs, consistent with observation of reduced number of independent motor modules in patients post-stroke with greater impairments. 37 These findings suggest that in more impaired limbs, there may be a potential inability to de-couple muscle activity or a merging of existing muscle synergies. In this study, we suggest that this de-coupling may be facilitated with the repeated practice of high-intensity LT. In contrast to previous studies that frequently reported a direct association between neuromuscular complexity and locomotor function, our small data set did not confirm any correlation between improvements in walking speed and changes in synergies. Further investigation with a larger sample size may be need to confirm this association for patients with iSCI.
Further, the number of synergies in our study (mostly three to five) seemed to be higher than those often reported for patients with motor iSCI (mostly two to three). 49,50 One explanation is perhaps different approaches to deeming the reconstruction acceptable. In general, a VAF >90% is adopted to choose the number of synergies from the NNMF algorithm. This threshold however may be applied per individual EMG signal (adopted in the present study) or per EMG matrix. The latter may lead to a VAF of <90% when reconstructing single EMG signals. In general, NNMF is a computational algorithm that has been reported to be sensitive to electrode placement, walking speed, or number of muscles considered in the analysis. 51 –53 Therefore, results should be interpreted with caution.
Several limitations of this investigation should be addressed. First, our study recruited a small sample population, and a separate cohort of participants may reveal conflicting results. Indeed, a recent case series delineating the effects of high-intensity variable training in individuals with iSCI revealed variable changes in locomotor function and kinematics. 42 Considering the heterogeneity in functional impairments, comparative training studies with sufficient sample sizes that evaluate neuromuscular changes are scarce. Accordingly, the crossover design was employed; although this paradigm introduces additional limitations such as potential order effects. As such, the washout period of 4 weeks may not be sufficient to fully clear the residual effects of the primary training paradigm. In the present study, non-significant effects of order were observed in neuromuscular synergies, however, and the length of washout period was adopted from literature and in consideration of time limits to assess a training efffect. 21,39 Nonetheless, as reported above, this crossover design may have influenced the number of synergies observed and difference prior to high versus low-intensity LT.
Another limitation was the assessment of locomotor performance on a TM versus overground, and EMG assessments. Despite previous data indicating the general similarities in gait biomechanics observed during walking in these two different conditions, 54 the use of a TM may certainly alter the variability of potential locomotor strategies utilized. Although both BSL and POST assessments were obtained in the same conditions, we cannot be certain that similar differences would be observed with assessments performed overground. Finally, the limitations of EMG analyses were related to measures of neuromuscular coordination, as the magnitude of EMG signals may depend also on the number of patients and testing factors that may vary across testing conditions separated by 6 weeks. Normalization of EMG amplitudes using well-established methods (M-wave normalization) will be necessary to evaluate changes in neuromuscular coordination versus activation.
In summary, the present study evaluated the contributions of training intensity on kinematic and neuromuscular coordination in individuals with iSCI, revealing positive associations between gains in speed and kinematic performance, and with improvements rather than deterioration of gait patterns. Further gain in neuromuscular coordination through synergy analyses were revealed primarily following high-intensity training, although their contributions to improved locomotor performance (i.e., speed) remain unclear.
Footnotes
Acknowledgments
Funding was provided by the National Institutes of Health (R01-NS079751) and the National Institute of Disability and Rehabilitation Research (H133N110014).
Author Disclosure Statement
No conflicting interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.