
Abstract
Microstructural white matter (WM) disruption and resulting abnormal structural connectivity form a potential underlying pathology in traumatic brain injury (TBI). Herein, to determine the potential mechanism of cognitive deterioration in TBI, we examined the association of damage to specific WM tracts with cognitive function in TBI patients. We recruited 18 individuals with mild-to-moderate/severe TBI in the chronic phase and 17 age-matched controls. We determined the pattern of WM aberrations in TBI using tract-based spatial statistics (TBSS) and then examined the relationship between cognitive impairment and WM damage using the threshold-free cluster enhancement correction in TBSS. TBSS analysis showed that TBI patients exhibited WM aberrations in a wide range of brain regions. In the majority of these regions, lower fractional anisotropy (FA) largely overlapped with increased radial diffusivity, but not with axial diffusivity. Further, voxel-wise correction in TBSS demonstrated that higher FA values were associated with better performance in the phonemic verbal fluency task (VFT) in widespread WM regions, but not with the semantic VFT. Despite variation in the magnitude and location of brain injury between individual cases, chronic TBI patients exhibited widespread WM aberrations. We confirmed the findings of previous studies that WM integrity is lower across the spectrum of TBI severity in chronic subjects compared to controls. Further, phonemic VFT may be a more sensitive cognitive measure of executive dysfunction associated with WM aberrations in TBI compared with semantic VFT.
Introduction
Traumatic brain injury (TBI) is a major cause of death and disability worldwide. 1 TBI survivors also exhibit a range of short- and long-term adverse clinical outcomes, including cognitive impairments or emotional dysregulation, resulting from traumatic axonal injury. 2 –4 These clinical problems can affect the individual's daily life and those of their families and communities.
Diffusion tensor imaging (DTI) is a non-invasive magnetic resonance (MR) imaging (MRI) technique that characterizes Brownian motion of water molecule in the brain and can provide insights into the pathophysiology of white matter (WM) microstructure. As such, DTI is considered a promising approach to detect “invisible” WM abnormalities related to TBI. 5 More specifically, using a whole-brain voxel-based analysis such as tract-based spatial statistics (TBSS), recent studies demonstrated that the neural pathophysiology related to mild TBI (mTBI) includes a disturbed structural connectivity involving multiple brain regions, rather than simply a single lesion. 6 For instance, despite variation in the magnitude and location of injury between individuals, a recent meta-analysis of TBSS studies reported that mTBI patients show lower fractional anisotropy (FA; a measure of the degree of diffusion anisotropy within a voxel) in three major WM tracts, including the left thalamus extended to the splenium of the corpus callosum (CC) and to the anterior thalamic radiation (ATR), the forceps minor, and the right superior longitudinal fasciculus (SLF). These findings suggest that TBSS may be useful for examining the abnormal structural connectivity underlying disturbed brain networks in TBI. 7
Cognitive impairments are common clinical features in TBI and are associated with progressive WM deterioration after injury. For example, regional FA values in the CC and sagittal stratum (SS) were reported to be correlated with performance on finger-tapping and visuomotor speed tasks, respectively. 8 A recent large meta-analysis also found that higher FA values in most brain regions were associated with better cognitive performance, including memory and/or attention in the CC, fornix, internal capsule, arcuate, and uncinate fasciculi (UF). 9 Thus, understanding the relationships between WM abnormalities described by DTI metrics and neuropsychological outcomes may provide important information on the pathogenesis of cognitive dysfunction in TBI.
In the present study, we confirmed the findings of previous studies that WM integrity is lower across the spectrum of TBI severity in chronic subjects compared to controls. Then, we explored the relationship between WM microstructure and cognition assessed with neuropsychological tests across the domains of executive, attention, and memory function.
Methods
Participants
This study included 18 individuals with a history of mild-to-moderate/severe TBI and 17 healthy controls (CON; Table 1). All participants were recruited from Keio University Hospital (Tokyo, Japan). The CON group was recruited from the general public, with subjects explicitly matched to TBI participants during recruitment. After an extensive description of the study, written informed consent was obtained from all participants. The study protocol was approved by the Ethics Committee of Keio University School of Medicine and prepared in accord with the ethical standards of the Declaration of Helsinki.
Demographics, Intelligence Quotient, and Cognitive Measures
A multi-variate analyses of variance (MANOVA) was performed in FAB for the purpose of multiple corrections.
JART, Japanese Adult Reading Test; MMSE, Mini-Mental State Examination; RCPM, Raven's Colored Progressive Matrices; FAB, Frontal Assessment Battery; VFT, Verbal Fluency Task; DEX, Dysexecutive Questionnaire; FBI, Frontal Behavioral Inventory; EMC Everyday Memory checklist.
TBI participants were diagnosed as mild or moderate/severe TBI based on the American Congress of Rehabilitation Medicine and the Department of Veterans Affairs and the Department of Defense guidelines 10,11 : 1) mTBI (Glasgow Coma Scale [GCS] = 15–13, loss of consciousness [LOC] duration ≤30 min, and post-traumatic amnesia [PTA] duration ≤24 h); 2) moderate TBI (GCS = 12–9, LOC duration <24 h, and PTA duration <7 days); and 3) severe TBI (GCS = 3–8; LOC duration ≥24 h, and PTA duration ≥7 days). Participants were also confirmed to have had no other neurological disease, chronic hypertension, or chronic alcoholism and no massive subarachnoid hemorrhage or subdural hematoma on conventional MRI. But TBI participants with focal subarachnoid hemorrhage, petechial hemorrhages, and focal contusion were included in this study. The days elapsed post-injury ranged from 333 to 2395 days (mean ± standard deviation = 1264.4 ± 765.9). Three-month post-injury was defined as the chronic phase. 12
Cognitive assessment
All participants were administered a 25-item short version of the Japanese Adult Reading Test (JART), 13,14 which is composed of 25 Japanese irregular words as an estimate of pre-morbid intelligence quotient. We further evaluated general cognitive function using the Mini-Mental State Examination (MMSE) and Raven's Colored Progressive Matrices (RCPM), attentional/frontal/executive function using Frontal Assessment Battery (FAB), Verbal Fluency Task (VFT), Dysexecutive Questionnaire (DEX), and Frontal Behavioral Inventory (FBI) and subjective memory function using the Everyday Memory Checklist (EMC).
Image acquisition
MR images were acquired using a 3 Tesla (T) whole-body Discovery MR 750 3.0T scanner (GE Medical Systems, Milwaukee, WI) with a 32-channel head coil. Diffusion-weighted images were collected using an echo-planar imaging spin-echo sequence with b0 images and 25 directions of diffusion gradients. Imaging parameters for the diffusion-weighted sequence were as follows: field of view, 25.6 cm; matrix size, 128 × 128; repetition time/echo time, 5000/79.9 ms; 42 axial-oblique slices; and slice thickness, 4 mm/no skip. The diffusion gradient duration was δ = 32 ms, and the diffusion weighting was b = 800 s/mm2, with b = 0 as reference images.
Tract-based spatial statistics processing
Pre-processing and analysis were performed using the FMRIB Software Library (FSL; version 6). Pre-processing included eddy-current and motion corrections. Our head motion index was the mean absolute intervolume displacement with respect to the first image of each run; the root-mean-square deviation was calculated using the FSL rmsdiff function. Because motion introduces artifacts in DTI data, 15 we set the inclusion criterion for motion as a mean head motion <2.5 mm. Data were then skull-stripped using the FSL Brain Extraction Tool and registered to the Montreal Neurological Institute 152 standard space using non-linear registration. FA images were estimated using DTIFIT. Next, all FA images were averaged to create a mean FA image and skeleton, which represented the centers of the major tracts common to the group. 16 The FA threshold was set at 0.3. 17 Other DTI parameters, including axial diffusivity (AD) and radial diffusivity (RD), were projected onto the mean FA skeleton.
Statistical analysis
To examine the differences in DTI parameters between individuals with TBI and CON, we conducted t-tests using FSL Randomise. Age and head motion were included as nuisance covariates. Statistical significance was set at a family-wise error rate (α = 0.05)-corrected threshold-free cluster enhancement of p < 0.05, with a minimum cluster size of 10 voxels. 18,19 To examine the correlation of DTI parameters indicating WM microstructure aberrations with cognitive function in TBI patients, correlation analyses were performed using the threshold-free cluster enhancement correction in TBSS.
Results
Demographics and cognitive measures
Among 18 TBI individuals, 11 patients (61%) were diagnosed with an mTBI and 7 patients (39%) were categorized into a moderate/severe TBI. There were no differences in age, duration of education, or pre-morbid intelligence quotient estimated by JART between the groups. Individuals with TBI showed significantly lower performance compared to CON on neuropsychological assessments such as MMSE, RCPM, FAB, phonemic VFT, DEX, FBI, and EMC (see details in Table 1).
Tract-based spatial statistics
Individuals with TBI had significant widespread low FA values compared to CON (Fig. 1). These results were observed bilaterally in the ATR, UF, anterior and posterior limb of the internal capsule, corticospinal tract (CST), anterior, superior, and posterior corona radiata, posterior thalamic radiation (PTR), fornix/stria terminalis, and SS including the inferior longitudinal fasciculus (ILF) and inferior fronto-occipital fasciculus (IFO). Additionally, FA was significantly low bilaterally in the SLF, SLF temporal part, cingulum (cingulate gyrus) and genu, body, and splenium of the CC. There were no clusters that exhibited high FA values in TBI patients compared to CON. TBI patients also showed a significantly greater RD compared to controls in regions showing significant FA group differences, whereas there were no group differences in AD values.
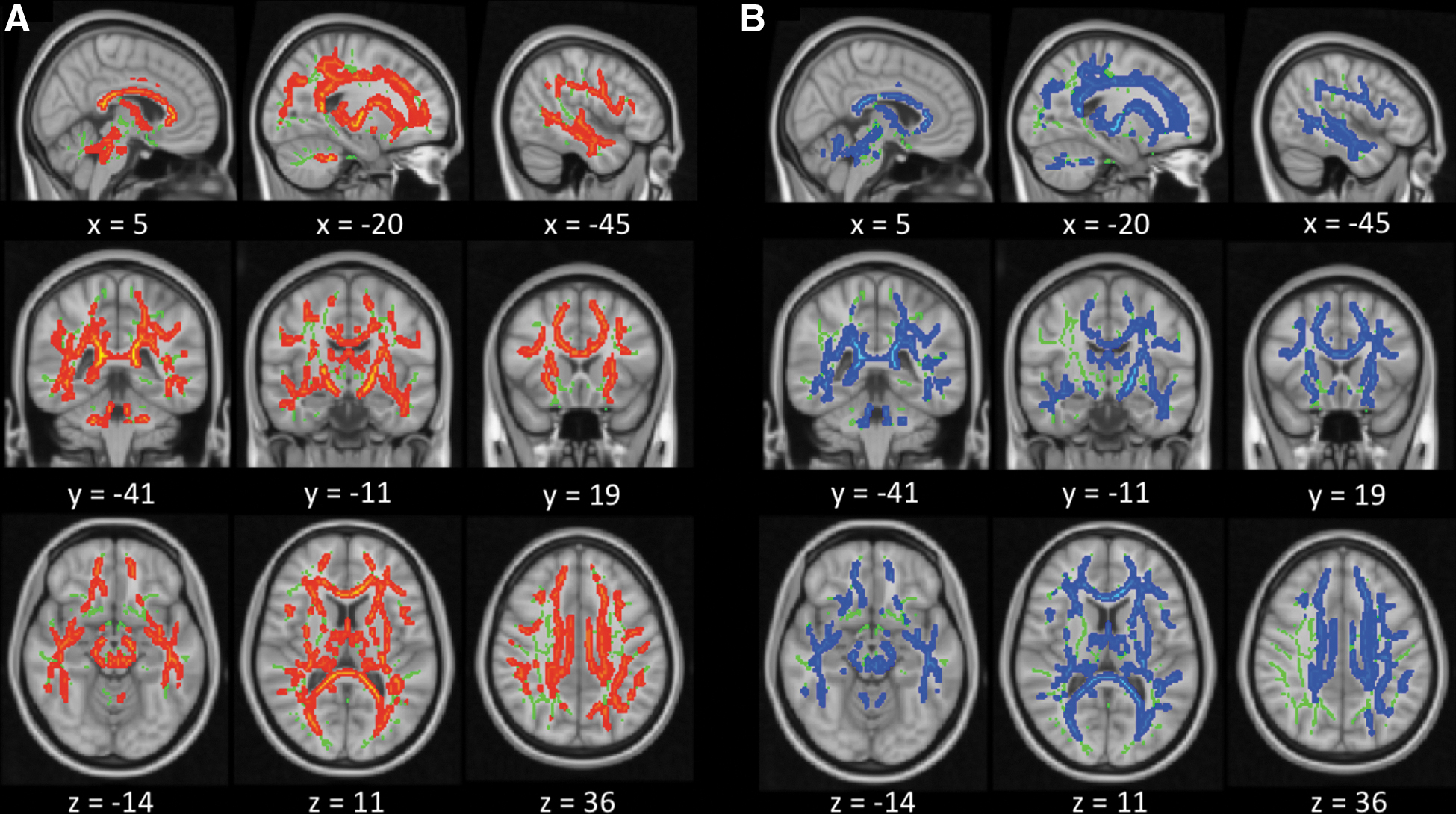
Results of voxels showing significant reductions in fractional anisotropy (FA) and increases in radial diffusivity (RD) in traumatic brain injury (TBI) patients compared to controls (CON; p < 0.05, family-wise error corrected). Group differences in tract-based spatial statistics were “thickened” (for visualization purposes) by expanding the significant white matter skeleton cluster to the full extent of the local FA map. (
Next, we divided TBI patients into clinical subgroups based on severity and separately examined TBI grades (i.e., mTBI [n = 11] vs. CON [n = 17]; moderate/severe TBI [n = 7] vs. CON [n = 17]]. When compared to CON, individuals with mTBI demonstrated significantly low FA values in most of the WM tracts showing significantly low FA values in all TBI stages; however, sizes of these WM regions of mTBI were slightly smaller than those of all TBI stages. Moderate/severe TBI showed significantly low FA values compared to CON in only a few WM tracts, such as the bilateral anterior corona radiate and genu, body, and splenium of the CC. There were no clusters that exhibited high FA values in mTBI and moderate/severe TBI compared to CON, respectively.
Correlation of regional fractional anisotropy values with cognitive measures
Regional associations of FA values with various cognitive measures were investigated using the threshold-free cluster enhancement correction in the TBI group. FA values were significantly positively correlated with phonemic VFT total scores in widespread WM regions (Fig. 2). By contrast, there were no correlations of regional FA values with semantic VFT total scores.

Regional associations of fractional anisotropy (FA) values with total scores of the phonemic verbal fluency task (VFT) in traumatic brain injury (TBI). The results of threshold-free cluster enhancement correction in tract-based spatial statistics are “thickened” (for visualization purposes) by expanding the significant white matter skeleton cluster to the full extent of the local FA map. Significant positive correlations of regional FA values with total scores of the phonemic VFT for TBI participants are displayed in green-light green (p < 0.05, corrected). Results are mapped onto a standard T1 Montreal Neurological Institute 152 template (right = left). Color image is available online.
Discussion
The main findings of the present study were that chronic TBI patients showed WM aberrations in a wide range of brain regions. Tracts that showed low FA values largely overlapped with the tracts that exhibited high RD values in TBI patients. In contrast, there were no group differences in AD values. Further, correlation analysis demonstrated that lower FA values in widespread regions were significantly associated with lower scores of phonemic VFT, but not with the semantic VFT, in chronic TBI. Our findings suggest that the underlying pathophysiology of TBI may represent demyelination, rather than alterations, in fiber coherence. Further, phonemic VFT may be a more sensitive cognitive measure of executive dysfunction associated with WM aberrations in TBI compared with semantic VFT.
Using TBSS, we found that mild-to-moderate/severe TBI patients in the chronic phase showed significantly lower FA values in many major WM tracts, including the bilateral ATR, UF, CST, corona radiata, PTR, fornix/stria terminalis, ILF, IFO, SLF, cingulum (cingulate gyrus), and genu, body, and splenium of the CC. These findings are similar to those in previous meta-analyses of TBI patients. For example, a previous meta-analysis of 26 studies indicated that mTBI patients had significantly lower FA values compared to CON in three WM clusters, including the left thalamus extending to the splenium of the CC and to the ATR, the forceps minor, and the right SLF. 7 Additionally, a recent meta-analysis study with samples from 44 DTI studies reported that 88% of all WM regions of interest (ROIs) in mTBI patients, and 92% of WM ROIs in moderate-to-severe TBI patients, showed lower FA values compared to CON. 9 In particular, the CC (more prominent in the splenium region) was consistently detected as an abnormal WM tract at all TBI stages. Further, low FA in widespread WM regions, including the centrum semiovale, cerebral peduncle, fornix, UF, cingulum, forceps minor, and the ATR, were identified as a potential pathology in TBI, with moderate-to-severe injury causing greater FA alterations than in mTBI.
Intriguingly, our findings from the subgroup comparisons indicate that severity of injury may have an opposite effect on WM aberrations compared with these previous studies, such that mild injury causes greater FA alterations than in moderate/severe TBI. However, considering statistical power attributable to relatively small sample size of the moderate/severe group (n = 7), the results of this exploratory analysis should be interpreted with caution.
Given that previous longitudinal studies have consistently reported progressive WM damage in chronic TBI, 20,21 the timing after injury is an important consideration when assessing WM alterations. For instance, Dinkel and colleagues reported that WM abnormalities in the CC and bilateral corona radiata evolved significantly between the initial assessment and up to 2 years after injury. 22 Further, TBI patients were reported to show longitudinal FA reductions in the CC over a 4-year study period. 8 Moreover, in chronic moderate-to-severe TBI, WM aberrations were observed in widespread WM tracts. 12,23 These findings of progressive WM deterioration for several years post-injury suggest that TBI likely involves a prolonged disease state with potentially lifelong systemic impacts. Taken together, despite the variability in the magnitude and location of brain injury in individual TBI patients, 24 these data provide additional evidence that chronic TBI involves WM microstructural alterations in a wide range of brain regions caused by progressive WM deterioration over time.
We observed that tracts with high RD values largely overlapped with the tracts with low FA values in the TBI group, whereas AD remained unchanged. Although a number of studies have revealed longitudinal increases in RD, 25 –27 findings of AD are inconsistent, with some studies finding increases, 28,29 decreases, 30 or no changes 25 in TBI. In our samples, we confirmed that there were no changes in regional AD values over time after injury from correlation analysis of AD values with duration between injury and MRI scan (results are not shown). Therefore, we speculated that lower FA values observed among our subjects were likely driven by alterations in radial (and not axial) diffusivity, suggesting that the underlying WM alterations may involve changes in fiber integrity and myelination, rather than fiber coherence. 31
VFT measures the cognitive performance to search lexical stores, retrieve semantic information, and switch cognitive setting. 32,33 Although two varieties of VFT (phonemic fluency and semantic fluency) are commonly used for assessing the neuropsychological aspects of TBI, it is widely assumed that TBI patients show greater impairment on phonemic fluency tests because of difficulties in self-generative behavior, flexibility, set shifting, and self-monitoring. 34 In the present study, voxel-wise corrections in TBSS revealed that higher FA values were associated with better performance in phonemic VFT (but not in semantic VFT), mainly in inter- and intrahemispheric connections projecting to the frontal lobe, rather than the temporal lobe, such as the bilateral ATR, forceps minor, and genu of the CC. ATR is a WM fiber bundle connecting the pre-frontal cortex (mainly in the dorsolateral pre-frontal cortex) and the thalamus through the anterior limb of the internal capsule and is involved in executive functions and planning complex behaviors. Both the forceps minor (frontal radiation of CC) and genu of the CC have interhemispheric connections projecting to frontal areas, and disruptions of these regions are involved in impairments of frontal lobe functions. 35,36 Thus, lower WM integrity in these tracts projecting to frontal areas might lead to impairments in executive function, resulting in poor performance in phonemic VFT.
Further, previous studies demonstrated that phonemic fluency may be more impaired in individuals with frontal brain damage, whereas semantic fluency may be more impaired in individuals with temporal brain damage, indicating that these two subtypes have potentially different neural substrates. 33,37 Taken together, our findings provide further support that phonemic VFT may be a more sensitive cognitive measure of executive dysfunction associated with WM aberrations in TBI compared with semantic VFT. However, although the phonemic task is more sensitive to TBI than the semantic fluency task, 38,39 it remains controversial as to which fluency test is the most sensitive for measuring executive dysfunction observed in TBI. 32,33,38,40
In addition, there are contrasting findings in previous neuroimaging studies examining the association of DTI parameters with VFT performance. For example, although the phonemic VFT score was recently reported to be a good predictor of DTI abnormalities at 5 years post-injury in TBI, 41 another study found that semantic VFT score was positively correlated with FA in the left cingulum-cingulate gyrus bundle. 42 Intriguingly, Croall and colleagues also demonstrated an opposite direction of the relationship between FA and VFT, with low FA associated with better phonemic VFT performance in chronic TBI patients. 43 Therefore, future studies with larger samples are required to address the inconsistencies between various studies.
Our study has several limitations. The causes of TBI in our patients were not consistent, and further studies are required to examine the contributions of different external insults on development of TBI. Thus, larger TBI cohorts are required to provide a comprehensive assessment and more thorough subgroup analysis.
In conclusion, we confirmed that chronic TBI patients exhibited widespread WM aberrations in various DTI parameters, suggestive of demyelination, rather than alterations, in fiber coherence. Further, WM abnormalities in widespread regions were associated with phonemic verbal fluency impairments in chronic TBI.
Funding Information
This work was partially supported by The General Insurance Association of Japan (to B.Y.).
Footnotes
Author Disclosure Statement
No competing financial interests exist.