
Abstract
Chronic verbal retrieval deficits have been noted in traumatic brain injury (TBI), but no U.S. Food and Drug Administration–approved interventions are available. The present study investigated whether 10 sessions of 20 min of 1 mA anodal high-definition transcranial direct current stimulation (HD-tDCS) targeting pre-supplementary motor area/dorsal anterior cingulate cortex (preSMA/dACC) compared with sham HD-tDCS would improve verbal retrieval deficits in TBI patients. Improvements in verbal retrieval processes were observed up to 8 weeks post-treatment. Thus, potential dysfunction to verbal retrieval circuitry in TBI appears amenable to remediation through electromodulation with HD tDCS to the preSMA/dACC. Although further studies clarifying mechanisms by which tDCS brought about these improvements will likely inform refinements in the application of this therapeutic technique, the findings suggest the efficacy of using HD-tDCS to target other systems vulnerable to TBI to improve functioning.
Introduction
Traumatic brain injury (TBI), even mild TBI, can lead to long-term deficits in a variety of memory and other cognitive functions. 1 –3 At present, pharmacological interventions (i.e., acetylcholinesterase inhibitors, amantadine, cyclosporine A, erythropoietin, growth hormone, stimulants/pre-stimulants, and dopamine agonists) currently used are off-label uses, with no medications having received U.S. Food and Drug Administration approval for cognitive dysfunction in TBI. 4 However, evidence suggests transcranial direct current stimulation (tDCS) has the potential to improve TBI-related cognitive deficits. 5 The present phase II (Class III) clinical trial examines the efficacy of high definition-tDCS (HD-tDCS), allowing more focal delivery of current 6 targeting dorsal medial frontal cortex, particularly, pre-supplementary motor area/dorsal anterior cingulate cortex (preSMA/dACC), as a therapeutic for verbal retrieval deficits in TBI.
Studies using two electrode preparations of tDCS have shown the potential to modulate systems involved in verbal retrieval. Left frontotemporal cathodal tDCS (vs. anodal and sham) for 10 min improved verbal retrieval in object naming in nonfluent aphasia. 7,8 Anodal (vs. cathodal and sham) 8 and 10 min of 2 mA tDCS to left dorsolateral prefrontal cortex (DLPFC) in healthy young adults improved verbal retrieval in object/action naming. 9 Anodal tDCS (vs. cathodal and sham) for 30 min to left PFC in healthy adults also increased retrieval clustering from within semantic networks in category fluency. 10 Additionally, in healthy older adults, anodal 2 mA tDCS to left DLPFC (compared with sham) improved retrieval in object naming while undergoing stimulation, although not immediately after 10 min of passive stimulation. 11
The present study investigated using HD-tDCS targeted to preSMA/dACC in improve verbal semantic retrieval deficits in chronic TBI. Compared with older two electrode preparations, HD-tDCS allows for more focal delivery of electrical current to specific brain regions via arrays of electrodes, including, better targeting of preSMA and dACC. 12 PreSMA has been shown to be involved in a range of verbal semantic retrieval tasks, including, category fluency, 13,14 abstract versus concrete word judgments, 15 lexical decisions, 16 semantic priming, 17 and semantic retrieval. 18 –21 Additionally, the integrity of white matter tracts connecting preSMA other brain regions have been shown to be compromised in mild to severe TBI. 22
A network including preSMA, caudate, and thalamus has been proposed to mediate verbal retrieval processes. 20 In the network, preSMA-thalamic-caudate interactions mediate verbal memory functions, indexed by theta and beta electroencephalography (EEG) frequency synchronizing rhythms, including, retrieval in verbal fluency, retrieval in verbal episodic memory, and semantic categorization tasks. More specifically, preSMA has been imputed to initiate interactions between multiple brain regions involved in semantic processing and memory. Thus, in present study, military veterans with chronic TBI and verbal retrieval deficits received 10 sessions of 20 min of sham or 1 mA HD-tDCS targeted to preSMA/dACC and change in verbal retrieval and other relevant cognitive abilities were assessed in immediate and 8-week follow-up sessions.
Method
Participants
The study was a prospective, single-blinded study. Patients were veterans from Operations Enduring Freedom, Iraqi Freedom, and New Dawn who were referred for treatment for cognitive dysfunction secondary to TBI (Fig. 1). Written informed consent was obtained, and the study was conducted in accordance with the ethical standards of the Helsinki declaration (1964) and approved by the Institutional Review Board of the University of Texas at Dallas.
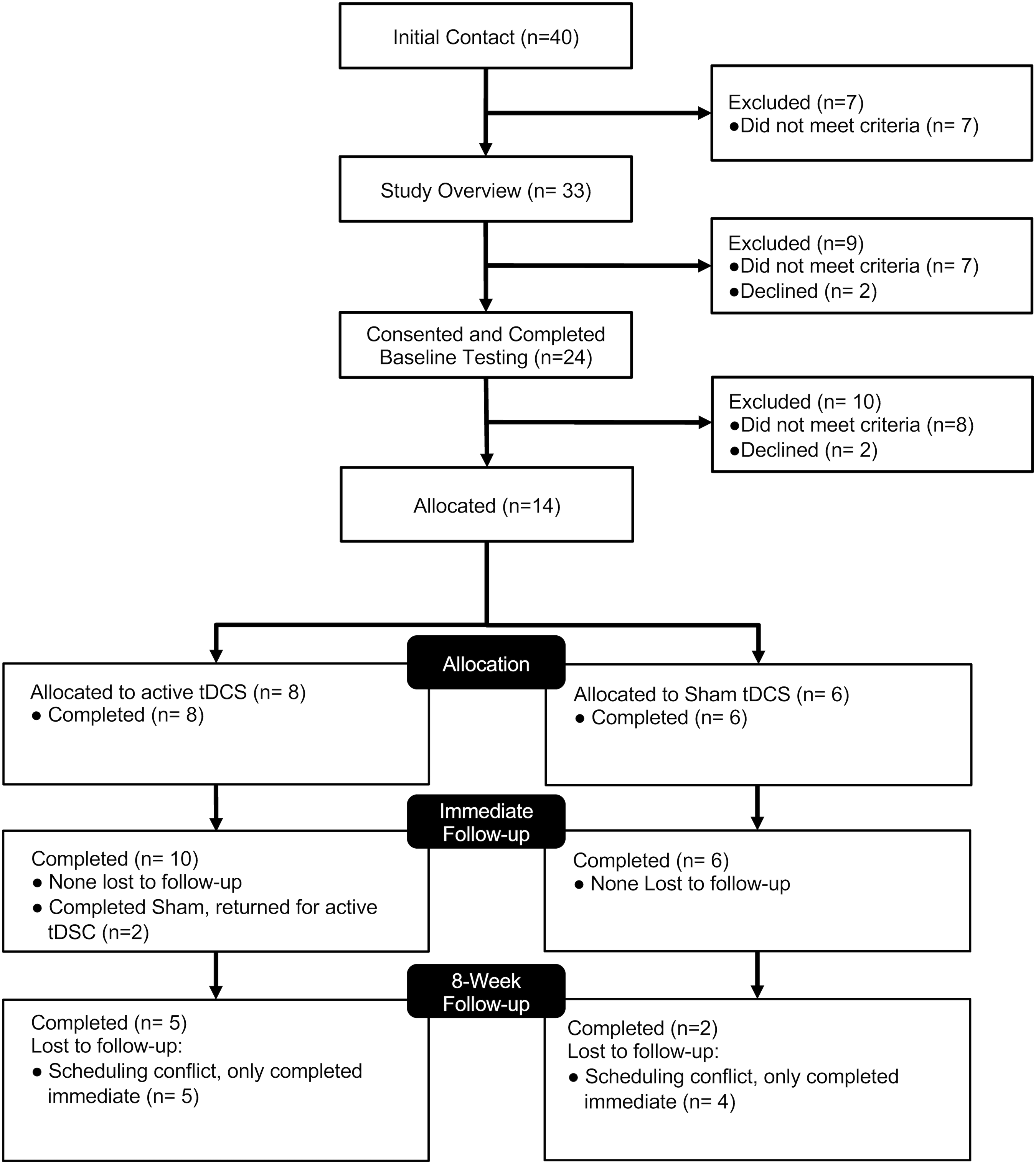
Patient flow diagram. Illustrates patient flow through the study from initial contact to allocation and follow-up.
Referred patients with subjective verbal retrieval complaints were administered measures of verbal retrieval. Patients with verbal retrieval complaints and a neuropsychological test score on at least one verbal retrieval assessment (phonemic fluency, category fluency, naming, verbal list learning) of a T-score less than 40 or that was greater than 1.0 standard deviation (SD) below the average score on their other verbal retrieval assessments were considered eligible for the study.
Eight patients (n = 1 female, Caucasian, non-Hispanic, and right-handed; n = 7 male, all Caucasian, n = 1 Hispanic, n = 7 right-handed and n = 1 left-handed) were assigned to the active condition (mean [M] = 40.9, standard deviation [SD] = 5.0 years of age; M = 14.7, SD = 2.2 years of education). Six (all male, Caucasian, non-Hispanic, and right-handed) were assigned to the sham condition (M = 40.8, SD = 10.9 years of age; M = 14.3, SD = 1.7 years of education). There were no significant differences in age [t(12) < 1.00] or education [t(12) < 1.00] between groups. Two patients who completed the sham protocol returned and completed the active protocol (following sham treatment, one began active treatment 1 week after the 8-week follow-up and one 4 weeks after the immediate follow-up for the sham treatment), and their immediate follow-up assessment data after completing the active protocol were acquired.
Retrospective concussion history, using the Ohio State TBI Identification Method 23 (Table 1), did not significantly differ between the groups [t(13) < 1.00; TBIs with loss of consciousness: Active M = 4.1, SD = 3.3 and Sham M = 2.3, SD = 2.5; TBIs with more than 30 min of loss of consciousness: Active M = 0.5, SD = 0.7, and Sham M = 0.8, SD = 0.5]. Additionally, symptoms on the Post-Traumatic Stress Disorder (PTSD) Checklist 24 (Table 1) did not significantly differ between groups [t(13) < 1.00].
Neuropsychological Test Battery Administered to Active and Sham Groups
TBI, traumatic brain injury; B, baseline; PTSD, post-traumatic brain disorder; IF, immediate follow-up; 8F, 8-week follow-up.
Participants were to abstain from alcohol 24 h and not to consume any caffeinated products or nicotine for at least 1 h prior to study sessions. Patients were assigned to one of two groups: active or sham HD tDCS targeting the preSMA/dACC. Both groups completed 10 sessions with 20 min per session over a 2-week period. Immediately following treatment and 8 weeks post-treatment, the neuropsychological battery (using parallel forms when available) was re-administered. All were blinded as to assigned conditions until all follow-up evaluations were completed. The two sham patients who returned to complete the active protocol remained blinded to conditions until their final active follow-up.
Neuropsychological Battery
The Neuropsychological Battery (Table 1) consisted of: 1) verbal retrieval measures—Controlled Oral Word Association Test 25 (COWAT), Category Fluency Test, 25 Boston Naming Test 26 (BNT), Rey Auditory Verbal Learning Test 27 (RAVLT); 2) other cognitive measures—Digit Span Forwards and Backwards, 28 Trail Making Test: A and B, 29 Delis-Kaplan Color Word Interference Test 30 (DKEFS); 3) Beck Depression Inventory-II 31 (BDI); and 4) Beck Anxiety Inventory 32 (BAI).
HD-tDCS
The HD-tDCS montage (Fig. 2) targeting preSMA/dACC consisted of FZ for the central anodal electrode and Fp1, Fp2, F7, and F8 for the return electrodes (i.e., five circular Ag/AgCl electrodes 1 cm radius with conductive gel) selected based on simulations (based on the International 10/20 Electroencephalogram System; and NeuroElectrics NIC2v2.0.10.3;
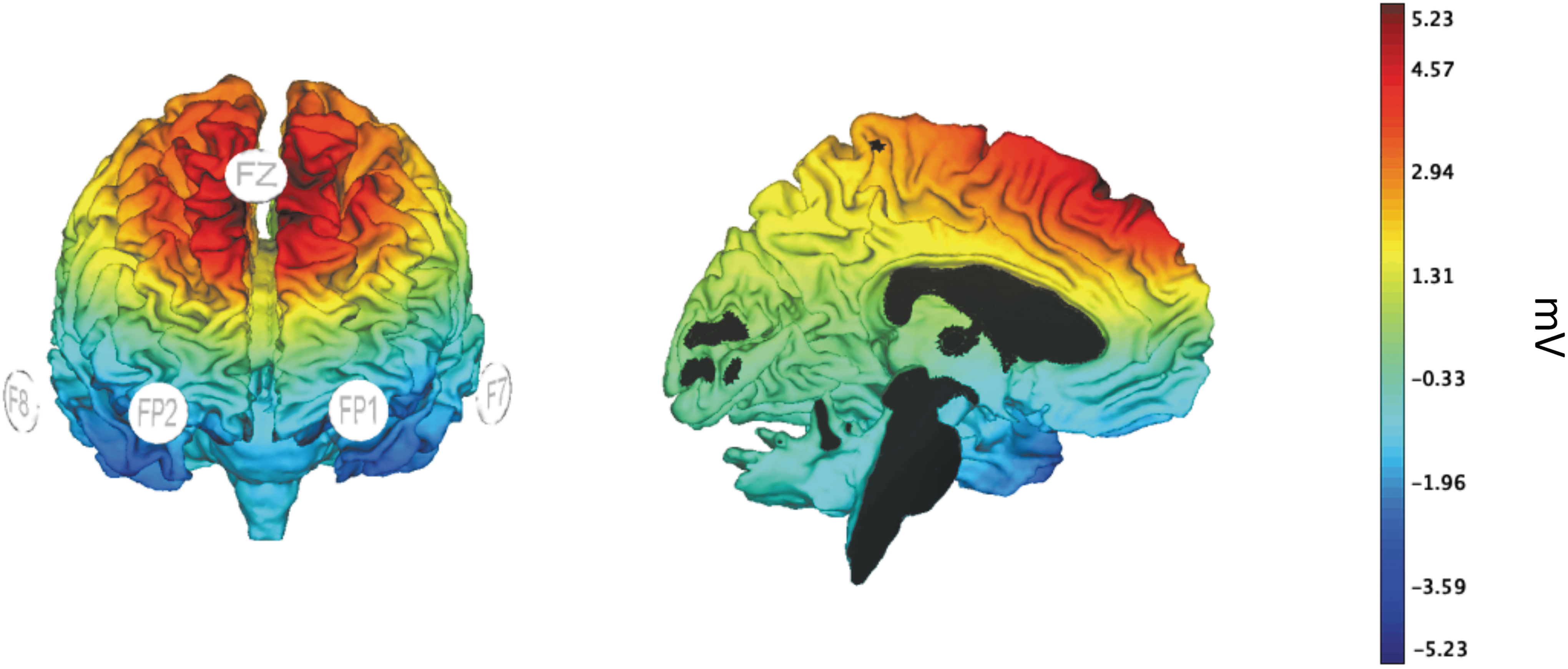
Estimate of current field magnitude. Simulated estimate of the current field magnitude using an electrode montage with Fz as a 1 mA anodal electrode and F8, FP2, FP1, and F7 as return electrodes with return stimulation at 25% each. Estimate obtained from NeuroElectrics NIC2 software (v2.0.10.3;
Statistical analysis
Constrained linear mixed effects modeling tested for mean treatment differences on immediate and 8-week follow-up change from baseline (i.e., yij = μ0 + μij + eij ; where yij = a neuropsychological variable; μ0 = common baseline mean prior to assignment to i = 1,2 treatments [sham, anode-active]; μij = mean change from baseline for treatment i and time point j = 1,2 [immediate follow-up and 8-week follow-up]; and eij = error term having positive correlation within participants across time). Treatment effects were linear contrasts, μ1j - μ2j for each time-point j, testing mean treatment differences between groups at the immediate follow-up session and the 8-week follow-up session, both relative to baseline.
Results
Interaction contrasts at immediate follow-up revealed significant differences between the active and sham HD-tDCS in change in RAVLT total score, DKEFS Inhibition time, and DKEFS Inhibition/Switching time (Table 2). The increase in RAVLT total score and the decreases in DKEFS Inhibition time and Inhibition/Switching time for the active HD-tDCS group significantly differed from the respective RAVLT total score decrease and DKEFS Inhibition time and Inhibition/Switching time increases for the sham group (Fig. 3). Interaction contrasts at the 8 weeks follow-up, revealed a significant difference between the active and sham HD-tDCS in change in category fluency total score (Table 2). The increase in category fluency total score for the active HD-tDCS group significantly differed from the decrease in category fluency total score for the sham group (Fig. 3). There were no other significant changes from pre-treatment baselines on other neuropsychological tests.
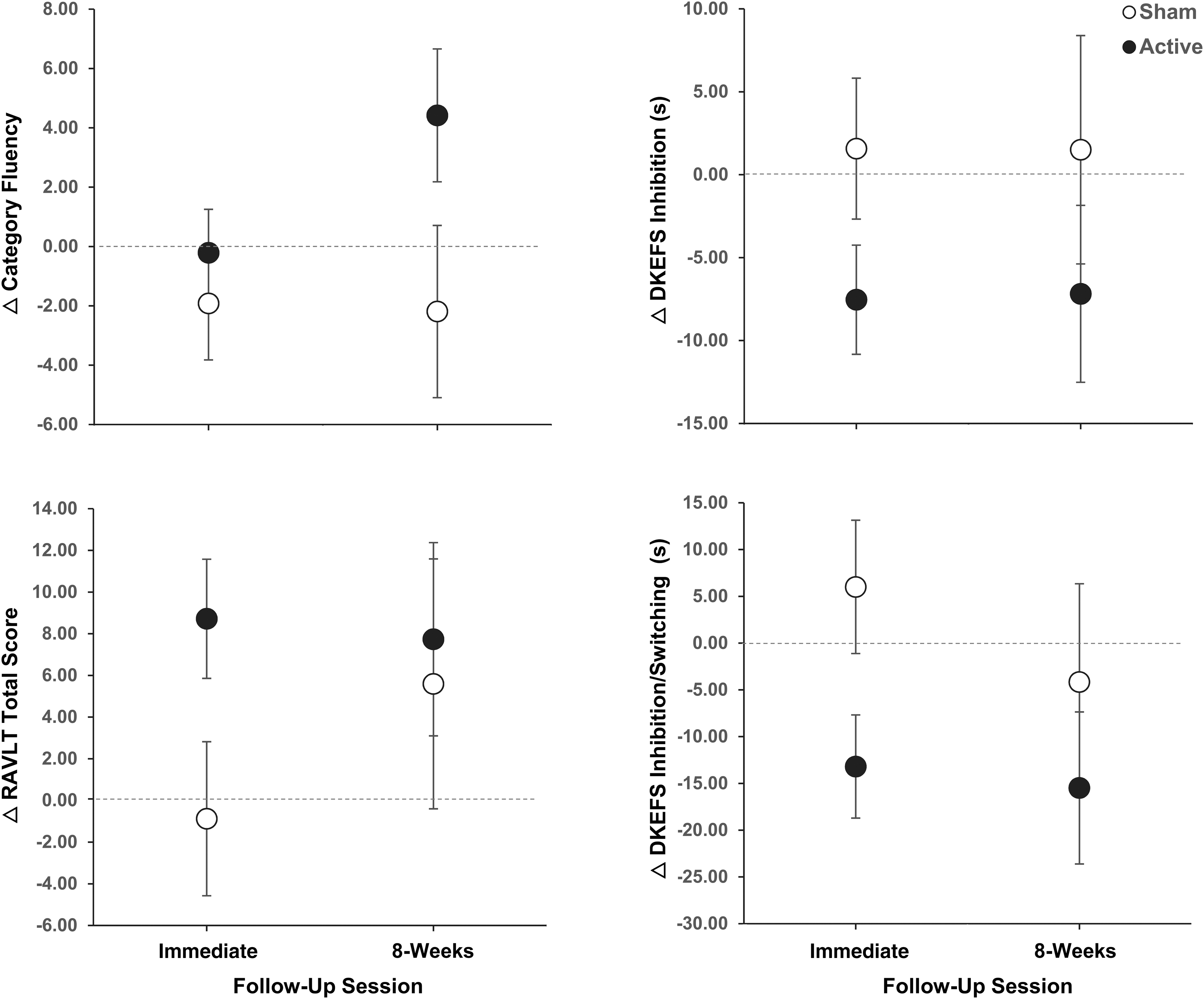
Mean change from baseline in category fluency, Rey Auditory Verbal Learning Test (RAVLT) Total Score, Delis-Kaplan Executive Function System (DKEFS) Inhibition, and DKEFS Inhibition/Switching at Immediate and 8-week follow-up sessions for the active and Sham Groups. Filled circles depict means for the active group, and open circles depict means for the sham group. Bars depict Least Significant Intervals (95% LSI) where non-overlapping bars indicate significant differences.
Active and Sham Group Means and Interaction Contrasts for Neuropsychological Tests per Assessment Session
p < 0.05.
Standard error in parentheses. Satterthwaite Degrees of Freedom in brackets.
B, baseline; IF, immediate follow-up; 8F, 8-week follow-up; COWAT, Controlled Oral Word Association Test; RAVLT, Rey Auditory Verbal Learning Test; s, seconds; DKEFS, Delis-Kaplan Executive Function System; BDI-II, Beck Depression Inventory II; BAI, Beck Anxiety Inventory.
Discussion
Ten sessions of preSMA/dACC targeted HD-tDCS led to improvements in category fluency at eight weeks after the final stimulation session. Improvement in category fluency at the 8-week follow-up shows evidence of efficacy for using HD-tDCS to bring about lasting improvement in this chronic impairment. Meta-analysis has shown deficits in both category and phonemic fluency following mild to severe TBI to be robust chronic deficits, present 10 days to over 2 years post-injury. 33 The preSMA/dACC region was targeted for electromodulation in the present study because of its imputed role in verbal retrieval processes 20,21 and its previously documented vulnerability in TBI. 22 The observed improvement in category fluency following electromodulation further validates involvement of the preSMA in verbal retrieval and provides evidence that traumatic injury to verbal retrieval circuitry, at least in mild-to-moderate TBI, appears amenable to improvement with targeted electromodulation.
HD-tDCS also led to improvement on RAVLT at immediate follow-up. Improvement was observed on RAVLT total score (i.e., summing the number of correctly recalled items over the five learning trials). Previous analysis of the factor structure of different metrics from the RAVLT suggests that total score indexes retrieval ability on a storage dimension rather than an aspect of acquisition. 34 Thus, improvement in RAVLT total score at intermediate follow-up also provides evidence for the use of HD-tDCS to modulate preSMA/dACC circuitry in TBI to improve verbal retrieval. However, the potential modulatory benefit was not maintained to the 8-week follow-up, and further research is needed on parameters affecting longer-term benefits.
PreSMA has been proposed to initiate search processing in verbal retrieval, associated with increased theta-band power in EEG in retrieval tasks. 20 Search initiation then has been proposed to lead to preSMA–thalamo-cortical interactions that modulate access to correct representations and suppress circuits to incorrect representations. Terminating the search by retrieving a memory has been associated with an increase in beta-band power in EEG. PreSMA could coordinate or bind together the activities of multiple cortical regions by driving beta synchronization via projections to the thalamus, as a relay, and then to cortical cells. 35 –37 In healthy participants, anodal tDCS 15 min at 1 mA, cycled in 20-sec intervals, over dorsal-anterior medial cortex been shown to increase midline theta-band power in EEG post-stimulation, 38 and thus anodal tDCS to preSMA could have brought about the retrieval improvements observed in the present study by improving neural functions within the circuit mediating search and retrieval processes.
HD-tDCS also led to improvements in DKEFS inhibition and inhibition/switching at the immediate follow-up session in this study. Both have been previously shown to be impaired in mild to moderate TBI. 1 Additionally, as described above, inhibition processes have been proposed to be part of semantic processing mediated by the preSMA-thalamus-caudate circuit. 20 Additionally, association between preSMA function and inhibition has been observed in tasks assessing cognitive control of motor responses, for example, stop signal 39 and go/no-go 40 tasks, and in healthy participants, both during 10 min of anodal tDCS to preSMA and following stimulation, inhibitory control has been shown to improve on a stop-signal task. 41 However, in the present study, as with the findings with RAVLT, the modulatory benefit to inhibition and switching was not maintained to the 8-week follow-up, and further research in needed on parameters affecting longer-term benefits.
Although HD-tDCS was not shown to improve performance on BNT in the present study, accuracy in object naming among the participants studied was near ceiling at baseline, providing minimal opportunity for improvement. Additionally, findings on the effects of tDCS interventions on object naming have been mixed. Left frontotemporal cathodal tDCS (vs. anodal and sham) for 10 min has been shown to improve object naming in nonfluent aphasia, 5 but a meta-analysis failed to find a general effect of tDCS on object naming in aphasia. 8 Anodal (vs. cathodal and sham) 2 mA tDCS to left DLPFC for 8 and 10 min in healthy young adults has been shown to lead to faster object/action naming, 8,42 and in healthy older adults, anodal 2 mA tDCS to left DLPFC (compared with sham) has led to faster object naming while undergoing stimulation but not immediately after 10 min of stimulation. 43 However, meta-analysis of single application tDCS effects on object naming and word reading in healthy participants also failed to show significant benefit overall, but secondary analyses did reveal evidence for anodal tDCS to right DLPFC leading to faster naming and reading in healthy participants. 44 Thus, future research on the effects of HD-tDCS on various aspects of verbal retrieval deficits in TBI might examine speed of object naming as an outcome measure, rather than accuracy.
Although the present findings provide evidence of efficacy for using HD-tDCS targeted to preSMA/dACC to improve verbal retrieval in chronic TBI, reviews have suggested that various tDCS preparation and treatment parameters can influence outcomes in the treatment of TBI-based cognitive deficits. 45,46 Meta-analyses have shown stronger tDCS effects on cognitive processes when tDCS was administered while patients were performing the diagnostic cognitive task compared with stronger effects observed after stimulation administration in healthy participants. 47,48 Additionally, in chronic TBI patients, anodal tDCS (compared with sham) to left dorsolateral PFC applied over 10 days has been shown to reduce theta power on EEG after the first session and to decrease delta and increase alpha after the last tDCS session. This decreased delta and increased alpha after the final session also were associated with improvements in attention, visual memory, and executive functions. 5 Yet, in severe TBI, 10 min/day over 15 days of anodal tDCS to left dorsolateral PFC failed to improve memory and attention. 49 Individual differences in multi-session effects of tDCS to left dorsolateral PFC in healthy participants also have been observed in working memory. 50 Thus, further studies are needed to understand individual differences in physiological responses to particular electromodulation intervention parameters and the effects of treatment parameters on outcomes to optimize treatments.
Although the mechanisms by which tDCS modulates neural activity have yet to be fully specified, research has revealed a cascade of effects, including enduring synaptic and non-synaptic effects, at neuronal and neural network levels. 51 –53 Applications of tDCS in humans have been suggested to be too weak to induce action potentials in neurons, the polarization of specific compartments of neurons varies with the orientation of the compartment to current flow, and compartments can polarize in opposite directions (e.g., pyramidal neuron apical dendrites and somas). 54 Yet, anodal tDCS has been shown to have a depolarizing effect on neural systems that lowers activation thresholds, for example, with 13 min of anodal tDCS to motor cortex leading to increased excitability (cathodal tDCS decreased excitability), indexed by motor evoked potential, up to 30 min following administration. 55
Additionally, as noted above, anodal tDCS has been shown to induce different system level changes over the course of 10 days of administration (i.e., reduced theta power on EEG after the first session and decreased delta and increase alpha after the last tDCS session). 5 Further, stimulation of a target cortical site also has been shown to induce change in subcortical regions within the neural network of the targeted cortical site. 56 Neural membrane polarization via tDCS has been proposed to amplify intrinsic or induced neural dynamics within a targeted region causing secondary cascades leading to spike-timing dependent plasticity. 51,52,57 In chronic TBI, HD-tDCS targeted to preSMA/ACC might induce plasticity at preSMA/ACC or within other regions of the verbal retrieval circuit, possibly affecting dopamine pathways putatively involved in verbal retrieval and executive functions, including, inhibition and switching. 58
This is the first study to investigate HD-tDCS effects on preSMA/dACC for chronic verbal retrieval deficits in patients with TBI. 20 The improvement in verbal retrieval processes persisted for at least 8 weeks post-treatment. Improvement also was observed initially in inhibition and inhibition/switching, previously shown to be impaired in mild to moderate TBI 1 and imputed to be part of semantic processing mediated by the preSMA-thalamus-caudate circuit. 20 Of course, appropriate cautions should be applied when considering results from any one study and, particularly, one study based on a relatively small sample with multiple outcome measures under study. The present findings from this initial trial, however, provide validation for the involvement of preSMA in verbal retrieval processes. Additionally, whatever the damage to the verbal retrieval circuit that is caused by TBI, the damage appears to be amenable to remediation with electromodulation with HD tDCS to the preSMA. Although HD-tDCS was tolerated well with no significant adverse events, further exploration of treatment parameters is warranted, particularly, with respect to increasing long-term effects. Although no training was prescribed in the present study, tDCS effects on cognitive processes in patients have been shown to be stronger when tDCS was administered while patients were performing the diagnostic cognitive task compared with after passive stimulation administration. 47,48 Thus, stimulation coupled verbal memory training, prescribed practice, participant-directed practice, or even conversation might improve effects targeting the verbal memory system.
Footnotes
Acknowledgments
The authors wish to thank the Veterans who participated in the study, and they also wish to thank the Boot Campaign for financial support and for referring participants to the study.
The views expressed here do not necessarily reflect those of the United States Department of Energy or the United States government.
Funding Information
Partial study funding was provided by the Boot Campaign (Assessment and Treatment of Veterans with TBI and/or PTSD, Boot Campaign; $339,963, 9/29/2016-no end date) and awarded to J. Hart, Jr. at 10% effort. Morgan Lutrell served as a Director of Development, in August of 2016, for the ReBOOT initiative for the non-profit (501c3) Boot Campaign and as interim CEO for the Boot Campaign, in January of 2017. However, he did not receive remuneration for his services in either of these roles. He was involved in the design and conceptualization or the study prior to taking on these roles, and his contributions to revisions of the manuscript came after his resignation from the Boot Campaign and after the completion of data collection for the study in 2018.
Author Disclosure Statement
No competing financial interests exist.