
Abstract
The quantification and objective documentation of autonomic dysfunction in traumatic brain injury (TBI) is neither well studied nor extensively validated. Most of the descriptions of autonomic dysfunction in the literature are in the form of vague non-specific clinical manifestations. Few studies propose the use of objective measures of assessing the extent of autonomic dysfunction to link them to the outcome of TBI. Our goal was to perform a scoping systematic review of the literature on the objective documentation of autonomic dysfunction in terms of functional and physiological variables to be linked to outcome of TBI. PubMed/MEDLINE®, BIOSIS, Scopus, Embase, Cochrane Libraries, and Global Health databases were searched. Two reviewers independently screened the results. Full texts for citations passing this initial screen were obtained. Inclusion and exclusion criteria were applied to each article to obtain final articles for review. The initial search yielded 2619 citations. Of 69 articles selected for final review, 14 were chosen based on the inclusion and exclusion criteria and are included in the results of this article. 9 of these articles assessed autonomic dysfunction using functional variables and 7 assessed autonomic dysfunction using physiological variables. Some studies included both functional and physiological variables. Of the nine studies linking autonomic dysfunction to functional variables, nine included heart rate variability (HRV), three included baroreflex sensitivity (BRS), and two included blood pressure variability (BPV). A total of 2714 adult patients were studied. Although the nature of association between autonomic dysfunction and outcome is unclear, the objective quantification of autonomic dysfunction seems to be associated with global patient outcome and other neurophysiological measures. Further studies are needed to validate its use and explore the underlying molecular mechanisms of the described associations.
Introduction
Autonomic dysreflexia (AD), also known as paroxysmal sympathetic hyperactivity (PSH), is a lesser studied phenomenon associated with traumatic brain injury (TBI). Although it is well described in spinal cord injury, it can be caused by various forms of injury to the central nervous system (CNS) including hypoxic brain injury, stroke, and brain tumors. 1 PSH is described as episodes of paroxysmal transient increase in sympathetic activity, manifested in the form of hypertension, hyperthermia, tachycardia, tachypnea, spasticity, and diaphoresis to non-noxious stimuli. 2 It can affect both the adult and pediatric population with severe TBI, with an incidence of 8–33%. 3 Recognizing PSH early in its course has been proposed as a means to determine outcome in TBI.
The quantification and objective documentation of autonomic dysfunction is not well studied or extensively validated in TBI. Most of the descriptions of autonomic dysfunction in the literature are in the form of vague non-specific clinical manifestations that include hypertension, hyperthermia, tachycardia, tachypnea, spasticity, and diaphoresis. A few studies proposed the use of objective measures of assessing the extent of autonomic dysfunction, including heart rate variability (HRV), baroreflex sensitivity (BRS), microneurography, and catecholamine sampling. The goal of this scoping review is to evaluate if objective documentation of autonomic dysfunction is linked to patient functional outcome or neurophysiological variables in adult moderate/severe TBI.
Methods
A systematic review using the methodology outlined in the Cochrane Handbook for Systematic Reviewers was conducted. 4 Data were reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 5 The search strategy was decided on by the primary author (M.H.) and supervisor (F.A.Z.).
Search question, population, and inclusion and exclusion criteria
We aimed to answer the broad question: What literature is available that documents the association between objectively measured autonomic dysfunction and both patient functional outcome and neurophysiological outcomes in adult moderate/severe TBI patients?
Objective measures of assessing the extent of autonomic function included HRV, BRS, blood pressure variability (BPV), microneurography, and catecholamine sampling. We also included sample entropy, apparent entropy, and multi-scale entropy calculations for heart rate (HR) and arterial blood pressure (ABP) as potential measures of HRV and BPV, respectively.
The primary outcome of interest was any association with patient functional outcome. The secondary outcome of interest was any association with other neurophysiological variables commonly recorded/measured during the intensive care unit (ICU) phase of care, including: intracranial pressure (ICP), cerebral perfusion pressure (CPP), brain tissue oxygen (PbtO2), cerebral oximetry, cerebral near-infrared spectroscopy (NIRS), cerebral blood flow (CBF)/cerebral blood flow velocity (CBFV), or cerebrovascular reactivity (as measured through any means of vascular reactivity/autoregulation bedside monitoring).
Inclusion/exclusion criteria
Inclusion criteria were: adult patient populations (i.e. being ≥18 years of age), moderate or severe TBI (defined as admission Glasgow Coma Scale [GCS] of 9–12 for moderate, and ≤8 for severe), prospective or retrospective study design, quantitative measurement of autonomic function (defined as objectively measured: HRV, BRS, BPV, HR, or ABP signal/sample entropy, microneurography, and catecholamine sampling), assessment at any point during acute admission or inpatient rehabilitation phase of care, and studies being in the English language.
Exclusion criteria included: pediatric patient populations, mild TBI only, subjective descriptions of autonomic dysfunction in the absence of quantitative assessments, and non-English-language studies.
Search strategy
Six databases were searched from inception up to the beginning of October 2017: PubMed/MEDLINE®, BIOSIS, Scopus, Cochrane Libraries, Global Health, and Embase. Following study selection, reference sections of each article were examined to ensure that relevant articles not captured by the initial search were included in the review. Appendix S1 highlights the search strategy implemented for each database (see online supplementary material at
Study selection
A two step review was performed. Two reviewers independently screened each resulting title and abstract from the initial search to determine if they met the inclusion criteria. Full texts for citations passing this initial screen were obtained. Inclusion and exclusion criteria were applied to each article to obtain final articles for review.
Data collection
Data were extracted from the final list of articles and stored electronically. Data from adult populations were organized into the following categories: objective measures of assessing the extent of autonomic dysfunction either linked to functional variables or to physiological variables. Data extracted included study country, design, objectives, outcomes, and conclusions made by the study authors.
Quality of evidence assessment
Each study was evaluated for quality of evidence using the RTI Item Bank on Risk of Bias and Precision of Observational Studies.
6
This validated item bank is applicable to a variety of observational study designs and evaluates the risk of bias and internal validity of studies using a comprehensive list of itemized questions. Tables S1 and S2 provide the tabulated results of the bias assessment for each study included in this scoping review (see online supplementary material at
Statistical analysis
A meta-analysis was not performed because of the heterogeneity of data, study design, and objective definition/measure of autonomic dysfunction within the studies. Therefore, this study comprises only a systematically conducted scoping review.
Results
The initial search yielded 2619 citations. Of 69 articles selected for final review, 14 were chosen based on the inclusion and exclusion criteria, and will be included in the Results section of this article. 7 –20 All studies are prospective observational studies except for three. Nine of the articles assessed autonomic dysfunction in relation to functional variables and seven assessed autonomic dysfunction in relation to physiological variables. Some studies included both functional and physiological variables. Of the nine studies that linked autonomic dysfunction to functional outcome variables, nine included HRV, three included BRS, and two included BPV. A total of 2714 adult patients were studied. A total of 2714 patients were included in the review. The age range was 14–84 and the male to female ratio was 2.8:1. Figure 1 displays the PRISMA flow diagram of the search results and filtering processes.
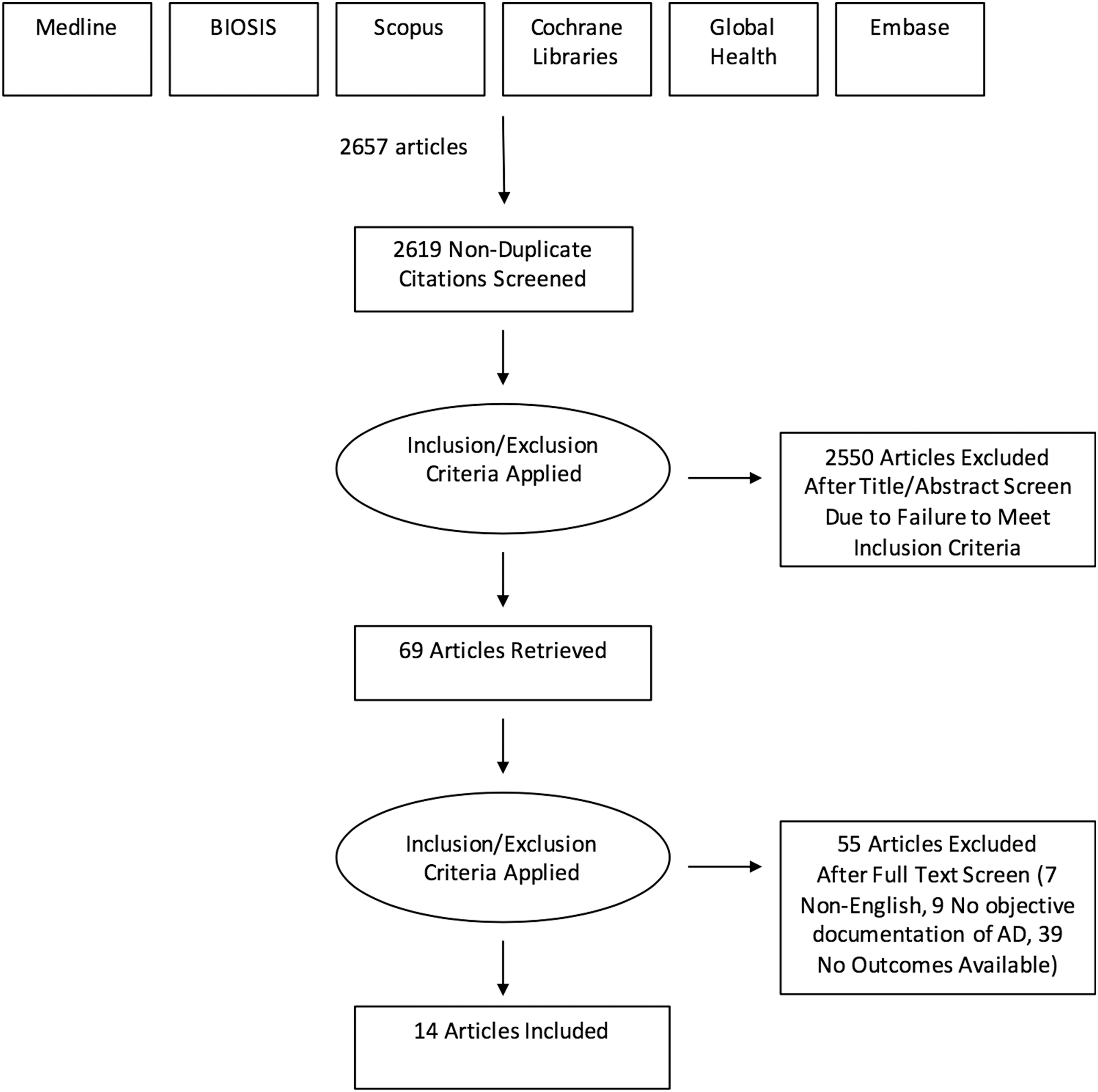
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the search results and filtering processes.
Functional variables
HRV
Nine studies assessed the use of HRV as a predictor of patient neurological outcome and mortality. 7 –15 Outcomes studied include mortality, length of stay (LOS), Glasgow Outcome Score (GOS) at 3 months, GOS at discharge, 12 month Glasgow Outcome Scale Extended (GOSE) score, pupillary examination, and functional scales (Early Functional Assessment [EFA] and Functional Independence Measure [FIM]). A total of 2625 patients were included. The age range was 14–84 and the male to female ratio was 2.75:1.
All studies are prospective observational studies except for two (retrospective chart reviews). In acute TBI patients, low HRV and sustained decrease in low-frequency (LF)/high-frequency (HF) HR signals, which indicates lower sympathetic regulation over HR rhythms, were linked with a high mortality rate. The mean total frequency (TF) (0.43 ± 0.29 vs. 1.11 ± 0.74, p < 0.05), and mean LF/HF (0.22 ± 0.29 vs. 0.62 ± 0.28, p < 0.01) were significantly successful in separating survivors from non-survivors. 8 This was significant, also, for very low frequency (VLF) (p < 0.001) and LF (p < 0.05) but not HF bands (p = 0.11). 11 All studies included linked LF/HF ratio to outcome except for one study that did not show a significant difference between the good and bad outcome groups. HF had the highest sensitivity (88%) and specificity (82%) to predict poor late neurological outcome in this group of patients. 12 One study investigated the association between HRV and functional outcome scales during neurorehabilitation, including EFA FIM. 13 Table 1 displays the studies on HRV and patient functional outcome.
The Studies on HRV and Patient Functional Outcome
HRV, heart rate variability; HR, heart rate; BRV, blood pressure variability; BRS, baroreflex sensitivity; GOS, Glasgow Outcome Scale; TBI, traumatic brain injury; OR, odds ratio; ICU, intensive care unit; TF, total frequency; Glasgow Coma Score; RRI, R-R interval; LOS, Length of stay; GOSE, Glasgow Outcome Scale-Extended; DRS, Disability Rating Scale; ANS, Autonomic nervous system; TP total power; ROC, receiver operator curve; EFA, early functional ability; FIM, Functional Independence Measure; RLAS, Ranchos Los Amigos Score; SDNN, standard deviation of normal-to-normal
BRS
Three prospective observational studies assessed changes in BRS in TBI during the ICU stay, as a prognostic parameter to predict neurological outcome. 8,11,12 All studies included patients with TBI, with the exception of one study that included all critically ill neurosurgical patients, for which the data on the TBI subcohort were extracted from the parent manuscript where possible. Outcomes studied include mortality, GOS at 3 months, GOS at discharge, and GOSE score at 1 year. A total of 68 patients were included. The age range was 14–83 and the male to female ration was 3.5:1.
BRS was found to be significantly lower in patients with good outcome (GOSE score ≥5) at 1 year (receiver operator curve [ROC] areas >0.78 with statistical significance set at p < 0.05). 12 The average value for patients with a good outcome was found to be 8.7 ± 0.2 msec/mm Hg vs. 4.4 ± 1.5 msec/mm Hg for patients who subsequently died (p = 0.03). 11 The mean TF of BRS was significantly successful in separating survivors from non-survivors (p < 0.05). Table 2 displays the studies on BRS and patient functional outcome.
The Studies on BRS and Patient Functional Outcome
HRV, heart rate variability; BRS, baroreflex sensitivity; GOS, Glasgow outcome scale; TBI, traumatic brain injury; ICU, intensive care unit; TF, total frequency; GOSE, Glasgow Outcome Scale-Extended; ROC, receiver operator curve.
BPV
Two prospective observational studies investigated BPV longitudinally in acute TBI patients and critically ill neurosurgical patients in the ICU, relating them to the severity of neurological dysfunction and outcome. 8,11 For the study on critically ill neurosurgery patients, data were extracted for the TBI subpopulations where possible. Outcomes studied include mortality and GOS at 3 months. A total of 49 patients were included. The age range was 18–83 and the male to female ratio was 4.4:1.
Both studies demonstrated that BPV was not associated with global outcome or mortality. 11 Table 3 displays the studies on BPV and patient functional outcome.
The Studies on BPV and Patient Functional Outcome
BPV, blood pressure variability; GOS, Glasgow Outcome Scale, TBI, traumatic brain injury; ICU, intensive care unit.
Physiological variables
Seven studies demonstrated associations between HRV and other neurophysiological measures including: ICP, CPP, and pressure reactivity index (PRx, a continuous index of cerebrovascular reactivity, derived through the moving correlation coefficient between ICP and mean arterial pressure). All studies are prospective observational studies except for two (both retrospective observational). A total of 343 patients were included. The age range was 20–82 and the male to female ration was 3.8:1.
In acute TBI patients, decreased HRV was associated with episodes of increased ICP and decreased CPP. 15 Moreover, the rate of return of HRV reflects the subsequent state of neuronal function; even when ICP has been restored to normal, HRV was found to be decreased rapidly if ICP rose. 19 The drop in HRV was found to be linked to CPP. HRV was found to increase in response to increasing ICP when CPP >60 mm Hg (p < 0.001), but decreased when CPP <60 mm Hg, even with ICP <20 mm Hg (p < 0.001). 17 HRV has been linked to plateau waves (defined as acute elevation of ICP to >50 mm Hg for 5–20 min 21 ) in the form of dramatic increase in HRV in the latter part of the plateau wave, followed by a decrease after the event and a new increase during the recovery. 16
A significant correlation was found between PRx and HRV spectral power in TBI (p < 0.001). 18 The HF component of HRV (0.15–0.4 Hz) can be used to predict impaired autoregulation (PRx >0.2), although sensitivity and specificity are low (ROC area under the curve [AUC] = 0.67; p = 0.001). Table 4 displays the studies on HRV and association with neurophysiological measures.
The Studies on HRV and Association with Neurophysiologic Measures
HRV, heart rate variability; HR, heart rate; TBI, traumatic brain injury ICP, intracranial pressure; BPV, blood pressure variability; CPP, cerebral perfusion pressure; PPVi, integer pulse pressure variability; HR, high frequency; ROC, receiver operator characteristic; AUC, area under the curve; CNS, central nervous system.
Quality of evidence
Quality of evidence was assessed using the RTI Item Bank on Risk of Bias and Precision of Observational Studies. 6 Based on its itemized list of questions, there was an overall low risk of bias in the studies included in this review.
Discussion
HRV and patient functional outcome
VLF, LF, HF, and TF components of HRV have been used and investigated to quantify the degree of sympathovagal balance of the autonomic nervous system. TF is a non-spectific variable that reflects the overall autonomic activity. LF is a band of power spectrum considered to be a strong indicator of sympathetic activity. VLF reflects slow mechanisms of sympathetic function too, but to a lesser extent. On the other hand, the HF band is linked to parasympathetic (vagal) activity. Various combinations of these frequency bands have been proposed to quantify the AD associated with various conditions, including TBI, linking them to outcome measures. LF/HF ratio and TF are examples of these combinations that are somewhat controversial in terms of application and ability to predict outcome. Nine studies in our review were found to validate the use of HRV as a predictor of patient outcome and mortality.
All studies are prospective observational studies except for two (retrospective chart reviews). All studies included linked HRV to outcome in TBI except for one study that included the diverse spectrum of traumatic injuries. 7 Among different combinations of the frequency bands of HRV, VLF (p < 0.001), LF (p < 0.05) and mean TF (p < 0.05) were found to be consistently significant in various studies investigating their predictive role. The mean LF/HF ratio was found to have a predictive value in one study (p < 0.05), 8 but Hendén and coworkers found that there was no significant difference between the good and bad outcome groups. 12 HF bands were controversial, too, with one study found to have no significant difference (p = 0.11), 11 whereas another concluded that they had the highest sensitivity (88%) and specificity (82%) to predict poor late neurological outcome in this group of patients. 12
Vistisen and coworkers 13 investigated the association between HRV and functional outcome scales during neurorehabilitation, including EFA and FIM. They found that standard deviation of normal-to-normal (NN) intervals (SDNN) and LF of HRV and its change during neurorehabilitation stay were associated with EFA changes over time at follow-up (p < 0.05) but not with FIM. Admission SDNN and LF were unable to provide prognostic information for the EFA and FIM at follow-up.
One study that included the diverse spectrum of traumatic injuries 7 failed to find a link between HRV and outcome in TBI. It found that early reduction of HR-multi-scale entropy (MSE) was associated with increasing mortality and was independent of probability of survival in all multivariate analyses across diverse injury etiologies including TBI (odds ratio [OR] 0.87–0.94). The relationship between MSE and death was moderately stronger in patients with isolated severe brain injury than in those with torso injury, and significantly stronger in patients with penetrating versus blunt mechanisms of injury. Gao and coworkers addressed the question about the timing of HRV and whether it implied a difference in the predictive power. 14 They found that there are significant differences across groups classified by the GCS in apparent entropy (ApEn)-HR (p = 0.007) in the first 6 h, which strengthened in a 24 h and 72 h analysis and was a significant independent predictor of mortality and favorable outcome (p < 0.001).
BRS and patient functional outcome
Regarding BRS, all studies included in this review found that BRS could predict good outcome (defined as GOSE score ≥5). One study found that the mean TF of BRS was successful in separating survivors from non-survivors. 8 The effect of the various medication used in the ICU is a concern when it comes to the interpretation of the value of BRS. Hendén and coworkers found that the use of BRS use for prognostication purposes was not affected by active ICU treatment of sedative, analgesic, and vasoactive drugs. Interestingly, BRS tended to better predict death than did the initial GCS score, which is the most widely used scoring system in the field of neurosurgery. 11
It has been proposed by Hendén and coworkers that the predictive power improved slightly when combining various autonomic indices (HRV and BRS as an example in their study) but this has not been widely addressed in other studies in the review. 12
BPV and patient functional outcome
BPV has the least number of studies for investigating its association with outcome. It seems that there is no predictive value for survival or functional outcome in either TBI patients or critically ill neurosurgical patients in any of the studies found in this review (both were prospective observational studies).
Association with neurophysiological measures
The presence of altered HRV in patients with brain injury has been known for many years to be correlated with severity of neurological injury and ICP elevations. 22 The automated analysis of HRV has been proposed to offer a non-invasive means to monitor autonomic function that can be widely applied in relation to physiological variables of the CNS including ICP, CPP, and PRx.
Winchell and coworkers 15 showed that the analysis of temporally matched ICP and CPP data was significant, and correlated to HRV in terms of low total power (TP) and high HF/LF ratio during the acute phase of the injury. During recovery, they found that low HF/LF ratio was associated with episodes of apparent improvement (lower ICP and higher CPP), which may provide an indication of possible improvement. Lowensohn and coworkers suggested that HRV may reflect the functional state of the CNS, too, as they found that the rate of return of HRV reflected the subsequent state of neuronal function, even when ICP had been restored to normal as seems to occur in the fetus. 19 Kahraman and coworkers proposed that the correlation between HRV and ICP seemed to be linked to CPP. In the case of CPP >60 mm Hg, HRV was found to increase in response to increasing ICP (p < 0.001). 17 HRV was found to increase when CPP <60 mm Hg, even with ICP <20 mm Hg (p < 0.001). This observation might imply that HRV might be better correlated to CPP instead of ICP to evaluate the status of the CNS injury and recovery. Plateau waves of ICP are acute elevation of ICP to >50 mm Hg for 5–20 min. 21 After a continuous period of elevation, termination of the wave is characterized by a rapid decrease of ICP. In the latter part of the plateau wave, Luis and coworkers found that HRV was linked to plateau wave in ICP. 16 They found that there was a dramatic increase in HRV (LF and HF), followed by a decrease after the event and a new increase during the recovery.
Cerebral blood vessels are innervated by autonomic fibers. Therefore, the autonomic nervous system is thought to modulate the autoregulation of cerebral blood flow in humans. 23 This can explain why autonomic disorders can severely affect cerebral vasoreactivity. Impairment of cerebral autoregulation following TBI might be related to the autonomic system dysfunction. Lavinio and coworkers found a significant correlation between cerebrovascular autoregulation (PRx) and HRV spectral power in TBI (p < 0.001). 18 Gao and coworkers reached the same conclusion and found the HF component of HRV (0.15–0.4Hz) specifically linked to impaired autoregulation (PRx >0.2), although sensitivity and specificity were low (ROC AUC = 0.67; p = 0.001). Collectively, this might suggest that with some refinements, HRV might become a tool for screening patients at risk for cerebral autoregulation derangement following TBI.
Limitations
There are a number of limitations to this review. First, the definition of what constitutes autonomic dysfunction varied significantly among studies. Dysautonomia may represent a spectrum of varying severity and duration that can be difficult to distinguish from other common complications associated with critically ill patients. If there were episodes of dysautonomia coexistent with systemic infection, for example, then the autonomic symptoms could be attributed to the systemic inflammatory response and the exact incidence of dysautonomia in the TBI populations described may be overestimated.
Second, the studies included in this review have a small sample size insufficiently powered to validate the questions studied, suggesting the need for multi-center projects in the future to solve this issue.
Third, another limitation is the effect of the other clinical variables, such as medications (i.e. sedation and ionotropic support) and ventilator settings on the parameters assessed. Most populations described consisted of heterogenous polytrauma patients, with heterogeneous patterns of TBI. Further, the therapies received during the ICU stay varied among patients and centers, further impeding the ability to obtain a clear understanding of the links between dysautonomia and both patient outcome and neurophysiological measures. The potential for variability in injury, cerebral pathology, and therapies on the various measures of autonomic dysfunction, neurophysiological measures, and patient outcomes cannot be understated.
Fourth, another important point is the time frame of assessment. The majority of the studies failed to include the exact timing of assessment. Some studies used short, one-time-point measurements, which might explain some controversial observations. Continuously updating measures based on sliding calculation windows would provide increased temporal data resolution, while providing data streams for online monitoring of such variables during the ICU stay for these patients. This was described in some of the included studies, 14,18 but not all. Future work in this area requires this type of higher frequency data.
Finally, there exist the technical challenges of data capture. In addition to diversity and variability, some concerns were raised about consistency and external validation within the parent manuscripts. Further to this, most studies did not exclude patients with other system injuries such as severe chest injuries and injuries of the abdominal regions. The potential impact of cardiac or central vascular injury was not properly assessed. Few studies limited the patient population to isolated brain injury patients, which is difficult, given that these TBI patient populations typically consist of heterogeneous polytrauma patients.
Future directions
Increased understanding of the natural history and the pathophysiology of this autonomic dysreflexia will be required to improve the design of future studies. Future research should focus on prospective analyses to improve understanding of the pathophysiology and etiology of dysautonomia, improving our ability to predict which moderate/severe TBI patients are at highest risk of developing this condition. Next, further analysis of the link between autonomic dysfunction and other neurophysiological measures is important. Preliminary works suggested the link between this and impaired cerebrovascular reactivity, which has a strong link to global outcome in TBI. 24 –26 There exists the potential that autonomic dysfunction/failure is a trigger for impaired cerebral autoregulation. Finally, exploring the link between both serum/microdialysate/cerebrospinal fluid biomarkers of dysautonomia and individual genetic profiles will allow for the elucidation of molecular targets that will produce therapies directed at prevention and treatment. Such studies are possible using the high-resolution data sets from large ongoing prospective observations studies in TBI, and are planned. 27,28
Conclusion
Although the nature of the link between autonomic dysfunction and outcome is unclear, the objective quantification of autonomic dysfunction seems to be associated with global patient outcome and other neurophysiological measures. Further studies are needed to validate its use and explore the underlying molecular mechanisms of the described associations.
Footnotes
Acknowledgments
F.A.Z. has received salary support for dedicated research time, during which this project was partially completed. Such salary support came from: the Cambridge Commonwealth Trust Scholarship, the Royal College of Surgeons of Canada – Harry S. Morton Travelling Fellowship in Surgery, and the University of Manitoba Clinician Investigator Program. F.A.Z.'s research program is supported through the University of Manitoba Thorlakson Chair in Surgical Research Establishment Fund.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.