
Abstract
Depression following a traumatic brain injury (TBI) is common and difficult to treat using standard approaches. The current study investigated, for the first time, transcranial magnetic stimulation (TMS) for the treatment of post TBI depression. We specifically assessed the safety, tolerability, and efficacy of TMS in this patient population. We also explored cognitive outcomes. Twenty-one patients with a current episode of major depression subsequent to a TBI participated in a randomized double-blind placebo-controlled trial of repetitive TMS (rTMS). Sequential bilateral rTMS (to the left and right dorsolateral prefrontal cortex) was provided in 20 treatments over a period of 4 weeks. Patients were randomly allocated to receive either active or sham stimulation. There were no adverse effects and treatment was well tolerated. There was no significant effect of rTMS on post-TBI depression, with all patients showing a significant improvement in depressive symptoms irrespective of their treatment group (p = 0.002). There were significant improvements in cognition following active rTMS in the areas of working memory (p = 0.021) and executive function (p = 0.029). rTMS was shown to be safe and well tolerated in patients who had developed depression after a TBI. We did not find a therapeutic effect for post-TBI depression; however, this approach may have some utility in improving cognitive function. Future research should focus on alternative rTMS treatment approaches for post-TBI depression and the direct investigation of rTMS as a treatment for cognitive impairment in TBI.
Introduction
Traumatic brain injuries (TBIs) are common and disabling, and it is estimated that they will become the third leading cause of disability and death internationally by 2020. 1 There are a number of behavioral consequences that can occur following TBI, including psychiatric and cognitive sequelae. 2 In particular, depression is a very common and well-recognized psychiatric outcome following TBI. There are a number of biopsychosocial factors thought to contribute to the onset of depression in this group; for example, a recent large prospective study (n = 559) identified that previous history of mental illness, substance use, and alcohol dependence were predictive of a depressive trajectory following TBI. 3 Major depression has been reported in between 25% and 60% of patients within 12 months following injury, and is associated with poorer recovery and increased lifetime suicide rates. 4,5 Selective serotonin reuptake inhibitors (SSRIs) and other antidepressants are commonly used in the treatment of post-TBI depression; 5,6 however, there is a substantial lack of double-blind randomized- controlled trials of adequate quality in this specific area of application. 4,5 The few such trials conducted to date have not found SSRIs (namely sertraline) to be superior to placebo in the treatment of post-TBI depression. 7,8 Additionally, a recent meta-analysis looking at non-pharmacological interventions for depression following TBI did not find “compelling evidence” for any of the approaches reviewed. 9 Therefore, although there have been some promising findings, these have largely been in small or uncontrolled trials, and more research is required to determine the efficacy of current treatment approaches for post TBI depression. 9
In addition to depression, cognitive impairment is a common and often debilitating outcome of TBI. 10 Areas most commonly affected include speed of information processing, attention, memory, and executive functioning. As with depression, there is a lack of effective treatments for these cognitive impairments. 2,11 The relative ineffectiveness of standard treatments for depression and cognitive impairment following TBI is likely related to the contribution of structural and functional brain changes that follow injury.
The presence of both depression and cognitive impairment following TBI is believed to be related to the complex pathophysiological cascade that occurs following injury, which results in structural and functional impairments in neural networks. 10,12,13 There is now considerable evidence that depression is a disorder of network dysfunction; namely, resulting from prefrontal-corticolimbic dysregulation. 14,15 Similarly, the cognitive functions commonly affected following injury (i.e., speed of information processing, attention, memory, and executive functioning) depend heavily on the integrated activity of neural networks throughout the brain. 16 Following a TBI, there are a series of neurometabolic and cytoskeletal changes that can lead to impairments in structural and functional connectivity. 10,13 Therefore, treatments aimed at enhancing neural connectivity in the relevant brain regions would represent a novel pathophysiologically based approach to treatment of depression following TBI, as well as potentially improving cognitive function. Recent research has shown non-invasive brain stimulation techniques to have considerable potential in this regard, in particular transcranial magnetic stimulation (TMS).
TMS is a non-invasive means of stimulating nerve cells in superficial areas of the brain, involving the repeated application of a strong but highly localized magnetic field to a small cortical area. 17 This magnetic field is able to produce depolarization of neurons in the area stimulated, thus causing neurons to fire. The repeated firing of a group of neurons will alter the activity of the local brain region as well as altering the strength of connections between this local region and more widespread brain regions to which these neurons project. 17 TMS may be repeated many times per second, which is referred to as repetitive TMS (rTMS). When applied over repeated sessions, rTMS has been shown to result in significant structural and functional changes throughout neural networks. 18,19 Specifically, rTMS has been shown to increase the physical integrity of white matter tracts throughout the brain; that is, improved structural connectivity (as measured using diffusion tensor imaging [DTI]) 20 to increase brain volumes (assessed with magnetic resonance imaging [MRI]), 21 and to improve the efficiency of communication throughout cortical networks; that is, improved functional connectivity (using electroencephalography [EEG] and functional MRI [fMRI]). 22,23 The ability of rTMS to alter cortical-cortical and cortical-subcortical connectivity makes it an ideal approach for the treatment of post-TBI depression, as well as potentially improving cognitive function in this group.
rTMS has been widely investigated as an alternative treatment for non TBI-related treatment resistant depression (TRD) in studies conducted over at least 20 years. 24 It has been shown, in a series of positive meta-analyses, to be an effective treatment for patients with major depressive disorder. 25 There is also evidence that rTMS is able to improve cognition, independent of its effect on mood. 26 However, a history of TBI has traditionally been considered an exclusion criterion for rTMS trials. This specifically related to the increased risk of seizure after a TBI and the fact that a number of seizures were induced by rTMS prior to the introduction of safety guidelines in 1998. 27 Since 1998, there has been a progressive increase in the number of rTMS trials conducted, with minimal seizures reported when stimulation is provided within these guidelines. Indeed, in our own clinical trials conducted over the last 15 years, there have been no treatment-related serious adverse events, including seizures. 24 In light of the need of effective treatments for the psychiatric and cognitive sequelae of TBI, the potential for rTMS to provide a pathophysiologically based approach, and the rTMS safety data that have accrued since 1998, there is now considerable impetus for conducting a pilot trial of rTMS for post-TBI depression, which investigates the safety and efficacy of this technique.
Therefore, the aim of the current study was to, for the first time, investigate the safety and efficacy of rTMS in the treatment of major depression post-TBI in a randomized double- blind placebo-controlled clinical trial. We utilized a sequential bilateral rTMS protocol, as the trial was developed during a period when we had demonstrated that sequential bilateral rTMS resulted in superior response rates compared with the more standard high-frequency left-sided rTMS for depression. 28 Since that time, a number of studies have failed to confirm these results, showing no advantage of sequential bilateral rTMS over standard approaches. 29,30 A secondary aim was to assess the possible effectiveness of rTMS for improving cognitive functioning post-TBI.
Methods
Trial protocol
This was a randomized double-blind placebo-controlled trial, with patients randomized to receive either active or sham rTMS. Although treaters were aware of the patient's treatment group allocation, they were in no way involved in any of the patient's clinical or cognitive assessments. Therefore both raters and patients were blind to group. Randomization occurred via the generation of a random number sequence, and individual patients were randomized following their baseline assessment and prior to their first treatment session. Patients underwent MRI scans to ensure that there were no contraindications to receiving TMS (detailed subsequently) and to allow neuronavigational localization of treatment sites. A total of 20 treatments were provided over a 4 week period (daily Monday–Friday). Clinical assessments were conducted at baseline, following 2 weeks of treatment and at the completion of the treatment course. Cognitive assessments were conducted at baseline and at the end of the 4 week treatment course only.
The trial was approved by the ethics committees of the Alfred Hospital and Monash University and informed written consent was obtained from all patients. The trial was prospectively registered with
Participants
We recruited a total of 21 patients with a current episode of major depression, according to Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria, subsequent to a closed TBI. Patients were recruited through a number of avenues, including direct referrals from general practitioners and neurologists as well as self-referrals. In addition, as part of the screening process for our TMS and depression trials, we routinely asked about a history of brain injury, and a number of participants for the trial were identified through this process. Participants were required to have experienced a closed head injury resulting in a disruption to consciousness preceding their depression. The injury must not have involved specific direct damage to either frontal lobe. Severity of TBI was measured using a combination of participants' duration of loss of consciousness, duration of post- traumatic amnesia, and/or Glasgow Coma Scale. Following referral to the trial, participants were required to complete a consent to release information form, which allowed the study staff to obtain medical records to confirm the brain injury diagnosis and severity. Out of the 21 participants, we were able to obtain confirmation of diagnosis in this manner for 15. For the remaining six participants, we relied on self-report. For all except one participant we had information (via medical records [n = 15] or self-report [n = 5])] on duration of loss of consciousness, duration of post-traumatic amnesia, and/or Glasgow Coma Scale to allow for severity classification.
The diagnosis of depression was made by the study psychiatrist and confirmed using the Mini-International Neuropsychiatric Interview (M.I.N.I.) 31 There were 11 female and 10 male patients between the ages of 25 and 78 years (mean = 46.29 ± 12.65). Patients needed to be experiencing a depressive episode of at least moderate severity (as defined by a score of >20 on the Montgomery Asberg Depression Rating Scale [MADRS]). Patients were required to be at least 6 weeks post-TBI and have no structural damage to either frontal lobe (as confirmed using pre-trial MRI scans) in order to enter the trial. Finally, it was required that patients not initiate a new antidepressant or psychotherapy in the 4 weeks prior to enrolment and throughout the duration of the trial. In addition, if they were taking antidepressant medication, they were required to not change the dose, again for 4 weeks prior to entry into the trial and for its duration. Patients were excluded if they had an unstable medical condition, neurological disorder, or any history of a seizure disorder, or if they were currently pregnant or lactating.
TMS treatment
rTMS treatment was provided using a MagVenture Magpro30 stimulator (MagVenture A/S Denmark) with a 70 mm figure of 8 coil. Stimulation was provided bilaterally to the left and right dorsolateral prefrontal cortex (DLPFC). Treatment stimulation intensity was determined relative to the patient's resting motor threshold (RMT), which was obtained bilaterally with standard methods. 32 Site of stimulation was individually determined using neuronavigation. All patients underwent a three-dimensional (3D) sagittally oriented T1-weighted structural scan (128 slices) on the Alfred Hospital's GE 1.5T MRI scanner. Patients then underwent a neuronavigational targeting procedure, which has been previously described in detail. 33 This allowed location of the scalp positions that corresponded to the two treatment sites, namely the left DLPFC (Talairach coordinates: -45, 45, 35) and the right DLPFC (Talairach coordinates: 45, 45, 35). The treatment coil was positioned at the individually defined treatment site with the handle pointing back and away from the midline at a 45 degree angle, and tangential to the scalp.
Treatment was provided in a sequential manner to the right DLPFC and then to left DLPFC in all patients. For right-sided treatment, a single train of 1 Hz stimulation was provided at 110% RMT (900 pulses). Left-sided treatment was then applied, consisting of 30 × 5 sec trains of 10 Hz stimulation with 25 sec train intervals, again at 110% RMT (1500 pulses). One participant in the active group received left-sided treatment only, because of the nature of their brain injury. Sham stimulation was applied using identical treatment parameters, but with the coil angled at 45 degrees off the head.
Safety and tolerability
The presence, nature, and frequency of TMS-related side effects were assessed via a structured interview at the completion of the 4 week treatment course.
Efficacy: Clinical and cognitive measures
The primary efficacy outcome variable was MADRS score during the double-blind phase of the trial. With respect to depression symptomatology, patients were also assessed with the Inventory of Depressive Symptomatology – Clinician-Rated version (IDS-CR) and Self-Rated version (IDS-SR). Clinical assessments were conducted at baseline, week 2, and week 4 (end of treatment).
We also assessed cognition, as a secondary outcome variable, to determine whether rTMS treatment resulted in cognitive improvement. Cognitive assessment covered the following domains: attention and concentration, working memory, speed of information processing, verbal and visual memory, and executive functioning. Specifically, we report on the performances at baseline and the end of 4 weeks of treatment on the following tests: Digit Span, Trail Making Test, Arithmetic, Rey Verbal Auditory Learning Test, Brief Visual Spatial Memory Test, Verbal Fluency, and Stroop.
Statistical analysis
To investigate demographic and clinical baseline differences between the groups, t tests and χ 2 tests were used. Safety, tolerability, and blinding data were also assessed using χ 2 . Linear mixed model analyses were then calculated for the dependent measures (MADRS, IDS-CR, IDS-SR, QLESFQ [Quality of Life Enjoyment and Satisfaction Questionnaire], SDS [Sheehan Disability Scale]) with fixed effects of group and time. An autoregressive first order (AR[1]) covariance structure was determined to provide an appropriate fit for the data, and restricted maximum likelihood (REML) was used to estimate parameters. Post-hoc pairwise comparisons between groups at each time point and within groups comparing time points were calculated for the MADRS data with Bonferroni correction. We also compared the number of people meeting response criteria (defined as at least a 50% reduction in MADRS score from baseline to end of treatment course) across groups using χ 2 .
We also conducted analyses on the cognitive data, and it is important to note that these analyses were conducted in the context of a secondary exploratory aim. Performance on the range of cognitive tests was assessed in two ways. First, change scores from baseline to end of treatment were calculated and differences in change scores between the two treatment groups werwe assessed with independent samples t tests. Change scores were calculated using the following formula to account for baseline performance, [(post-pre)/pre] × 100. Second, paired t tests were used to investigate changes in cognitive performance within each group with treatment. For these analyses, results were only considered significant if the p value was <0.01, and p values of <0.05 were considered trends.
Finally, as there were only limited data from the unblinded maintenance phase, this is presented descriptively.
All statistical analysis was conducted using SPSS 20.0 (SPSS for Windows), and all procedures were two tailed with significance set at an α level of 0.05 unless otherwise specified.
Results
Participants
Of the 21 patients consented, 3 withdrew during the initial 4 week double-blind phase of the trial (1 active, 2 sham), and all had undergone at least a 2 week MADRS prior to withdrawing. All patients were included in an intention-to-treat analysis. Neither patients nor assessors were able to guess the allocated treatment groups at a rate greater than that expected by chance (patients: p = 0.351; assessors: p = 0.341).
Baseline clinical and demographic characteristics are summarized in Table 1. The groups were not significantly different on the majority of these variables. There were significantly more patients taking antidepressant medication active group than in the sham group (p = 0.03), and the active group was trending toward having a significantly lower mean age than the sham group (p = 0.05). In addition, there were no significant differences in any cognitive measures between the groups at baseline (p > 0.05).
Clinical and Demographic Characteristics
Significant; **Large effect size.
TBI, traumatic brain injury; MADRS, Montgomery Asberg Depression Rating Scale; IDS-CR, Depressive Symptomatology – Clinician-Rated version; IDS-SR, Depressive Symptomatology – Self-rated version; GAD, generalized anxiety disorder; OCD, obsessive-compulsive disorder; PTSD, post-traumatic stress disorder.
Safety and tolerability
There was a higher proportion of patients reporting the presence of side effects during the treatment course in the active (72%) than in the sham (30%) group; however, this was not statistically significant (p = 0.146). There was no difference with respect to the nature of side effects (i.e., site discomfort, mild headache, severe headache, both headache and site discomfort, not applicable) between the two groups (p = 0.343). Nor was there a difference in frequency of reported side effects (i.e., once, some treatments, all treatments, not applicable) between the two groups (p = 0.410). There were no serious adverse events in either treatment group.
Clinical outcomes
There was a significant overall reduction in MADRS ratings (effect of time, F (2,35.9) = 7.210, p = 0.002), with no difference in response between the active and sham groups (see Fig. 1). There was also no difference in the mean reduction in MADRS scores between the groups (active = -20.75% ± 34.33; sham = -27.30% ± 30.20, p = 0.65, d = 0.21)
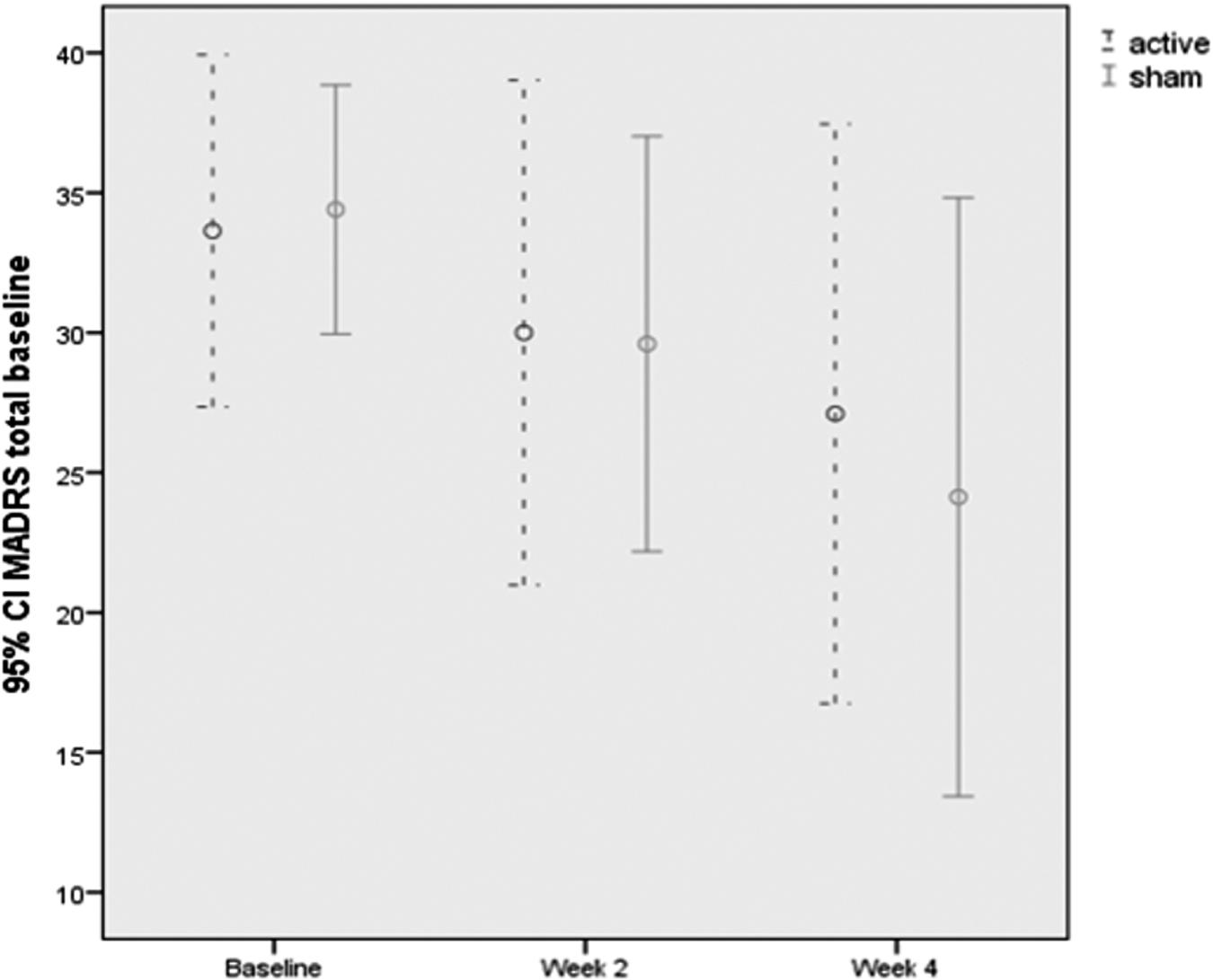
Montgomery Asberg Depression Rating Scale (MADRS) scores over time as a function of treatment group.
This pattern of response was also seen in IDS-CR (F (2,36.3) = 7.773, p = 0.002) and the IDS-SR (F (2,19.9) = 9.126, p = 0.002) (see Table 2). There was also no difference in the response rate between the groups (3 for active, 4 for sham, p > 0.05). Finally, there was no relationship between response and any of the demographic baseline variables.
Means and Standard Deviations for Madrs and IDS (CR and SR) at Baseline and End of Treatment
MADRS, Montgomery Asberg Depression Rating Scale; IDS-CR, Depressive Symptomatology – Clinician-Rated version; IDS-SR, Depressive Symptomatology – Self-rated version.
Cognitive outcomes
A trend toward improved performance in the active compared with the sham group over time was seen for Digit Span Backwards (t (16) = 2.44, p = 0.027). For the within-treatment group analysis, a trends toward improved cognitive performances was seen in the active group over time on Arithmetic (t (8) = 2.87, p = 0.021), and the Trail Making Test B (t (9) = 2.66, p = 0.029). In the sham group there was a significant decrease in Digit Span Backwards (t (8) = 3.41, p = 0.009) over time, and no improved performances (Table 3).
Cognitive Outcome Data from Baseline to End of Treatment as a Function of Treatment Group
RVALT, Rey Verbal Auditory Learning Test; BVMT, Brief Visuospatial Memory Test.
Discussion
This was the first ever randomized clinical trial of the use of rTMS in the treatment of post-TBI depression. We showed that the provision of a treatment course of rTMS in patients who have experienced a TBI is both safe and tolerable. Although the active group showed a non-significant higher percentage of side effects than sham (i.e., 72% vs. 30%) this is not unexpected in light of the nature of TMS and the method of sham we employed. Most importantly, there were no serious adverse events reported. We did not find a significant effect of sequential bilateral rTMS on depression however, with all patients showing a significant improvement in depression symptoms over time irrespective of whether they received active or sham stimulation. This pattern of results was also seen in the functional outcomes for patients, as measured by the SDS. There were some significant findings with respect to the within-group analyses of cognition, with patients in the active group showing significant improvement over time in tasks that load on working memory and executive function (Wechsler Adult Intelligence Scale [WAIS] – Arithmetic and Trail Making Test-B), compared with no change in patients who received sham stimulation. The between-group analyses showed a significant difference in Digit Span Backwards, another working memory assessment; however, this was largely driven by a decrease in performance in the sham group.
The current trial's finding that a course of rTMS is safe and tolerable for patients who have experienced a TBI is significant, as it provides a framework for future research. In addition to the standard rTMS contraindications, we only included patients who were at least 6 weeks post-injury and who, on scanning, showed no structural damage to the intended stimulation site. It is therefore recommended that any future research in patients with TBI also include these criteria.
There are a number of limitations of the current trial that need to be taken into account when considering the lack of a significant antidepressant effect in this population with rTMS. First, we utilized sequential bilateral rTMS rather than the more standard depression protocol of left-sided high frequency rTMS. As mentioned in the Introduction, at the time of the trial design there was evidence that the bilateral approach may be more effective; however, this contention was not borne out by subsequent research. In addition, the stimulation dose in the current study (namely 900 pulses right side, 1500 pulses left side) was considerably less than what is considered optimal for antidepressant effect, particularly with respect to left-sided stimulation, in which now more than double the number of pulses per treatment is commonly used. 34 Also, as this was a pilot trial, the sample size was relatively small and the trial may have been underpowered to detect differences in what is a complex and heterogeneous population. In addition, the differences seen in cognitive performances were part of a secondary analysis that cannot fully account for practice effects because of the lack of a mixed model design. Although we were able to obtain medical records confirming brain injury diagnosis and severity for 15 of the 21 participants, we had to rely on self-report for the remaining 6. Although all six gave detailed information, lack of confirmation is a limitation. Finally, there is a possibility that the higher age in the sham group, although not significant, may have impacted the response to stimulation.
That we found some improvements in cognition following active treatment, in light of the limitations mentioned, is encouraging. Cognitive impairment is common following TBI and is strongly associated with the degree of functional outcome following injury, impacting many areas including employment, education, and social participation. 35 To date, treatment approaches for TBI-related cognitive impairment have shown only small to moderate benefits, and so novel approaches are needed. 11 Brain stimulation techniques, including TMS, are increasingly being investigated for their utility in improving cognition, with working memory seemingly particularly amenable to enhancement. 26,36 Therefore, the cognitive findings in the current trial provide a strong preliminary indication that future research should be conducted, which directly investigates the potential of TMS as a treatment for cognitive impairment following TBI.
The current study shows that providing a course of rTMS in people who have had a TBI can be conducted safely and is well tolerated. This is an important outcome, as it allows for continued research in the area, including the investigation of unilateral rTMS approaches, which may be more efficacious for treating depression, and to further investigate the potential for rTMS to improve cognition in this population.
Footnotes
Acknowledgements
K.E.H. is supported by a National Health and Medical Research Council (NHMRC) Fellowship. P.B.F. is supported by an NHMRC Practitioner Fellowship. Funding for this study was provided by Victorian Neurotrauma Initiative (VNI).
Author Disclosure Statement
P.B.F. has received equipment for research from Magventure A/S and Brainsway Ltd. For the remaining authors, no conflicts of interest were declared.