
Abstract
Neurofilament light (NF-L) might have diagnostic and prognostic potential as a blood biomarker for mild traumatic brain injury (mTBI). However, elevated NF-L is associated with several neurological disorders associated with older age, which could confound its usefulness as a traumatic brain injury biomarker. We examined whether NF-L is elevated differentially following uncomplicated mTBI in older adults with pre-injury neurological disorders. In a case–control study, a sample of 118 adults (mean age = 62.3 years, standard deviation [SD] = 22.5, range = 18–100; 52.5% women) presenting to the emergency department (ED) with an uncomplicated mTBI were enrolled. All participants underwent head computed tomography in the ED and showed no macroscopic evidence of injury. The mean time between injury and blood sampling was 8.3 h (median [Md] = 3.5; SD = 13.5; interquartile range [IQR] = 1.9–6.0, range = 0.8–67.4, and 90% collected within 19 h). A sample of 40 orthopedically-injured trauma control subjects recruited from a second ED also were examined. Serum NF-L levels were measured and analyzed using Human Neurology 4-Plex A assay on a HD-1 Single Molecule Array (Simoa) instrument. A high correlation was found between age and NF-L levels in the total mTBI sample (r = 0.80), within the subgroups without pre-injury neurological diseases (r = 0.76) and with pre-injury neurological diseases (r = 0.68), and in the trauma control subjects (r = 0.76). Those with mTBIs and pre-injury neurological conditions had higher NF-L levels than those with no pre-injury neurological conditions (p < 0.001, Cohen's d = 1.01). Older age and pre-injury neurological diseases are associated with elevated serum NF-L levels in patients with head trauma and in orthopedically-injured control subjects.
Introduction
Axonal damage is a pathological characteristic of traumatic brain injury (TBI), and it has been found to play a role in neuropsychological outcome. 1 Neurofilaments are intermediate filaments (thread-like structures) 2 that are involved in the growth and structure of axons. 3 Neurofilament light (NF-L) is the smallest subunit of the neurofilament heteropolymer (a macromolecule composed of several bonded monomer subunits). 4 Together with the neurofilament medium and heavy subunits, NF-L is believed to facilitate scaffolding of the neural cytoskeleton—providing structural support for the axon and regulating axon diameter. 4,5 NF-L plays a role in the structure of neurofilaments, assembly of the neurofilament heteropolymer, and formation of a stable stationary neurofilament network. 5 NF-L also is involved in the transport of neurofilaments through the axon 6 and axonal and dendritic branching and growth, 3 and is abundant in long subcortical white matter axons. 7 Proteolytic (i.e., enzyme breakdown) processes that occur during axonal degeneration lead to incomplete neurofilament degradation. 8 Therefore, following axonal damage 8 or neuronal degeneration, 9 neurofilaments are released and are present in both the cerebrospinal fluid and the bloodstream. 10,11
There is steadily growing interest in examining NF-L following neurotrauma. NF-L levels have been found to increase in both cerebrospinal fluid (CSF) and blood during the first week(s) following TBI. 12,13 They are elevated in those with traumatic structural abnormalities visible on computed tomography (CT), 14 highly elevated following severe TBI and diffuse axonal injury, 15 and are associated with outcome in patients with severe TBIs. 12,13 NF-L is also elevated following mild neurotrauma, such as sport-related concussion. 16 Interestingly, in one study, NF-L was reported to increase in American football players, over the course of a season, who had not experienced a symptomatic concussion. 17
There has been a clarion call for more research focusing on TBI in older adults. 18 In Western countries, overall hospital admission rates for TBIs are decreasing, while admissions are increasing in patients older than 65 years. 19 –21 Falls are a common cause of emergency department (ED) visits 22,23 and TBI 24 –26 in older adults. Because older adults are more likely to have neurological conditions prior to brain injury, NF-L might be elevated differentially in older adults, compared with middle-age or younger adults, following mild traumatic brain injury (mTBI). A number of studies indicate that serum NF-L levels are higher in people with diverse neurological and neurodegenerative diseases. 9,27 –39 Therefore, as a potential diagnostic or prognostic biomarker for neurotrauma, it is important to determine whether there is an association between age and NF-L levels in individuals who sustain mTBIs. The purpose of this study is to determine whether NF-L is elevated differentially in older adults with pre-existing neurological disorders or diseases who present to the ED following mTBI. We hypothesized that there would be an association between older age and NF-L levels in both orthopedically-injured trauma control subjects and patients who sustain uncomplicated mTBIs. In addition, we hypothesized that older adults who sustain mTBIs who have pre-existing neurological diseases would have the highest levels of NF-L.
Methods
Participants
A sample of 325 adults and older adults were evaluated in the ED of Tampere University Hospital (Tampere, Finland) following head trauma and enrolled in a study. Of those, 224 underwent head CT and 190 had no trauma-related abnormalities identified on CT. Of the 190 with normal head CT scans, 130 had their blood sampled for long-term storage. For the final sample, 118 patients were included if their Glasgow Coma Scale score was 14 or 15 in the ED and they had their blood drawn within 72 h of injury. The mean age of the sample was 62.3 years (standard deviation [SD] = 22.5, range = 18–100; 52.5% women). Their mechanisms of injury were as follows: ground level fall = 70.3%; fall from height or unclassified fall = 7.6%; violence = 5.9%; sports = 5.1%; bicycle accident = 3.4%; motor vehicle accident = 2.5%; motorcycle accident = 0.8%; and other or unknown = 4.2%.
In the ED, a detailed case report form was completed for each enrolled patient. The percentages of the sample with loss of consciousness documented in the ED records were as follows: yes, witnessed = 17.8%; suspected = 31.4%; no = 41.5%; and unknown = 9.3%. The percentages of the sample with post-traumatic amnesia documented in the ED records were as follows: yes = 40.7%; no = 53.4%; and unknown = 5.9%. The percentages with focal neurological signs in the ED were: yes = 10.2%; no = 88.1%; and unknown = 1.7%. The health history of each enrolled patient was reviewed from the electronical patient records. Prior diagnosed diseases (including neurological diseases) were coded according to the International Classification of Diseases, 10th Revision (Table 1). All patients provided written informed consent according to the Declaration of Helsinki. The study protocol was approved by the ethical review board of Pirkanmaa Hospital District, Finland (ethical code: R15045).
Pre-Injury Neurological Conditions Identified in the Centralized Electronic Medical Records
N = 118. Some subjects have more than one diagnosis.
An orthopedically-injured control sample (n = 40) was obtained from the ED of Turku University Hospital (Finland) and included a subgroup of a previously published sample. 40 The orthopedic control sample included 22 men (55%) and 18 women. Their mean age was 52.15 years old (SD = 18.83, interquartile range [IQR] = 35.75–64.75, range = 22–90). The orthopedic injuries sustained by the control sample were as follows (n, percentage of sample): simple ankle fracture (n = 11, 27.5%); complex ankle fracture (n = 10, 25.0%); wrist fracture (n = 5, 12.5%); hip fracture (n = 3, 7.5%); humerus fracture (n = 3, 7.5); and forearm fracture (n = 2, 5.0). One person in the sample (2.5%) sustained each of the following injuries: clavicle fracture, complex pelvic fracture, knee fracture, hand fracture, and foot fracture. We were not able to determine whether some subjects experienced some degree of peripheral nerve injury because no neurophysiological assessments were undertaken. Control subjects were not included if there was any suspicion of an acute TBI (injury signs to the head, any suspicion of TBI signs at the time of injury, or symptoms suggesting a possible TBI) or they experienced polytrauma needing intensive care.
After completion of the study, the health history of each enrolled patient was reviewed from the electronical patient records. One subject was identified as having cerebrovascular disease and one subject was identified as having Alzheimer's disease. Many of the control subjects underwent magnetic resonance imaging (MRI) of their brain for research purposes (n = 31, 77.5% of the sample). If on MRI they had clear evidence of small vessel ischemic disease, multiple white matter hyperintensities, small infarcts, or frontal cortical dysplasia (or possible low-grade glioma; n = 1) they were classified as have a pre-injury neurological disease (n = 14). Some incidental findings on MRI were classified as broadly normal, such as frontal calcification in the corpus callosum (n = 1) and venous angiomas or cavernoma (n = 3). None of the subjects had imaging evidence of moderate-severe brain atrophy. The one subject with Alzheimer's disease documented in medical records did not undergo an MRI scan for research purposes. The control subjects were divided into three subgroups: no documented pre-injury neurological disease and broadly normal brain MRI scan (n = 16), no documented neurological disease and missing MRI scan (i.e., unknown pre-injury neurological disease; n = 9), and those with pre-injury neurological disease (n = 15). The study protocol was approved by the ethical review board of the Hospital District of South-West Finland (code: 68/180/2011).
Blood sampling and analytics
Venous blood samples for the mTBI group were collected in the ED. The mean time between injury and blood sampling was 8.3 h (median [Md] = 3.5; SD = 13.5; IQR = 1.9–6.0, range = 0.8–67.4, and 90% collected within 19 h). For the trauma control sample, venous blood samples were collected on the day of injury or the following day. Serum NF-L levels were measured using the Human Neurology 4-Plex A assay (N4PA) on an HD-1 Single Molecule Array (Simoa) instrument according to instructions from the manufacturer (Quanterix, Lexington, MA). The measurements were performed by board-certified laboratory technicians who were blinded to clinical data. The limit of detection for NF-L was 0.104 pg/mL and the limit of quantification was 0.241 pg/mL, with a calibration range of 0.533 to 453 pg/mL. Two internal quality control (QC) samples were analyzed in each run. For a QC sample with a concentration of 13.9 pg/mL, repeatability and intermediate precision was 4.4%, while for a QC sample with a concentration of 7.1 pg/mL, repeatability and intermediate precision was 6.1%. The trauma control sample was run at a different time than the mTBI sample, and the two runs were not calibrated for each other. Although the groups were analyzed in different runs, the control of the internal QC data showed that there were no differences between these runs and thus the results can be combined, and the approach will not unduly influence the results.
Statistical analysis
The associations between age and NF-L were examined in each group separately using Spearman correlations and nonparametric interferential statistics (Mann Whitney U tests) because both the biomarker levels and age were not normally distributed. Nonparametric analyses also were used to examine subgroups with the mTBI group with and without pre-injury neurological diseases. Receiver operator characteristic curve (ROC) analyses with a nonparametric estimate of the area under the curve were used to compare patients with mTBIs to trauma control subjects.
Results
Descriptive statistics for NF-L for the groups and subgroups are presented in Table 2. Within the orthopedically-injured trauma control group, the Spearman correlation between age and NF-L values was high (r = 0.76). For exploratory purposes, a subgroup of patients age 60 and older was compared with younger adults. The subgroup age 60 or older had higher NF-L levels than those younger than 60 (U = 349, p < 0.001, Cohen's d = 1.67; also see Fig. 1). There was one extreme outlier in the trauma control group (NF-L level of 140 pg/mL), a man in his mid-to-late 60s who was later found to have multiple periventricular white matter changes on brain MRI. The subgroup of control subjects with neurological disorders was older than the subgroup without neurological disorders (U = 229, p < 0.001, d = 2.37), and they also had higher NF-L levels (U = 184.5, p = 0.011, d = 1.59).
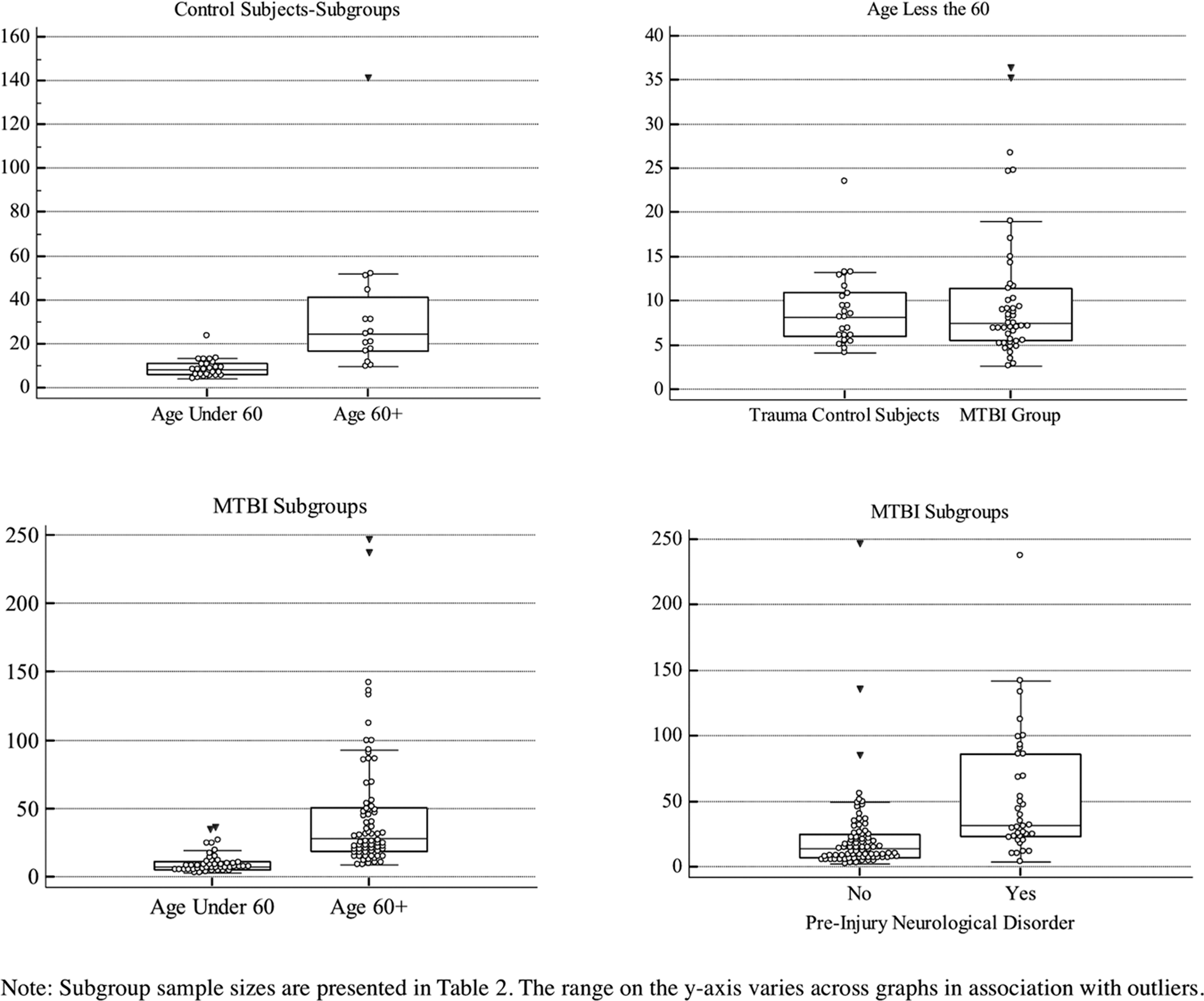
Box and whisker plots comparing subgroups.
Descriptive Statistics for NF-L (pg/mL) for the Groups and Subgroups
The average ages for control subjects were as follows: no neurological conditions, M = 36.2, Md = 33.5, SD = 11.5; neurological conditions unknown, M = 57.1, Md = 55.0, SD = 15.4; and pre-injury neurological conditions, M = 66.2, Md = 65.0, SD = 13.9.
NF-L, neurofilament light; M, mean; Md, median; SD, standard deviation; IQR, interquartile range; mTBI, mild traumatic brain injury.
Within the uncomplicated mTBI group, there was no significant difference in NF-L levels between men and women (U = 1470, p = 0.152). The NF-L levels were not associated with the time between injury and blood sampling (r = −0.072). The Spearman correlation between age and NF-L values was high (r = 0.80). The correlations between age and NF-L in subgroups of those with no pre-injury neurological conditions (r = 0.76) and pre-injury neurological conditions (r = 0.68) were high. Those with pre-injury neurological conditions had higher NF-L levels than those with no pre-injury neurological conditions (Md = 30.82 vs. 12.64, respectively; U = 2638, p < 0.001, d = 1.01). Again, for exploratory purposes, a subgroup of patients age 60 and older was compared with younger adults. The subgroup age 60 or older had higher NF-L levels than those younger than 60 (Md = 28.16 vs. 7.52; U = 3,048, p < 0.001, d = 1.14). For those with no pre-injury neurological conditions, those age ≥60 had higher NF-L levels than those age <60 (Md = 19.80 vs. 7.15; U = 850, p < 0.001, d = 1.18). For those with pre-injury neurological conditions, those age ≥60 had higher NF-L levels than those age <60 (Md = 35.20 vs. 8.36; U = 404, p < 0.001, d = 1.12). Box and whisker plots comparing subgroups are illustrated in Figure 1.
A ROC analysis under a nonparametric assumption revealed a modest statistically significant area under the curve (AUC) estimate of 0.635 (standard error [SE] = 0.48, p < 0.011, 95% CI = 0.540–0.730) for differentiating those with uncomplicated mTBIs from the trauma control subjects. However, when those with known pre-injury neurological diseases were excluded from the mTBI group only, there was no significant differentiation between the groups (AUC = 0.524, SE = 0.058, p = 0.684, 95% CI = 0.409–0.638). When those with known pre-injury neurological diseases were excluded from both groups, there was no significant differentiation between the groups (AUC = 0.601, SE = 0.065, p = 0.139, 95% CI = 0.474–0.729), despite the fact that the mTBI group (n = 64) was older (M = 54.5 years, SD = 23.1) than control subjects (n = 25; M = 43.7 years, SD = 16.3). There was no significant differentiation between age-stratified subgroups with uncomplicated mTBIs and the trauma control subjects who were younger than 60 (AUC = 0.498, SE = 0.071, p = 0.981, 95% CI = 0.360–0.637) or older than 60 (AUC = 0.582, SE = 0.079, p = 0.317, 95% CI = 0.427–0.736). There was a significant differentiation between subgroups with uncomplicated mTBIs and the trauma control subjects, both of whom had pre-injury neurological disease (AUC = 0.678, SE = 0.076, p = 0.036, 95% CI = 0.528–0.827).
Figure 2 illustrates every individual subjects' serum NF-L level. The subjects are sorted by age, beginning with age 18 and ending with age 100. Note that serum NF-L levels are well below 20 for the large majority of people in all three groups younger than 60. As seen in Table 2, 75% of those with mTBIs who are younger than 60 have NF-L values less than 11.5 (see the IQR). In contrast, individuals in their 70s, 80s, and 90s have highly elevated NF-L levels compared with young and middle-age adults. Older adults with pre-injury neurological conditions, in general, have higher NF-L levels than older adults who do not have pre-injury neurological conditions (Table 2; Fig. 1 and 2).

Neurofilament light levels in adults and older adults sorted by age.
Discussion
There is considerable interest in understanding the diagnostic and prognostic potential of NF-L as a serum biomarker for axonal injury associated with TBI. 12 –14 It is recognized that TBI in older adults is understudied, 18 and the effects of neurotrauma on the aging brain are not well understood. It is essential to examine NF-L in association with aging and neurological diseases because these factors might fundamentally compromise its usefulness as a diagnostic or prognostic biomarker for TBI in older adults. Our study is the first to examine whether NF-L is elevated differentially following uncomplicated mTBI in older adults with pre-existing neurological disorders. This study was not designed to be a diagnostic biomarker study. The kinetics of NF-L are slower than other blood-based biomarkers, making it less useful during the first few hours following injury. 13,16 This study was conceptualized to illustrate the associations between age, pre-injury neurological conditions, and acute mild head trauma on NF-L levels. As hypothesized, we found that age is associated with NF-L levels in subgroups of individuals with mTBIs and no pre-injury neurological disorders and in those with pre-injury neurological disorders. Specifically, individuals age ≥60 with mTBIs had higher NF-L levels than individuals younger than 60 for those with pre-injury neurological disorders and for those without pre-injury neurological disorders. We also found that, overall, individuals with mTBIs and pre-injury neurological disorders had higher NF-L levels than individuals without pre-injury neurological disorders. The strong association between older age and higher NF-L levels also was present in the orthopedically-injured trauma control sample. In general, NF-L was not particularly useful for differentiating those with uncomplicated mTBIs from trauma control subjects on the day of injury.
Recent studies have illustrated an association between age and blood-based biomarkers. 41,42 For example, S100B and glial fibrillary acidic protein (GFAP) levels have been shown to increase in relation to age. Calcagnile and colleagues concluded that older patients with acute mTBI (< 65 vs. ≥65 years) expressed significantly higher S100B levels. 42 Additionally, Gardner and colleagues reported that GFAP was less accurate for identifying CT-positive intracranial trauma among older versus younger mTBI patients. 41
Our results are consistent with past studies showing that serum levels of NF-L are higher in people with diverse neurological and neurodegenerative conditions. Researchers have reported that serum levels of NF-L are higher in people with multiple sclerosis, 9,27 –29 acute ischemic stroke, 30 active cerebral small vessel disease, 31 familial Alzheimer's disease, 32,33 Huntington's disease, 34 frontotemporal dementia, 35 Creutzfeldt-Jakob disease, 36 Parkinsonian disorders, 37 other degenerative ataxias, such as multiple system atrophy 38 and amyotrophic lateral sclerosis. 39
With regard to clinical usefulness, there are no established and validated cutoff values for NF-L as a biomarker for TBI of any severity across the lifespan using any commercially-available assay. It is important to note that studies suggest that NF-L has quite slow serum level dynamics. After acute injury, it appears to reach its peak concentration more than 7 days after the injury. 13,16 NF-L may therefore be of limited use in the ED but may prove to be a useful biomarker for predicting clinical outcome with samples taken several days following injury (e.g., Days 7–10). Future research can address the methodological limitations of the present study, and gaps in the literature more broadly by: 1) examining NF-L levels in older adults stratified by brain injury severity upon admission (i.e., mild, moderate, and severe); 2) studying the temporal kinetics of NF-L in the bloodstream after TBI to determine reliable time windows for acute diagnostics of TBI and outcome prediction (across the lifespan); 3) determining if NF-L levels can differentiate older adults with mild head trauma and positive or negative day-of-injury head CT findings; and 4) examining if extracerebral and especially peripheral nerve injuries affect the clinical reliability of NF-L in TBI diagnostics. Much additional research is needed to determine whether NF-L is useful for diagnostic or prognostic purposes following TBIs of all severities in older adults.
Footnotes
Acknowledgments
The authors acknowledge research assistant Anne Simi for her assistance with the patient enrollment and data collection at Tampere University Hospital, and research coordinator Annamari Aitolahti for her assistance with blood sample logistics. The authors thank TBIcare investigators Riikka S.K. Takala, Ari J. Katila, Janek Frantzén, Henna Ala-Seppälä, Anna Kyllönen, Henna-Riikka Maanpää, and Jussi Tallus for their contribution in control patient recruitment at Turku University Hospital.
Funding: The study was financially supported by the Finnish State Research Funding, and the Finnish Medical Society Duodecim. Dr. Luoto and Dr. Posti have received funding from Government's Special Financial Transfer tied to academic research in Health Sciences (Finland). Dr. Posti has received funding from the Emil Aaltonen Foundation sr and the Finnish Brain Foundation sr. Dr. Blennow acknowledges funding from The Torsten Söderberg Foundation, the Swedish Research Council, and the Swedish Brain Foundation. Dr. Zetterberg is a Wallenberg Academy Fellow and acknowledges support from the Swedish and European Research Council and the Dementia Research Institute at UCL.
Author Disclosure Statement
Grant Iverson acknowledges unrestricted philanthropic support from the Mooney-Reed Charitable Foundation and ImPACT Applications, Inc. He serves as a strategic scientific advisor for BioDirection, Inc. Jussi Posti has received speaker's fees from Orion corporation and Finnish Medical Association. Dr. Blennow has served as a consultant or at advisory boards for Alzheon, BioArctic, Biogen, Eli Lilly, Fujirebio Europe, IBL International, Merck, Novartis, Pfizer, and Roche Diagnostics, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB, a GU Venture-based platform company at the University of Gothenburg.