
Abstract
Methods of post-concussion diagnosis are still under debate with regard to sensitivity, objectivity, reliability, and costs. Spontaneous displays of nonverbal hand movement behavior during interaction are indicative of psychopathology and are relatively simple to record and analyze. Increased continuous (irregular) body-focused hand movement activity in particular indicates psychopathologies that overlap in symptomatology with those of sport-related concussions (SRCs). We therefore hypothesized that the duration of “irregular,” “on body,” and “act on each other” hand movements is increased in athletes with SRC who suffer from post-concussion symptoms. Three matched groups of 40 athletes were investigated: 14 symptomatic athletes with a concussion, 14 asymptomatic athletes with a concussion, and 12 non-concussed athletes. Using the Neuropsychological Gesture (NEUROGES)-Elan analysis system, four certified raters analyzed all nonverbal hand movements that were displayed during a videotaped standardized anamnesis about concussion history, incidence, course of action, and post-concussion symptoms. The duration of irregular Structure units among symptomatic athletes was significantly longer compared with asymptomatic athletes. Irregular, on body, and act on each other hand movement durations correlated with post-concussion symptoms. Whereas the duration of irregular units significantly predicted the post-concussion symptom score, working memory performances showed only marginal effects. Increased duration of irregular hand movement units indicates post-concussion symptoms in athletes with SRC. Because the recording of spontaneous displays of nonverbal hand movement behavior is relatively simple and cost efficient, we suggest using the neuropsychological analysis of hand movement behavior as a future diagnostic parameter of concussion management protocols.
Introduction
Sport-related concussions (mild traumatic brain injury [mTBI]) are recognized as a major public health concern 1 ; however, many concussions in sports remain undiagnosed. 2 In fact, players often dissimulate post-concussion symptoms in order to continue playing. 2 Consequently, athletes often return to play before symptoms are diminished, with an increased risk of cumulative effects from recurrent injury. 3 Therefore, multiple symptom scales and assessment tools of sport-related concussions have been proposed 4 that often remain difficult to administer due to problems of objectivity, costs, required materials, and expertise of the personnel. 5,6 Thus, the aim of this research is to explore potential post-concussion impairments that can serve as a basis for the development of more sensitive methods for future concussion diagnoses.
Increasing evidence suggests that mTBIs in sports are associated with a physical impact on the brain that can result in neuronal injury and subsequent motoric dysfunction. 7 –10 De Beaumont and colleagues reported reduced motor cortex excitability and reduced motor velocity in concussed athletes compared with athletes without reported concussions. 8 The duration of the cortical silent period, a marker of intra-cortical inhibition, showed to be prolonged in athletes who have experienced multiple concussions, pointing out that neuro-motor functions are impaired as a post-concussion deficit. 7 Heitger and colleagues reported that multiple motor systems, such as arm movement speed and accuracy, can be impaired as a post-concussion impairment independently of neuropsychological deficits (e.g., attention or working memory performances). 9,10 When individuals were asked to move with their hands an arrow into a box by using a steering wheel, wait for the go signal, then move the arrow past a line as fast as possible, individuals with mTBI showed reduced hand movement velocities compared with individuals with no history of mild, moderate, or severe head injury. 9 The study of patients with mTBI regarding their hand movement performance and the time post-concussion revealed that whereas reaction times are prolonged until 1 week post-concussion, hand movement velocities are reduced at least 12 months post-concussion compared with healthy control participants. 10 Thus, given the link of reduced hand movement velocities and therefore increased movement durations, 11 we assume that increased hand movement durations present a particularly sensitive parameter of post-concussion deficits.
Spontaneously displayed (implicit) hand movement behavior during interaction is associated with cognitive processes, 12,13 emotional processes, and psychopathology. 14 –18 Post-concussion symptoms concern alterations on the cognitive, emotional, and physical level. 4 SRCs are a risk factor for several disorders, such as Alzheimer's disease, depression, Parkinson's disease, or chronic traumatic encephalopathy (CTE) 19 –21 —that is, impairments that commonly present altered movement velocities 15,22,23 or alterations of the nonverbal hand movement behavior as a pathological consequence. 14,15,24 Although the behavior of athletes with multiple concussions and (post mortem) diagnoses of CTE has been described as agitated or restless years before death, 25 a systematic analysis of hand movement durations of concussed athletes is still missing. With regard to previous observations of altered movement velocities in concussed individuals, 7 –10 we hypothesize that the duration of spontaneous displays of nonverbal hand movement production is increased as a post-concussion impairment. Further, previous studies showed that increased durations of continuous (irregular) body-focused hand movements particularly characterize patients with psychopathology 14 –16 thus, we assume that irregular body-focused hand movements serve as an indicator of post-concussion symptoms. We therefore hypothesize that the duration of irregular body-focused hand movement units is increased in concussed athletes that suffer from post-concussion symptoms and when compared with asymptomatic or non-concussed athletes.
Methods
Participants
A total of 40 athletes (mean age: 22.7 ± 4.5; 13 females, 27 males; 35 right-handers, four left-handers, one ambidextrous; average years of sports participation: 9.2 ± 5.8) from various sports (American football, n = 13; hockey, n = 8), etc.) participated in the study. Participants were recruited via cooperation from local sports clubs for concussion assessment and baseline protocols. Informed consent was obtained from all individual participants included in the study. The local Ethics Committee approved the study.
Concussed participants (n = 28; mean age: 23.5 ± 4.7; eight females, 20 males) included athletes with self-reported post-concussion symptoms (n = 14) and without symptoms (n = 14). Non-concussed athletes (matched by age, gender, years of sports participation, and years of education; n = 12, mean age: 20.6 ± 3.4; five females, seven males) served as a control group. The two concussed participant groups were matched according to age, time post-concussion, and the amount of experienced concussions (i.e., no significant differences existed; mean time post-concussion = 22.0 ± 46.5 months; mean amount of experienced concussions = 1.8 ± 0.9; Table 1).
Participants
PCS, post-concussion symptom.
Concussions were assessed using self-reports according to the definition of the Consensus Statement on Concussion in Sport. 4 The symptom assessment scale of the Sport Concussion Assessment Tool—3rd edition (SCAT3) 26 was used to collect participants post-concussive symptoms. In this Likert-like symptom scale, each symptom is rated from 0 (none) to 6 (severe). The number of 22 symptoms is summated to a post-concussion symptom score (PCS score) with a maximum of 132 (22 × 6). We used a PCS score of 10 as a cut-off to differentiate between symptomatic and asymptomatic (concussed) athletes. Symptomatic athletes had significantly higher PCS scores [F(2, 37) = 36.507, p < 0.001; (mean) PCS = 30.0 ± 15.0], compared with asymptomatic (p < 0.001; PCS = 3.7 ± 3.3) and non-concussed athletes (p < 0.001; PCS = 3.7 ± 3.3). The most frequently reported symptoms in the symptomatic athlete group were “difficulty concentrating” (n = 13), “feeling slowed down” (n = 10), “fatigue or low energy” (n = 10), “sensitivity to light” (n = 9), “drowsiness” (n = 9), and “headaches” (n = 9).
Interview situation
Participants were questioned using a standardized questionnaire to obtain the athletes background, occurrence of a mild traumatic brain injury, description of the incident, time post-concussion, and post-concussion symptoms. If athletes answered no to the “occurrence of a mild traumatic brain injury” question, they were asked “if they observed concussions in their sport and how the incident happened.” The interview (/hand movement behavior of each participant) was recorded using a digital video camera (Canon Powershot G10) placed 3 m in front of the interviewee (Fig. 1.).
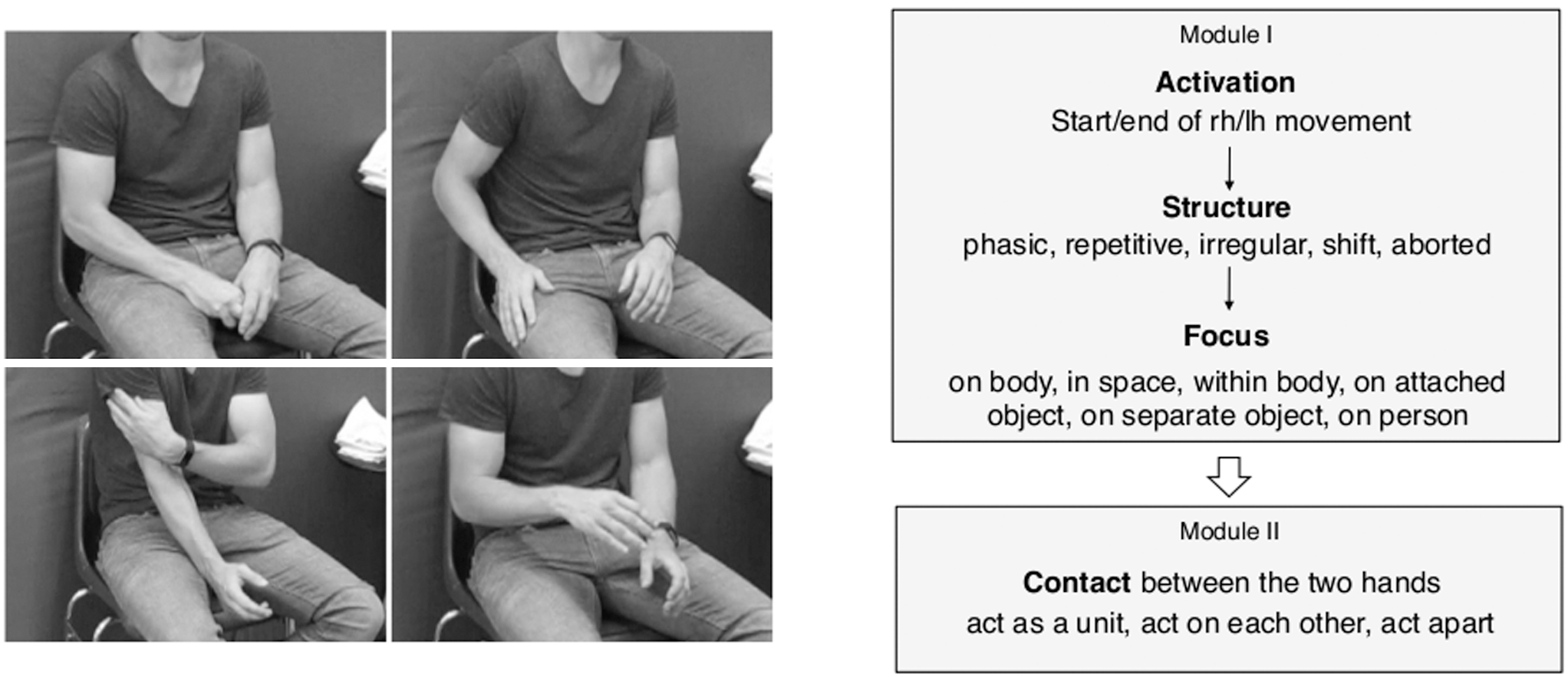
Left: Standardized interview situation and exemplary hand movement behavior of one participant. Right: Schematic (and shortened) overview over the Neuropsychological Gesture (NEUROGES)-algorithm adopted from Lausberg. 29
Memory task
Athletes performed a working memory (wm) task, which has been proven effective in the investigation of functional abnormalities of concussed athletes. 27,28 The depending variable of the wm task constitute the correct answers (%). For a more detailed description of this task, please see Helmich and colleagues. 27
Measurements
All occurring hand movements and gestures were coded using the Neuropsychological Gesture (NEUROGES)-Elan coding system. 29 Among the existent coding systems for hand movements, NEUROGES was chosen as it is objective and reliable. 13,14,30 –32 NEUROGES offers the possibility to examine the whole repertoire of hand movements (i.e., not only gestures but also self-touches, shifts, etc.; Module I).
Module I comprises the categories Activation, Structure and Focus. In the first evaluation step (Activation category), the stream of hand movement behavior is segmented into movement units versus no-movement (rest/pose) units based on the criteria motion, anti-gravity position and muscle contraction. All muscle contractions that immediately affect finger, wrist, elbow, or shoulder joints are considered. The Activation category provides a general impression of an individual's level of motor activity, as any appearing left- or right-hand movement is coded.
In the Structure category, the movement units are further assessed concerning specific combinations of trajectory, displacement, and velocity. In addition to these criteria, human raters consider the presence/absence of efforts and the presence/absence of hand shaping. Hand movements are evaluated based on whether they are executed with or without a phase structure (i.e., preparation, complex/stroke, and retraction phases). According to these criteria, five Structure values are distinguished: phasic, repetitive, shift, aborted, and irregular (Table 2.). There is evidence that the production of the different Structure values is associated with different levels of cognitive complexity. 29
The phasic, repetitive, and irregular units are further classified according to their orientation (Focus category). The Focus category refers to the presence or absence of dynamic contact with something/someone that the hand acts on. Thus, six Focus values are distinguished: within body, on body, on attached object, on separate object, on person, and in space (Table 3.).
Module II registers the relation between the two hands during simultaneous movement. The temporal overlaps of the right hand and left hand concatenated Structure Focus units constitute the new units for the Module II assessment. For these units, in which both hands move simultaneously, the Contact category is evaluated (Table 4.). It is operationalized by the presence/absence of physical contact between the hands and the quality of that contact. Three Contact values are distinguished: act apart, act as a unit, and act on each other. Act apart refers to sequences in which both hands move but do not touch each other (e.g., when forming both hands in order to describe the shape of a ball). Act as a unit refers to sequences in which the right and left hand establish static contact during a complex phase (e.g., when praying). Act on each other refers to sequences in which at least one hand has dynamic contact to the other hand (e.g., when fidgeting or the hands are rubbing each other).
Coding and inter-rater agreement
Four independent (and naive to the research question) raters were trained and certified to analyze hand movement behavior according to NEUROGES. 29 The videos were analyzed without sound to avoid raters being biased by verbal information. For each video, one rater coded 100% of the data for statistical analysis, whereas the second rater coded 25% of the data to establish inter-rater agreement (IA) for all categories of the NEUROGES. IA for the Activation category was calculated as the ratio between total length of overlaps from both annotators and total length of movement units from both annotators. IA on all other NEUROGES categories was established calculating a modified Cohen's kappa according to Holle and Rein. 33 This modified Cohen's kappa takes into account not only the categorization of values but also the temporal overlap of the raters' annotations. Results of the IA are presented as the modified Cohen's kappa and the raw agreement in Table 5. The raw agreement represents the number of agreeing cases divided by the total number of cases. The modified Cohen's kappa not only considers the raters' agreement concerning the value, but also the segmentation of behavior in time (i.e., if there is a unit and when it begins and ends). In terms of Landis and Koch, 34 the agreement in the present investigation can be described as “substantial.”
IA, inter-rater agreement.
Statistical analysis
Repeated measures analyses of variance (ANOVAs) were performed using SPSS (IBM SPSS Statistics version 25). The between-subjects factor constituted three groups; non-concussed, asymptomatic (PCS score <10), and symptomatic athletes (PCS score >10) athletes. The duration (D; seconds/movement unit) of hand movement units of each category (Activation, Structure, Focus, and Contact) served as the dependent variable. Multiple post hoc pairwise comparisons were corrected with Bonferroni corrections. If fewer than 10 individuals in each group performed a hand movement value, we skipped the value from the statistical analysis. Thus, the following values were included in the statistics: movement (Activation); phasic, irregular, repetitive (Structure); in space, on body (Focus), act apart, act on each other (Contact). To determine a relationship of hand movements and post-concussion symptoms, we correlated hand movements with the PCS score using the Pearson correlation coefficient (rp). Significant correlations were then analyzed by a linear regression analysis to gain insights if a particular hand movement value predicts post-concussion symptoms. To set hand movements in ratio to cognitive functions, we additionally correlated (and performed a regression analysis) between hand movements, wm scores, and the PCS score. In a final step, a Spearman's rank-order correlation (rs) was run to determine the relationship of each single symptom and the duration of irregular hand movement units.
Results
ANOVAs: hand movement durations
Significant effects were found on the hand movement Structure level for group [F(2, 35) = 3.337, p < 0.05, η 2 = 0.160], Structure [F(2, 70) = 6.685, p < 0.01, η 2 = 0.160], and the interaction of group and Structure [F(4, 70) = 3.506, p < 0.05, η 2 = 0.167]. Post hoc comparisons between groups revealed that symptomatic athletes had significant longer Structure units compared with asymptomatic athletes (p = 0.05; Fig. 2.).
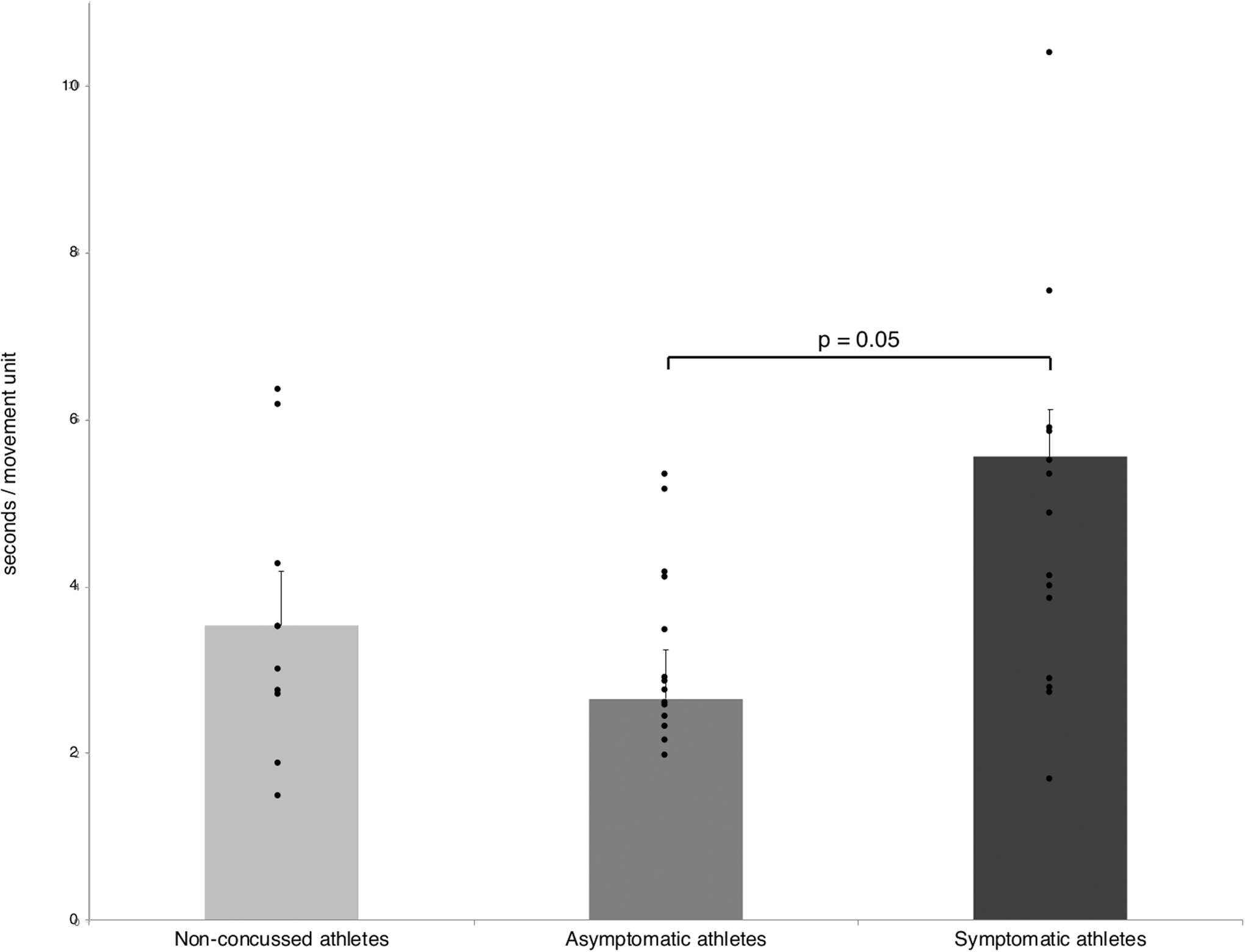
Structure unit durations of symptomatic, asymptomatic, and non-concussed athletes.
Further, irregular units had the longest unit durations, significantly different from the phasic units (p < 0.05). Repetitive units are significantly longer compared with phasic units (p < 0.05). The interaction effect of group and Structure showed that symptomatic athletes had significantly longer irregular units compared with asymptomatic athletes (p < 0.05; Fig. 3.).

Irregular, phasic, and repetitive unit durations of symptomatic, asymptomatic, and non-concussed athletes.
The analysis of the Focus of hand movement units revealed significant effects for Focus [F(1, 36) = 14.892, p < 0.001, η 2 = 0.293]. On body units were significantly longer than in space units (p < 0.001). The analysis of Contact durations revealed significant effects for Contact [F(1, 36) = 20.161, p < 0.001, η 2 = 0.359]. Act on each other units were significantly longer compared with act apart units (p < 0.001).
Correlation/regression analyses: Irregular unit durations and PCS score
A significant correlation was found for (higher) PCS scores and (longer) durations of movement [rp(40) = 0.500, p = 0.001], irregular [rp(40) = 0.546, p < 0.001], on body [rp(40) = 0.546, p < 0.001], and act on each other units [rp(40) = 0.546, p < 0.001]. The linear regression with PCS score as the dependent variable and movement units of movement, irregular, on body, and act on each other as the independent variables revealed a significant effect [F(4, 38) = 4.990, p < 0.001, R2 = 0.370], that is, the duration of irregular units significantly predicted the PCS score (β = 1.257, t = 2.527, p < 0.05; Fig. 4.).
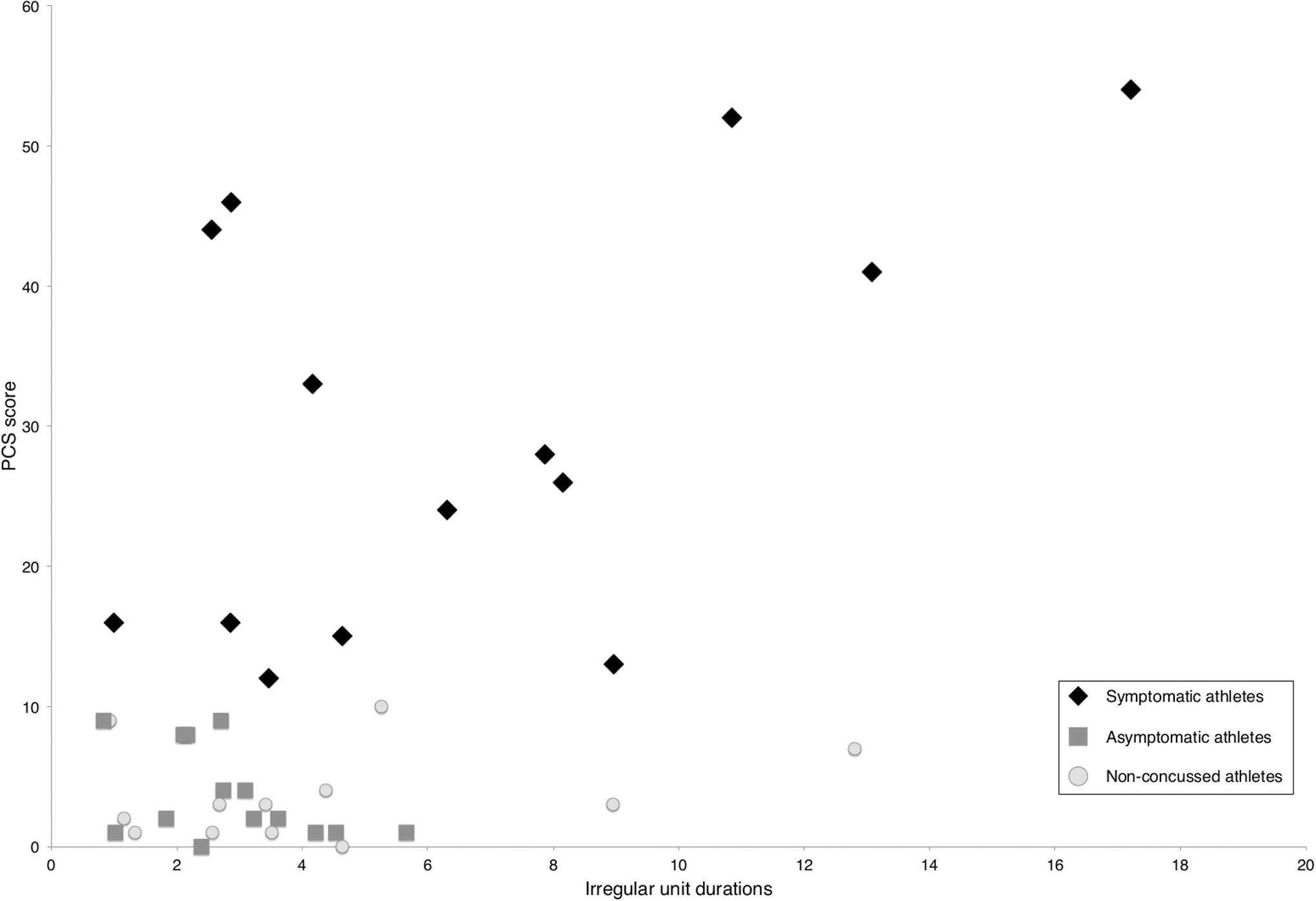
Significant correlation of irregular unit durations and post-concussion symptoms.
Working memory task and irregular unit durations
No significant differences between groups were found for the wm scores [F(2, 39) = 2.589, p = 0.089]. Still, symptomatic athletes had fewer correct answers (86%) compared with asymptomatic (88%) and non-concussed athletes (90%). A significant (negative) correlation was found between correct wm answers and post-concussion symptoms [rp(40) = -0.315, p < 0.05]. A linear regression with PCS score as the dependent variable and movement units of irregular and wm scores as the independent variables revealed significance [F(2, 39) = 10.318, p < 0.001, R2 = 0.358], that is, the duration of irregular units significantly predicted the PCS score (β = 0.513, t = 3.860, p < 0.001). The wm score showed a marginal influence (β = -0.248, t = -1.866, p = 0.07).
Irregular unit durations and post-concussion symptoms
Significant correlations were observed for irregular units and the post-concussion symptoms “pressure in the head” [rs(40) = 0.479, p < 0.01], neck pain [rs(40) = 0.361, p < 0.05], difficulty concentrating [rs(40) = 0.361, p < 0.05], fatigue or low energy [rs(40) = 0.338, p < 0.05], and drowsiness [rs(40) = 0.352, p < 0.05]. A linear regression analysis with irregular unit durations as the dependent variable and the (significant) symptoms as independent variables revealed significance [F(5, 39) = 5.773, p < 0.01, R2 = 0.459], that is the post-concussion symptom drowsiness significantly predicted the duration of irregular units (β = 0.488, t = 2.806, p < 0.01; Fig. 5.).
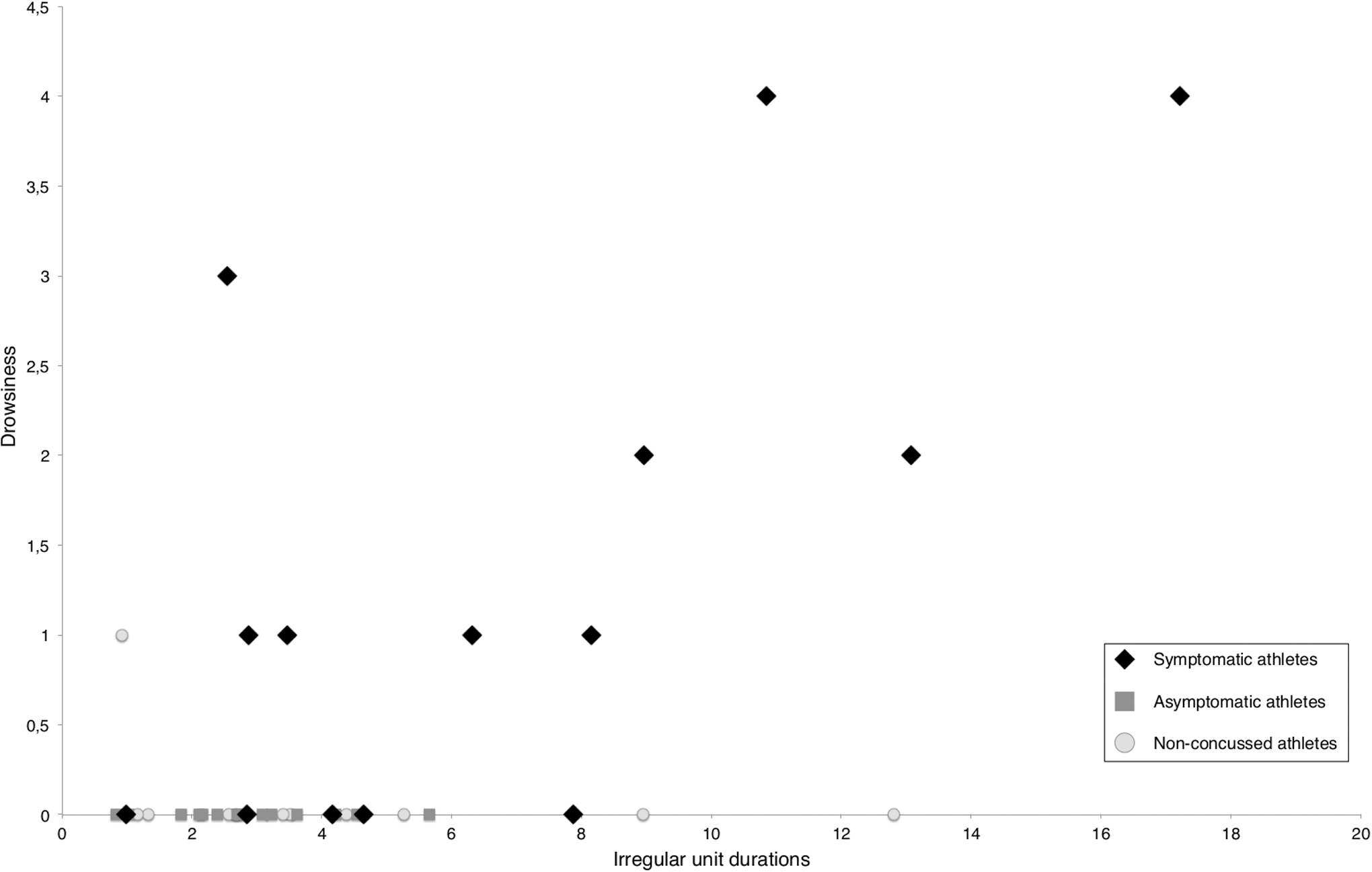
Significant correlation of irregular unit durations and the post-concussion symptom drowsiness.
Discussion
This research revealed that the duration of nonverbal hand movements that are spontaneously displayed during an anamnesis for sport-related concussions is altered in symptomatic athletes with a mTBI. The main findings of this study are that irregular unit durations indicate post-concussion symptoms. Although longer irregular, on body, and act on each other hand movement units correlate with increased post-concussion symptoms, only irregular hand movements differentiate symptomatic from asymptomatic athletes. Further, unit durations of irregular hand movements showed superiority when predicting the PCS score versus working memory score. Although several symptoms correlate with longer irregular units, solely the symptom drowsiness predicts increased unit durations of irregular hand movements.
Altered durations of nonverbal hand movements
Symptomatic athletes had longer hand movement durations compared with asymptomatic and non-concussed athletes. This fact was present for all NEUROGES categories; however, only on the Structure level significant differences emerged. This finding indicates that concussed athletes with post-concussion symptoms move their hands longer and therefore potentially slower compared with asymptomatic athletes. Decreased hand movement velocities have been commonly described as a post-concussion deficit when analyzing reaction times, 35,36 when steering a wheel during visuo-motor tests, 9,10 or for grasp-release movements. 37 However, and in contrast to the nonverbal hand movement activity, the previously described impairments 9,10,35 –37 have in common that those hand movements were performed on command during specific experimental setups. In our study, the data expands those findings by the fact that the duration of nonverbal hand movements is altered independently of any specific experimental task.
No significant differences were observed between the symptomatic athlete group and non-concussed athletes. This result is grounded in the fact that two non-concussed athletes presented increased hand movement durations, similarly to those of symptomatic athletes. In fact, when excluding these athletes from the statistical analysis, significant results emerge between symptomatic and non-concussed athletes. A particular problem in sports constitutes the fact that players often do not report concussions; in fact, players often dissimulate post-concussion symptoms in order to continue playing. 2 The two athletes were active players in ice hockey and American football (i.e., sports with a high occurrence of sport-related concussions). 4 Because implicit hand movements are expressed beyond a person's awareness, 30 it is possible that those athletes experienced concussions but did not report them. Future studies must therefore address whether the nonverbal behavior can identify concussed/symptomatic athletes by their hand movement behavior independently from the athlete's self-reports.
Irregular hand movement durations predict post-concussion symptoms
Symptomatic athletes execute particularly longer irregular hand movement durations compared with asymptomatic athletes. Irregular activity has been shown to characterize patients with psychopathology, particularly depressive patients. 14 –16 This resulted in the proposition that irregular hand movements serve to regulate stress and arousal. 17,30 With regard to these findings, 14 –16 we assume that symptomatic athletes spend more time for the execution of irregular movements in relation to their symptomatic state. Thus, irregular hand movement durations indicate a behavioral marker of post-concussion symptoms.
Further, irregular, on body and act on each other unit durations were shown to correlate with post-concussion symptoms. On body and act on each other movements present hand movements that act on the body surface, such as when fidgeting. This indicates that symptomatic athletes are increasingly dealing with their own body. Thus far, body-focused activity has been increasingly reported in psychiatric disorders. 14,15,24,38 A previous proposition constitutes that on body movements serve to stabilize oneself mostly in order to care or calm oneself. 30 Self-soothing behavior also has been linked to the release of oxytocin associated with well-being and the reduction of stress levels. 39 We therefore hypothesize that symptomatic athletes execute longer irregular, on body, and act on each other hand movement units in order to alleviate their post-concussion symptomatology.
Although irregular, on body, and act on each other unit durations were shown to correlate with post-concussion symptoms, only irregular unit durations significantly predicted higher symptom scores. Further analyses showed that irregular unit durations served as a stronger predictor of post-concussion symptoms than even wm scores. This is not surprising as previous motor impairments have been reported independently from deficits during attention or working memory performances post-concussion. 9,10 Because increased hand movement durations have been observed in several disorders that often overlap in symptomatology with mTBI, such as depression, mild cognitive impairment, Alzheimer's disease, or dementia, 14,15,22,40 we propose that future diagnostic assessment protocols must include the neuropsychological analysis of nonverbal hand movement behavior, particularly irregular hand movement unit durations.
Irregular unit durations further were shown to correlate with single symptoms such as “pressure in the head,” neck pain, difficulty concentrating, fatigue or low energy, and drowsiness; however, drowsiness had the strongest influence on increased irregular unit durations. Symptoms of drowsiness, nausea, and concentration problems previously were shown to be associated with prolonged symptoms in concussed athletes. 41 Thus, irregular hand movement behavior might serve as a predictive tool of prolonged post-concussion symptomatology.
Conclusion
Increased durations of irregular hand movement units present a behavioral marker of post-concussion deficits that is not only superior to other hand movement categories but also to cognitive assessments such as working memory tasks. As the recording of nonverbal movement behavior is relatively simple and cost efficient and provides an implicit behavioral expression that cannot be concealed from diagnosis, we suggest to include the neuropsychological analysis of hand movements, particularly irregular hand movement Structures, as a future diagnostic parameter of concussion management protocols.
Footnotes
Acknowledgments
The study was funded by the University research funding of the German Sports University, Cologne (L-11-10011-175-122000).
Author Disclosure Statement
No competing financial interests exist.