
Abstract
Evidence suggests that blast exposure has profound negative consequences for the health of the human brain, and that it may confer risk for the development of neurodegenerative diseases such as chronic traumatic encephalopathy and Alzheimer's disease (AD). Although the molecular mechanisms linking blast exposure to subsequent neurodegeneration is an active focus of research, recent studies suggest that genetic risk for AD may elevate the risk of neurodegeneration following traumatic brain injury (TBI). However, it is currently unknown if blast exposure also interacts with AD risk to promote neurodegeneration. In this study we examined whether apolipoprotein (APOE) ɛ4, a well-known genetic risk factor for AD, influenced the relationship between blast exposure and white matter integrity in a cohort of 200 Iraq and Afghanistan war veterans. Analyses revealed a significant interaction between close-range blast exposure (CBE) (close range being within 10 m) and APOE ɛ4 carrier status in predicting white matter abnormalities, measured by a voxelwise cluster-based method that captures spatial heterogeneity in white matter disruptions. This interaction remained significant after controlling for TBI, pointing to the specificity of CBE and APOE in white matter disruptions. Further, among veteran ɛ4 carriers exposed to close-range blast, we observed a positive association between the number of CBEs and the number of white matter abnormalities. These results raise the possibility that CBE interacts with AD genetic influences on neuropathological processes such as the degradation of white matter integrity.
Introduction
Because of the frequent use of explosive devices in modern warfare, blast exposure has been a common occurrence in the Iraq and Afghanistan wars. Estimates suggest that 75% of traumatic brain injuries (TBIs) that occurred during these wars were caused by blasts, and that more than half of the veterans who did not report a TBI during their service were still exposed to two or more nearby explosive blasts. 1 However, despite the prevalence of blast exposure in veterans of the wars in Iraq and Afghanistan, research on the health effects of blast exposure is still in its early stages.
Emerging evidence suggests that blast exposure, even in the absence of a diagnosed TBI, may have adverse neural consequences. For example, using diffusion tensor imaging (DTI) and a voxelwise cluster-based method that accounts for spatially heterogenous white matter abnormalities, Taber and colleagues 2 found that blast exposure, regardless of TBI, was associated with a greater number of clusters with reduced white matter integrity, as indicated by reduced fractional anisotropy (FA). Similarly, Bazarian and colleagues 3 showed that compared with unexposed individuals, veterans exposed to one or more blasts had reductions in FA across the brain. Additionally, Robinson and colleagues 4 found that exposure to a blast within ≤10 m was associated with decreased functional connectivity of bilateral primary somatosensory and motor cortices. Together, these studies suggest that blast exposure, particularly when experienced at close range, is associated with neural abnormalities.
The neural consequences of blast exposure are of great concern, as preliminary evidence suggests that blast exposure may negatively impact brain-aging trajectories in white matter, 5 potentially exacerbating neurodegenerative processes. These findings echo research surrounding TBI, which has been shown to be a robust environmental risk factor for neurodegenerative diseases such as Alzheimer's disease (AD) and chronic traumatic encephalopathy (CTE). 6 –11 The mechanisms linking these environmental factors to increased risk for neurodegenerative disease are the focus of many ongoing studies. Evidence suggests that TBI may interact with genetic risk for AD in conferring risk for neurodegeneration. Specifically, studies focused on TBI in individuals carrying the apolipoprotein (APOE) ɛ4 allele, a well-established AD genetic risk factor, suggest that ɛ4 carriers with head trauma have an increased risk of AD 12 –15 and poorer outcome. 16 –18 Additionally, APOE ɛ4 may promote amyloid deposition in individuals with TBI, 19,20 and the combination of mild TBI and genetic risk for AD may play a role in the degradation of structural brain integrity in vivo. 21 These results highlight the possibility that TBI exaggerates genetically associated neuropathological processes. However, it is unknown whether blast exposure also influences the association between genetic risk for AD and compromised neural integrity.
In this study, we used voxelwise cluster-based methods previously shown to be sensitive to white matter abnormalities in blast exposure 2,22,23 in a large group of Operation Enduring Freedom/Iraqi Freedom/New Dawn (OEF/OIF/OND) veterans. These voxelwise cluster-based methods capture diffuse and spatially non-overlapping white matter disruptions by examining the total number rather than the location of white matter abnormalities. The aim of this study was to examine whether the relationship between close-range blast exposure (CBE) and white matter structural integrity varied as a function of APOE ɛ4 carrier status. Further, because blast exposure is often complicated by coexisting conditions, we also examined other potential confounding factors including TBI, post-traumatic stress disorder (PTSD), and sleep impairment.
Methods
Participants
Our sample included 200 Iraq and Afghanistan war veterans (i.e., deployed to OEF/OIF/OND), consecutively enrolled into the Translational Research Center for TBI and Stress Disorders (TRACTS) 24 at the VA Boston Healthcare System, who had available genetic, clinical, and neuroimaging data. Individuals were recruited from the Boston metropolitan area through community outreach events. Exclusion criteria for this study included history of moderate/severe TBI, abnormal incidental findings on research scans (i.e., fluid-attenuated inversion recovery [FLAIR] susceptibility-weighted, and high resolution T1 scans) as determined by a neuroradiologist, history of seizures not related to TBI, vascular disease, heart conditions, serious mental illness such as bipolar disorder or significant psychiatric conditions such as psychosis, current suicidal or homicidal ideation, and incompatibility with magnetic resonance imaging (MRI) because of ferromagnetic objects in the body or pregnancy.
An additional 17 Iraq and Afghanistan veterans (i.e., deployed to OEF/OIF/OND) without a history of blast exposure or lifetime TBI and who did not meet diagnostic criteria for PTSD as assessed by the Clinician-Administered PTSD Scale (CAPS) for the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) 25 formed the reference group for neuroimaging analyses.
All study procedures were in accordance with the Declaration of Helenski and were reviewed and approved by the appropriate institutional review board. All participants provided written informed consent.
Clinical and cognitive measures
History of blast exposure and TBI was assessed by doctoral-level psychologists using the Boston Assessment of TBI-Lifetime (BAT-L), 26 a semistructured interview based on Department of Defense TBI diagnostic criteria. The BAT-L queries participants about blast exposure and TBI that occurred before, during, and after military experience. The BAT-L also includes classification of blast exposure events into distance ranges (0–10 m, 11–25 m, 26–100 m). Members in the CBE group were defined as positive if they experienced at least one blast in the 0–10 m range or negative if they experienced no blasts in that range. Additionally, the total number of blast exposure events in the 0–10m range was summed for each individual to obtain a continuous measure of CBE. For the purposes of this study, moderate and severe TBI were exclusionary criteria and only mild lifetime and military TBI were examined, which was defined as the presence of altered mental status for <24 h, post-traumatic amnesia of <24 h, and/or loss of consciousness for <30 min before, during, or after military experience (lifetime) or during military experience related to blast or other deployment mechanisms (military).
PTSD was assessed with the CAPS for DSM-IV 25 by doctoral level psychologists. The CAPS is a structured interview that is currently the gold standard for assessment of PTSD. Total CAPS scores were used as a measure of current PTSD symptom severity. Sleep impairment was assessed with the Pittsburgh Sleep Quality Index (PSQI) and defined as a global score >5 on the PSQI. 27
All diagnoses were reviewed by a diagnostic team consensus of at least three PhDs or MDs for confirmation of TBI and DSM-IV diagnoses.
MRI acquisition and processing
Neuroimaging data were collected with a 12 channel head coil on a Siemens 3-Tesla TIM Trio whole-body scanner at VA Boston from 2010 to 2015. Two T1-weighted magnetization-prepared rapid gradient-echo (MP-RAGE) anatomical scans were collected for each participant with the following parameters: voxel size = 1 mm3, T1 = 1100 ms, repetition time (TR) = 2530 sec, echo time (TE) = 3.32 ms, field of view (FOV) = 256 × 256, number of slices = 176, flip angle = 7 degrees. These two MP-RAGE scans were then averaged into a single image to create a high contrast-to-noise image. Additionally, a DTI scan ∼12 min long was collected with the following parameters: one acquisition of 60 directions, interleaved, 2 × GeneRalized Autocalibrating Partial Parallel Acquisition (GRAPPA) acceleration, FOV = 256, matrix = 128 × 128, TR = 10,000 ms, TE = 103 ms, voxel size = 2 mm3, b value = 700 sec/mm2, 10 b0 volumes.
All imaging data, including reference group cases, were analyzed using the Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) Diffusion Toolbox (FDT) of the FSL software package (version 5.0.8;
To identify clusters with reduced FA, z-score maps from the FA standard space skeletonized images produced by TBSS were calculated. 22,30 This involved converting each white matter voxel into a z-score based on the reference group (n = 17). Z-score maps were then thresholded at z = -3 to limit the maps to clusters with abnormally reduced FA. The total number of white matter clusters with z ≤ -3 in at least five contiguous voxels was calculated for each individual, excluding those in the reference group, and used for further analyses (see Fig. 1 for group maps).
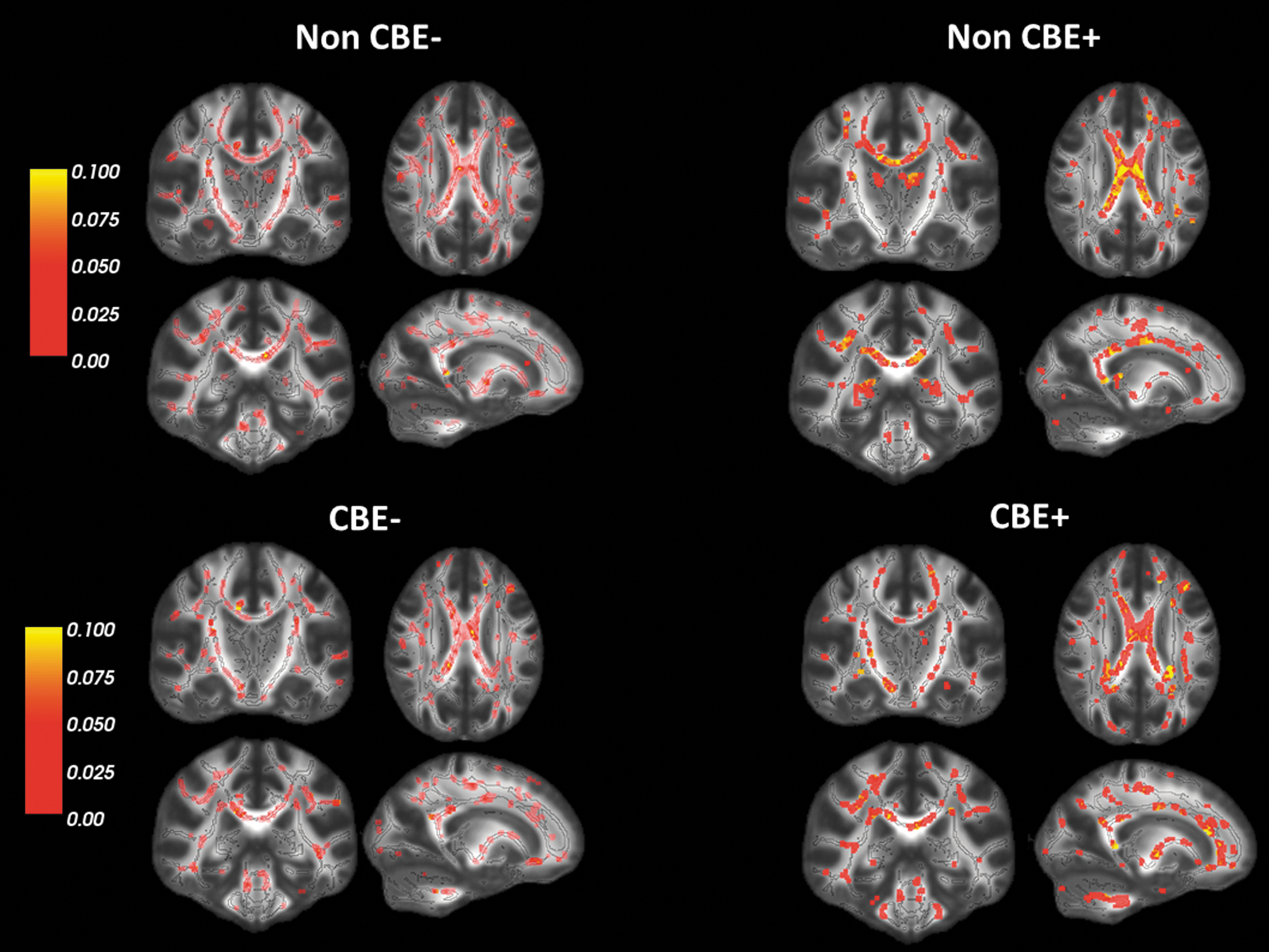
Distribution of clusters with reduced fractional anisotropy (FA) by apolipoprotein (APOE) status within close-range blast exposure (CBE) groups (non-CBE+/CBE+ indicates APOE ɛ4 carriers within respective CBE group, non-CBE/CBE- indicates non ɛ4 carriers within respective CBE group). Scale represents the proportion of individuals within each group that have a cluster with reduced FA in the area marked. Lighter red indicates fewer individuals with a cluster in the area marked, and yellow indicates a greater number of individuals with a cluster in the area marked. The black outline represents the outline of the white matter skeleton used in calculation of z-score maps. Clusters with reduced FA were dilated for ease of viewing.
DNA genotyping and polygenic risk score (PRS) calculation
DNA was extracted from whole blood using the Qiagen Qiamp mini kit. Genotyping of the APOE single nucleotide polymorphisms (SNPs) (rs429358 and rs7412) was performed using an ABI TaqMan® 7900 Fast Real-Time PCR system, with the TaqMan® SNP Genotyping Assays C-3084793-20 and C-904973-10 and TaqMan® Universal PCR Master Mix, AmpErase® UNG. Finally, assays were performed on an ABI 7900HT apparatus according to the manufacturer's protocol. APOE genotype was coded as APOE ɛ4 carriers versus non-carriers (i.e., subjects with at least one ɛ4 allele vs. subjects with ɛ2/ ɛ3 or ɛ3/ ɛ3 genotypes; there were no ɛ2/ ɛ2 subjects observed in this cohort).
To obtain principal components representing population substructure, we also generated genotypes at the Pharmacogenomics Analysis Laboratory (PAL) at the Central Arkansas Veterans Healthcare System in Little Rock, Arkansas. DNA was extracted from peripheral blood samples hybridized to Illumina HumanOmni2.5-8 BeadChips and imaged with the Illumina iScan System (Illumina, San Diego, CA). Concordance with self-reported ancestry and genotype was investigated in a genetic principal components analysis using the program EIGENSTRAT, 31 based on 100,000 SNPs merged with 1000 genomes' phase 1 reference data. 32
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY). Total number of clusters with reduced FA was log transformed with base 10 to account for the positive skew of the data before entering the variable into further analyses.
To examine the effect of CBE group and its interaction with APOE on the number of clusters with reduced FA, a hierarchical linear regression analysis was performed in which number of clusters with reduced FA was the dependent variable. Age, sex, the first two principal components representing population substructure, current PTSD symptom severity, and sleep impairment were added as covariates in the first step of the model, main effects of CBE group and APOE were added in the second step, and the interaction between CBE group and APOE was added in the final step. To confirm that the effect was associated with CBE group and not with underlying TBI effects, we repeated analyses including lifetime TBI or military TBI as a covariate in the first step of the model.
Additionally, to investigate potential dose effects of CBE, we repeated hierarchal linear regression models replacing CBE group with the number of CBEs to examine the interaction between the total number of CBEs and APOE on the number of clusters with reduced FA.
To examine other potential influences on the association between APOE and clusters with reduced FA, linear hierarchal regression analyses examined the main effects of (1) lifetime TBI (yes/no), (2) military TBI, (3) PTSD (total CAPS score), and (4) sleep impairment (yes/no) as well as their interactions with APOE. These analyses followed the primary hierarchal regression model and replaced CBE group with either lifetime TBI, military TBI, PTSD symptom severity, or sleep impairment. In the analyses focused on PTSD and sleep impairment, PTSD symptom severity or sleep impairment was examined as a main effect in the second step of the model and CBE group was added as a covariate in the first step.
Results
Participant demographics and clinical characteristics are listed in Table 1. Compared with the non-CBE group, the CBE group were younger on average, exhibited more PTSD symptoms, and had a greater percentage of individuals with TBI and sleep impairment.
Demographic and Clinical Characteristics
Group comparisons are measured between the CBE groups. CBE group was defined as an exposure to a blast that was <10 m away. PSQI sleep impairment was unavailable for one participant, and APOE genotype was unavailable for three participants in the reference group. The reference group was selected based on no lifetime TBI, current PTSD, or blast exposure.
The reference group had significantly fewer participants with sleep impairment than either the CBE or the non-CBE group (χ2[2]) = 9.3, p = 0.009). The total number of white matter clusters is not log transformed for ease of interpretation.
p < 0.05; ** p < 0.001.
APOE, apolipoprotein; CBE, close-range blast exposure; TBI, traumatic brain injury; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder.
Results of regression analyses revealed that there were no significant main effects of CBE group or APOE on clusters with reduced FA (p's > 0.07, Table 2, Fig. 1). However, there was a significant interaction between CBE group and APOE on clusters with reduced FA, whereby there was an effect of the ɛ4 allele with CBE on the number of white matter abnormalities (p = 0.04, Table 2, Fig. 2). Given that individuals with CBE had significantly more lifetime TBIs than individuals without CBE, we repeated analyses controlling for lifetime TBI in the first step of the model. Results did not change, with a significant interaction between APOE and CBE group on clusters with reduced FA after accounting for either lifetime or military TBI (p's = 0.04).

Increased number of clusters with reduced fractional anisotropy (FA) in apolipoprotein (APOE) ɛ4 carriers who experienced a close-range blast exposure (CBE). Values on the x-axis represent whether an individual experienced a CBE (yes or no), which was defined as a blast within ≤10 m. Values on the y-axis represent the log transformed total number of clusters with reduced FA. Dark gray bars indicate non-ɛ4 carriers and light gray bars indicate individuals with at least one APOE ɛ4 allele. Error bars reflect 95% confidence intervals.
Summary of Regression Analysis for the Association of CBE Group by APOE E4 Carrier Status on White Matter Integrity
p < 0.05; ** p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; CBE, close-range blast exposure; PC, principal components; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error.
To further explore the nature of the interaction between APOE and CBE group on clusters with reduced FA, we performed analyses of covariance (ANCOVAs), adjusting for covariates, in which we divided the sample by APOE carrier status. Results revealed a trend toward a greater number of clusters with reduced FA among ɛ4 carriers exposed to a close-range blast compared with carriers not exposed to a close-range blast (F 1,47 = 4.03, partial η2 = 0.079, p = 0.05; Fig. 2). There were no significant group differences in non-carriers (F 1,137 = 0.493, partial η2 = 0.004, p > 0.4; Fig. 2).
We then performed a hierarchal linear regression, adjusting for covariates, in which we focused on a continuous measure of CBE (mean = 1.73, standard deviation [SD] = 5.08, range = 0–55). Results revealed a significant interaction between total number of CBEs and APOE on the number of clusters with reduced FA, whereby ɛ4 carriers with more CBEs had a greater number of white matter clusters with reduced FA (p < 0.001, Table 3, Fig. 3A). 1 Follow-up partial Pearson correlations revealed that there was a significant positive correlation between the number of clusters with reduced FA and CBEs in APOE ɛ4 carriers (n = 55, r = 0.404, p = 0.004) but not in non-carriers (n = 145, r = -0.078, p > 0.3). Upon closer inspection of the data, there were several individuals who had extreme values for the number of CBEs. To ensure that the results were not driven by these extreme values, we repeated analyses removing these four individuals (n = 196; number of CBEs mean = 1.12, SD = 1.99, range = 0–12). The results remained significant (regression: R2 = 0.146, β = 0.027, p = 0.027; APOE ɛ4 carriers correlation: n = 54, r = 0.3, p < 0.04; non-carriers correlation: n = 142, r = -0.035, p > 0.6; Fig. 3B).

There is a greater number of clusters with reduced fractional anisotropy (FA) in apolipoprotein (APOE) ɛ4 carriers with an increasing number of close-range blast exposures (CBEs) in (
Summary of Regression Analysis for the Association of Total Number of CBEs by APOE E4 Carrier Status on White Matter Integrity
p < 0.05; ** p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; CBE, close-range blast exposure; PC, principal components; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error.
Finally, to examine other potential influences on the association between APOE and the number of clusters with reduced FA, we performed hierarchal regression models in which we replaced CBE group in the primary model with (1) lifetime TBI, (2) military TBI, (3) PTSD, or (4) sleep impairment. Results revealed that neither the main (p's > 0.2) or interaction (p's > 0.1) effects of TBI, PTSD, or sleep impairment were significantly associated with clusters with reduced FA (Tables 4 –7).
Summary of Regression Analysis for the Association of Lifetime TBI by APOE E4 Carrier Status on White Matter Integrity
p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; PC, principal components; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error; TBI, traumatic brain injury.
Summary of Regression Analysis for the Association of Military TBI by APOE E4 Carrier Status on White Matter Integrity
p < 0.05; ** p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; PC, principal components; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error; TBI, traumatic brain injury.
Summary of Regression Analysis for the Association of PTSD Symptom Severity by APOE E4 Carrier Status on White Matter Integrity
p < 0.05; ** p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; CBE, close-range blast exposure; PC, principal components; PSQIPi, ttsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error; TBI, traumatic brain injury.
Summary of Regression Analysis for the Association of Sleep Impairment by APOE E4 Carrier Status on White Matter Integrity
p < 0.05; ** p < 0.01.
APOE, apolipoprotein; CAPS, Clinician-Administered PTSD Scale; CBE, close-range blast exposure; PC, principal components; PSQI, Pittsburgh Sleep Quality Index; PTSD, post-traumatic stress disorder; SE, standard error.
Discussion
In a cohort of 200 young veterans (average age = 31 years), we found that among APOE ɛ4 carriers, CBE was significantly associated with spatially heterogenous white matter alterations. This association was specific to CBE relative to more distant blast exposures and other TBI-related variables such as the presence of a lifetime or military-related TBI. Further, we found that the number of CBEs was significantly associated with the number of white matter clusters with reduced FA in APOE ɛ4 carriers, potentially suggesting a dose-effect of CBE. These findings are consistent with recent work showing the relevance of CBE in brain health, 4 and suggests that close-range exposure within 10 m may be a useful marker for blast-related neural changes, particularly when examined in concordance with genetic differences.
PTSD and sleep impairment were highly comorbid with CBE in our sample, a finding that has been observed in other studies, 4,33 and raises a question concerning the specificity of our findings. Nonetheless, our findings were significant when PTSD and sleep impairment were included in the model. Moreover, our analyses revealed that neither PTSD nor sleep impairment was significantly associated with heterogeneous white matter alterations in individuals with the ɛ4 allele.
Our finding that CBE in combination with genetic risk for AD was associated with spatially heterogeneous white matter alterations adds to the emerging literature pointing to the importance of blast exposure in heterogeneous disruptions of white matter integrity, 2,3 and is consistent with previous reports showing white matter abnormalities in the pre-symptomatic and amnestic mild cognitive impairment stages of AD. 34 –37 Our finding extends this work by showing that blast exposure in combination with APOE ɛ4 may be an important risk factor for diffuse alterations in white matter integrity. Research suggests that axonal injury may lead to the accumulation of proteins that form diffuse amyloid β (Aβ) plaques similar to those that appear in early AD. 38 –40 Moreover, APOE ɛ4 has been linked to the propagation and accumulation of misfolded proteins and Aβ 20,38,41 –43 as well as impairments in neuronal recovery following brain injury, including alterations in Aβ clearance and tau-mediated neurodegeneration. 44,45 Our results raise the possibility that CBE may influence processes that work synergistically with neurodegenerative genetic influences to trigger pathological accumulation of misfolded proteins. 9,46
In this study, we did not find a main effect of the presence of TBI or an association between TBI and APOE on spatially diffuse white matter alterations. One possibility for this negative finding is that our TBI measure did not account for sub-concussive blows to the head, which may have adverse consequences on brain health. Recent work has shown that repetitive and sub-concussive injuries without apparent acute symptoms are especially important in neurodegenerative processes. 46,47 Therefore, it is possible that CBE, particularly when combined with genetic risk for neurodegenerative disease, may be a more sensitive marker for sub-clinical but persistent effects on the brain related to potential neurodegenerative processes. Notably, prior work examining the main effects of mild TBI on spatially heterogeneous white matter integrity has found that mild TBI with loss of consciousness is significantly associated with white matter alterations above and beyond the effects of blast exposure alone. 22,23,48 Taken together, these results suggest that although mild TBI with loss of consciousness may be related to negative neural effects alone, blast exposure requires the additive genetic influence to impact white matter integrity. Another possibility for the negative TBI finding is that there may be differences in how primary blast injuries interact with APOE on the brain compared with brain injuries associated with blunt forces. For example, the vasculature may be more vulnerable to blast, 49,50 and mounting evidence suggests that cerebrovascular damage may be a pathological link between neural integrity disruptions and neurodegenerative disease. 51,52 Therefore, it is possible that the observed finding in this study may reflect sensitivity to underlying cerebrovascular damage. However, more research is needed to confirm this hypothesis.
Limitations of this study should be noted. First, this study was cross-sectional and, therefore, we cannot make causal inferences. Therefore, we cannot determine whether any of the individuals in this study will develop AD in the future or whether these structural alterations were present prior to injury. It will be important for future longitudinal work to examine these possibilities. Second, given the small sample size of the study, we may have been underpowered in our analyses, which may have contributed to our negative TBI result as well as our limited subgroup findings when decomposing the interaction. However, our sample size was comparable with previously published studies investigating genetics, clinical conditions, and neuroimaging. 21,53 –55 Further, our subgroup finding is strengthened by the significant effects in the APOE ɛ4 group when examining a dimensional variable of CBE. Nonetheless, it will be important to replicate these findings in larger samples. Third, CBE was based on self-report and may be subject to reporting bias. However, participant reports were guided by a semistructured interview, which is currently the gold standard approach. Fourth, this study only examined white matter disruptions along the TBSS white matter skeleton. However, TBSS has been refined to minimize spurious influences from gray matter and cerebral spinal fluid (CSF), and aims to improve sensitivity and interpretability for DTI multi-subject analyses, which are often composed with the use of standard registration algorithms in DTI. 29 Nonetheless, it will be important for future work to examine white matter disruptions within specified AD-vulnerable brain regions not along the skeleton in association with blast exposure. Fifth, using number of clusters with reduced FA, regardless of size, may have produced unintended results. It is possible that one large cluster may represent more substantial disruption than smaller clusters, which would be obstructed by a metric focused on number rather than size. However, the number of clusters with reduced FA was highly correlated with total volume, suggesting that the number of clusters with reduced FA is sensitive to these larger volumetric disruptions and thereby reduces the concern that this metric is not adequately addressing white matter disruption. Finally, our sample consisted of combat veterans who were predominately male. It is unknown whether these effects will be observable in cohorts consisting primarily of non-military groups exposed to blasts, or females.
Conclusions
In summary, we report that CBE in combination with APOE ɛ4 genotype is associated with spatially heterogeneous alterations in white matter integrity. Given the number of veterans who are returning with blast exposure from the Iraq and Afghanistan wars, these results underscore the importance of examining the long-term consequences of blast exposure and the mechanisms by which it may increase the risk for future neurodegenerative disease.
Footnotes
Acknowledgments
This work was supported by Career Development Award (grant number: 1 IK2 CX001772-01) from the United States Department of Veterans Affairs, Clinical Science Research and Development Service awarded to D.R.S., and the Translational Research Center for TBI and Stress Disorders (TRACTS), a VA Rehabilitation Research and Development National Network Research Center (B9254-C). This work was further supported with resources and the use of facilities at the National Center for PTSD, the Neuroimaging Research for Veterans Center, VA Boston Healthcare System, and the Pharmacogenomics Analysis Laboratory Research and Development Service, Central Arkansas VA Healthcare System, Little Rock, Arkansas. The authors thank the team of investigators at TRACTS for their assistance with data collection and management, and the team at the Pharmacogenomics Analysis Laboratory Research and Development Service. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Author Disclosure Statement
No competing financial interests exist.