
Abstract
Hypotension worsens outcome after all severities of traumatic brain injury (TBI), with loss of cerebral autoregulation being a potential contributor. Previously, we demonstrated that intravenous injection of a high capacity catalytic antioxidant, poly(ethylene)glycol conjugated hydrophilic carbon clusters (PEG-HCCs) rapidly restored cerebral perfusion and acutely restored brain oxidative balance in a TBI model complicated by hemorrhagic hypotension without evidence of toxicity. Here, we tested whether these acute effects translated into behavioral and structural benefit. TBI was generated by a cortical contusion impactor in 38 Long Evans rats, followed by blood withdrawal to a target mean arterial pressure of 40 mm Hg. PEG-HCC (2 mg/kg) or diluent was injected intravenously 80 min later at the onset of blood resuscitation followed by another injection 2 h later (doses determined in prior studies). Performance on beam walking (performed on days 1–5) and Morris water maze (MWM) (performed on days 11–15) was tested, and lesion size was determined at the termination. PEG-HCC treatment nearly completely prevented motor dysfunction (p < 0.001 vs. diluent), improved MWM performance (p < 0.001; treatment vs. time interaction) and reduced lesion size by 61% (p = 0.054). Here we show that treatment with PEG-HCCs at a clinically realistic time point (onset of resuscitation) prevented a major portion of the neurological dysfunction induced in this TBI model, and that PEG-HCCs are candidates for additional study as a potential therapeutic agent.
Introduction
Traumatic brain injury (TBI) is a leading cause of death and disability in the United States. Annually, an estimated 1,700,000 individuals sustain some form of TBI, resulting in 52,000 deaths and 275,000 hospitalizations. 1,2 Hypotension, often caused by hemorrhage from concomitant injury, worsens outcomes in TBI. 3
Oxidative stress is a prominent feature of TBI, especially when complicated by secondary trauma such as hemorrhagic hypotension. We previously demonstrated a triphasic increase in superoxide (SO) anion concentration, first immediately after the injury, second following hemorrhagic hypotension, and third accompanying resuscitation with blood infusion. 4 Other work suggests that loss of cerebral autoregulation that is found following even mild TBI is mediated at least in part by reactive oxygen species (ROS). 5 –8 Particularly in hypotensive conditions, a decrease in cerebral blood flow worsens the outcome after injury. 5 However, there is no conclusive evidence that antioxidant therapies improve outcome following TBI and hypotension in patients. 8 –10
We identified several features of current antioxidants that limit their likely effectiveness when administered after an injury, including low capacity, reliance on either regeneration or downstream enzymes that may be depleted in the injured tissue, and narrow range of radicals quenched that cannot address the cascade of radicals that occur after an injury. We developed a new class of highly modified carbon nanomaterial, poly(ethylene)glycol conjugated hydrophilic carbon clusters (PEG-HCCs), and determined that they were high-capacity antioxidants in acellular systems and in cultures of brain endothelial cells and primary neurons. 5,11,12 PEG-HCCs are non-toxic carbon nanoparticles that are soluble in biological media and contain a blood half-life of 2–3 h after intravenous injection. 13 Histological analysis did not suggest any toxicity in normal mice and accumulation in Kupffer (macrophage) cells of the liver, suggesting carbonaceous uptake as a major form of metabolism. 13
PEG-HCCs exhibited SO anion quenching by a SO dismutase (SOD)-mimetic mechanism of high capacity. 14 Molecular oxygen and hydrogen peroxide were identified as products of this reaction. PEG-HCCs are capable of detoxifying many ROS, 5 both SO and hydroxyl radical, while remaining unreactive toward nitric oxide (NO), a potent vasodilator. 14 Unlike large unmodified nanotubes, PEG-HCCs have shown no toxicity to a variety of cell types. 5,11 –13,15–17 Further, the rapid onset of action of PEG-HCCs is faster than in PEG-SOD and the small molecule antioxidant, phenyl-a-tert-butyl nitrone (PBN) in protecting endothelial cells from lethal oxidative stress. 5
Our prior work showed that PEG-HCCs were able to completely restore cerebral blood flow that occurred in our model of cortical contusion injury. This model transformed from a non-cavitary lesion into a cavitary lesion by 50 min of hemorrhagic shock followed by resuscitation followed by two phases of resuscitation, first utilizing saline, mimicking first responder, and then definitive resuscitation using reinfusion of blood. 6,13 This restoration of blood flow occurred even though treatment was delayed to 80 min following injury, mimicking the delays encountered in a realistic clinical scenario. Oxidative balance, specifically an increase in NO expression and a decrease of SO levels in brain endothelial cells, accompanied this restoration of autoregulation. 5
We designed the present study to test the ability of PEG-HCC treatment, administered at the delayed time of “definitive resuscitation” in a TBI model combined with hypotension and resuscitation, to improve functional outcome and brain structure. Rats survived following the injury, and behavior variables including beam balancing duration, beam walking duration, and Morris water maze latency were examined as was brain lesion size.
Methods
Synthesis of and characterization of PEG-HCCs
The PEG-HCCs were prepared using methods described in the literature. 8,15 As the study progressed, the need for thorough characterization of each batch was recognized as variation was observed, mostly related to the degree of PEGylation. We have previously reported 13 the characterization details, including infrared spectroscopy (FTIR), Raman spectroscopy, X-ray photoelectron spectroscopy (XPS), atomic force microscopy (AFM), thermogravimetric analysis (TGA), UV/vis spectroscopy, dynamic light scattering (DLS), and zeta potential measurements, but were not employing the complete set for each batch as is now done. Trace metal contaminants as determined by inductively coupled plasma mass spectrometry (ICP-MS) were not present. We estimated the number of PEG chains per HCC particle to be 50 so that the PEG made up ∼80% of the entire mass of the particle including both the particle core and the covalently bound PEG. 14
Treatment groups
In this study, a total of 38 Long Evans rats, weighing 300–350 g, were used. The TBI model used was a cortical impact injury (3 m/sec, 2.5 mm deformation) followed by 50 min of hemorrhagic hypotension. The rats were randomly assigned to receive either PEG-HCC (2 mg/kg, n = 21) or saline as placebo (n = 17). The assigned study drug was given intravenously at the beginning of resuscitation and again 2 h after the first dose. We chose the treatment dose, 2 mg/kg, as an extrapolation for dilution using the average rat blood volume based on the effective concentration in vitro that is protective against a variety of toxins, 2–8 mg/L. 12,18 The second administration of particles was given because of the 2–3 h half-life of PEG-HCCs in the blood. 5 It is important to note that these are the identical doses used in our prior work that demonstrated sustained restoration of cerebral blood flow and restoration of oxidative balance. 5
Anesthesia
General anesthesia was induced using 5% isoflurane in 100% oxygen, by placing the rats in a vented anesthesia chamber for ∼3–5 min. After anesthesia induction, the animals were intubated with a 14 gauge angiocatheter and mechanically ventilated using a volume-controlled ventilator. A surgical plane of anesthesia was maintained throughout the impact injury and period of hypotension with 2% isoflurane.
Surgical preparation
Using aseptic techniques, intravascular catheters were placed in the tail artery and femoral vein. The tail artery was dissected through a 2–4 mm incision in the proximal segment of the tail and cannulated using a 22 gauge Angiocath™ Teflon catheter to monitor blood pressure. Through a 5–8 mm incision in the left groin, the femoral vein was dissected free and cannulated using a 22 gauge Angiocath Teflon catheter to allow for the controlled hemorrhagic shock and resuscitation using Lactated Ringer's solution or the shed blood. The catheters were secured to the skin with nylon sutures. After catheterization, the animals were mounted in a stereotactic frame in the prone position with the head secured by ear bars and an incisor bar. Body temperature was monitored and kept between 36 and 37°C with a heating pad controlled by a rectal probe. Arterial blood gas values, including pH, pCO2, and pO2 were obtained on blood drawn from the tail artery catheter with an IRMA TruPoint blood gas analysis system.
Craniectomy and controlled cortical impact injury
The scalp was shaved and cleaned using an iodine-based solution. The surgical field was draped with sterile linens. A medial sagittal skin incision was performed and the scalp (including the periosteum) and the temporalis muscle were reflected. To expose the brain for the impact injury, a 10 mm diameter craniectomy was performed over the right parietal cortex between bregma and lambda using a dental drill. Care was taken to not injure the dural surface. A small amount of saline solution was directed at the site of drilling to prevent thermal injury to the brain tissue. With the impactor rod locked in the extended position, the impactor tip was centered in the craniectomy site perpendicular to the exposed surface of the brain at an angle of ∼45 degrees to the vertical, and then the tip was lowered until it just touched the dural surface. The impactor rod was then retracted, and the tip advanced an additional distance in order to produce a brain deformation of 2.5 mm at the time of the impact. To induce a non-cavitary level of traumatic injury, the controlled cortical impact device was adjusted to 30 psi giving an impact velocity of ∼3 m/sec. With the help of a heating lamp aiming at the head of the animal, the brain temperature was kept between 36 and 37°C using a temperature probe placed into the temporalis muscle. After cortical injury, the skull defect was closed by using an artificial bone flap, composed of dental acrylic, to avoid extrusion of brain tissue.
Hemorrhagic shock and phases of resuscitation
Using a mechanical standard infusion/withdrawal pump (Harvard Pump Dual RS-232), blood was withdrawn to reduce the mean arterial pressure (MAP) to ∼40 mm Hg for a period of 50 min. The blood volume required to decrease MAP to such a level was ∼2 mL/100 g of weight. Half of this volume was withdrawn in the first 5 min, another 25% over the next 5 min, and the final 25% over the next 5 min. This decelerating rate of blood loss mimics the clinical situation of traumatic blood loss. Animals were kept hypotensive for the remaining hypotensive period if necessary by continued intermittent hemorrhage. The shed blood was collected into citrate phosphate dextrose and kept at 4°C for the duration of the hypotensive and fluid resuscitation period. The shed blood was rewarmed to body temperature (36–37°C) just prior to reinfusion. Following the assigned hypotensive period (50 min), animals were first resuscitated with Lactated Ringer's solution using the infusion pump to maintain a constant infusion rate of 1 mL/min until a MAP of at least 50 mm Hg was obtained. The final resuscitation was accomplished by reinfusion of the shed blood and providing 100% oxygen ventilation after 80 min.
Post-operative management and assessment
After the final resuscitation, anesthesia was discontinued to allow animals to recover. When fully awake, the animals were returned to their cages and allowed free access to food and water. For the first 3 days post-injury, the animals were given buprenorphine 0.1 mg/kg IM q 12 h for analgesia, and enrofloxacin 5 mg/kg IM q d to prevent post-operative infections. Buprenorphine's effects on respiratory depression are relatively minor at this dose and the analgesia regimen was the same in both the treated and placebo groups. 19
Each rat was weighed on the day of beam walking pre-training, the day of surgery, days 1–5 post-surgery, and days 11–15 post-surgery using a digital scale. On days 1–5 post-injury, the animals were tested on the beam-walking and beam-balancing tasks. On days 11–15 post-injury, the animals were tested on the Morris water maze task. Following the last behavioral assessment, the animals were euthanized and the brains removed for histological examination.
Motor tasks
Beam walking task
Each rat was pre-trained 2 days before surgery to walk down a beam 1 m long, 2.5 cm wide, and 1 m above the ground into a darkened goal box to escape white noise of 90 db. At the beginning of each training and test trial, the rat sat in the goal box for 30 sec. During training trials, the rat was placed at successively longer distances from the goal box until it learned to walk down the entire beam. Any distance from which the rat did not walk down the beam into the goal box was repeated until it did. The rat was given a 30 sec rest period in the goal box between trials. After it had traversed the beam in ≤5 sec on three successive trials, four plastic pegs (7.5 cm high) were placed in holes in the beam at ∼20 cm intervals alternating from side to side, 5 mm in from the edge of the beam. The rat was then trained to another criterion of three consecutive trials completed in ≤10 sec. If both of these criteria were not met by 30 trials, the rat was disqualified. The final criterion for inclusion in the study was beam-walking times on the day of surgery with the pegs present that were ≤5 sec on three consecutive trials within 15 trials. Beam walking with the pegs present was assessed on days 1–5 post-injury.
Beam balancing task
Each animal was placed lengthwise along the center of a beam 1.5 cm wide, 1 m long, and 1 m above the ground. The rat attempted to balance on the beam for up to 60 sec on each of three trials on the day of surgery and on days 1–5 post surgery. The rat was taken off the beam and placed in the goal box for 30 sec between trials.
Morris water maze test
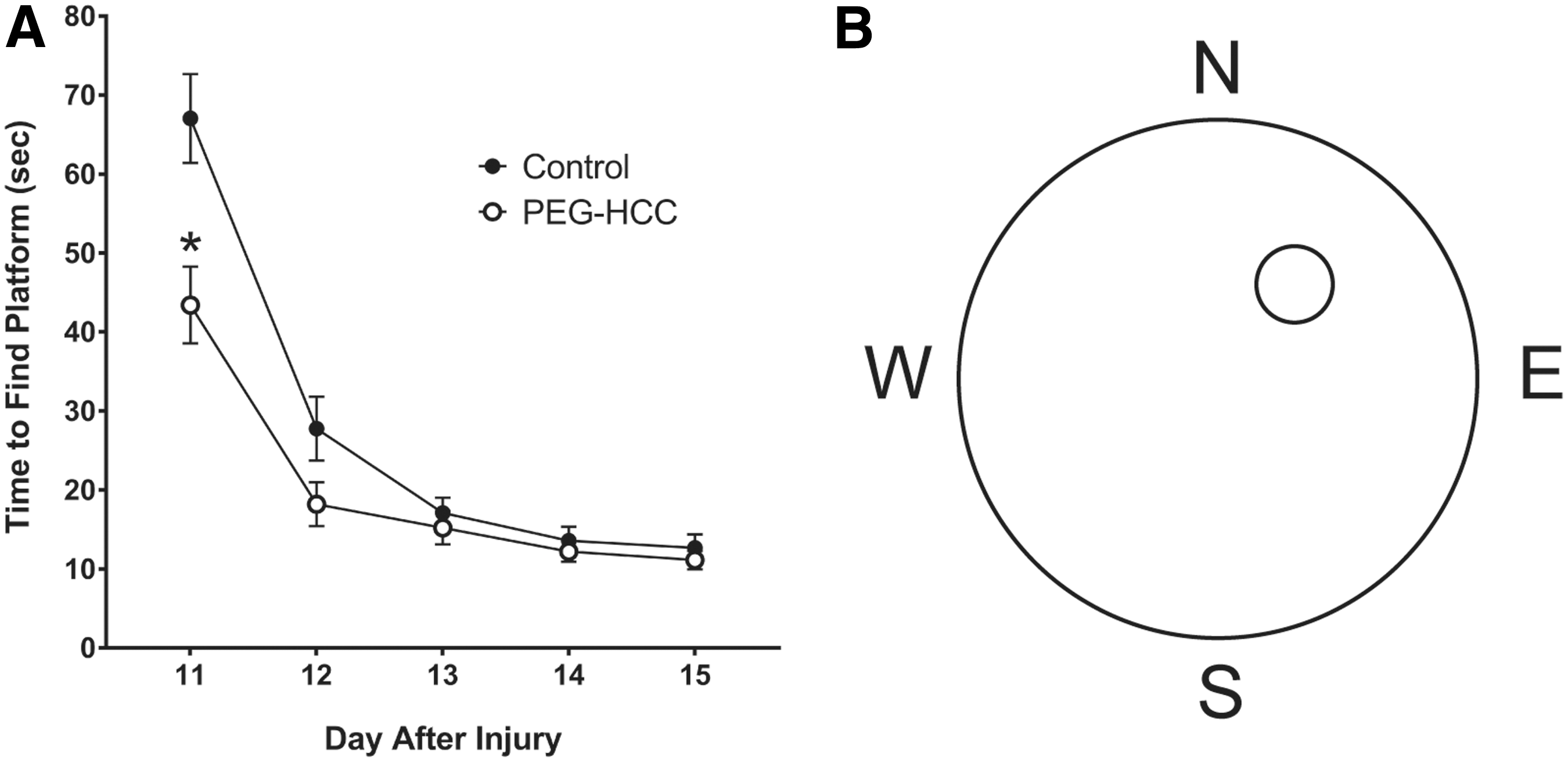
The Morris water maze consisted of a 1.5 m diameter galvanized steel pool which contained a 10 × 10 cm Plexiglas platform 26 cm high and hidden 2 cm below the water. There were four starting positions (north, south, east, west) with a fixed platform. The design of the Morris Water Maze is shown in Figure 3B. Each rat in each group was given a specific sequence to follow throughout the water maze trials. The maze was filled with water until it was 2 cm above the Plexiglas platform. In each trial, the rat was placed in the water facing the wall in the indicated position. If the rat did not find the platform within 120 sec in any trial, it was placed on the platform for 30 sec. If the rat found the platform within 120 sec, it was allowed to remain on the platform for 30 sec. Four trials were performed with 4 min for rest between trials; the rat was kept warm with a heating lamp between trials. The rat was tracked in the water maze with the Water maze 2020 Video Tracking System. Pre-injury performance was not tested. Instead, maze performance was assessed on each of days 11–15 post-injury.
Morris water maze performance.
Histology
At 2 weeks after the impact, the animals were deeply anesthetized, and perfused transcardially with 0.9% saline, followed by 10% phosphate-buffered formaldehyde. The entire brain was removed and fixed in 4% formalin. The fixed brains were examined grossly for the presence of contusion, hematoma, and herniation. The brains were photographed, sectioned at 2 mm intervals, and embedded in paraffin, and hematoxylin and eosin stained slides were prepared cut at 5 μm. Hematoxylin and eosin stained sections were washed with 0.9% saline, followed by 10% phosphate-buffered formaldehyde. The brain sections were photographed using a section scanner (Polaroid Corporation, Waltham, MA) equipped with a PathScan Enabler (Meyer Instruments, Houston, TX). The injury volume was measured by determining the cross-sectional area of injury in each coronal image and multiplying by the thickness of the tissue between the slices. This slab volume technique was implemented on the image-processing program Optimas 5.2 (Optimas Corporation, Seattle, WA). Neurons in the middle 1 mm segments of the cornu ammonis (CA)1 and CA3 regions of the hippocampus were counted at a magnification of 200 × . Neurons were identified by nuclear and cytoplasmic morphology, and individual cells were counted as either normal or damaged. Neurons with cytoplasmic shrinkage, basophilia, or eosinophilia, or with loss of nuclear detail were regarded as damaged. The regions measured were 1 mm long and 1 mm wide (0.5 mm on either side of the long axis of the segment). The total number of neurons and the number of neurons that seemed normal were expressed as neurons per square millimeter.
Statistical analysis
Physiological variables were compared between treatment groups before, during, and after TBI surgery using a t test. The behavioral data were analyzed using repeated measures analysis of variance. When there was a significant time by treatment group interaction, a Holm–Sidak test was used to determine which times were different. Histological indices were analyzed using a t test. Mortality was compared with a Fisher exact test.
Results
Physiological variables
Physiological variables (Table 1) were obtained in a subset of the rats in order to minimize blood loss and because of technical issues. pCO2 was higher, and as a consequence, pH was lower in the placebo control rats at baseline, but this trend shifted to the PEG-HCCs as the experiment progressed. No other significant differences were observed.
Physiological Variables between Control and PEG-HCC-Treated Rats
p value was considered significant at <0.05. Note that complete physiology was successfully obtained from a subset of each group (4 controls, 8 PEG-HCC-treated). Only notable trends were a higher baseline pCO2 and subsequently lower pH in the placebo controls at baseline, which then normalized with a trend for higher pCO2 in the PEG-HCC group as the experiment proceeded.
PEG-HCC, poly(ethylene)glycol conjugated hydrophilic carbon clusters.
Mortality rate
Overall, the mortality rate was 17.9%. Five (23.8%) of the 21 rats in the PEG-HCC group died, and 2 (11.7%) of the 17 rats given saline died (p = 0.20). Mortality occurred through procedural events as well as post-treatment. Although the PEG-HCC mortality was not significantly increased, the higher trend did prompt us to fully characterize each batch, and we discovered that there was variability especially in the extent of PEGylation. Going forward, we set a minimum threshold of 80% PEGylation.
Performance on motor tasks
Overall, the rats that received the PEG-HCC treatment were able to cross the beam an average of 4.6 sec faster than the saline-treated rats (4.2 ± 1.1 compared with 8.9 ± 1.1 sec respectively, p = 0.007). The day x treatment interaction was significant (p < 0.001) for the beam-walking task, and the individual day times required to cross the beam for days 1–3 were significantly faster in the PEG-HCC-treated group (Fig. 1).
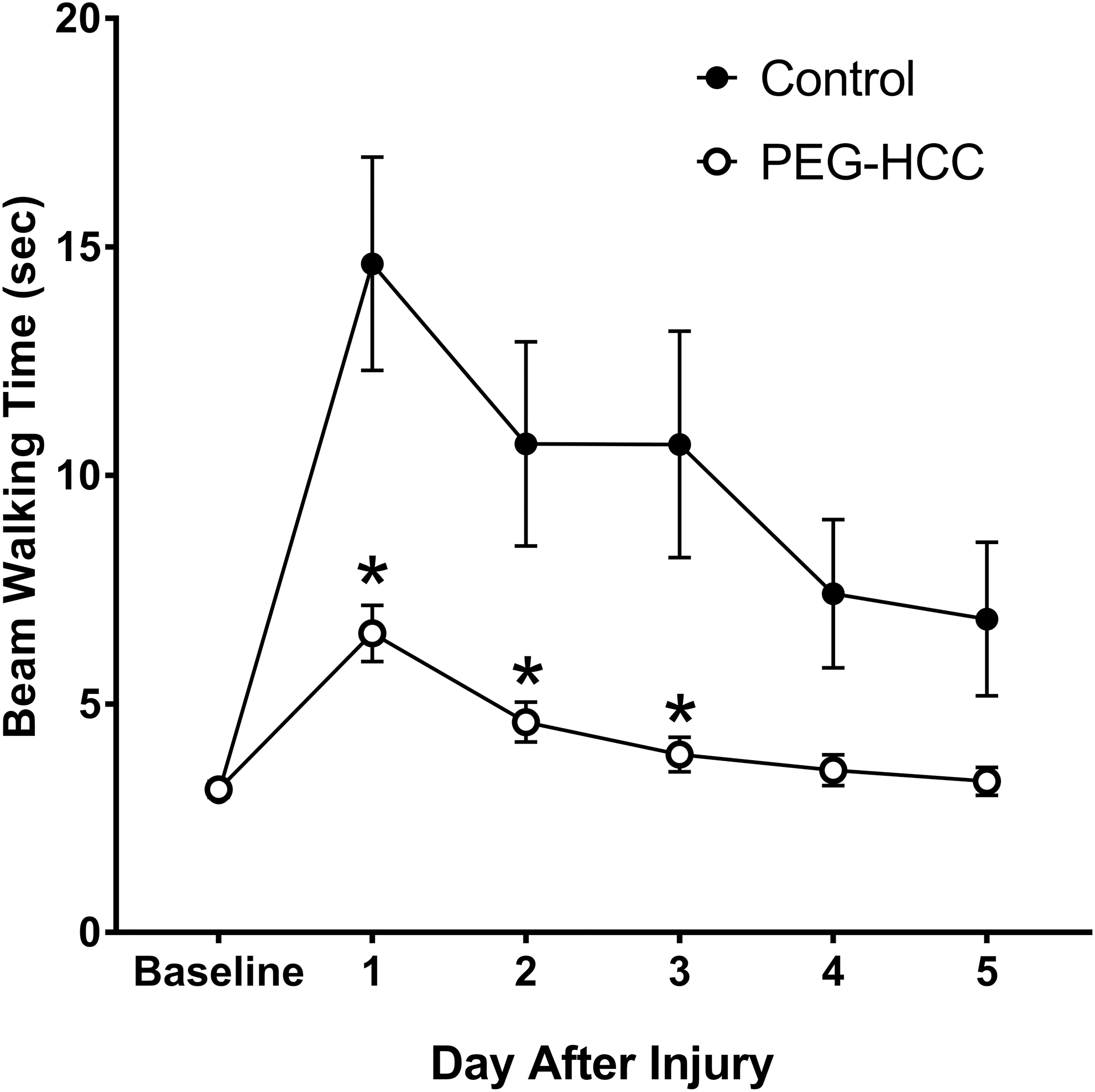
Beam walking performance. Beam walking task results between poly(ethylene)glycol conjugated hydrophilic carbon clusters (PEG-HCC)- and saline- treated subjects. Beam walking time is on the Y axis in seconds and number of days after injury is on the X axis. The time required to traverse a beam is ≤5 sec with four plastic pegs (7.5 cm high) present at ∼20 cm intervals alternating from side to side, 5 mm from the edge of the beam. This task was assessed on days 1–5 post-injury. Results show that PEG-HCC treatment resulted in a significantly reduced beam walking time at all points (treatment effect, p = 0.007; treatment x day interaction, p < 0.001). On average, PEG-HCC-treated animals crossed the beam 4.6 sec faster than saline-treated rats, and the individual day times required to cross the beam for days 1–3 were significantly faster in the PEG-HCC-treated group.
On the beam balance task, the rats that were given PEG-HCC treatment were able to balance an average of 10 sec longer than the saline-treated rats (51.2 ± 1.9 compared with 41.2 ± 1.9 sec, respectively, p < 0.001). The day x treatment interaction was significant (p < 0.001) for the beam balance task, and the individual day times that the rats were able to balance for days 1–4 were significantly faster in the PEG-HCC- treated group (Fig. 2).
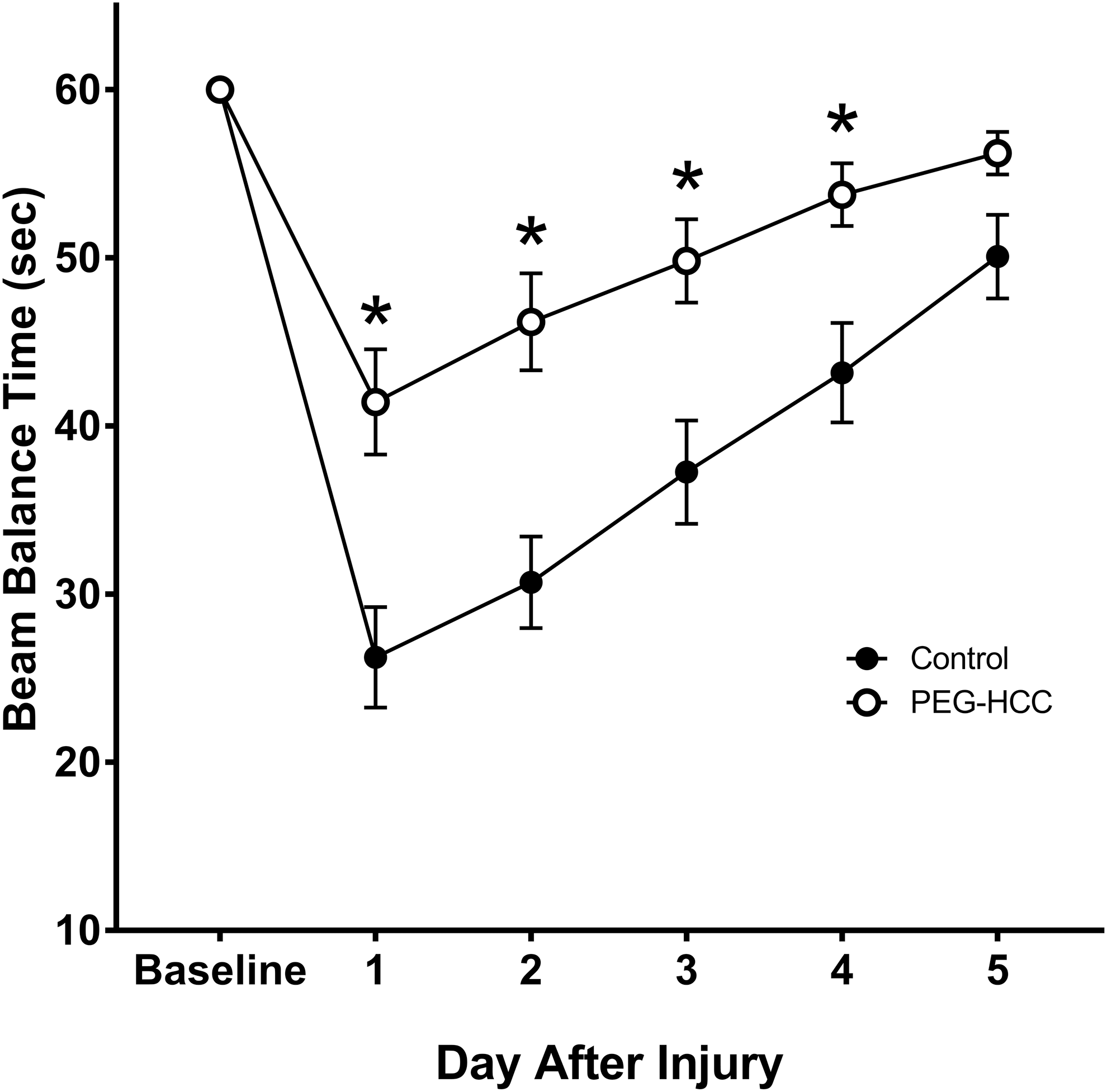
Beam balance performance. Beam balance task results between poly(ethylene)glycol conjugated hydrophilic carbon clusters (PEG-HCC)- and saline- treated subjects. Beam balance time is on the Y axis in seconds and number of days after injury is on the X axis. Each animal was placed lengthwise along the center of the beam and attempted to balance on the beam for up to 60 sec. This task was assessed on days 1–5 post-surgery. Results show that PEG-HCC-treated animals performed significantly better than saline-treated ones (treatment effect, p < 0.001; treatment x day interaction, p < 0.001). On average, rats given PEG-HCC treatment were able to balance 10 sec longer than the saline-treated rats, and the individual day times that the rats were able to balance for days 1–4 were significantly faster in the PEG-HCC-treated group.
Performance on Morris water maze task
For the Morris water maze task, 20 which was performed on days 11–15, the rats that received treatment with the PEG-HCC were able to find the hidden platform an average of 7 sec faster than the saline-treated rats (20.0 ± 1.9 compared with 27.2 ± 1.9 sec, respectively, p = 0.010). Performance on the task rapidly improved in both treatment groups over the days of testing. The day x treatment interaction was significant (p < 0.001) for the Morris water maze task, and the time to find the platform was significantly faster on day 1 in the PEG-HCC-treated group (Fig. 3A).
Histology indices
Contusion volume (Figs. 4 and 5) was 4.6 ± 1.1 mm3 in the PEG-HCC-treated rats, compared with 11.7 ± 3.4 mm3 in the saline-treated rats (p = 0.054), a 61% reduction in volume. CA1 cell counts were 47.1 ± 4.6 and 37.2 ± 4.9 cells/mm2 in the PEG-HCC- and saline-treated animals, respectively (p = 0.154). CA3 cell counts were 28.7 ± 2.9 and 26.7 ± 2.2 cells/mm2 in the PEG-HCC- and saline-treated animals, respectively (p = 0.585).
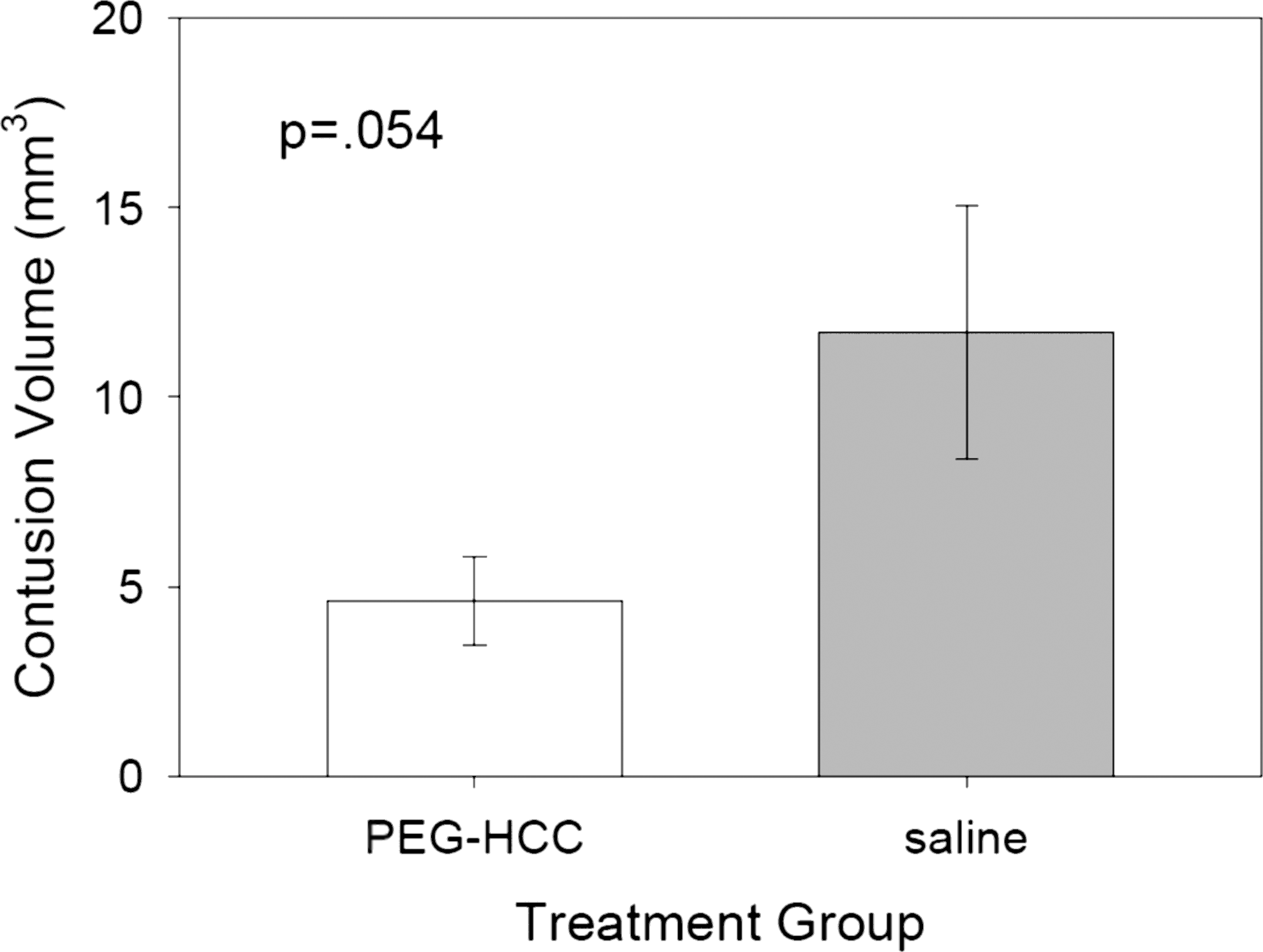
Contusion volume. Contusion volume results between poly(ethylene)glycol conjugated hydrophilic carbon clusters (PEG-HCC)- and saline-treated subjects. Contusion volume in mm3 sec on the Y axis and treatment group is on the X axis. The injury volume was measured by determining the cross-sectional area of injury in each coronal image and multiplying it by the thickness of the tissue between the slices. The contusion volume was measured at 2 weeks post-injury. The PEG-HCC treatment group had a contusion volume of 4.6 ± 1.1 mm3 compared with 11.7 ± 3.4 mm3 in the saline-treated rats (p = 0.054), or a 61% reduction in volume.
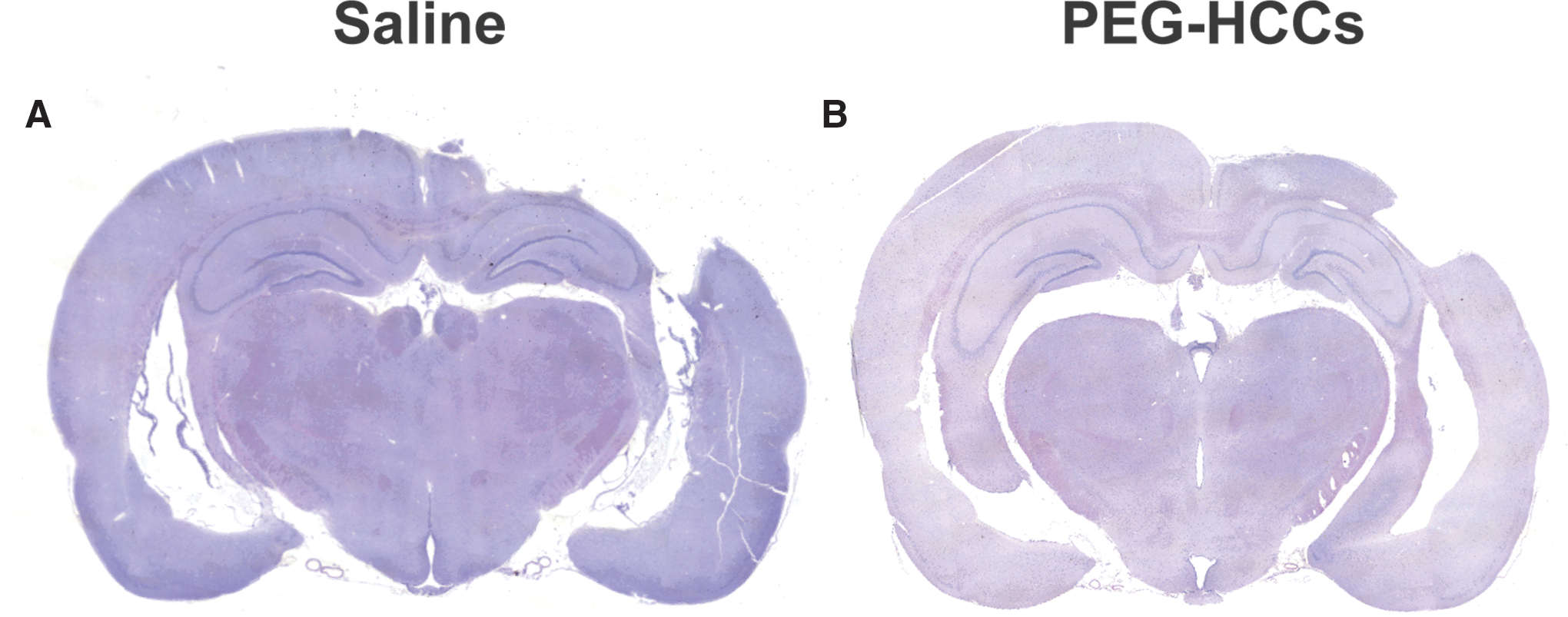
Hemispheric contusion. Right parietal hemispheric contusion comparison of saline-
Discussion
In this study we used a model of TBI that we had previously demonstrated was insufficient to produce minimal visible histological lesion; however, combined with hypotension and resuscitation, it generates structural and functional injury. 3 In the present study, PEG-HCCs, given at the onset of definitive resuscitation and repeated 2 h later, improved measures of functional outcome and reduced lesion size. The exacerbating effect of hypotension suggests that a major vascular injury component accompanies the TBI. Loss of cerebral autoregulation even with mild TBI is likely a factor, and there is evidence, through pre-treatment with antioxidants, that oxidative stress contributes to this phenomenon. 21 –23 In our prior work, administration of the broadly active, catalytic nanomaterial, PEG-HCCs, at the time of “definitive” resuscitation with the reinfusion of blood to restore MAP rapidly and completely restored cerebral blood flow in the affected hemisphere as well as the balance between SO and NO in the vasculature. However, given that there are multiple releases of ROS during this time period, it did not ensure that treatment at this later point would be functionally and structurally beneficial. Here we show that even at this latest time point, the treatment was efficacious both structurally and functionally, suggesting that viable tissue is salvageable.
Based on in vivo studies of PEG alone as a neuroprotectant, we previously considered the possible contributions of the PEG moieties to therapeutic benefit. However, any intrinsic activity of PEG appears to considerably less potent than when attached to PEG-HCCs. For example, in our prior publication, we report that only ∼13% of the PEG-HCCs antioxidant action against SO (using electron paramagnetic resonance) could be explained by the PEG moieties. 14 Additional unpublished work in our laboratory comparing the antioxidant capacity using the Trolox assay, 12,24 of both PEG-HCCs and PEG, found that 1 mole of PEG is equivalent to ∼6 moles of Trolox. However, PEG-HCCs were equivalent to 1500 molar Trolox equivalents. Therefore, of the 1500 Trolox equivalents, only 300 could be accounted for by PEG, leaving the remaining 1200 to be accounted for by the HCC itself, suggesting that the HCC has a considerably larger antioxidant capacity relative to the poly(ethyleneglycol) (PEG) alone. The electron paramagnetic resonance (EPR) data are in good agreement with the Trolox equivalent assay and further support that the PEG alone is not the primary source of antioxidant activity.
There is a similar difference in magnitude of contribution seen in vivo. There are studies indicating that PEG showed efficacy protecting spinal cord and cortical tissue from injury following blunt force trauma. 25 –28 However, the doses of PEG used were ∼70–100-fold higher than what was injected here as part of the PEG-HCC (see Table S1 for details on prior studies). For example, work by Koob and coworkers 25 demonstrated that 1000 mg/kg PEG following a pneumatic ram-induced TBI in rats significantly reduced lesion size. By comparison, the total concentration of PEG (covalently bound to the PEG-HCCs) in our studies is ∼10 mg/kg. We therefore do not consider the PEG moieties to be responsible for the majority of benefit seen both here and in our prior studies.
PEG-HCCs have unique properties that potentially explain their effectiveness in injured tissue. PEG-HCCs are water-soluble carbonaceous particles that are stable without refrigeration and showed no toxicity in an acute TBI model or in mice following 10 weeks of weekly treatment. They have inherent antioxidant properties that differ from other agents. 5,12 In vitro, they are protective against the lethal effects of the mitochondrial toxin, antimycin A, even when administered after the toxin, whereas conventional agents such as PEG-SOD or the small molecule PBN were only effective in much higher doses and only when pre-treatment was used. 5,12
Additional protective effects may involve restoration of the balance between SO and NO. The damaging anion peroxynitrite mediates many of the deleterious effects of oxidative stress caused by the irreversible oxidation of nucleic acids, lipids, and amino acids. 29 Excess production of SO versus NO can occur through a variety of mechanisms including uncoupling of nitric oxide synthase (NOS). 29,30 In our prior work in this model, we found that PEG-HCCs restored a condition that we have termed “functional uncoupling,” 29 the excess of perivascular SO versus NO irrespective of their sources. We also demonstrated that PEG-HCCs do not react directly with NO but do catalytically quench SO, 14 and we considered recoupling of NOS as a potential mechanism for restoration of oxidative balance. 12 Future studies will directly address peroxynitrite as well as the coupling status of NOS.
Limitations of the model include the use of concomitant medications. For example, buprenorphine may produce respiratory depression, 19 although the rats are intubated during the surgical procedure. Moreover, it is unlikely that any effects on blood pressure or respiration could explain these results, as the drug was administered to both cohorts. The analgesics were administered to both the control and experimental arms to control for potential effects.
The use of pre-clinical TBI models in general for identifying promising therapeutics has been extensively discussed, given the failure of clinical translation. 31 –33 Some of these issues are inherent to use of non-human species, such as species differences in pathological mechanisms, whereas others are possible to address, including lack of information related to physiological variables, lack of important co-morbidities, unrealistic treatment windows, sex differences, and others. Our methods address some key factors including a realistic treatment time point and incorporation of one of the most important comorbidities related to TBI outcome regardless of severity of injury: systemic hypotension. Other factors need to be studied in the future including sex differences and other models and species to insure these results are not unique. The promising longer-term results seen here that complement our earlier finding of acute benefit to restoration of blood flow, suggest that PEG-HCCs are worth studying under these different conditions. Moreover, our results support that the oxidative burst associated with the onset of resuscitation contributes to worsened outcome and is a potential therapeutic target even at this later time point.
Footnotes
Acknowledgments
This work was supported by the National Institutes of Health (NIH) (R01 NS094535 T.A.K., J.M.T.), Department of Defense CDMRP PT074693P (T.A.K.), Grant No. BE-0048 from the Welch Foundation (T.A.K.), the National Defense Science Engineering Graduate (NDSEG) Fellowship (K.M.), and Department of Defense W81XWH-08-2-0132 (C.S.R.)
Author Disclosure Statement
Drs. Kent and Tour are named inventors on intellectual property surrounding the PEG-HCCs. The intellectual property is owned by their respective universities. The other authors have nothing to disclose.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.