
Abstract
The objective of this study was to systematically review the literature and perform a meta-analysis of randomized controlled trials (RCTs) on the effectiveness of pharmacological and non-pharmacological interventions for depression in patients with moderate-to-severe traumatic brain injury. Databases searched were: Embase, PubMed, PsycInfo, Cochrane Central, Web of Science, and Google Scholar. Depression score on a self-report questionnaire was the outcome measure. Outcomes were collected at baseline and at the first follow-up moment. Data extraction was executed independently by two researchers. Thirteen RCTs were identified: five pharmacological and eight non-pharmacological. Although not all individual studies had significant results, the overall standardized mean difference (SMD) was −0.395, p ≤ 0.001, indicating that interventions improved the depression scores in patients with TBI. The difference in effectiveness between pharmacological interventions and non-pharmacological interventions was not significant (ΔSMD: 0.203, p = 0.238). Further subdivision into methylphenidate, sertraline, psychological, and other interventions showed a significant difference in effectiveness between methylphenidate (ΔSMD: −0.700, p = 0.020) and psychological interventions (reference). This difference was not found if other depression outcomes in four of the included studies were analyzed. The SMD of low-quality studies did not differ significantly from moderate- and high-quality studies (ΔSMD: 0.321, p = 0.050). Although RCTs targeting interventions for depression after TBI are scarce, both pharmacological and non-pharmacological interventions appear to be effective in treating depressive symptoms/depression after moderate-to-severe TBI. There is a need for high-quality RCTs in which the add-on effects of pharmacological and non-pharmacological interventions are investigated.
Introduction
Worldwide, traumatic brain injury (TBI) affects an estimated 69 million people annually, of which 81% will have mild, 11% moderate, and 8% severe TBI. 1 Mood disorders are a frequent complication of TBI, with depression occurring between 7–63% of the time, depending on diagnostic criteria, severity of TBI, selected population, and time post-onset. 2 Most depressive episodes will occur in the first year after injury but even decades afterwards patients remain at risk. 3,4 This makes depression the most common psychiatric disorder after TBI that interferes with rehabilitation, is a major predictor of poor psychosocial outcome, and increases the risk of suicidality and acting out behavior. 3,5 –7 Post-traumatic depression may be explained by the injury itself and by psychosocial factors. An inverse dose–response relationship has been described, with higher rates of depression among patients with mild TBI than among patients with severe TBI. Alderfer and colleagues 8 describe that the left dorsolateral prefrontal cortex and left basal ganglia are regions of interest in the neurobiology of post-traumatic depression and depict an array of psychosocial pre- and post-injury factors that relate to post-traumatic depression. Treatment of post-traumatic depression may therefore focus on neurobiological mechanisms, psychosocial factors, or a combination of these.
Because of depression's detrimental effect, treating depression after TBI is pivotal. However, well-designed trials on treating post-traumatic depression are scarce. This study therefore aims to evaluate the effectiveness of pharmacological and non-pharmacological interventions for post-traumatic depression.
Pharmacological treatments are defined as interventions in which solely pharmacological agents are used that may include antidepressants or psychostimulants. 9 –13 Non-pharmacological interventions include psychosocial therapies, such as motivational interviewing and cognitive behavioral therapy, 14 –18 but also exercise programs and neurofeedback, which are discussed separately. 19 –21
Multiple meta-analyses have been published on pharmacological treatments for depression after TBI, which include both single-group, pre–post intervention studies and randomized controlled trials (RCTs). For example, Salter and colleagues 22 included nine clinical trials in a meta-analysis, of which three were RCTs. Participants had predominantly mild-to-moderate TBI. Pharmacotherapy was associated with a significant reduction in depressive symptoms within the intervention groups, and also in comparison to placebo groups. Because of the small number of RCTs, the authors were cautious about these conclusions. 22 Slowinski and colleagues 23 included 12 studies on pharmacotherapy in depression after mild to severe TBI in their meta-analysis. Overall, a mild to moderate effect size was found in pre–post designs. However, when focusing on the seven studies with a control group, this effect disappeared. 23 This is in line with three other pharmacological meta-analyses 24 –26 in which RCTs were included. No significant effect of antidepressants on depression after TBI was found in any of these studies.
Also, several meta-analyses on psychosocial interventions have been published. Gertler and colleagues 27 investigated the effectiveness of non-pharmacological interventions for depression in adults and children with TBI. They included six RCTs on various interventions, including cognitive behavior therapy, supportive psychotherapy, mindfulness-based cognitive therapy, a supervised exercise program, and repetitive transcranial magnetic stimulation. No compelling evidence was found in favor of any of these interventions. 27 Stalder-Lüthy and colleagues 28 investigated the effectiveness of psychological interventions in long-term rehabilitation after acquired brain injury (ABI) including strokes and TBI. In a pre–post analysis, 13 studies were included, of which seven RCTs were eligible for a meta-analysis. The conclusion was that psychological interventions are promising treatment options for depressive symptoms in long-term rehabilitation after ABI, but that more RCTs are required. 28 Only two RCTs in TBI were included in this meta-analysis, which did not show significant improvement of depression. Liu and colleagues 29 performed a systematic review on two RCTs and one non-randomized controlled trial, focusing on either mindfulness-based cognitive therapy or cognitive behavioral therapy compared with usual care (n = 2) and supportive therapy (n = 1). No significant effect was found in favor of these therapies. 29 The effectiveness of physical exercise as an intervention for reducing depression in patients with TBI was studied by Perry and colleagues. 30 Nine studies, of which two were RCTs, were included. The settings and interventions varied between studies. A small-to-medium positive overall effect was found in the pre–post analysis, but in the two RCTs the pooled effect of exercise on depression was not significant. 30
One systematic review 31 included both pharmacological research and non-pharmacological research, but until the current study, a meta-analysis has not been performed. Fann and colleagues 31 included 26 studies with all kinds of designs, including case reports, open trials, RCTs, and non-randomized trials. Based on this systematic review, serotonergic antidepressants and cognitive behavioral therapy (CBT) seemed to be the most promising interventions for treating depression following TBI. In line with other research, the authors concluded that there is a need for more RCTs in patients with TBI. 31
From the above, it is clear that to date, no meta-analysis of RCTs has been published that studied effects of pharmacological and non-pharmacological interventions, with the result that both types of interventions cannot be compared directly. The purpose of this meta-analysis of RCTs, therefore, is to compare the effectiveness of pharmacological and non-pharmacological interventions for depression in patients with TBI. In the Netherlands, patients with moderate-to-severe TBI are often admitted to post-acute rehabilitation programs, whereas patients with mild TBI are referred to community-based programs. This article therefore focuses on moderate-to-severe TBI.
Methods
Inclusion/exclusion criteria
Randomized controlled trials (RCTs) addressing the effectiveness of subacute and long-term interventions (any treatment modality) for depression or depressive symptoms were included. A study met this criterion if having a depression was an inclusion criterion or if reducing depression/depressive symptoms was the main aim of the study. Any comparison group was possible. The target population needed to include patients with moderate-to-severe traumatic brain injury, age ≥16 years old at time of injury. Studies examining a patient sample with brain injuries other than TBI were included if data of patients with TBI were reported separately. The same holds for studies with both patients <16 and ≥16 years old. The primary outcome was depression score on a self-report questionnaire, such as the Center for Epidemiologic Studies Depression Scale, or an observational scoring instrument, such as the Hamilton Depression score. Studies were included if baseline and follow-up depression scores were reported for both the intervention and control group. Only full text articles written in English were included; data solely published in meeting abstracts were excluded.
Studies examining interventions focusing solely on patients with mild TBI or on prevention of depression were excluded, as well as studies in which all respondents had post-traumatic stress disorder. Also, studies with fewer than 10 participants or fewer than five per group were excluded.
Search strategy
A biomedical information specialist from our institution was consulted for setting up a search strategy to identify studies that examined interventions for depression after TBI, that were published from databases inception until February 1, 2017, and updated on September 11, 2018. Search terms included combinations of brain injury, depression, and controlled clinical trials, limited to human studies and English language. The comprehensive search strategy is presented in Supplementary Data S1. Databases searched were: Embase, Medline EPub, PsycInfo, Cochrane Central, Web of Science, and Google Scholar. In addition, references of previously published meta-analyses were searched by hand.
Data extraction
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 32 were followed. Using a standardized data extraction form, the following study characteristics were collected: total number randomized, total number analyzed, mean age, male/female ratio, TBI severity, time post-onset, and details of the intervention and control group (group size, type, duration, intensity of intervention). As outcomes for the intervention- and control group(s), the raw baseline and post intervention depression scores were extracted (means and standard deviations) or calculated from data or figures presented in the study. If the study consisted of three randomized study arms, investigating two intervention groups and one control group, the data were extracted separately for each intervention group. Data were independently extracted by two reviewers (MH and LP). If there was disagreement between the reviewers, this was resolved by discussion or, if necessary, by a third reviewer (GR).
Quality assessment
A risk of bias assessment was performed independently by two researchers (MH and LP). Domains evaluated were random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment, (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias) from the Cochrane Collaboration's tool for assessing risk of bias. 33 Disagreement between researchers was resolved by discussion. Each domain was classified as low, high, or unclear risk. High and unclear risk of bias were converted into a quality score of 0 points and low risk of bias in a quality score of 1 point. A total score was calculated for each study, ranging from 0 to 6. A higher score means higher quality. We classified studies with a total score <3 as low quality, a score of 3 or 4 as moderate, and a score of 5 or 6 points as high quality.
Statistical analysis
Changes in the depression score over the intervention period were extracted or calculated from baseline and the post-intervention score for both the intervention and control groups. Because the scales of the depression outcome measures varied between the included studies, standardized mean differences (SMDs) were calculated (Hedges' g). SMDs are reported with a 95% confidence interval and significance level; p values <0.05 were considered significant in all analyses. Meta-analyses were performed to examine the effectiveness of pharmacological and non-pharmacological interventions for depressive symptoms/depression in combination and separately. Subgroup analyses were performed for methylphenidate, sertraline, psychological interventions and “other” non-pharmacological interventions and for low-quality and medium-high quality studies. In meta-regression analyses, the differences in effectiveness between the types of intervention and between the quality levels were analyzed. If studies used more than one outcome measure for depression, all analyses were repeated replacing these outcome measures to study the effect of different measurement instruments. Random effects were used to deal with potential heterogeneity. Further, an I2 test was performed to test whether heterogeneity was present. The following cut-offs were used for interpretation of the SMDs; small effect 0.2–0.3, medium effect 0.3–0.8 and large effect >0.80. A “leave-one-out” meta-analysis was performed to test the influence of a single study on the overall effect size. All meta-analyses were performed using the open-source software OpenMeta[Analyst] downloaded from
Results
Study selection
The total search in multiple databases yielded 5176 studies. After de-duplication, 3072 studies remained. After a first selection based on title and abstract, 106 studies were screened in full-text. Of those, 12 were included in the meta-analysis: five were pharmacological 9 –11,13 and eight were non-pharmacological RCTs. 14 –21 We found one extra pharmacological study by hand search. 12 Three studies included a three-arm RCT, each comparing two interventions groups with one control group, of which two were non-pharmacological 16,17 RCTs and one was pharmacological. 9 Thus, the total of 13 studies resulted in 16 intervention groups. A flowchart of the study selection procedure is presented in Figure 1.
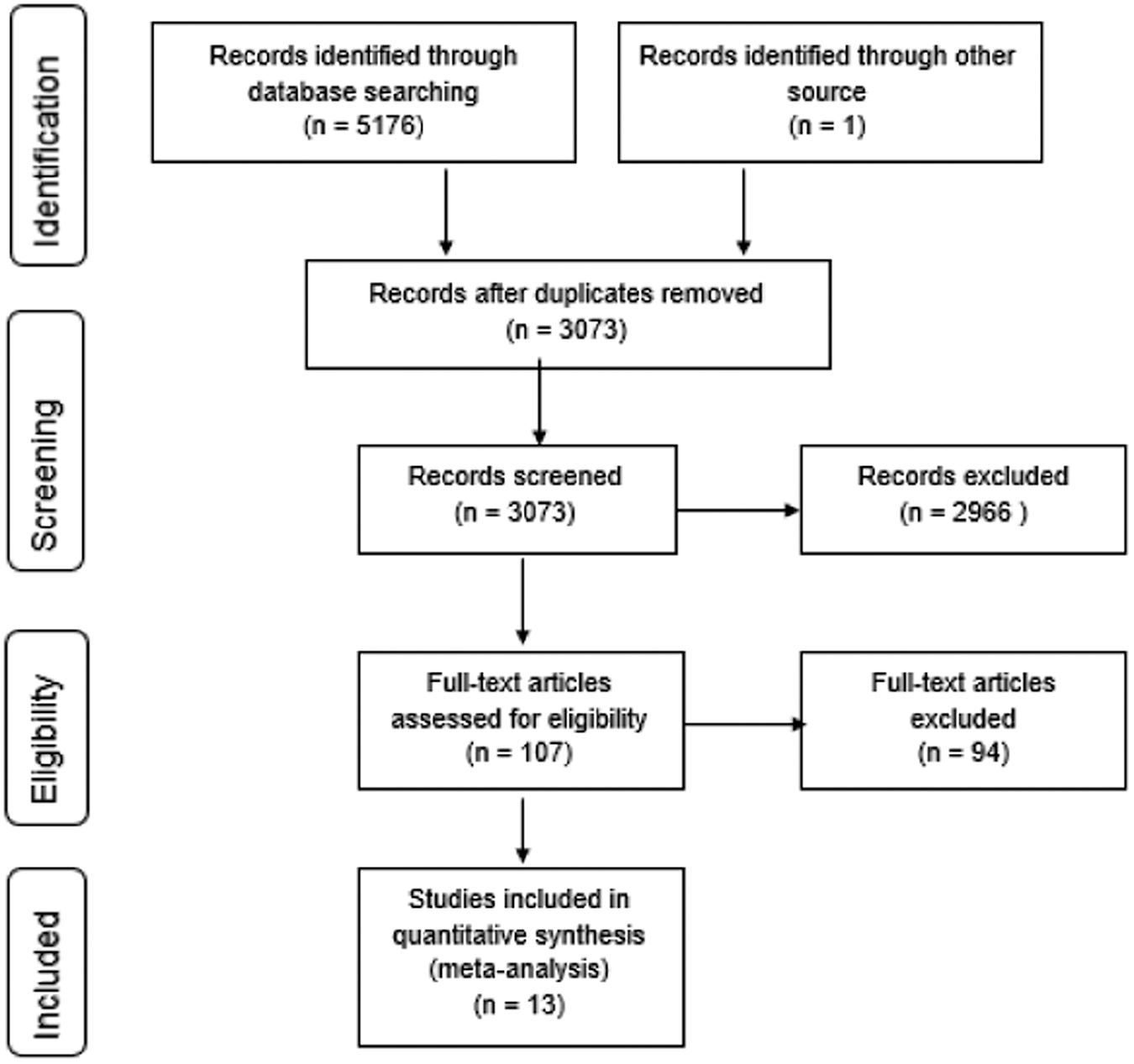
Flowchart of study selection.
Study characteristics
Study characteristics are listed in Table 1. The total sample size was 659, the study size varied between 12 and 100 participants. Although studies that included solely patients with mild TBI were excluded, the severity varied widely between studies. In one study 75% of the participants had mild TBI. 19 In another study, the mean coma duration was 36.9 days, indicating severe TBI. 14 The studies included participants with mean ages ranging from 29.7 to 49.1 years. The time post-injury varied from 14.0 days to 17.7 years. Intervention duration varied between 4 and 36 weeks. Several depression outcomes were used: Beck Depression Inventory (BDI), Hospital Anxiety and Depression scale (HADS), Hamilton Rating Scale for Depression (HAMD), Patient Health Questionnaire (PHQ-9), Brief Symptom Inventory-Depression scale (BSI-D), the Profile of Mood States-Depression scale (POMS-D), Patient-Reported Symptom Checklist-20 (SCL-20), Depression, Anxiety and Stress Scale –Depression scale (DASS-D), Katz Adjustment Scale-Withdrawn Depression subscale (KAS-D). A higher score on each of these scales means more depressed/more depressive symptoms. Seven studies 9 –13,15,16 included solely patients with depression, one study included patients with depression or anxiety, 17 and four studies had no inclusion criteria about the presence of depression in their patients. 14,19 –21 Patients included in the study conducted by Bombardier and colleagues 18 were not required to experience problems with depression, but a subgroup analysis was performed in patients with depression.
Characteristics of the Studies Included in the Systematic Review and Meta-Analysis
Subgroup of 37 depressed patients out of 146 participants.
TBI, traumatic brain injury; SD, standard deviation; BDI-II, Beck Depression Inventory-II; Mod, moderate; Sev, severe; HAM-D, Hamilton Rating Scale for Depression; CBT, Cognitive Behavioral Therapy; PHQ-9, Patient Health Questionnaire-9; NR, not reported; SCL-20, Patient-Reported Symptom Checklist-20; reh, rehabilitation; tx, treatment; KAS, Katz Adjustment Scale; SPT, Supportive Psychotherapy; CBT-T, Cognitive Behavioral Therapy-Telephone; CBT-IP, Cognitive Behavioral Therapy-In Person; MI, Motivational Interviewing; NDC, Non-Directive Counseling; FNS, Flexyx Neurotherapy System; NS, not specified; DASS-D, Depression, Anxiety and Stress Scale-Depression scale; BSI-D, Brief Symptom Inventory-Depression scale; POMS-D, Profile of Mood States-Depression scale; CES-D, Center for Epidemiological Studies-Depression scale.
In four of five pharmacological studies, placebo was used as control intervention. 9 –11,13 The control group in Ansari and colleagues 12 did not receive placebo or any other treatment. Two non-pharmacological studies compared the intervention with usual care 16,18 and two had a waitlist control group. 17,19 In the remaining four studies, the control intervention concerned supportive psychotherapy, 15 nutrition control group, 21 vocational rehabilitation class, 20 and day treatment. 14
Meta-analysis
For each study, baseline and post-intervention outcomes per group are presented in Supplementary Table S1. The results of the meta-analysis are presented in Figure 2. A significant SMD of −0.395 (p < 0.001) was found, which is a moderate negative effect size favoring the interventions for depression overall. A negative effect size means that participants in the intervention groups had significantly greater reduction in depression outcomes over the intervention time, compared with participants in the control groups. With a non-significant I2, heterogeneity was not significant. Subgroup analyses were performed for pharmacological and non-pharmacological interventions (Fig. 2). Again, there was no significant heterogeneity. For both subgroups, the overall intervention effect was significant, but no significant difference was found between pharmacological and non-pharmacological interventions in the meta-regression analysis (Table 2).
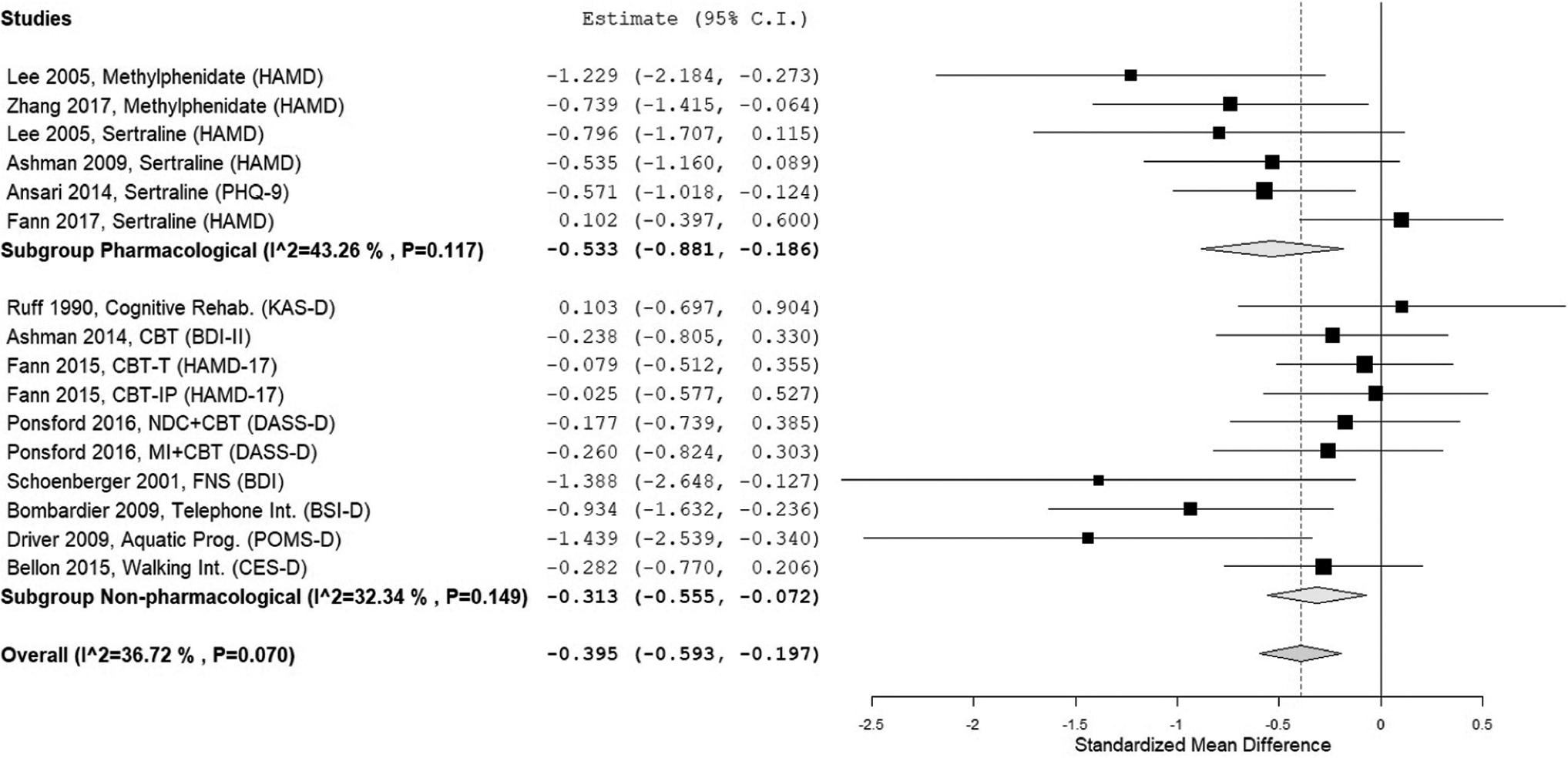
Results of the meta-analysis for subgroups of pharmacological and non-pharmacological interventions.
Meta-Regression Analyses on Subgroups Focused on HAMD versus BDI and SCL-20
p < 0.05
HAM-D, Hamilton Rating Scale for Depression; BDI, Beck Depression Inventory; SCL-20, Patient-Reported0 Symptom Checklist-20; SMD, standardized mean difference, confidence interval.
A subgroup analysis was performed in which interventions were divided in methylphenidate, sertraline, psychological, and “other” non-pharmacological interventions (Fig. 3A). Significant intervention effects of methylphenidate, sertraline and “other” non-pharmacological interventions were found, but the effect of psychological interventions was not significant compared with the control interventions. No significant differences were found between the types of interventions, except for methylphenidate, which was significantly more effective than psychological interventions (Table 2).

Results of the meta-analysis for subgroups of methylphenidate, sertraline, psychological interventions and other interventions with focus on different outcome measures:
The meta-analysis for the total group and the meta-regression analyses were performed twice because four studies used two outcome measures for depression. 9,10,13,16 HAMD was entered in the first analysis, and SCL-20 and BDI in the second analysis. With an overall significant SMD of −0.339 (p < 0.001), the effect size became a little smaller in the second analysis, but still in the moderate range (Fig. 3B). In line with the first analysis (on HAMD) of pharmacological versus non-pharmacological interventions, significant intervention effects were found for both subgroups, but no significant difference between the two types of intervention (Table 2). Focusing on SCL-20 and BDI instead of the HAMD for the four types of intervention (Fig. 3B), significant intervention effects were found for psychological and “other” non-pharmacological interventions. No significant differences in effectiveness were found between the four subgroups, which means that the difference between methylphenidate and psychological interventions, which were found in the first analysis focusing on the HAMD, disappeared (Table 2).
Leave-one-out analysis
To test the influence of a single study on the overall effect size, a “leave-one-out” analysis was performed. As shown in Figure 4, none of the single studies affected the significance of the overall effect size, which indicates that the moderate effect size is robust.
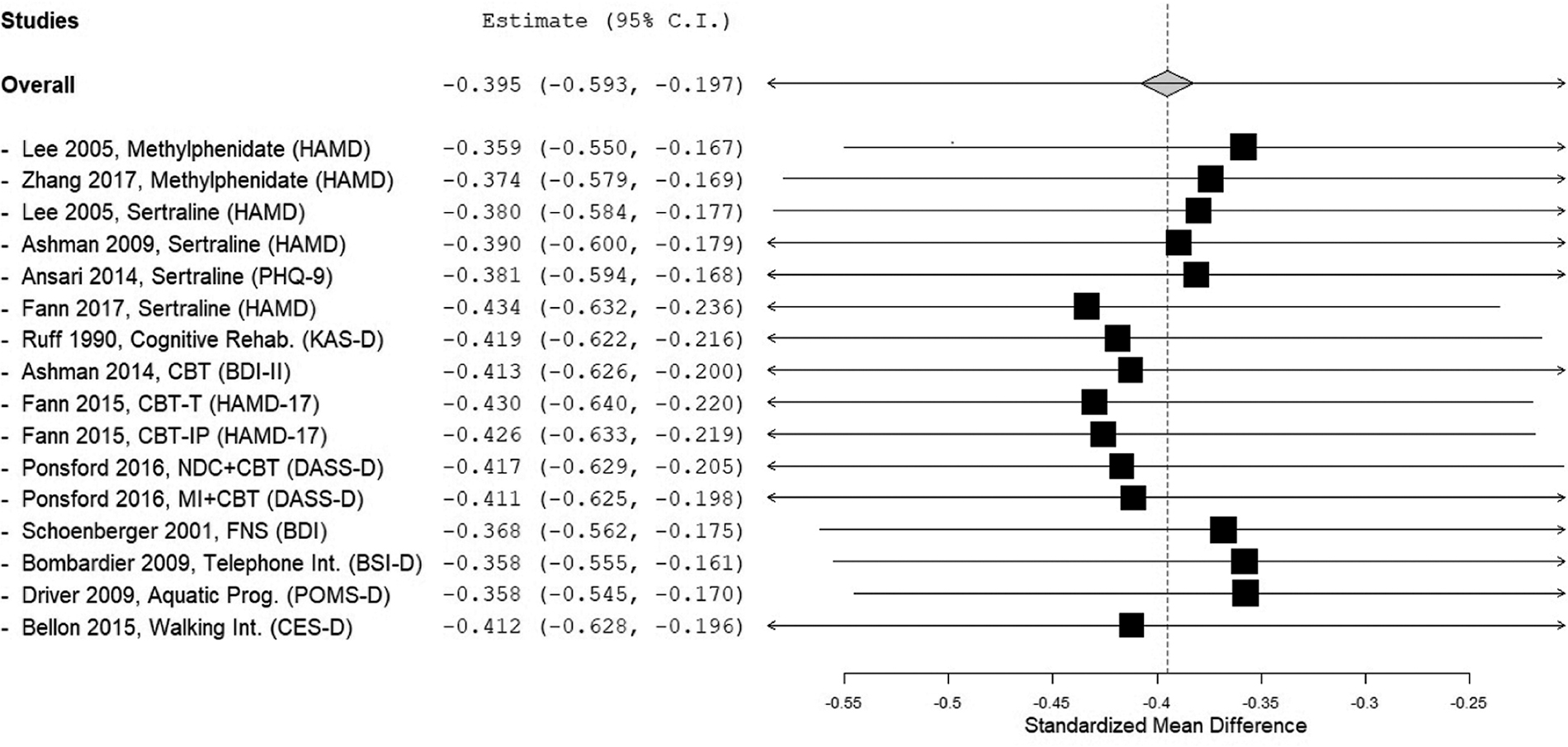
Results of leave-one-out meta-analysis.
Risk of bias assessment
The results of risk of bias assessment are presented in Figure 5. Five studies had a total score of 5 out of 6, 10,11,13,15,16 one study had a total score of 4 out of 6, 17 and another study 3 out of 6. 18 We classified these studies as moderate-to-high quality. Studies with a total score of 0, 1, or 2 out of 6 were classified as low-quality studies. 9,12,14,19 –21 We performed a subgroup analysis for moderate-high versus low-quality studies (Fig. 6). The meta-regression analysis showed that the difference between the effect size of low-quality studies and moderate- and high-quality studies was borderline significant (Table 2). If HAMD was replaced by SCL-20 or BDI in four studies, no significant difference between low-quality studies and moderate-high quality studies was found (Table 2).
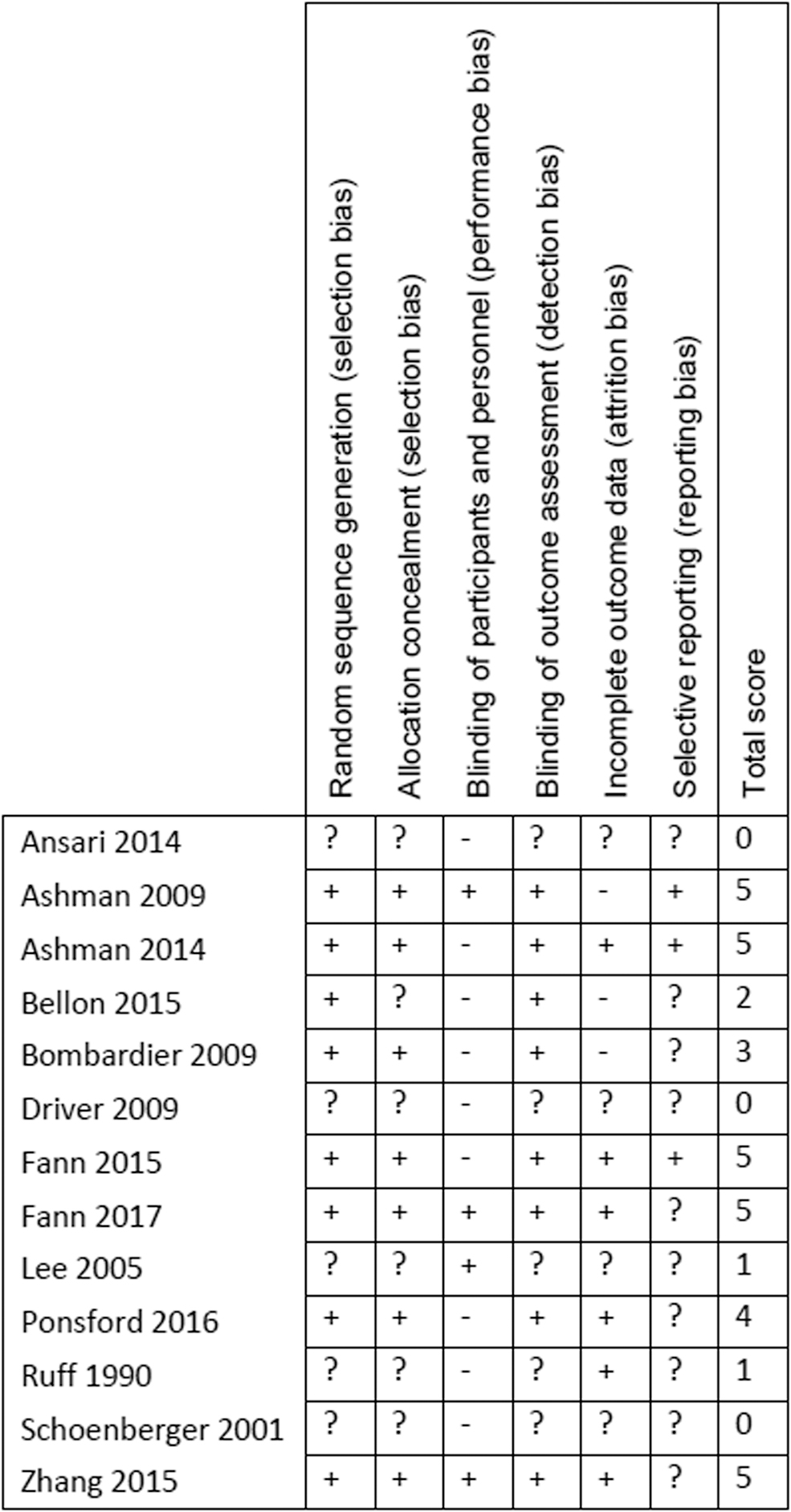
Outcomes of risk of bias assessment.
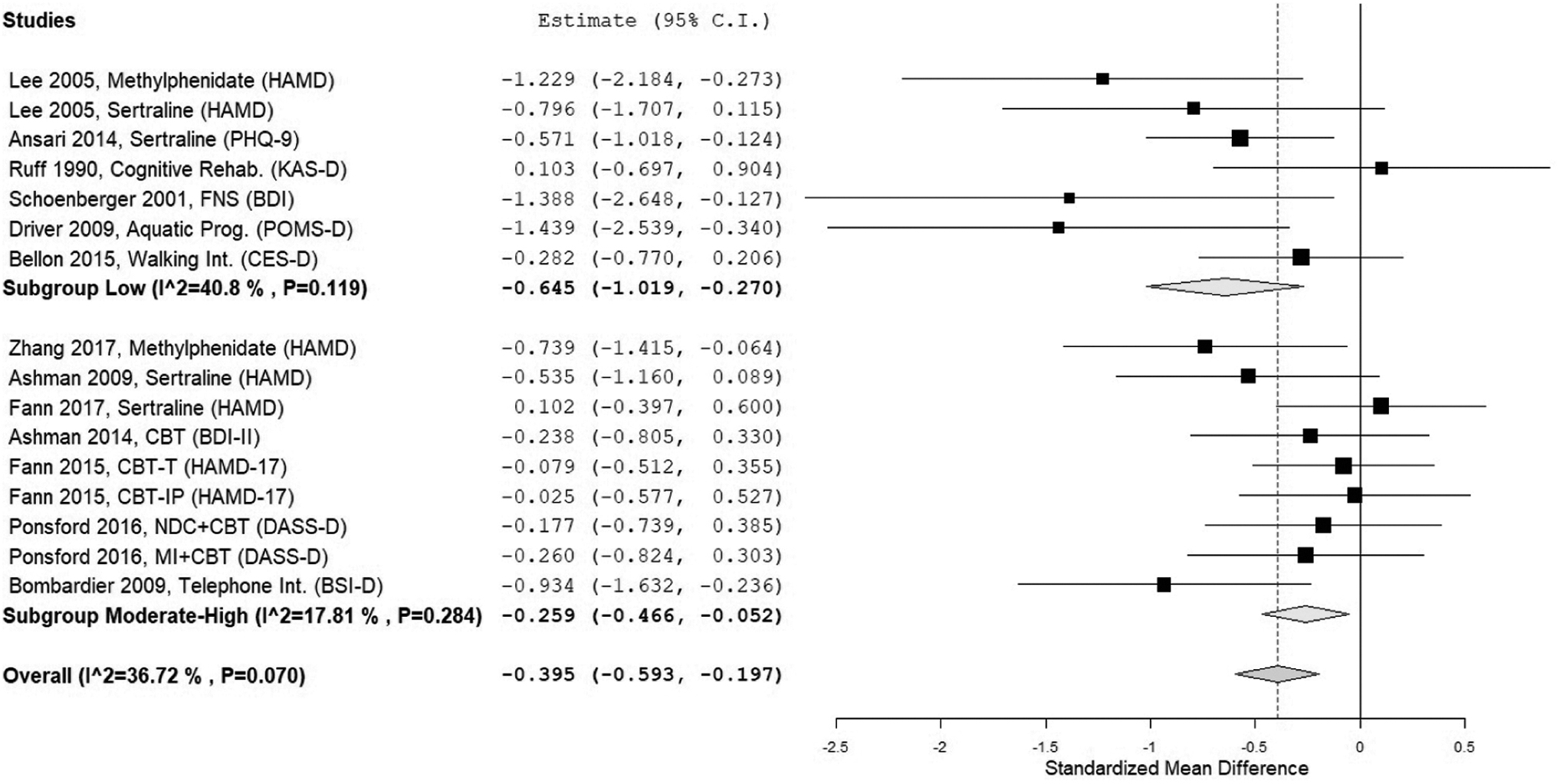
Results of the meta-analysis for subgroups of low- and moderate-/high-quality studies.
Discussion
To our knowledge, this research is the first meta-analysis that compares the effect of pharmacological and non-pharmacological interventions for depression after TBI. Both pharmacological and non-pharmacological interventions reduce depressive symptoms and depression after moderate-to-severe TBI.
A stronger effect of pharmacological compared with the non-pharmacological interventions or vice versa was not established. The moderate effect of −0.492 is small compared with the large effect sizes reported in several meta-analyses. 22 –24 Where our study compared the intervention effect between intervention and control groups, these studies used pre–post treatment comparisons in their main analyses, not controlled for placebo-effects, which may explain the large effect sizes. In sub-analyses restricted to controlled studies only, the pooled intervention effect only remained significant in Salter and colleagues, in which sertraline was found effective as in our sub-analysis of the sertraline RCTs. 22
In our meta-analysis on non-pharmacological studies, we found a significant intervention effect. Previous meta-analyses in patients with TBI 27 –29 found no significant effects for psychological interventions, which is in line with our subgroup analysis that also showed that CBT-based interventions had no significant effect on depression post-TBI. However, the significance of the intervention effect depended on the measurement instrument selected; replacing HAMD by SCL-20 or BDI, CBT-based interventions did have a significant effect on depression post-TBI. In line with two other meta-analyses on exercise-based interventions, 30,34 we did find a significant effect of “other” non-pharmacological interventions, which included exercise therapy and flexyx neurotherapy. Most of these studies were of low quality and therefore these results should be interpreted with caution. Overall, comparing low- versus medium- and high-quality studies showed no difference in effect.
Although these data are informative, several methodological issues still hinder their use in clinical decision making. First, the variation in depression criteria made it difficult to compare studies. In seven studies, 9 –13,15,16 the diagnostic criteria for major depression based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) and/or scoring above the cut-off for depression on a depression scale was an inclusion criterion. In one study patients were required to have a depression or anxiety disorder according to the DSM-IV. 17 In addition, DSM-IV criteria for depression are not always in line with scores on a depression scale. For example, in the study of Ashman and colleagues, 15 patients could participate when depression diagnosis was based on the DSM-IV, or on a score of at least 21 on the BDI questionnaire. Only 70% of patients met both criteria. Four studies 14,19 –21 did not report inclusion criteria with regard to depression. Based on the risk of bias assessment, these four studies were all classified as low-quality studies. One study explicitly stated that patients were not required to have a depression or any form of psychological distress, but a subgroup analysis was performed in the patients with depression. 18
Second, various instruments were used for the measurement of depression, including self-report questionnaires and observational rating scales. Measurement instruments may include items related to psychological or physical problems, which could be depression-related but also TBI-related. Thus, the measurement instrument chosen may influence the level of depression measured. We therefore repeated the meta-analysis assessing secondary outcome measures for depression. 9,10,13,16 Substitution of the HAMD by BDI in two studies and by SCL-20 in two studies resulted in a smaller pooled effect size, which means a smaller treatment effect (SMD HAMD: −0.395 vs. SMD BDI and SCL-20: −0.339). In addition, replacing the depression outcome measures had influence on the results of the analyses. For example, Methylphenidate turned out to be more effective compared with psychological interventions when the focus was on the HAMD. This effect disappeared in the analysis with SCL-20 and BDI. To make reliable comparisons between interventions, it is important to select a preferential depression scale which is validated in patients with TBI.
Third, there was heterogeneity between patient populations. The number of studies that solely included patients with moderate-to-severe TBI was scarce. Some studies did not specify the severity (i.e., mild, moderate, or severe). 9,10,14,20 Therefore, although studies that only included patients with mild TBI were excluded from our meta-analysis, this may be a cause of selection bias. A fourth limitation is the variability in the control condition, which varied from no treatment or waitlist control, or placebo to usual care or specific care, such as supportive psychotherapy, 15 nutrition control group, 21 vocational rehabilitation class, 20 and day treatment. 14 Finally, dropout rates and methodological quality varied considerably between studies and some non-pharmacological studies allowed participants to take medication for depression during the intervention and some did not report the use of anti-depressants. Background medication may influence the effect estimates if not controlled for.
In this meta-analysis, three studies had multiple treatment arms. Within these studies two treatment arms were compared with the same control group, which is a possible violation of the assumption of independence, which can be seen as a limitation of the study. We could not account for the clustering of the control groups, because of the limited number of co-variables that we could enter in this analysis.
Conclusions
Both pharmacological and non-pharmacological interventions seem effective in reducing depression or depressive symptoms after moderate/severe TBI. However, the evidence supporting a treatment or a combination of treatments is limited and depends on the outcome measures selected, heterogeneity between patient populations, and study designs. Treating post-traumatic depression may improve compliance in post-acute rehabilitation and even long-term outcome. As such, quick initiation of treatment of post-traumatic depression is reasonable from a clinical perspective. This topic needs a thorough RCT with well-defined outcome measures and a more homogenous patient population.
Footnotes
Acknowledgments
We thank Gerdien B. de Jonge, biomedical Information Specialist from the Medical Library of Erasmus Medical Center for her support in literature searching.
Part of this work was presented at the 13th World Congress on Brain Injury, Toronto, Canada, March 15, 2019.
Funding Information
This study was partly funded by the Dutch Brain Foundation (PS2014-06).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.