
Abstract
The rate of paroxysmal sympathetic hyperactivity (PSH) was retrospectively assessed using the Paroxysmal Sympathetic Hyperactivity–Assessment Measure (PSH-AM) scale in patients with disorders of consciousness attributed to traumatic and non-traumatic acquired brain injury during the rehabilitation phase. These results were compared with previous studies carried out in the same clinical scenario, in order to verify the prevalence of PSH signs from 1998 to 2014. The entire sample consisted of 140 patients in vegetative state/unresponsive wakefulness syndrome or minimally conscious state admitted to a neurorehabilitation subacute unit from June 2010 to December 2014. PSH-AM revealed the presence of PSH in 16% of traumatic and 12% of non-traumatic younger patients. In the non-traumatic group, the rate was higher in patients with anoxia-hypoxia (37.5%) etiology than those with vascular brain injury (6.7%). A comparison with previous studies revealed a reduction in the number of PSH cases in traumatic patients. This study provides evidence that PSH-AM can be used prospectively to detect the rate of PSH and stratify severity of signs. Further longitudinal analysis is warranted to confirm the prevalence of PSH signs in non-traumatic brain injured patients.
Introduction
An increase in the activity of the sympathetic nervous system often occurs in the acute phase after acquired brain injury (ABI). According to Baguleyet and colleagues, 1 from 62% to 92% of patients sustaining traumatic brain injury (TBI) will develop some form of autonomic arousal. In some patients, this physiological response to insult, characterized by increased blood pressure, heart rate, respiratory rate, temperature, sweating, muscle spasticity, and pathological posturing, may also persist over time. 2
Wilder Penfield 3 first described these kinds of signs in ABI patients. Since then, this syndrome has been reported both during admission to the intensive care unit (ICU) and during rehabilitation, but for many years there has been a lack of uniformity regarding nomenclature and diagnostic criteria.
A systematic review of studies published up to 20084 identified 81 articles presenting data from patients reporting paroxysmal sympathetic hyperactivity (PSH) after ABI. What clearly emerged from this analysis was the lack of consensus guidelines for the clinical diagnosis. For instance, 31 synonyms were used to describe these crises, indicating a marked variability in the use of terminology by researchers, whereas only one third of the studies used a priori diagnostic criteria. In 2011, experts proposed a consensus work to share diagnostic criteria and develop a tool to be used to promote uniformity in research and clinical practice. 5
After this critical period, the term PSH 2 was chosen because it seemed the most appropriate for the condition that identifies the neurovegetative crises deriving from the paroxysmal hyperactivity of the sympathetic system.
In 2014, Baguley and colleagues 6 reported final conclusions from an international consensus of experts about the conceptual definition of PSH and on how to quantify this disorder. Indeed, the consensus group developed the: Paroxysmal Sympathetic Hyperactivity–Assessment Measure (PSH-AM). This diagnostic tool consists of two separate constructs: 1) the Clinical Features Scale, to assess the presence and severity of excess adrenergic and motor activity, and 2) the Diagnosis Likelihood Tool, to evaluate the probability of PSH signs.
Our group has performed several epidemiological evaluations of PSH symptoms in ABI patients. In two different retrospective studies, investigating the outcome of 333 patients 7 and 169 patients 8 in vegetative states after massive brain injury, we found a decreasing rate of PSH over time, ranging from 32% (for TBI) and 16% (for non-traumatic causes) between 1998 and 2005 to 18% and 7%, respectively, between 2006 and 2010.
The aim of this study was to: 1) evaluate the rate of PSH in patients with disorders of consciousness (DOCs), attributed to traumatic and non-traumatic ABI; and 2)compare these results with previous studies carried out in the same scenario, in order to confirm the trend of decreased PSH rate in ABI patients.
Methods
This was an observational retrospective study of patients with DOCs attributed to acquired brain injury with a traumatic, vascular, or anoxic-hypoxic etiology, admitted to the neurorehabilitation subacute unit of the S. Anna Institute (Crotone, Italy) from June 2010 to December 2014. The patients were at their first admission to the rehabilitation unit because they had been transferred directly from ICU or neurosurgery.
The study only included patients who at the time of admission were in vegetative state/unresponsive wakefulness syndrome (VS/UWS) 9 or minimally conscious state (MCS), according to the Coma Recovery Scale-revised (CRS-r). 10 The CRS-r was administered by expert neuropsychologists within 48 h of admission. Patients were excluded if they had other comorbidities, such as spinal cord injury, or other neurological diseases or conditions of brain disability attributed to a previous injury.
The rate of PSH was assessed retrospectively using the PSH-AM, which is based on the severity of the clinical signs and the likelihood of diagnosis. Adding together the scores of the two components produces an unlikely diagnosis score of <8, possible diagnosis score of 8–16, and likely diagnosis score of ≥17. 6
Patients were divided into two groups based on the absence (PSH−) or presence (PSH+) of PSH crises. In the PSH+ group, probable and possible patients were pooled together.
The outcome was defined using the Glasgow Outcome Scale (GOS) 11,12 at discharge from the neurorehabilitation subacute unit. The ranking classes were: 1 = death, 2 = VS, 3 = recovery, with severe disabilities, 4 = recovery, with mild disabilities, and 5 = full recovery.
The study was approved by the local public healthcare ethics committee. Regulations regarding privacy and the ethical principles of the Declaration of Helsinki (1964) of the World Medical Association concerning human experimentation were followed.
Statistical analysis
Statistical analyses were performed using R software (version 3.4.1;
Results
Demographic and clinical characteristics are described in Table 1. PSH signs assessed with PSH-AM were present in 19 (13.5%) of the 140 patients (possible in 4 patients and probable in 15 patients). The PSH+ patients were younger than PSH- without sex difference. In the entire ABI cohort, the vast majority of patients were characterized by vascular pathology, followed by traumatic and anoxic etiology. On the other hand, the highest prevalence of PSH signs was detected in patients with anoxic with respect to traumatic or vascular etiology.
Demographic and Clinical Characteristics
PSH, paroxysmal sympathetic hyperactivity; UWS, unresponsive wakefulness syndrome; LOS, length of stay; ICU, intensive care unit; GOS, Glasgow Outcome Scale.
At admission, the vast majority of PSH− patients were in VS/UWS, whereas in the PSH+ group, there was an almost equal proportion of VS/UWS and MCS. During rehabilitation, a small portion of patients died (11%), but none of the inpatients that died during the rehabilitation period had signs of PSH.
As concerns the temporal delay in the patient transfer between first hospitalization and admission to neurorehabilitation subacute unit, there was no difference between PSH groups. On the other hand, PSH+ patients showed a greater LOS in the neurorehabilitation subacute unit with respect to PSH− group.
Uni- and multi-variate logistic regression analyses were used to assess factors associated with PSH. Table 2 highlights that age was the only factor that significantly correlated with the occurrence of PSH in both analyses. This demonstrates that in younger patients with ABI, the likelihood of PSH was greater. With regard to etiology, the anoxic patients in our study were those with an increased risk of PSH instead of vascular and traumatic patients. Finally, neither LOS in ICU nor diagnosis (VS/UWS vs. MCS) were found to be associated with PSH.
Uni- and Multi-Variate Logistic Regression Analyses Assessing Factors Associated with PSH
p < 0.05.
TCE, trichloroethylene; LOS, length of stay; ICU, intensive care unit; DOC, disorder of consciousness; VS/UWS, vegetative state/unresponsive wakefulness syndrome; MCS, minimally conscious state; OR, odds ratio; CI, confidence interval.
Figure 1 shows the clinical outcome at discharge from the neurorehabilitation subacute unit, and highlights that unlike other ABI patients, 19 individuals with PSH were in VS/UWS or MCS (GOS 2) or with a severe disability (GOS 3).
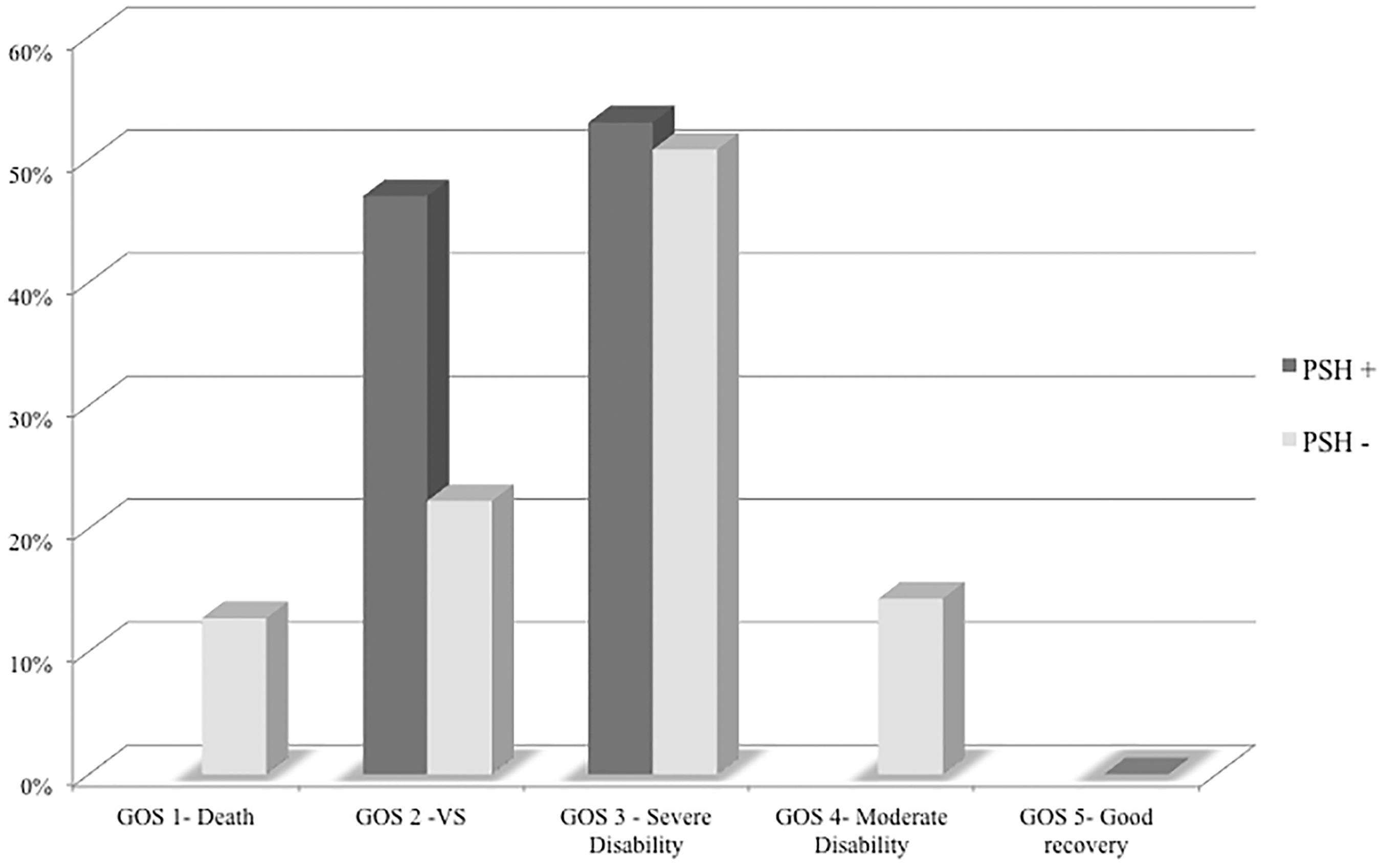
Glasgow Outcome Scale (GOS) in patients with PSH (PSH+) and without PSH (PSH−). We found a worse clinical outcome at discharge from the neurorehabilitation subacute unit since none of the subjects with PSH+ achieved moderate or good recovery categories. PSH, paroxysmal sympathetic hyperactivity; VS, vegetative state.
Table 3 compares etiology, age, and PSH rates with previous studies published in 20087 and 20128 carried out by our group at the S. Anna Institute. In the present study, we revealed a trend toward a reduction of traumatic injury cases (35%) with respect to earlier periods: 52% (2006–2010 period) and 63% (1998–2005 period). As a consequence, increasing of non-traumatic etiology was detected. Interestingly, in patients with traumatic etiology, the proportion of PSH signs followed a similar trend, moving from 32% (1998–2005 period) to 18% (2006–2010 period) and 16% (2010–2014 period), whereas in the non-traumatic population, there was no evidence of a linear trend in PSH prevalence.
Etiology, Age, and PSH Rates Compared with Previous Studies
PSH, paroxysmal sympathetic hyperactivity; TBI, traumatic brain injury.
Discussion
Different PSH rates among ABI patients reported in the literature can be partially explained by the lack of a set of common diagnostic criteria. 4,5,13,14 The results of the Consensus Working Group published in 2014, 6 which led to the publication of PSH-AM, enabled this bias to be overcome. In this study, we utilized PSH-AM and revealed PSH signs in a subsample of the ABI population (13.5%), more often in younger patients with a prevalence of anoxic etiology. With respect to our previous studies, 7,8 the PSH-AM scale improved our diagnostic ability in terms of quantification of the severity of clinical signs and the exclusion of some previous criteria (horripilation, flushing). 7 However, it should be highlighted that using the PSH-AM scale, rather than the criteria described by Dolce and colleagues, 7 did not modify the prevalence of PSH cases in this new study.
Our results on the presence of PSH+ signs in younger ABI patients are perfectly in agreement with previous literature, although the pathophysiological mechanisms underlying the association of PSH signs in younger patients are still unclear. 2,15 –18 For instance, studies performed on a large pediatric cohort of ABI patients 19,20 demonstrated that, despite etiology, diagnosis in younger patients is associated with a higher likelihood of PSH.
As concerns the etiology in the occurrence of PSH, most of the literature has reported a rate ranging from 8% to 33%, above all in TBI patients in ICUs. 1,2,15,21 –24 Generally speaking, there are few studies presenting large cohorts of ABI patients investigated in neurorehabilitation subacute units. 7,8,18 The clinical data reported in these studies could explain why some studies have reported a higher prevalence of PSH+ in neurorehabilitation subacute unit with respect to the ICU (from 18% to 33%). 7,8,18 This might be dependent on the fact that most patients enrolled in neurorehabilitation subacute units are characterized by severe ABI with DOCs.
A review by Parkes and colleagues 4 investigated 349 PSH cases, demonstrating that the vast majority (80%) of patients with PSH resulted from traumatic etiology, followed by anoxic (9.7%) and vascular lesions (5.4%). On the other hand, other researchers have highlighted the impact of anoxic brain injury on the occurrence of PSH signs. Baguley and colleagues 15 described significant preadmission hypoxia in 22 of 35 patients with PSH after TBI. Finally, two additional large-case pediatric case series revealed a high prevalence of PSH after hypoxic (29% and 31%) with respect to TBI (10% and 14%). 19,20
An additional important result of this study is the evaluation of how the prevalence of PSH changed over time. With respect to previous works carried out by our group, a decline in prevalence was revealed above all in the traumatic patients (from 32% to 18%), 7,8 whereas Laxe and colleagues 18 reported a higher prevalence of PSH+ investigating the same clinical population.
We believe that the decrease in PSH rate over time (in the same scenario) was attributed to the early diagnosis during the ICU hospitalization period and attributed to a more effective clinical management during the acute phase, consisting in increased diffusion of decompressive craniectomy together with improved procedures to reduce cerebral edema and to control for intracranial hypertension. In addition, early diagnosis of the PSH in ICU and more effective drug treatments have also helped clinicians to prevent PSH crises, by means of: 1) more gradual weaning of powerful analgesics—mainly opioids 25 ; 2) treatment for pathological adrenergic hyperactivity (i.e., gabapentin, beta-blockers, and clonidine) 26 –29 ; and 3) pathological motor hyperactivity (baclofen). 30,31
The limitations of our monocentric study include the lack of assessment of hypoxia in the early phase of traumatic etiology. As already demonstrated by Baguley and colleagues, 15 in TBI patients, dysautonomia is a clinical syndrome strongly associated with pre-admission hypoxia. In this study, we did not assess whether patients with PSH+ were affected by this specific clinical complication. Second, we did not evaluate as PSH signs change over time in relation to the evolution of consciousness disorders during the rehabilitation period. This type of information could be useful for assessing the influence of environmental or pharmacological factors on the clinical expression of dysautonomic signs. Finally, another issue was the utilization of the GOS for clinical outcomes, which might not be sufficiently sensitive to detect subtle differences in neurological status at the worse end of the outcome scale.
Regarding the clinical outcome, although no patients with PSH died during neurorehabilitation, they remained in a condition of VS/UWS, MCS, or severe disability, consistent with the observation that PSH is associated with poorer outcome. However, the prognosis of ABI patients with PSH+ is currently not well defined. In some studies, 13,15,23,32 the occurrence of PSH was mirrored by a poorer prognosis, whereas others did not find significant differences. 18,21,22,24,33 However, what clearly emerges from this literature is that PSH signs increase the length of hospitalization, as also confirmed by our data (282 days in the PSH+ group compared to 177 days in the PSH− group).
Conclusions
The publication of the PSH-AM by the Consensus Working Group 6 increased the level of sensitivity in the detection of signs of PSH, and, as a consequence, it may improve the clinical management of ABI patients. In fact, we retain that the PSH-AM can be useful in clinical practice if used prospectively to detect the PSH rate, stratify the severity of signs, and test the efficacy of drug treatments and for possible interventions to reduce hyper-reactivity.
Compared with previous studies on the rate of dysautonomia, in our case series, a reduction in PSH was found in patients in SV/UWS and MSC attributed to traumatic ABI. However, the relationship between PSH and etiology in the group of non-TBI is not clear. For this reason, further multi-centric studies including a large sample of heterogeneous ABI patients are needed.
Footnotes
Acknowledgments
In memory of professor Giuliano Dolce who has always paid great attention to the problem of dysautonomic crises in patients in vegetative state and who has taught us a lot in the management of these patients.
The study was carried out at the S. Anna–RAN Institute with support from the institute; authors are all employees of the institute.
Author Disclosure Statement
No competing financial interests exist.