
Abstract
Epidural spinal cord stimulation (SCS) is currently regarded as a breakthrough procedure for enabling movement after spinal cord injury (SCI), yet one of its original applications was for spinal spasticity. An emergent method that activates similar target neural structures non-invasively is transcutaneous SCS. Its clinical value for spasticity control would depend on inducing carry-over effects, because the surface-electrode-based approach cannot be applied chronically. We evaluated single-session effects of transcutaneous lumbar SCS in 12 individuals with SCI by a test-battery approach, before, immediately after and 2 h after intervention. Stimulation was applied for 30 min at 50 Hz with an intensity sub-threshold for eliciting reflexes in lower extremity muscles. The tests included evaluations of stretch-induced spasticity (Modified Ashworth Scale [MAS] sum score, pendulum test, electromyography-based evaluation of tonic stretch reflexes), clonus, cutaneous-input-evoked spasms, and the timed 10 m walk test. Across participants, the MAS sum score, clonus, and spasms were significantly reduced immediately after SCS, and all spasticity measures were improved 2 h post-intervention, with large effect sizes and including clinically meaningful improvements. The effect on walking speed varied across individuals. We further conducted a single-case multi-session study over 6 weeks to explore the applicability of transcutaneous SCS as a home-based therapy. Self-application of the intervention was successful; weekly evaluations suggested progressively improving therapeutic effects during the active period and carry-over effects for 7 days. Our results suggest that transcutaneous SCS can be a viable non-pharmacological option for managing spasticity, likely working through enhancing pre- and post-synaptic spinal inhibitory mechanisms, and may additionally serve to identify responders to treatments with epidural SCS.
Introduction
Spasticity is an emergent feature of disordered sensorimotor control resulting from lesions of the central motor system and expressed as involuntary activation of muscles. 1,2 Following a spinal cord injury (SCI), spasticity develops gradually over several months, affects ∼70% of the individuals in the chronic stage, 3 –5 and can manifest as velocity-dependent, abnormal activation of muscles to an externally imposed stretch, 6 as clonus, spasms, continuous muscle activation even in a state of rest, and uncoordinated movement patterns. 7 Spasticity may debilitate residual motor function, contribute to the development of contractures and pain conditions, restrict activities of daily living, disturb sleep, and hamper rehabilitative efforts. 4,5,8,9
Spasticity is caused by lesions of descending brainstem pathways 10,11 and results from the loss of monoaminergic modulation of spinal interneurons and motoneurons 12 –14 as well as from plastic changes at the cellular level to compensate for the lack of these neuromodulators below the lesion. 15 –17 Consequences are a reduced depression of neurotransmitter release from Ia muscle spindle afferents upon their repeated activation, 12,18 –20 hyper-excitability of interneurons that mediate polysynaptic excitation, 17,21 a decrease of the inhibitory capacity of post-synaptic inhibitory circuits, 22,23 and an increase of motoneuronal excitability. 24 –26 Morphological changes in skeletal muscle and connective tissue secondary to spastic conditions may further accentuate resistance to passive stretch. 27 –30
In spite of the clinical and social need, effective management of spasticity has remained a challenge because of its various presentations, the multitude of underlying mechanisms, and the variability of these factors across individuals. 7,9 Current options for the clinical management of spasticity involve, in the first instance, physiotherapy and oral administration of anti-spasticity drugs, and further, chemical neurolysis, intramuscular injections of botulinum toxin, and more invasive approaches such as intrathecal drug pumps or rhizotomy. 7,31,32 These treatments either reduce the afferent transmission to the motoneurons or the efferent drive to muscles. 16,31 Notably, orally administered anti-spasticity agents, the most common treatment, do not act locally within the spinal cord but produce a generalized depression of the central nervous system, often resulting in weakness and dizziness. Further, the modulation of spinal circuits that normally regulate motoneuronal output is generally not the target of current therapies. 16,31 Hence, alternative treatment options are continuously being sought.
The use of epidural spinal cord stimulation (SCS) in recent high-profile studies reporting unprecedented improvements of motor function following severe SCI has triggered a resurgence of interest in the therapeutic potential of this intervention. 33 –35 Remarkably, epidural SCS was originally considered a promising therapy for spasticity in this subject population. 36 –38 Indeed, computational modelling 39,40 and human physiological studies, 38,41,42 as well as microdialysis techniques in animal experiments 43,44 collectively suggest that SCS can recruit local inhibitory spinal circuits trans-synaptically through the stimulation of afferent fibers, and can enhance the release of inhibitory neurotransmitters.
In parallel to our early studies to identify the neural structures electrically activated by epidural lumbar SCS, 45 –47 we developed the method of transcutaneous SCS to target the same neural input structures to the spinal cord non-invasively; 48 that is, predominantly medium-to-large diameter afferent fibers within posterior rootlets/roots. 49,50 In three individuals with incomplete SCI, we previously presented that some manifestations of spasticity were reduced immediately after a single 30 min session of transcutaneous SCS. 51 Others recently reported a decline of stretch-induced quadriceps spasticity 45 minutes after a single 30-minute session of transcutaneous SCS. 52 In fact, transiently persisting therapeutic effects beyond the period of the active intervention are of particular clinical relevance, because as a surface-electrode-based method, transcutaneous SCS cannot be applied chronically, and the stimulation conditions are considerably influenced by changes in body position. 53
The objective of the present study was to gain a comprehensive understanding of the carry-over effects of transcutaneous SCS on various presentations of spinal spasticity. Using multiple assessment measures, we investigated the effects of a 30 min session of transcutaneous SCS on stretch-induced spasticity, clonus, cutaneous-input-evoked spasms, and walking speed immediately as well as 2 h after the intervention in 12 individuals with chronic SCI. Further, we tested for the first time the applicability of transcutaneous SCS as a home-based therapy over a period of 6 weeks and whether multiple stimulation sessions would lead to cumulative and longer-term therapeutic effects in one of the participants.
Methods
Participants
Twelve otherwise healthy adults (41.3 ± 19.1 years, mean ± standard deviation [SD]) with traumatic, chronic SCI (≥ 1 year post-injury) were studied (Table 1). Participants 1, 3, 7, 8, and 10 were taking oral anti-spasticity medication (Table 1) and took the last dose 12–15 h before the experiments. Among the exclusion criteria were active and passive implants at vertebral level T9 or caudally, such as osteosynthesis material. The study was approved by the Ethics Committee of the City of Vienna, Austria, and conducted in accordance with the Declaration of Helsinki. All participants signed written informed consent prior to their participation.
Participants' Data and Neurological Status According to the International Standards for Neurological Classification of Spinal Cord Injury
AIS, American Spinal Injury Association Impairment Scale; LEMS, lower-extremity motor score; LT, light touch; Neurol., neurological; Part., participant; PP, pin prick; WISCI, Walking Index for Spinal Cord Injury.
Study protocols
Carry-over effects of a 30 min session of 50 Hz transcutaneous SCS on spasticity were investigated using comprehensive assessments conducted before (A0), immediately after (A1), and 2 h after (A2) the cessation of the stimulation (Fig. 1A). The assessments at the different time points were identical and comprised, in this sequence, the clinical evaluation of lower-extremity muscle tone using the Modified Ashworth Scale (MAS), 54 the 10 m walk test (if possible) with walking aids as required (same in all three assessments), the Wartenberg pendulum test, 55 and an electromyography (EMG) based evaluation of lower-extremity muscle activation during a set of manual testings. 56,57 In the clinical evaluation, the resistance of a relaxed single joint to movement throughout its full range of motion imposed by an examiner was rated from 0 to 4 according to the MAS. Movements tested were flexion, extension, abduction, and adduction, as well as internal and external rotation of the hip; flexion and extension of the knee with the hip in an extended position; and ankle dorsiflexion with the hip and knee in a flexed position as well as dorsiflexion, plantar flexion, and pronation of the ankle with the hip and knee in an extended position (12 separate tests per side). For the pendulum test, participants were in a supported sitting position with the trunk reclined by ∼30 degrees, while the examiner lifted one leg to a horizontal position, released it, and let it oscillate passively until it stopped. The EMG-based evaluation was conducted with the participants lying supine and included passive unilateral hip and knee flexion-extension movements performed by the examiner (3 sec each for flexion, holding hip and knee flexed at 90 degrees, and extension), the attempt to elicit an Achilles clonus by a brisk manual ankle dorsiflexion, and cutaneous-input-evoked spasms by stroking the foot sole with a blunt rod. The pendulum test, as well as the tests of the EMG-based evaluation, were repeated three times each on both sides, separated by 10 sec phases of relaxation without detectable EMG activity. The assessments were thus selected to evaluate abnormal muscle tone (MAS, pendulum test, and passive-movement segment of the EMG-based evaluation), clonus, and spasms, as well as residual walking function. Between the two post-SCS assessments A1 and A2, the participants rested in their wheelchairs.
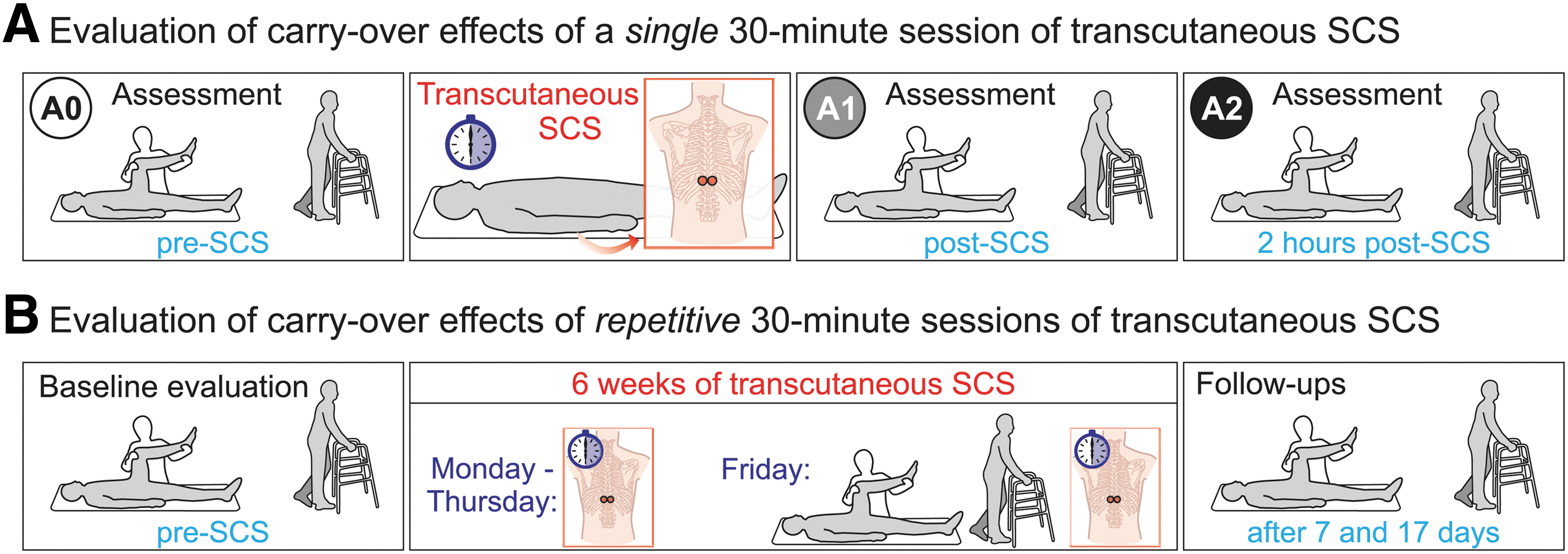
Evaluation of carry-over effects of transcutaneous spinal cord stimulation (SCS) on spinal spasticity and walking speed.
Additionally, in participant 3, the applicability of transcutaneous SCS as a home-based therapy as well as the potential to induce cumulative and longer-lasting therapeutic effects by multiple stimulation sessions over a period of 6 weeks were tested (Fig. 1B), 6 months after his participation in the single-session protocol. Specifically, after an initial baseline evaluation of spasticity, 50 Hz transcutaneous SCS was applied from Mondays to Thursdays for 30 min per day. On Fridays, 24 h after the preceding stimulation session, the participant underwent a re-evaluation of spasticity, followed by another 30 min application of transcutaneous SCS. Stimulation was paused on Saturdays and Sundays. After 6 weeks, transcutaneous SCS was withdrawn and two follow-up evaluations were conducted after 7 and 17 days. The baseline and weekly evaluations as well as the follow-ups included the same tests as the single-session protocol. Additionally, the participant completed a daily questionnaire on the average perceived spasticity using the visual analogue scale, 58 the frequency and intensity of spasms according to the Penn spasm frequency scale, 59 and bladder and bowel function.
Stimulation
Transcutaneous SCS was applied through a pair of self-adhesive hydrogel surface electrodes (each 5 cm in diameter; Schwamedico GmbH, Ehringshausen, Germany) positioned between the T11/T12 spinous processes, left and right to the spine, and a pair of indifferent electrodes (8 × 13 cm each) placed para-umbilically over the lower abdomen. 48,51,60 The electrodes of each pair were interconnected and used as single, larger electrodes. A current-controlled stimulator (Stimulette r2x+, Dr. Schuhfried Medizintechnik GmbH, Moedling, Austria) delivered charge-balanced, symmetrical, biphasic rectangular pulses of 1 ms width per phase. With reference to the abdominal electrodes, the paraspinal electrodes were the anode for the first and the cathode for the second pulse phase. The second phase of the biphasic rectangular pulses was the effective stimulating phase. 50
Electrode placement over the lumbar spinal cord was verified by applying single stimuli to elicit posterior root-muscle (PRM) reflexes 48 in the L2–S2 innervated rectus femoris, biceps femoris, tibialis anterior, and triceps surae muscle group bilaterally with the participants relaxed in the supine position (Fig. 2A). Across participants, the mean threshold (± SD) for the elicitation of PRM reflexes was 49.6 ± 25.1 mA (per phase of the biphasic stimulation pulse), ranging from 16 mA to 100 mA. Stimulation of afferent fibers was tested by applying double stimuli at intervals of 30 ms, 50 ms, and 100 ms, and confirmed by the depression and gradual recovery 61,62 of the responses evoked by the second pulse of each pair of stimuli. 48,63,64
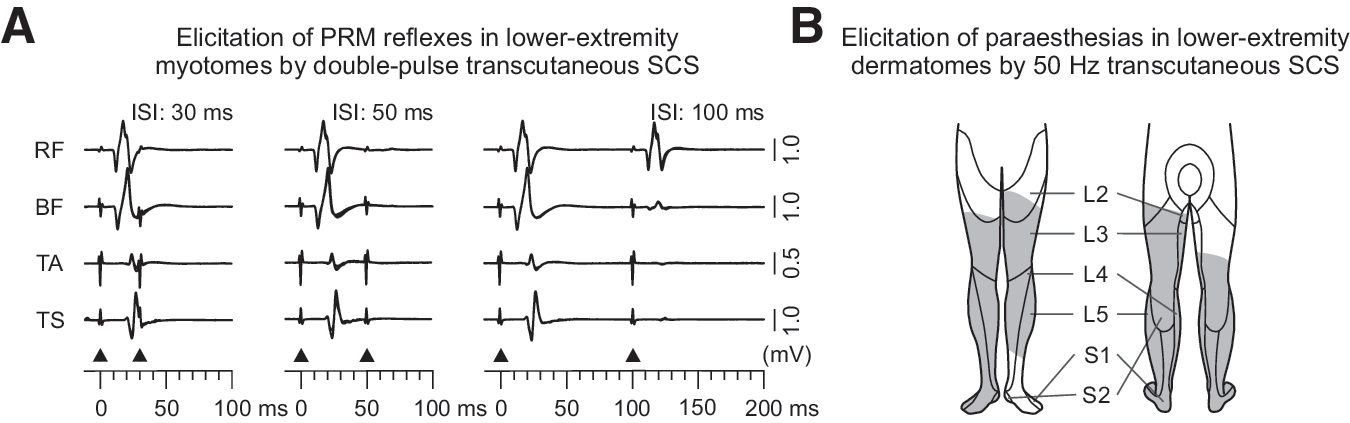
Verification of bilateral L2–S2 afferent fiber stimulation.
Subsequently, the stimulator was set to continuous mode to deliver stimulation at a frequency of 50 Hz, in accordance with previous experience with epidural SCS for spasticity control. 38 With the participants lying supine, the stimulation amplitude was slowly increased from 0 mA to an amplitude that generated distant paresthesias (tingling sensations) in bilateral L2–S2 lower extremity dermatomes but was subliminal to the PRM-reflex threshold (Fig. 2B). The generation of paresthesias was previously used in epidural SCS to guide the effective stimulation amplitude for spasticity control. 37 In participants 10–12 with complete absence of sensory perception below the level of SCI, the stimulation amplitude was set at 90% of the lowest PRM-reflex threshold across muscles. For the 30 min intervention, the stimulation amplitude across participants was 40.8 ± 24.1 mA, ranging from 15 mA to 90 mA.
In participant 3, in whom transcutaneous SCS was repetitively applied for 6 weeks as a home-based therapy, the placement of the paraspinal stimulating electrodes was identified in the baseline evaluation and re-verified in the weekly assessments. For the identification of the correct placement at home, moles and anatomical landmarks on the back were used by the participant's partner. 50 Hz stimulation applied from such site, with an appropriate amplitude induced paresthesias in the lower extremity dermatomes with characteristic, reproducible distribution, which served the participant as feedback for correct stimulation application. During the 6 weeks of repetitive sessions of 50 Hz transcutaneous SCS, the participant applied an average stimulation amplitude of 24.0 ± 4.8 mA.
Data acquisition
EMG was acquired from the rectus femoris, biceps femoris, tibialis anterior, and triceps surae muscle group of both legs with pairs of silver-silver chloride surface electrodes (Intec Medizintechnik GmbH, Klagenfurt, Austria), placed in longitudinal alignment and an inter-electrode distance of 3 cm. 56 Common ground electrodes were placed over the fibular heads bilaterally. Abrasive paste (Nuprep, Weaver and Company, Aurora, CO) was used for skin preparation to minimize signal noise. EMG signals were recorded via instrumentation amplifier (INA 118, Texas Instruments Inc., Dallas, TX), amplified with a gain of 600, filtered to a bandwidth of 10–500 Hz within the analogue front end, and digitized at 2048 samples per second and channel with a USB-NI 6261 data acquisition card (National Instruments Inc., Austin, TX), and recorded using DasyLab 11.0 (Measurement Computing Corporation, Norton, MA). In participants 5, 10, and 11, the Phoenix multi-channel EMG system (EMS-Handels GmbH, Korneuburg, Austria) was used, set to a gain of 502 over a bandwidth of 10–1000 Hz and digitized at 2048 samples per second and channel. All EMG signals were additionally bandpass filtered offline between 10 and 500 Hz using a second order Butterworth filter. For the Wartenberg pendulum test, electro-goniometers (SG150, Penny & Giles Biometrics, Ltd., Gwent, UK) were used to monitor knee joint angles. The goniometer output signals were low-pass filtered to 15 Hz, and digitized at 2048 samples per second.
Data analysis and statistics
Data were analyzed offline using Matlab R2017b (The MathWorks, Inc., Natick, MA) and IBM SPSS Statistics 24.0 (IBM Corporation, Armonk, New York, NY).
Resistance to passive leg movements was clinically graded according to the MAS. 54 A single score, the MAS sum score, was obtained per assessment (A0, A1, A2) by summing the individual scores of the 12 different movements tested per leg (with a value of 1.5 for the 1+ scoring category), resulting in a value ranging from 0 to 96 (0, no increase in muscle tone).
The spasticity index was calculated based on the knee angle of the initial horizontal leg position of the Wartenberg pendulum test
65
(Start), the angle at which the leg reversed for the first time from flexion to extension (Flex), and the final knee resting angle (Rest):
Values ≥1 denote non-spastic conditions, and 0 denotes extreme spasticity. For each assessment (A0, A1, A2), a single index was obtained by averaging the six values (three pendulum tests, two legs).
The time required to walk 10 m was measured and used to calculate the walking speed (m/sec) for each assessment (A0, A1, A2).
The EMG during passive multi-joint movements was evaluated by calculating the total activity of ipsilateral leg muscles as the sum of the root mean square (RMS) values of the EMG of each muscle group from the onset to the offset of the movement (9 sec). Analogously, the EMG of ipsilateral leg muscles in response to the attempt to elicit ankle clonus and cutaneous-input-evoked spasms were evaluated during 3 sec time windows following the onset of each test. For each test (passive movement, clonus, spasms), mean RMS values per assessment (A0, A1, A2) were obtained by averaging the three repetitions on both sides.
To test the hypothesis that a single 30 min session of 50 Hz transcutaneous SCS would ameliorate spasticity from before (A0) to immediately after the application (A1) and that these effects would persist for 2 h (A2), the measures obtained in A1 and A2 were separately compared with those of A0 using the non-parametric Wilcoxon signed-rank test (α = 0.05). To assess potential cumulative effects of repetitive sessions of transcutaneous SCS over a period of 6 weeks in participant 3, the results of each measure taken were ranked from best (rank 1) to worst (rank 9) over the nine evaluations conducted (baseline, six weekly evaluations, two follow-ups), and a mean rank across measures was then calculated for each evaluation. Spearman's rank correlation (α = 0.05) was calculated to evaluate the relationship between rankings and evaluations (thus potentially providing information on the “training effect” of repetitive stimulation sessions).
Results
Carry-over effects of a single 30 min session of transcutaneous SCS
Thirty-minute sessions of transcutaneous SCS at 50 Hz and with the targeted amplitude could be successfully applied in all participants. The stimulation continuously produced mild tingling sensations in the leg dermatomes of the participants with partially preserved sensory function (see Fig. 2B). Local sensory and neuromuscular stimulation beneath the stimulating electrodes was well tolerated by all participants.
The stimulation resulted in several significant improvements of the measures of spasticity that persisted for the duration of data acquisition in the post-SCS assessments (Figs. 3 and 4). Immediately after the intervention (assessment A1 compared with A0), the MAS sum score, clonus, and cutaneous-input-evoked spasms were significantly improved. Two hours post-stimulation (A2 compared with A0), all spasticity measures evaluated were significantly improved. All significant changes met the criteria of large effects sizes.
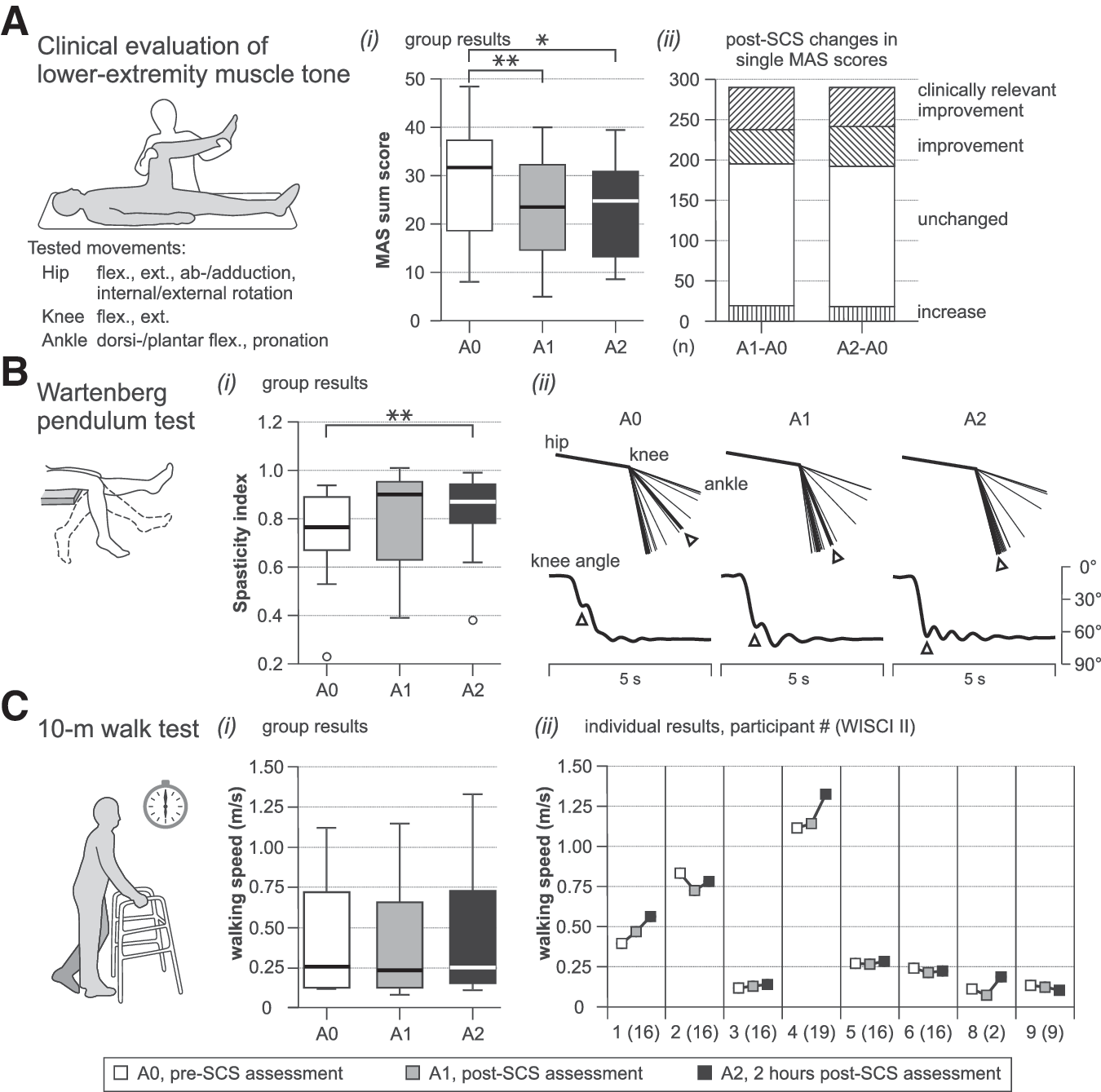
Carry-over effects of a 30 min session of 50 Hz transcutaneous spinal cord stimulation (SCS) on lower-extremity muscle hypertonia and walking speed.
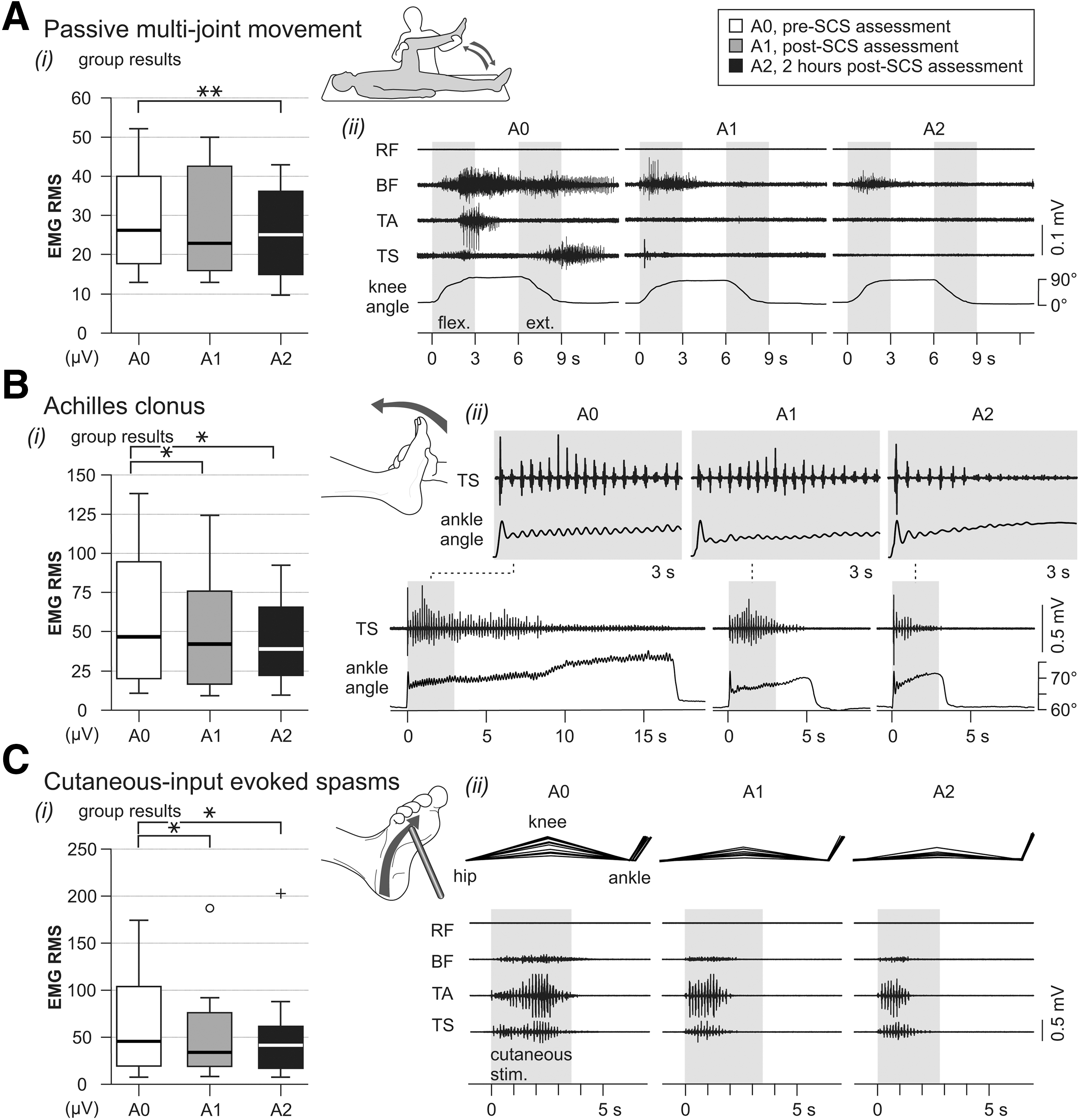
Carry-over effects of a 30 min session of 50 Hz transcutaneous spinal cord stimulation (SCS) on various presentations of spasticity tested by an electromyography (EMG)-based evaluation.
Specifically, the MAS sum score was significantly reduced from A0, median 31.75 (interquartile range [IQR]: 18.63–37.38) to 23.50 (14.63–32.25) in A1 (z = -2.944, p = 0.003, r = 0.850), and to 24.75 (13.25–30.88) in A2 (z = -2.590, p = 0.010, r = 0.748) (Fig. 3A[i]), with a clinically relevant decrease of abnormal muscle tone (i.e., single MAS scores reduced by values of ≥1) 66,67 occurring in each of the participants (Fig. 3A[ii]).
The median spasticity index was 0.765 (IQR: 0.668–0.890) in A0 and 0.900 (0.630–0.953) in A1, showing no statistical difference (z = -1.452, p = 0.146, r = 0.419), and was significantly improved to 0.870 (0.778–0.943) in A2 (z = -2.787, p = 0.005, r = .805) (Fig. 3B[i]), reflecting changes of the swinging movement of the lower leg (Fig. 3B[ii]). Individually, in A1, the angle at which the leg reversed for the first time from flexion to extension showed an increase by ≥12 degrees in six participants, which was previously suggested to be a clinically meaningful difference following an anti-spasticity treatment; 52,68 in one participant, the change was moderate (increases of 6–11 degrees), and mild in two participants (1–5 degrees). In A2, three participants showed a clinically meaningful increase, five showed a moderate increase, and three showed a mild increase.
In the EMG-based evaluation, the median RMS of the EMG activity produced during passive unilateral hip and knee flexion and extension was 26.2 μV (IQR: 17.8–39.8 μV) in A0 and 22.9 μV (15.9–42.7 μV) in A1, showing no statistical difference (z = -0.784, p = 0.433, r = 0.226), and was significantly reduced to 25.2 μV (14.8–36.3 μV) in A2 (z = -2.824, p = 0.005, r = 0.815) (Fig. 4A[i]). The EMG traces in Figure 4A[ii] show abnormal tonic stretch reflexes and reflex spread induced by the imposed movement and their attenuation following the stimulation. The median EMG RMS values of the activity associated with clonus were significantly reduced in both post-stimulation assessments, from 46.9 μV (IQR: 20.2–94.8 μV) in A0 to 42.2 μV (16.7–76.1 μV) in A1 (z = -2.589, p = 0.010, r = 0.747) and to 39.1 μV (22.1–66.0 μV) in A2 (z = -2.589, p = 0.010, r = 0.747) (Fig. 4B[i]). Figure 4B[ii] illustrates an example of sustained clonus evoked by the examiner after rapidly flexing the ankle in A0, whereas an equivalent stretch (see initial deflections in the goniometric traces) applied in A1 induced a shorter-lasting clonus, and only a few beats in A2. The median RMS values of the EMG produced in response to plantar stimulation were significantly reduced from 45.7 μV (IQR: 19.4–103.8 μV) in A0 to 34.0 μV (19.0–76.1 μV) in A1 (z = -2.040, p = 0.041, r = 0.589) and to 41.6 μV (17.0–61.5 μV) in A2 (z = -2.275, p = 0.023, r = 0.657) (Fig. 4C[i]). The attenuated cutaneous-input-induced spasms were also seen as reduced withdrawal movements from the mechanical stimulation (Fig. 4C[ii]).
Eight of the 12 participants were able to complete the 10 m walk test. Across these individuals, there were no changes in the median walking speed from 0.26 m/sec (IQR: 0.12–0.72 m/sec) in A0 to 0.24 m/sec (0.12–0.66 m/sec) in A1 (z = -0.634, p = 0.526, r = 0.224) and to 0.25 m/sec (0.15–0.73 m/sec) in A2 (z = -0.985, p = 0.325, r = 0.348) (Fig. 3C[i]). The individual results showed some noticeable variability, both between participants and between the time points of post-SCS evaluation (Fig. 3C[ii]). The largest relative changes in walking speed were seen in participants 1 and 8. Participant 1 improved by 19% in A1 and by 43% in A2. Participant 8 (with knee and ankle extensor motor scores of 1) critically depended on the considerable tone of his extensor muscles to cover the distance of 10 m in A0, with a walking speed of 0.12 m/sec. In A1, hypertonia was visibly reduced and leg extension during stance was clearly compromised, resulting in a reduced walking speed of 0.08 m/sec. In A2, his ability to perform steps improved and the walking speed increased to 0.19 m/sec, likely related to the reappearance of some critical level of lower-extremity muscle tone. Participant 7 (American Spinal Injury Association [ASIA] Impairment Scale [AIS] C) was unable to complete the test in any assessment, and participants 10–12 had a complete SCI (AIS A), being unable to stand or step.
Applicability of transcutaneous SCS as a repetitively applied home-based therapy
Transcutaneous SCS was repetitively self-administered in a home-based setting for 6 weeks by participant 3 without any complications or intervention-related adverse events. In weeks 2–3 of the stimulation period, the participant was affected by an acute urinary tract infection.
The generation of tingling sensations in the lower extremities, in terms of both the sequence in different leg areas when stimulation amplitude was gradually increased, and the final paresthesia coverage, served the participant as reliable guidance for the correct usage of the stimulation. The participant applied an average stimulation amplitude of 24.0 ± 4.8 mA at home, and the mean PRM reflex threshold identified in the weekly evaluations was 23.9 ± 8.0 mA.
The MAS sum scores of the participant's lower-extremity muscle hypertonia tested clinically in the weekly evaluations showed a strictly monotonous decrease during the stimulation period, a maintained improvement 1 week after withdrawal of the stimulation followed by an increase another 10 days later (Fig. 5A). The evolution of the other outcome measures was less obvious, including some intermittent worsening in weeks 2 and 3 (Fig. 5B–D). Yet, four out of the six outcome measures attained their respective best values in the two last evaluations during the stimulation period (week 5, week 6) as well as the first follow-up (F1) and showed deterioration thereafter. Considering all outcome measures, there was a negative correlation between rankings and evaluation time points (ρ = -0.411, p = 0.002; Fig. 5E), indicating that spasticity improved over the stimulation period. It should be repeated at this point that each evaluation during the stimulation period was conducted 24 h after the preceding stimulation session.
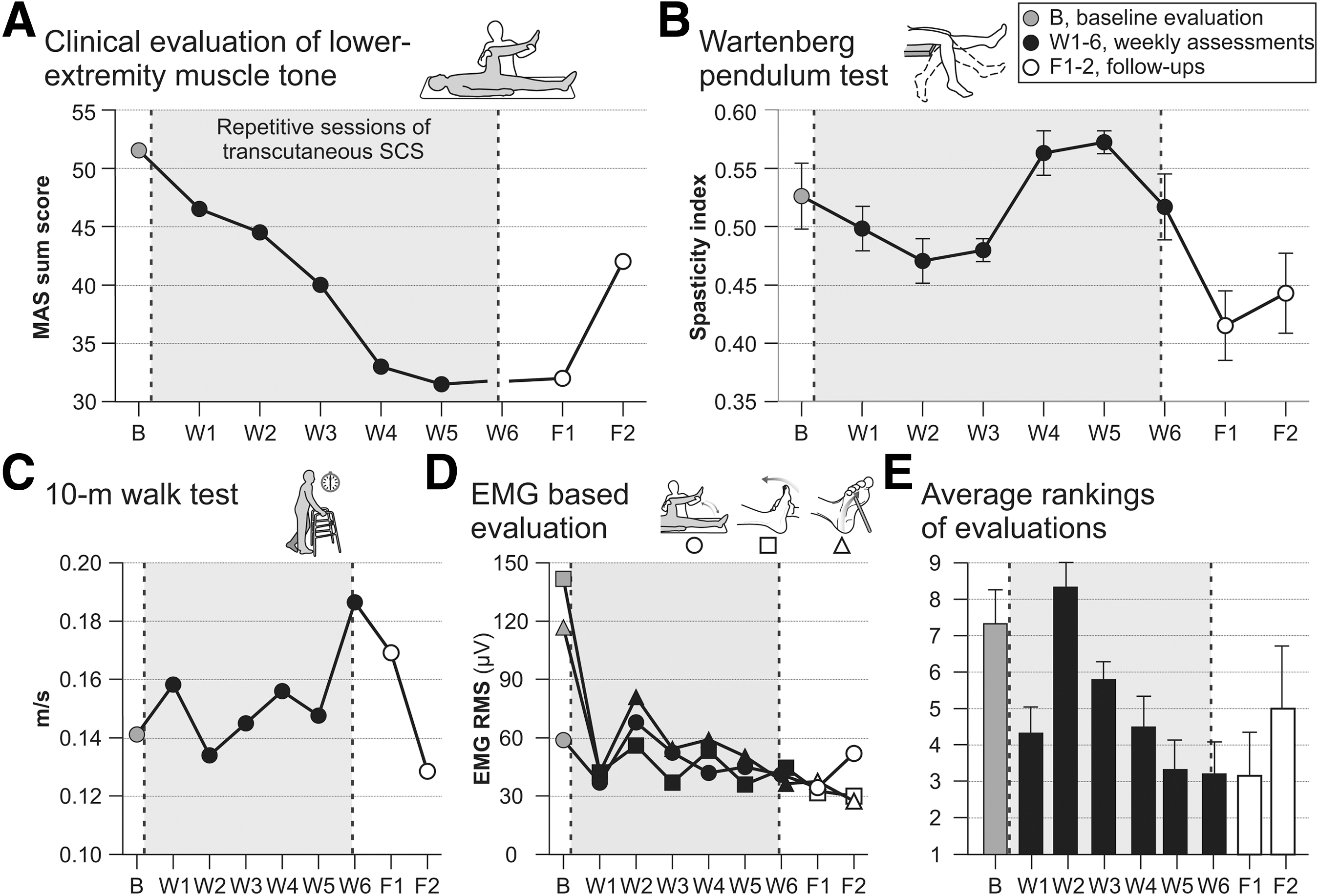
Effects of repetitive 30 min sessions of 50 Hz transcutaneous spinal cord stimulation (SCS) administered over a period of 6 weeks in a home-based setting; participant 3. Results of weekly evaluations of
The participant rated his average perceived spasticity as 65 on the visual analogue scale in the baseline evaluation, and as 50 after the 1st week of stimulation until 10 days after the final stimulation session. Thereafter, the participant assigned scores between 60 and 63, and raised his daily dose of baclofen from 20 mg to 30 mg. There were no effects on frequency and intensity of spasms, with scores of 1, respectively, on the Penn spasm frequency scale throughout the evaluation period. Bladder function (managed by a suprapubic catheter with continuous drainage) and bowel movement remained unchanged.
Subjectively, the participant reported several beneficial effects during the stimulation period, including increased trunk stability, facilitation of upright standing, improved endurance during activities of daily life, and enhanced sensory perception in the soles of his feet. Further, he described effects in his upper extremities, including reduced muscle tone Fig. S1A, the absence of spasms otherwise induced by touching hot surfaces, increased range of movement of fingers and wrists, improved fist closure, and augmented dexterity, including improved handwriting (Fig. S1B).
Discussion
Thirty minutes of 50 Hz transcutaneous SCS improved several measures of lower-extremity spasticity for 2 h post-intervention across 12 individuals with chronic SCI. Because exaggerated stretch reflexes are regarded as the core feature of spasticity, 6,11 three complementary assessment methods were used to evaluate abnormal muscle tone during passive movement. The clinical evaluation using the MAS 54 and testing different joints was applied to obtain a single, comprehensive measure for the overall lower-extremity hypertonia, the MAS sum score. 68 The pendulum test, which correlates with the MAS in persons with SCI, 68,69 was used as a biomechanical method, using gravity to provoke passive stretch for examining the tone of muscles spanning the knee joint. 52,65 The EMG-based evaluation of tonic stretch reflexes tested abnormal tone independently of soft-tissue properties of the muscles. 2,56 These measures were complemented by the assessments of other presentations of spasticity; that is, clonus and muscle spasms, the latter being pathophysiologically distinct from exaggerated stretch reflexes. 17 This thorough set of assessments of the severity of spasticity demonstrated treatment efficacy across participants: 70 the MAS sum score, clonus, and spasms were significantly improved immediately after the intervention, and all spasticity measures were significantly improved 2 h post-intervention. The 10 m walk test was chosen to assess whether alterations in spasticity would impact walking function. Walking speed did not change significantly across participants. Additionally, a single case study showed that transcutaneous SCS could be adequately self-administered without complications over a period of 6 weeks and suggested carry-over effects on spasticity and cumulative improvements over the stimulation period that endured for at least 1 week after withdrawal of the stimulation.
In the following discussion, we will propose that the anti-spasticity effects of transcutaneous SCS were based on the generation of multi-segmental afferent synaptic inputs, which engaged pre- and post-synaptic mechanisms. With the relatively low stimulation amplitudes and high stimulation frequency used, inhibition of spinal reflex circuits outweighed the excitatory actions on motoneuronal activity. We will further briefly reflect on how the stimulation could have provoked the transiently enduring effects. Finally, we will address some methodological considerations.
Neural structures electrically stimulated by transcutaneous SCS
The key characteristics of transcutaneous SCS are the generation of a current flow across the spine at the thoracolumbar junction 48,49,71,72 and the activation of afferent fibers with origins in distant dermatomes and myotomes. 47,50,51,73,74 A fraction of the generated current flows through the vertebral canal, 49 mainly via the ligaments and intervertebral discs. Of all intrathecal neural structures, large-to-medium diameter afferent fibers 75,76 within the posterior rootlets have the lowest excitation thresholds upon entering the spinal cord, because of changes in their spatial fiber orientation with respect to the electric field and the voltage drop at the electrical conductivity boundary between the cerebrospinal fluid and the spinal cord. 45,49,71,77,78 Transcutaneous SCS hence activates similar neural target structures as epidural lumbar SCS. 35,49,50,79
For the intervention, stimulation was applied at 50 Hz with an amplitude below PRM-reflex elicitation, yet generating tingling sensations in multiple lower extremity dermatomes, which reflect the electrical stimulation of A-beta/group II afferents from skin mechanoreceptors. 41,80 As group I afferents have larger diameters than those of group II and therefore lower thresholds for external electrical stimulation, 75 –77 Ia muscle spindle afferents must have been recruited as well, yet only producing volleys subliminal to evoke measurable reflex activation of motoneuron pools. 62,81 This is supported by the detection of anti-dromic potentials in mixed peripheral nerves during epidural stimulation applied over the low-thoracic dorsal columns 41 and lumbar posterior roots, 79 with intensities eliciting paresthesias in the legs without producing visible muscle contractions. Further, the recruitment of group Ia muscle spindle afferents by sensory-level epidural stimulation was demonstrated by monosynaptic facilitation of motoneurons during slight voluntary activity. 41 It can be therefore concluded that tonic transcutaneous SCS as applied here generated afferent volleys in group I and II fibers to lumbar and upper sacral spinal cord segments. In turn, these repetitive afferent inputs likely enhanced intrinsic inhibitory mechanisms in the spinal cord. Indeed, the stimulation parameters were in accordance with previous studies employing epidural SCS to reduce spasticity that had emphasized the importance of applying stimulation amplitudes generating paresthesias in the affected extremities without muscle activation, at frequencies of 50–100 Hz. 37,38
Potential neural mechanisms recruited by transcutaneous SCS underlying the anti-spasticity effects
Pre-synaptic inhibition from homonymous and heteronymous nerves is reduced following SCI in humans, 12,82 as is post-activation depression 18,20 of repetitively activated Ia afferents. 17,83 Dysfunction in these pre-synaptic regulatory mechanisms following SCI thus results in an increased excitatory neurotransmitter release from Ia afferents and likely contributes to the exaggerated stretch reflexes and hypertonia associated with spasticity. 17,19,31 The continuous generation of Ia activity in multiple roots by transcutaneous SCS, especially in those containing afferents from flexor nerves, would increase the level of pre-synaptic inhibition distributed to Ia terminals associated with ipsilateral leg muscles. 41,62,84,85 Further, the repetitive activation of Ia afferents at 50 Hz would profoundly decrease the neurotransmitter release from the activated afferent terminals to motoneurons, and therefore the transmission within the stretch reflex arc. 17,41,83
Post-synaptically acting Ia inhibitory interneurons 86 are effectively activated by Ia muscle spindle afferents. 87 In epidural SCS, the recruitment of reciprocal Ia inhibitory circuits has been suggested by computational modelling 39,40 and by reciprocally organized EMG activities in human physiological studies. 42,88 Tonically increasing the activity of Ia inhibitory interneurons by the stimulation-induced synaptic inputs would reduce the overall excitability of the lumbosacral motoneuron pools. 89 An increase of post-synaptic inhibition would be of further relevance for attenuating spasticity; 90 enhanced activation of persistent inward currents in SCI has been suggested to play a major role in the generation of long-lasting exaggerated reflexes and muscle spasms in response to brief or weak afferent volleys 17,25 in animal 26,91 and human studies. 24,92 –94 Hyperpolarization of the motoneuronal membrane potential through post-synaptic inhibition can deactivate persistent inward currents and hence terminate plateau potentials and self-sustained firing of the motoneurons. 95 –97
The role of the stimulation of afferents from skin mechanoreceptors is less evident, because of their complex connectivity to excitatory and inhibitory interneurons within the lumbar spinal cord. 87 Other electrical stimulation approaches have attributed the reduction of spasticity to the stimulation of cutaneous afferents, 31 yet the exact mechanisms by which these structures exert their effects have not been identified. 98 Various hypotheses were put forward, including the enhancement of reciprocal inhibition 99 and pre-synaptic inhibition, 100 and depression of the propriospinal system. 101
Carry-over effects of transcutaneous SCS
The above discussed pre- and post-synaptic mechanisms triggered by the stimulation-induced afferent activity typically last only from a few milliseconds 71,76 to a few seconds. 62,102 The observed carry-over effects would require temporary alterations of the transmission along the spinal circuits following their repetitive stimulation, but at this stage, we can only speculate about the mechanisms.
Previous studies applying electrical stimulation to peripheral nerves have shown carry-over effects on impaired motor function and spasticity, both with single and repetitive sessions, 99 –101,103–107 but the underlying mechanisms remained unclear. One explanation could be long-term potentiation, 101 an increase in synaptic efficacy resulting from repetitive activation of the synapse that outlasts a conditioning high-frequency stimulation of afferent pathways by at least 30 min. 108 Long-term potentiation was demonstrated between dorsal root afferents and neurons in the spinal cord of rats, 109 but studies have focused on nociceptive pathways. 110 The induction of long-term potentiation requires the depolarization of the post-synaptic membrane, the activation of N-methyl-d-aspartate (NMDA) receptors by synaptically released glutamate, and a temporal coincidence between the post- and pre-synaptic activities. 109
The depolarization of the very proximal portions of lower-extremity afferents by transcutaneous SCS would produce highly synchronized afferent inputs to multiple lumbar and upper sacral spinal circuits, and thus result in a sharp temporal relationship between the post-synaptic activity and the excitatory synaptic inputs, likely mediated through glutamate. 111,112 With the prolonged stimulation at 50 Hz, long-term potentiation could presumably be induced and would increase the transmission in local inhibitory pathways; for example, by strengthening the glutamatergic Ia afferent effect upon the Ia inhibitory interneurons or on the first-order excitatory primary afferent depolarization interneurons. Concurrently, the Ia inhibitory synapse on the motoneuron could be potentiated. 113 Further, the repetitive and highly synchronous neurotransmitter release from the Ia terminals to motoneurons at 50 Hz could result in a prolonged decrease of neurotransmitter release probability from the activated afferents and hence reduce excitatory post-synaptic potentials in target motoneurons, 109 increasing post-activation depression in the spastic individuals.
Finally, repetitively applied sessions of transcutaneous SCS may change further cellular properties by partially reversing long-standing receptor up- or downregulation, enhancing the potassium-chloride cotransporter KCC2 activity and reducing the facilitation of persistent inward currents. 16,23
Ascending effects on cervical spinal cord segments
Striking effects on upper extremity function were reported in early studies employing epidural stimulation of the mid-thoracic spinal cord in multiple sclerosis patients, 114,115 including a near-identical observation of improved handwriting as reported here. 116 In humans, evidence for intraspinal transmission of afferent signals from lower extremity nerves to the cervical spinal cord was provided by the elicitation of ascending inter-limb reflexes in upper extremity muscles in individuals with (motor) complete cervical SCI. 117 –119 These studies proposed long propriospinal pathways that couple the lumbar spinal cord with the cervical enlargement, or sprouting of disrupted sensory fiber branches ascending from the lumbar spinal cord.
Methodological considerations and limitations
The study is neither blinded nor placebo controlled
As with epidural SCS, a patient-blinded study is not realizable with transcutaneous SCS because of the inherent stimulation-induced paresthesias. As for many other non-pharmacological treatments, a sham-intervention without any potential active effect may not exist. 52,120 Importantly, information about the non-intervention-related effects in the present work can be directly inferred from a recent study in which the sham intervention consisted of a brief ramp-up and ramp-down electrical stimulation after which the SCI participants remained reclined with their lower extremities extended for 30 min without any further stimulation. 52 This sham-intervention significantly increased stretch-induced quadriceps spasticity, indicating that immobility in this position even for short durations increases spasticity in SCI individuals.
Stimulation parameters were not optimized individually
In applications of epidural SCS in spinal spasticity, the stimulation parameters are individually adapted, often within a trial phase, which can last up to 2 weeks to optimize the attainable therapeutic outcomes. Effective stimulation frequencies vary individually between 50 and 100 Hz. 37,38 In the present study, we had chosen to test the same stimulation frequency of 50 Hz across all participants. It can be assumed that in clinical applications, individually tailored parameter settings could further enhance the effects of transcutaneous SCS. Two interconnected horizontally placed paraspinal electrodes were used in the present study because of the original electrode setup for transcutaneous SCS. 48 The idea was to later utilize this setup for field steering, but asymmetrical stimulation then never appeared to be a critical issue. We would hence suggest a single stimulating electrode placed midline over the spine for future studies.
Use of anti-spasticity medication
It is not trivial to suspend anti-spasticity medication for a longer period of time in study participants, considering the direct impact on their quality of life. Five of the 12 participants were taking oral anti-spasticity medication and took the last dose 12–15 h prior to the experiments. With the exception of tetrazepam (used by a single subject), the half-lives of the medications taken are relatively short (∼ 2–4 h), hence drug effects on the study assessments must have been negligible. Any residual effects would have affected the baseline assessments (A0) the most, because the elimination is a logarithmic function in time, therefore resulting in an underestimation of the transcutaneous SCS effects.
Variability in functional outcome
We had chosen the 10 m walk test to explore the effect of the modification of spasticity on function. 70 Influences on functional tasks following an intervention aimed at reducing spasticity are complex, and modification in spasticity can have positive or negative effects in individuals with different levels of injury severity and different profiles. For individuals with low lower extremity motor scores, hypertonia in extensors can assist with weight bearing, whereas resistance in joint movement or restricted active range of motion would be detrimental for those with some capacity to ambulate. 32,70,121 This complexity was reflected in our data. Our personal experience was also that participants with chronically adopted walking strategies had difficulties adapting to the acute changes in spasticity, including changes in their overall posture. An improvement in the effects of transcutaneous SCS on ambulation could be realized by individual optimization of the stimulation parameters 60,122 or by multiple applications of the intervention. 120,123 Alternatively, single applications of transcutaneous SCS could be used just before dedicated locomotor rehabilitation sessions to adjust the individual spasticity level.
Limitation of the single case multi-session study
The single case study exploring the applicability of transcutaneous SCS as a repetitively applied home-based therapy had no long-term baseline or control data. Yet, several measures of lower extremity spasticity clearly worsened after withdrawal of the stimulation, following improvements during the active stimulation period, suggesting a causal relationship of the changes in spasticity to the intervention. Further, improvements in upper extremity function happened with no expectation bias either by the rater or the subject. Therefore, we believe that sharing our early experience with this protocol would be useful for planning future studies that will focus on multi-session effects of transcutaneous SCS.
Conclusion
By using a comprehensive test-battery approach, we have shown that transcutaneous lumbar SCS can decrease various presentations of spinal spasticity for at least 2 h beyond a single application. A single case study further suggested that administration of the stimulation over a longer period of time is feasible and safe in a home-based setting. The anti-spasticity effect of transcutaneous SCS with relatively low stimulation amplitude and high stimulation frequency is based on the generation of multi-segmental afferent synaptic inputs, which likely enhanced the intrinsic inhibitory mechanisms in the spinal cord. Activation of the spinal cord circuits to normalize reduced inhibition appears to be a more natural method of alleviating spasticity than anti-spasticity medication, and would not cause sedation and dizziness. Compared with other non-pharmacological interventions, the equipment is affordable and accessible, the time required for a therapist to apply the intervention would be short, and advantages could be in the treatment of diffuse types of spasticity 31 as well as in a longer duration of the induced carry-over effects. 52 Finally, transcutaneous SCS could be used to identify responders to the treatment of spasticity with epidural stimulation to justify the invasiveness and higher costs of the implantable system.
Footnotes
Acknowledgments
We acknowledge the continuous support of Wolfgang Drexler, Head of the Center for Medical Physics and Biomedical Engineering, Medical University of Vienna, Austria. We also offer special thanks Peter Lackner, Head of the Neurological Center, SMZ Baumgartner Hoehe, Otto-Wagner-Hospital, as well as Edith Bem and the entire physical therapy team, Neurological Center, SMZ Baumgartner Hoehe, Otto-Wagner-Hospital, Vienna, Austria. This work was supported by the Vienna Science and Technology Fund,
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.