
Abstract
Initial studies examining patient demographics and outcomes in traumatic brain injury (TBI) suggest a trend toward increasing patient age and decreasing rehabilitation length of stay, but such studies have not been repeated since the passage of healthcare reform legislation, most notably the Affordable Care Act. This study utilized the Uniform Data System for Medical Rehabilitation® (UDSMR) for patients admitted to medical rehabilitation facilities after sustaining a TBI from January 1, 2002 through December 31, 2016. Trends for demographic and medical data were evaluated. In total, 233,843 patients from 1290 facilities were included; mean patient age increased from 54.1 to 64.8 years, rehabilitation length of stay decreased from 19 to 14.5 days, and mean admission Functional Independence Measure® (FIM) decreased from 56.9 to 54.5. Sex and racial distribution remained relatively stable across all years, as did discharge FIM. There was an increase in Medicare patients from 40.7% to 62.1%, a concomitant decrease in commercially insured patients from 29.2% to 15.4%, and a decrease in unreimbursed patients from 7.2% to 2.6% over the course of the study. Based on these data, medical rehabilitation facilities appear to be admitting an older TBI patient population that is less functional on admission and discharging them after shorter rehabilitation lengths of stay. Similar discharge functional status, despite shorter rehabilitation lengths of stay and an older population may suggest a change in the typical mechanism of injury. Many current TBI patients would fail to meet inclusion criteria for post-acute clinical trials in TBI because of their age, and treatments based on such trials may not be generalizable, which has significant implications on both research and clinical care realms within brain injury rehabilitation.
Introduction
Studies have sought to evaluate trends in traumatic brain injury (TBI) over time, investigating changes in patient age, rehabilitation length of stay, and functional status at admission and discharge. A study of patients admitted to medical rehabilitation facilities after sustaining a brain injury from 2000 to 2007 reported an increase in age from 47.1 to 58.6 years over the course of the study, with the greatest rate of change during a period from 2001 to 2004. 1 At the end of the study, 35.2% of the patients admitted were over the age of 75, compared with 18.4% at the start of the study; patients younger than 45 years of age decreased from 51% to 30% of the sample. This apparent increase in mean age for TBI patients admitted to rehabilitation facilities was corroborated by a study of Pennsylvania residents from 1992 to 2009, which found that incidence of elderly TBI approximately doubled over the study period, with the greatest increase in incidence for individuals between the ages of 83 and 90 years. 2 With this increase in elderly patients sustaining TBIs comes a concurrent increase in medical complexity and comorbidities, which may further complicate their rehabilitation course and impact subsequent outcomes. Further, there is an association between sustaining a moderate-to-severe TBI at the age of 55 or older, or mild TBI at the age of 65 or older, and the risk of developing dementia, which could have a dramatic impact on the long-term sequelae for aged TBI survivors. 4 Similarly, patients over the age of 55 who sustain a TBI have an estimated 44% increased risk of developing Parkinson's disease in the following 5–7 years. 5
Researchers working to characterize these trends have attempted to provide explanations for the shift in patient age over time. Legislative efforts have reduced motor vehicle fatalities, and as a result the number of generally younger patients sustaining severe brain injuries has decreased. 6 As life expectancy and mobility in the elderly increased compared to previous decades, the prevalence of TBIs in elderly populations similarly increased. 7,8 In another study, the rate of increase in emergency department visits for TBI in elderly patients more than tripled that of a younger cohort, with an age-controlled rate of hospitalization 4 times higher than that of younger patients. 9 Potential complications after a TBI in an elderly patient are compounded when considering the prevalence of systemic anticoagulation in elderly populations, which may contribute to worsening outcomes after a brain injury attributed to traumatic intraparenchymal hemorrhage, subdural hematoma, or subarachnoid hemorrhage. 10
The Uniform Data System for Medical Rehabilitation® (UDSMR) maintains a large database for medical rehabilitation outcomes, with >70% of national medical rehabilitation facilities reporting outcomes to the UDSMR. 1 The database contains demographic, medical, and rehabilitation outcomes data for tens of thousands of patients since its inception. As such, the UDSMR represents a valuable source for patient characteristics and outcomes data within the medical rehabilitation setting for a wide array of impairments and rehabilitation diagnoses. 11,12 In contrast, the Traumatic Brain Injury Model Systems (TBIMS) represents a smaller, but important, subset of predominantly academic, highly specialized rehabilitation centers, but contains significantly more injury-specific data. Despite the greater amount of injury-specific data, such as initial Glasgow Coma Scale (GCS) for brain injury, the smaller subset of facilities when compared to the UDSMR raises the potential for selection bias and may be less representative of the national sample of brain injury patients admitted to medical rehabilitation facilities. Building upon earlier work by Granger and colleagues, we sought to characterize trends in demographics, particularly age, as well as medical characteristics of patients admitted to medical rehabilitation facilities after sustaining a TBI in the United States from 2002 to 2016 utilizing the UDSMR. 1
Methods
Definition of terms
Payer source
Payer source identifies the person or party responsible for financing the patient's rehabilitation stay, whether Medicare, Medicaid, private insurance, Workers' Compensation, unreimbursed, or “other.”
Living situation before injury
Living situation before injury indicates the setting in which the patient lived before sustaining their TBI, including home, community-based retirement facility (board and care), transitional living, intermediate care (nursing home), skilled nursing facility (SNF), acute unit of own facility, acute unit of another facility, chronic hospital (long-term acute care hospital), rehabilitation facility, alternate level of care (ALC) unit, subacute setting, assisted living residence, and other.
Time post-injury (onset days)
Time post-injury indicates the number of days which passed from the patient's TBI and their admission to a medical rehabilitation facility.
Functional Independence Measure®
Functional Independence Measure (FIM) is a measure of a patient's functional status, containing 18 items over six domains (self-care, sphincter control, mobility, locomotion, communication, and social cognition). Each item is rated from 1 (complete dependence) to 7 (complete independence), with a higher total score indicating greater functional independence (total scores range from 18 to 126).
Functional Independence Measure gain
FIM gain indicates the numerical difference between discharge FIM and admission FIM. It is used to measure the amount of functional gain achieved during an individual's rehabilitation stay.
Length of stay efficiency
Length of stay (LOS) efficiency represents the FIM gain divided by the total rehabilitation length of stay, a calculated value of total FIM gain per day of rehabilitation.
Rate of readmission to acute care hospital
Rate of readmission to acute care hospital represents the percentage of patients who were unexpectedly readmitted to an acute care hospital during their rehabilitation stay.
Sample population selection
Patients with traumatic brain dysfunction admitted to an inpatient rehabilitation facility between January 1, 2002 through December 31, 2016 with a Rehabilitation Impairment Code (RIC) of 2.21 (traumatic, open) and 2.22 (traumatic, closed) were obtained from the UDSMR data repository. 13 Patients <18 years of age, those with non-traumatic brain dysfunction (RIC code 2.1) and those with other brain dysfunction/not specified (RIC code 2.9) were excluded.
Demographics
Demographics data were categorized by year, including age, sex, living situation, race, primary payer source, and living situation before injury.
Medical characteristics
Medical data were categorized by year, including time post-injury (onset days) and admission FIM.
Discharge metrics
Discharge metrics were categorized by year, including discharge FIM, FIM gain, LOS efficiency, rate of readmission to acute care hospital from inpatient rehabilitation, and percentage discharged to the community setting after a rehabilitation stay.
Trends by type of injury
The above variables were further analyzed by type of traumatic injury (open TBI and closed TBI). Tables containing mean age, LOS, onset days, admission FIM, percentage living at home pre-morbidly, discharge FIM, LOS efficiency, rate of readmission to acute care hospital, and percentage discharged to the community setting were constructed, in addition to median age on admission by year.
Age stratification
Using age categories of <55 years of age, 55–64, and age 65 and older, mean admission and discharge FIM, mean LOS, mean LOS efficiency, mean rate of readmission to acute care hospital, and mean percentage of patients discharged to the community were calculated by year for all TBIs, regardless of type, for additional subgroup analysis.
Statistical analysis
To evaluate for statistically significant changes in outcomes data in the years 2002 and 2016, two-tailed t-tests were constructed comparing these data. Differences were considered statistically significant for p ≤ 0.05.
For data that were stratified by age (those <55 years of age, 55–64, and those age 65 and older), Pearson chi-squared testing was used to test the equality of proportions by age groups across years, whereas linear regressions were constructed for admission and discharge FIM, LOS, and LOS efficiency. A logistic regression was utilized for analysis of the rate of transfer to acute facilities within 30 days of rehabilitation admission and for the rate of discharge to the community setting for the same age groups.
Institutional review board exempt status
Because this study utilized a pre-existing, de-identified database review, institutional review board approval for this research project was not required.
Results
The UDSMR contained data for 233,843 patients discharged for TBIs (both open and closed TBIs) from 1290 medical rehabilitation facilities over the study period. There was an increase in the total number of patients discharged per year (Table 1). Demographic factors, including race, sex, marriage status, and pre-hospital living situation, remained largely unchanged (Supplementary Table S1). Mean age increased from 54.1 (standard deviation [SD], 22.9) to 64.8 (20.5) years, and median age increased from 54 (interquartile range [IQR], 34–76) to 70 (53–82) years over the course of the study (Fig. 1). There was a decrease in both mean onset days (22.5 [SD, 34.2] to 15.0 [24.9] days) and LOS (19.0 [16.7] to 14.5 [11.4] days) from 2002 to 2016 (Fig. 2). There was a slight decrease in admission FIM (56.9 [23.8] to 54.5 [19.5]) whereas discharge FIM in 2002 and 2016 was unchanged (86.6 [26.4, 23.9] in both years), albeit with a nadir of 82.7 [25.4, 25.0] in 2008–2009 (Fig. 3). There was an increase in FIM gain (29.7 [20.7] to 32.1 [18.3]) and LOS efficiency (2.0 [2.1] to 2.7 [2.0]) over the course of the study. There was an increase in the rate of readmission to acute hospitals within 30 days of rehabilitation admission (8.9% [28.5] to 10.2% [30.3]), whereas the percentage discharged to the community in 2002 and 2016 was similar (75.0% [43.3] and 75.2% [43.2]), with a nadir of 70.5% in 2009. The proportion of Medicare patients increased over the course of the study, and there was a concomitant decrease in the proportion of commercially insured patients (Supplementary Table S1). t-tests comparing 2016 data against 2002 data determined that changes in mean age, LOS, onset days, admission FIM, FIM gain, LOS efficiency, and rate of readmission were statistically significant (p < 0.001), whereas changes in discharge FIM and percentage discharged to the community were not statistically significant (p = 0.97 and 0.65, respectively). Changes in demographics, including sex, proportion of married patients, those living alone, those living at home pre-morbidly, and payer source, were statistically significant (p < 0.05), whereas the change in race (percentage of white patients) was not statistically significant (p = 0.053).
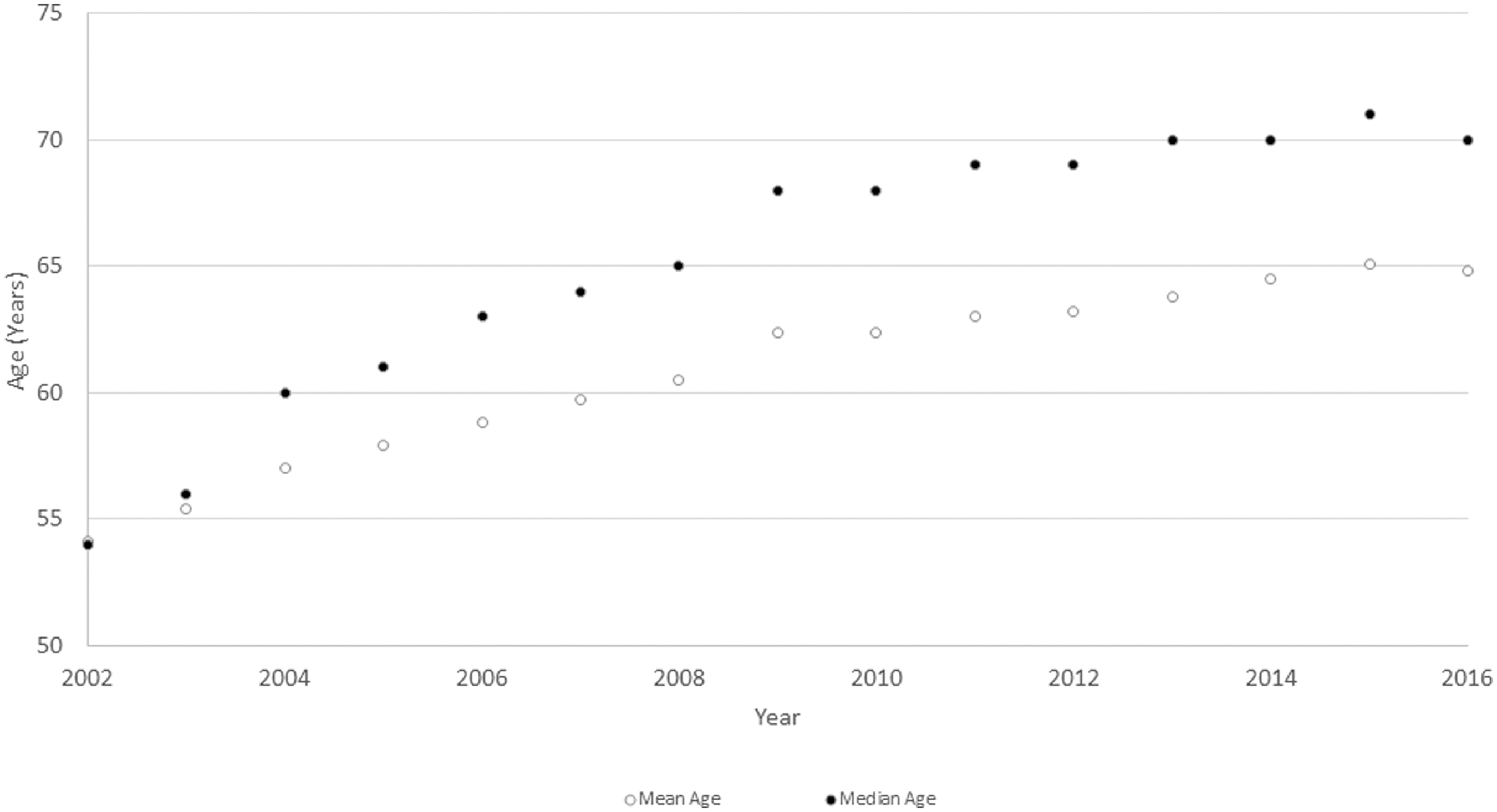
Mean and median age for all patients admitted to rehabilitation facilities included in the UDSMR. UDSMR, Uniform Data System for Medical Rehabilitation.
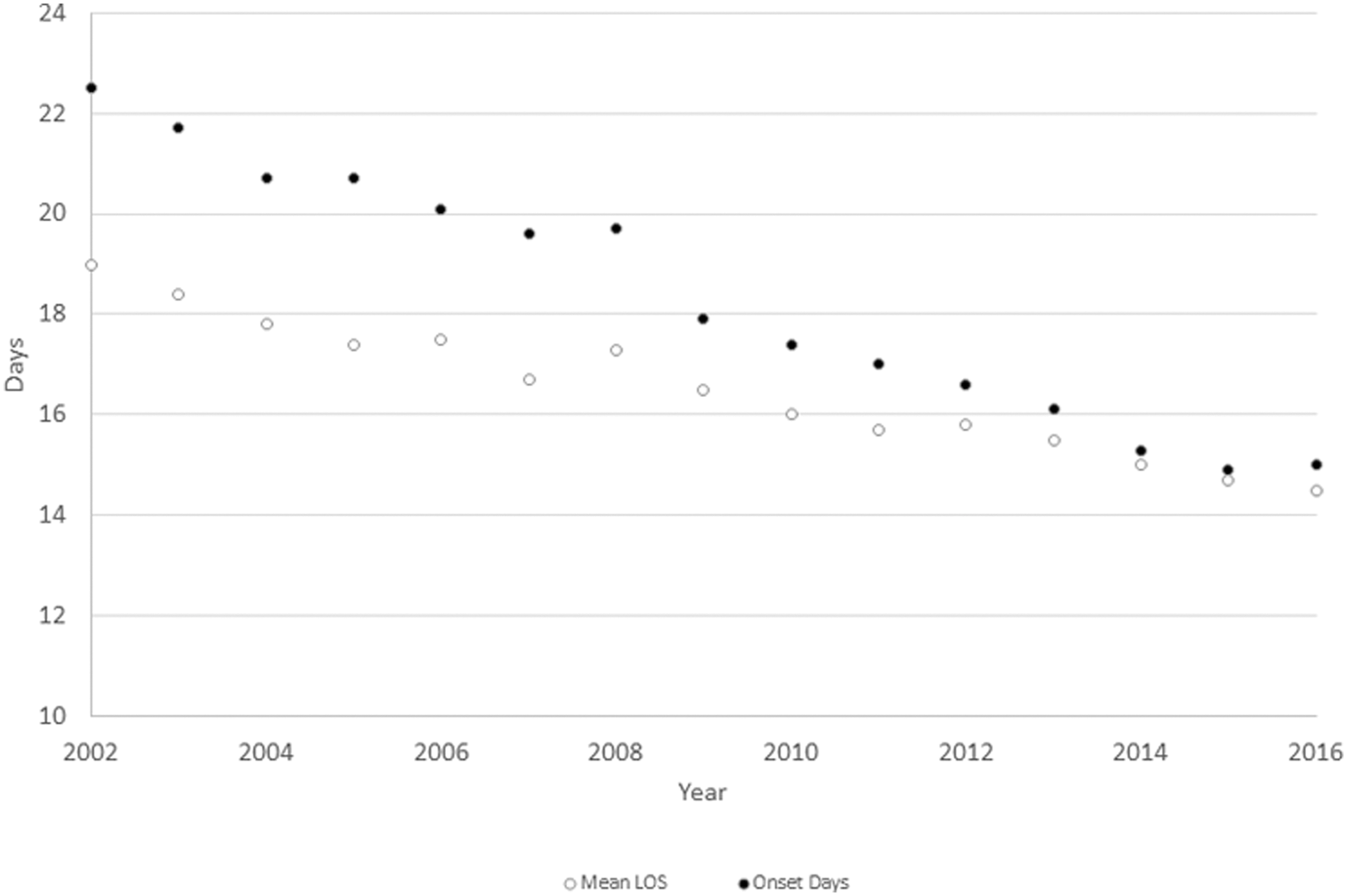
Mean length of stay and onset days for TBI inpatient rehabilitation patients from 2002 to 2016. LOS, length of stay; TBI, traumatic brain injury.
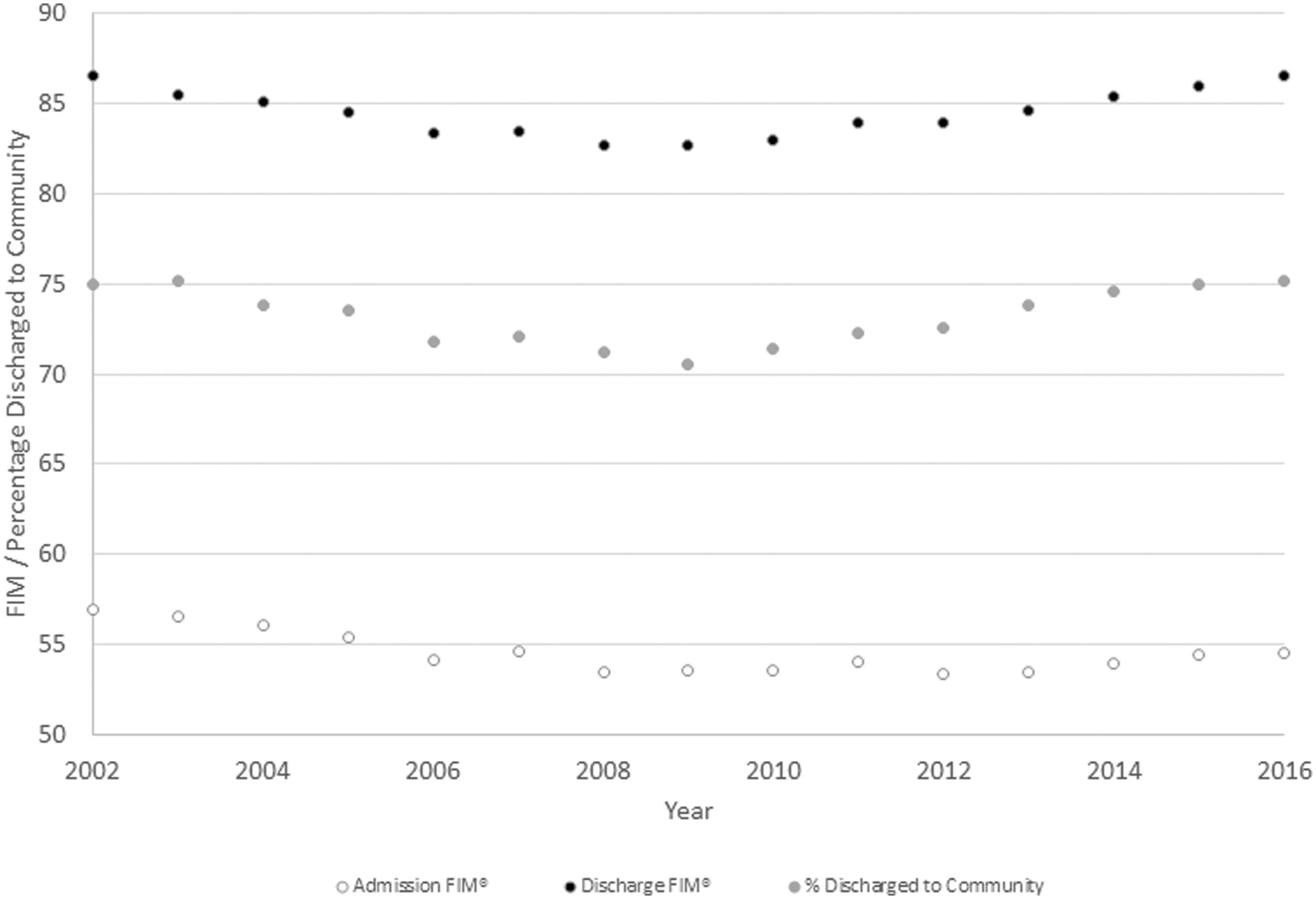
Admission and discharge FIM and percentage discharged to the community for all TBI inpatient rehabilitation patients from 2002 to 2016. FIM, Functional Independence Measure; TBI, traumatic brain injury.
Patient Medical Characteristics on Admission and Discharge Metrics for All Patients Admitted with Impairment Code 2.21 (Traumatic, Open) and 2.22 (Traumatic, Closed) Brain Dysfunction
Std Dev, standard deviation; LOS, length of stay; FIM, Functional Independence Measure.
Open TBIs totaled 10,034 discharges over the study period, representing 4.3% of all TBIs in the sample (Supplementary Table S2). Mean and median age remained relatively stable (44.8 [SD, 22.1] to 45.3 [22.1] years and 40 [IQR, 26–62] to 39 [25–62] years, respectively); mean LOS decreased (19.6 [15.9] to 17.0 [14.4] days), as did onset days (28.1 [37.9] to 24.1 [31.2] days). Admission and discharge FIM increased, as did FIM gain and LOS efficiency. Changes in mean LOS, onset days, FIM gain, and LOS were statistically significant, whereas changes in mean age, admission and discharge FIM, and percentage discharged to the community were not statistically significant. There was a decrease in the percentage of white patients admitted, and fewer patients were living alone before their injury (Supplementary Table S3). The proportion of Medicaid patients increased over the course of the study. Changes in percentage of those living alone, those living at home pre-morbidly, the proportion of white patients, and payer source were statistically significant, whereas the change in percentage of married patients was not.
Closed TBIs composed 95.7% of all patients in the sample, at 223,809 discharges in total (Supplementary Table S4). Mean and median age both increased (54.7 [SD, 22.9] to 64.5 [20.0] years and 55 [IQR, 34–76] to 71 [54–82] years, respectively), whereas LOS and onset days decreased (18.9 [16.8] to 14.4 [11.2] days and 22.1 [33.8] to 14.7 [24.5] days, respectively). Admission FIM decreased whereas discharge FIM remained relatively stable, with a slight nadir in 2008. FIM gain and LOS efficiency increased. There was an increase in the rate of readmission to acute hospitals, whereas the percentage discharged to the community remained largely unchanged.
Changes in mean age, LOS, onset days, admission FIM, FIM gain, LOS efficiency, and rate of transfer to acute facility were statistically significant, whereas changes in discharge FIM and percentage discharged to the community were not. Changes in demographics, including percentage married, those living alone before their injury, and those living at home pre-morbidly, were statistically significant (Supplementary Table S5), whereas the change in proportion of white patients was not. There was an increase in the proportion of patients insured by Medicare over the course of the study; this change, as well as concomitant decreases in Medicaid, private insurance, and unreimbursed care, was statistically significant.
Patients over the age of 65 years made up the majority of all patients discharged, at 53.1%, and their proportion increased over the course of the study, from 39.8% to 60.3% (Supplementary Table S6). Discharge FIM was lowest for those >65 years old (ranging from 78.6 [SD, 24.1] to 83.8 [23.2] compared to 87.2 [26.6] to 91.2 [24.6] for those younger than 55 and 85.4 [24.1] to 89.7 [23.3] for those 55 to 64), whereas admission FIM was similar for all age groups. Elderly patients tended to be admitted to rehabilitation hospitals for shorter periods of time, with a lower LOS efficiency, and a generally higher rate of readmission to acute hospitals. Those older than the age of 65 years were less frequently discharged to the community setting after their rehabilitation stay. Differences between age groups from 2002 to 2016 were statistically significant (p < 0.05) for mean age, admission FIM, discharge FIM, LOS, LOS efficiency, and discharge to the community setting. Differences in the rate of transfer to acute facilities within 30 days of rehabilitation admission for all age groups between 2002 and 2016 were not statistically significant.
Discussion
This study sought to characterize trends in the TBI patient population admitted to medical rehabilitation facilities, with a particular focus on demographics and medical characteristics. The data for all included patients, collected from 2002 through 2016, indicate an overall increase in mean and median patient age, decreasing rehabilitation lengths of stay, with relatively stable FIM scores at rehabilitation discharge. Patient demographics, including race, sex, and pre-hospital living situation remained relatively stable over the study period. The trends in the closed TBI cohort, comprising 223,809 of the 233,843 patients in the sample (95.7% of the total sample) are predominantly driving the changes noted in the TBI population at large. In comparing the open and closed TBI groups, the closed TBI group was older, was admitted closer to their initial injury, and stayed for a shorter period of time.
Closed TBI patients were more likely to be married, were more often white, and were more often insured by Medicare. Interestingly, discharge FIM was similar for both closed and open TBIs. Patients with a closed TBI were less likely to be discharged to the community setting when compared to those with open TBIs and had a slightly lower rate of readmission to acute care hospitals. The open TBI group was largely stable over the course of the study, with <800 admissions to rehabilitation facilities per year, and the mean age remained relatively stable over time. The decrease in onset days was less drastic for the open TBI cohort (28.1–24.1 days), and functional status on both admission and discharge remained stable, within 2–3 FIM points, from the beginning to conclusion of this study. In contrast, the closed TBI cohort increased in size (from 11,002 admissions to 17,512 admissions annually), and, over the course of this study, this group had larger changes in medical characteristics and discharge metrics. There was a significant increase in mean age from 2002 to 2016, and onset days decreased by more than 1 week on average. As admission FIM decreased and discharge FIM remained stable, the LOS efficiency increased, driven largely by a shorter LOS (from 18.9 to 14.4 days).
The findings of this study have significant implications for the patient care, research, and healthcare policy arenas, given that they demonstrate that trends identified in earlier data sets within the TBI population are continuing: These patients are becoming increasingly elderly as time progresses. 1 This trend is not isolated to rehabilitation settings, because it has also been documented in inpatient acute hospital settings and in emergency departments, which presents its own unique challenges for providers in those settings. 2,3 Our study demonstrated that as the mean age of patients admitted to medical facilities after a TBI increased, there was a concomitant increase in patients insured under Medicare compared to private insurers. An increasing number of Medicare patients accruing rehabilitation costs after a TBI could further increase national Medicare expenditures and could increase the overall taxpayer burden. With the financial cost per TBI exceeding $80,000 per patient in many instances, the expenditures for both acute care and long-term care, including home nursing, supervision, follow-up medical appointments, and outpatient therapy appointments, could cost hundreds of millions of dollars in sum. 14 Nonetheless, this study supports past literature, in that older patients can make significant functional improvements after a TBI when given the proper rehabilitative environments. 15
The trend toward an aged medical rehabilitation population after a TBI may be a result of several factors working in synergy. These numbers may, in part, be reflective of an increasingly aged U.S. population, but a review of 2010 Census data demonstrates an increase in those age 65 and older from 12.4% to 13.0% of the total U.S. population (an increase from 34,991,753 to 40,267,984). 16 As such, this increase in proportion alone is unlikely to be the only source of change in our study. Given that older patients are more mobile and more independent when compared to previous generations, there is a risk for more falls and associated injuries, and thus an increase in the elderly brain injury population admitted to medical rehabilitation facilities, consistent with earlier studies. 7,8,17
Highway safety laws may disproportionately reduce the number of young individuals sustaining brain injuries when compared to elderly patients. 17,18 One study has suggested that ridesharing applications such as Uber® or Lyft® may decrease alcohol-related traffic incidents by as much as 61.8% in some cities; such incidents preferentially affect younger populations. 19 Last, given that younger patients often have more-severe mechanisms of injury, there may be a disproportionate number of younger patients who succumb to their injuries in intensive care units, including those for whom care is withdrawn in the early stages after injury, as suggested by Turgeon and colleagues. 20 With advances in brain injury rehabilitation, there may be a case for advocating for continued aggressive medical and surgical management in the acute care setting after a severe TBI, given that these patients demonstrate the potential for ongoing functional gains years after their initial injury. 21
As a whole, the marked decline in average LOS is, in part, attributed to a shift from an overall younger patient population, with generally longer rehabilitation LOSs, to an older patient population with generally shorter LOS, for which there may be several reasons, addressed below. The mean LOS decreased for all ages, by more than 4 days for those younger than 55, by almost 4 days for those 55–64, and by more than 2 days for those older than 65 years. The overall decrease in LOS is likely driven, in part, by changes in inpatient rehabilitation facility (IRF) regulations and reimbursement structures, which reward efficiency in the delivery of medical care. Despite shorter LOSs, there was an increase in mean discharge FIM and an improvement in LOS efficiency across all age groups, suggesting that multi-disciplinary medical rehabilitation teams are better able to achieve desired outcomes in an ever-decreasing amount of time. This is noteworthy given that older patients tend to have greater numbers of comorbidities and medical complexity, which, without skilled management, could hinder progress during inpatient rehabilitation. 3 Alternatively, rehabilitation facilities may be selecting patients with different mechanisms of injury or fewer comorbidities, facilitating faster recovery.
The shift toward an overall older patient population may also be suggestive of a change in the predominant mechanism of injury resulting in brain dysfunction. As onset days decrease, it could be expected that the risk of transfer to acute hospitals would increase, given that many complications occur in the early post-operative course. 22 Yet, a small increase in the acute hospital transfer rate was noted for patients younger than 55 and relative stability or declines in the rate for elderly patients. It is possible that this is reflective of a change in the predominant mechanism of injury, namely shifting to cerebral contusions from falls, and that these patients undergo fewer operative interventions and have less complications as a result.
For medical rehabilitation facilities, an increase in the proportion of elderly TBI patients poses many challenges. Based on these data, elderly patients are more likely to be discharged to secondary rehabilitation facilities, such as SNFs, by 6–9%. This places an increased burden on case managers who are often responsible for securing disposition plans for such patients. Similarly, discharges to secondary facilities increase the number of provider-to-provider handoffs by both nursing and medical staffs and can increase the risk of miscommunication or lack of adequate documentation. Issues may arise regarding medication reconciliation at discharge to SNFs and documentation may be incomplete, both of which can result in delays of care, foster negative perceptions regarding SNF staff competency, and increase the risk of rehospitalization. 23,24 The highest likelihood of readmission to an acute care hospital was consistently in those older than 65 and thus pose challenges to rehabilitation facility administrators and admissions departments as they work to balance the hospital's readmission risk profile. Given that reimbursement strategies further target unexpected readmissions, this trend may become increasingly burdensome for medical rehabilitation facilities if not aggressively targeted by readmission reduction strategies or legislative adjustments.
An aging TBI rehabilitation patient population has additional significant implications on both the clinical care and research realms. A search of trials enrolling brain injury patients listed on
Similarly, current research and treatment principles founded upon clinical trials which excluded older brain injury patients may not be generalizable to the majority of brain injury patients admitted to medical rehabilitation facilities today. Many key studies in the field of brain injury rehabilitation utilized lower maximum ages for clinical trials, such as 55 or 65 years of age. 29,30 If such studies are not generalizable, elderly patients may be exposed to ineffective treatments or potentially unexpected adverse health outcomes. As a result, some studies have begun enrolling increasingly elderly patients, in some cases up to and beyond the age of 75 years. 31 There is a clinical imperative that research studying the management of TBI in the elderly continue to expand and evolve, in order to determine best practices, avoid adverse outcomes, and maximize functional gains within the TBI elderly.
Strengths of this study include the large and diverse sample size (i.e., 233,843 patients from 1290 medical rehabilitation facilities), and an observational period that spans nearly two decades. The UDSMR may be more generalizable to patient populations at community-based rehabilitation centers when compared to data collected at larger academic rehabilitation facilities participating in the TBIMS. This study utilized common outcome metrics, such as the FIM, discharge to the community setting and the rate of readmission to acute care hospitals, which are all standardized, validated, and consistently used outcomes measures at medical rehabilitation facilities in the United States.
Limitations of this study mostly pertain to the lack of injury-specific details, such as the specific medical diagnosis (diffuse axonal injury, cerebral contusion, traumatic intracranial hemorrhage, or focal traumatic brain injury not otherwise specified), the presence of any abnormalities on computerized tomography imaging, initial Glasgow Coma Scale (GCS), Coma Recovery Scale, Glasgow Outcomes Scale, etiology of injury (fall, automobile accident, blunt trauma/hit to the head, sport-related injury, or workplace accident), and severity of injury. Additionally, such database studies are limited by possible errors in patient assessment, coding, and documentation by participating facilities. Coding an injury on admission is dependent on the interpretation of the admitting physician. In spite of these limitations, this study provides a valuable contribution to the literature, in that it confirms that previously identified trends in patient age have continued, brings to light concerns regarding an aging population, enrollment in clinical trials, and the generalizability of such findings; and highlights the challenges that an aging TBI population may have for IRF administrators.
Future studies should further examine the effect of medical comorbidities on outcomes of patients with TBIs, given that this information could lend further insight into the severity of the mechanism of injury as well as the impact of medical complexity on functional improvement and post-acute care outcomes. Additionally, future research comparing outcomes of patients with other non-TBIs is warranted given the marked changes observed over time in age, function at admission, and LOS in inpatient rehabilitation in the current study with the TBI population.
Conclusions
This study, an extension of earlier work by Granger and colleagues, indicates that patients admitted to medical rehabilitation facilities after a TBI are significantly older, less functional on admission, staying at rehabilitation facilities for shorter periods of time, but with similar functional status at the time of discharge. 1 Such trends may be driven, in part, by changes in rehabilitation facility reimbursement structures, improved multi-disciplinary rehabilitation efficiency, selection bias by admitting facilities, a change in the predominant mechanism of injury, or other unidentified factors. Future studies are needed to evaluate the role to which such factors are influencing the trends observed.
Footnotes
Acknowledgments
Data from this article were presented as a poster presentation for the 2018 American Academy of Physical Medicine & Rehabilitation Annual Assembly in Orlando, Florida.
Author Disclosure Statement
Dr. Zafonte and Giacino's contributions were partially supported by awards from the National Institute on Disability, Independent Living and Rehabilitation Research (NIDILRR), Administration for Community Living (Award Nos. 90DP0039, Spaulding-Harvard TBI Model System; 90DP0036). The contents of this article do not necessarily represent the policy of the U.S. Department of Health and Human Services, and endorsement by the federal government should not be assumed. Additionally, Dr. Zafonte and Dr. Giacino are involved with the TBI Model Systems, grant number TBIMS-90DPTB0011-01-00; as well as a clinical trial involving the use of huperzine in TBI, grant number W81XWH-11-2-0210.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.