
Abstract
Diffusion tensor imaging (DTI) quantifies microstructural lesion characteristics, but impact of the interval between spinal cord injury (SCI) and examination on imaging characteristics is unclear. Our objective was to investigate the impact of duration of injury on DTI indices in dogs with acute, spontaneous SCI from thoracolumbar intervertebral disc herniation (IVDH) and explore associations with clinical severity. Twenty-six dogs with acute thoracolumbar IVDH of variable severity who underwent DTI were included. Neurological severity was graded using the modified Frankel Score (0–V). Fractional anisotropy (FA) and mean diffusivity (MD) were calculated on regions of interest within and adjacent to the lesion epicenter. Relationships between FA or MD and duration (injury to imaging interval) or neurological severity were determined using regression analysis and Wilcoxon rank sum. Median age was 6.8 years (1–13), median duration was 1.5 days (1–9), and neurological signs ranged from ambulatory paraparesis (MFS II) to paraplegia with absent pain perception (MFS V). Mean FA was 0.61 ± 0.09 cranial to the lesion, 0.57 ± 0.12 at the epicenter and 0.55 ± 0.10 caudally. Mean MD was 1.18
Introduction
Diffusion tensor imaging (DTI), a type of diffusion weighted imaging, utilizes the magnitude and direction of cellular diffusion of water molecules to construct images. 1 –3 It provides information on tissue microstructure, most notably the integrity and organization of white matter tracts. 1 –3 Quantitative DTI analysis involves calculation of specific indices with the most common being fractional anisotropy (FA) and mean diffusivity (MD). The FA expresses the percent directionality of diffusion within a given tissue as a value between zero (isotropic) and one (complete directional dependence along a single axis) while MD assesses the magnitude of diffusion in any direction within a given area. 3,4
While DTI was developed originally as a brain imaging modality, there are increasing numbers of studies of spinal cord DTI in people and animals with spinal cord injury (SCI). 3,5 –11 After SCI, DTI can highlight microstructural abnormalities including axonal damage, demyelination, cavity formation, and regional loss of cellular architecture. 12 –17 Dogs commonly have severe, acute, spontaneous SCI secondary to intervertebral disc herniation (IVDH) and trauma and offer a readily available population in which to study naturally occurring injury. 18 –20
Similar to human traumatic SCI, dogs typically sustain mixed compressive and contusive lesions and display heterogeneity at the population level. 18 –20 As such, there is a growing effort to utilize dogs as a translational large animal model capable of capturing the complexity and heterogeneity of human SCI to complement experimental models. 18,19 Developing DTI as a non-invasive imaging biomarker and prognostic indicator in dogs with SCI will further expand their utility as a clinically relevant, translational model. 18,19
In persons with acute SCI, FA and MD have each been associated variably with injury severity while MD has also been associated with post-operative recovery. 5,21 –23 Study populations are small, however, and there is inconsistency between results, suggesting that the relationship between DTI values, injury severity, and prognosis remains unclear in acute SCI in people. 5 In canine SCI, DTI has been able to differentiate injured from healthy controls and acute from chronic injury, but was not shown to be a better predictor of outcome compared with clinical neurological evaluation. 6 –8,10 The relationship between acute DTI values and injury severity has not been explored in dogs.
In addition to injury severity, there are other factors that have been reported to impact DTI calculations. In people, this includes age, sex, and the location along the spinal cord, with the latter also suggested in canine studies. 6,24 –28 In addition, the timing of imaging within the acute setting might affect imaging results because of dynamic and complex changes associated with acute injury (e.g., hemorrhage, local inflammation, edema, etc.). Optimal imaging timing post-injury has been reported in an experimental rodent model, but has not been established in people or dogs with SCI. 29
The aims for this project were to investigate the impact of duration of injury on DTI parameters and the association between DTI and clinical severity for dogs with IVDH imaged in the acute setting. We hypothesized that, for DTI performed in the acute setting, FA would decrease and MD would increase with increasing duration of injury and that DTI indices could differentiate neurological grade.
Methods
Dogs with a thoracolumbar SCI secondary to IVDH of variable severity that underwent magnetic resonance imaging (MRI) with DTI were enrolled. To be included, dogs must have been imaged within 10 days of the onset of neurological signs and have a single, focal lesion within the thoracolumbar spinal cord identified on conventional MRI sequences. Information obtained from the medical record included signalment, duration of neurological signs, severity of neurological dysfunction at the time of imaging, lesion location, and diagnosis.
Lesion location and diagnosis of IVDH were made based on MRI characteristics and confirmed during surgery. Duration of injury, defined as the interval from onset of neurological signs to imaging, was recorded for each dog and ranged from one to nine days. For dogs imaged within 24 h of onset, a duration of less than or equal to one day was used. Clinical severity was graded using the modified Frankel Scale (MFS) where 0 = normal neurological status, I = pain only, II = ambulatory paraparesis, III = non-ambulatory paraparesis, IV = paraplegia, and V = paraplegia with absent pain perception.
Because subsequent treatment and follow-up varied, outcome was only assessed in severely affected dogs (MFS grade IV or V). The outcome was determined to be “successful” if there was improvement in neurological function or “unsuccessful” if there was no improvement based on the last follow-up evaluation at the hospital or telephone communication with the owner.
Thoracolumbar MRI was performed on a 1.5T magnet (Siemens Medical Solutions USA Inc., Malvern, PA) using circularly polarized spine array and body array flex coils. The following standard sequences were acquired in the transverse and sagittal plane: T1 weighted pre- and post-contrast, T2 weighted, short T1 inversion recovery (STIR), half-Fourier acquisition single-shot turbo spin-echo (HASTE), proton density and gradient echo/T2*. The DTI was acquired in the same region in the transverse plane using the following imaging protocol: slice thickness of 3.5 mm with no gap, voxel size of 3.5
Raw diffusion weighted images (b = 1000 s/mm2) were used to calculate the signal to noise ratio (SNR) and were inspected visually for quality. Images with any malalignment of the spinal cord or major distortions or artifacts were eliminated and not included in this study. The SNR was defined as the ratio of the mean of the region of highest intensity to the standard deviation of background values. A SNR cutoff value of >20 was used to determine adequate quality.
Raw diffusion Digital Imaging and Communications in Medicine (DICOM) images were converted to 4D Neuroimaging Informatics Technology Initiative (NIfTI) format, also generating diffusion direction files (.bvec, .bval) using MRIcron. Using FSL commands, data were corrected for eddy current and motion distortion, and an automated mask was used to remove non-relevant tissues. A diffusion tensor model was fitted to processed images using the dtifit command in the FSL Diffusion Toolkit providing a matrix-valued tensor for each voxel that was used to compute standard indices.
Standard MRI sequences were utilized to identify the lesion epicenter and the visible cranial to caudal extent of the injured spinal cord. Using T2 weighted transverse images for reference, regions of interest (ROI) were drawn manually around the circumference of the spinal cord within the lesion epicenter as well as cranial and caudal to the visible extent of the lesion (Fig. 1). These were denoted as cranial, lesion, and caudal ROI. Cranial and caudal ROI were placed within one vertebral body above or below to the visible margins of the lesion, respectively, as visualized on T2-weighted images. Care was taken to avoid including extradural structures when constructing ROI. The FA and MD were then calculated for each ROI from the corresponding FA and MD maps using Mango (
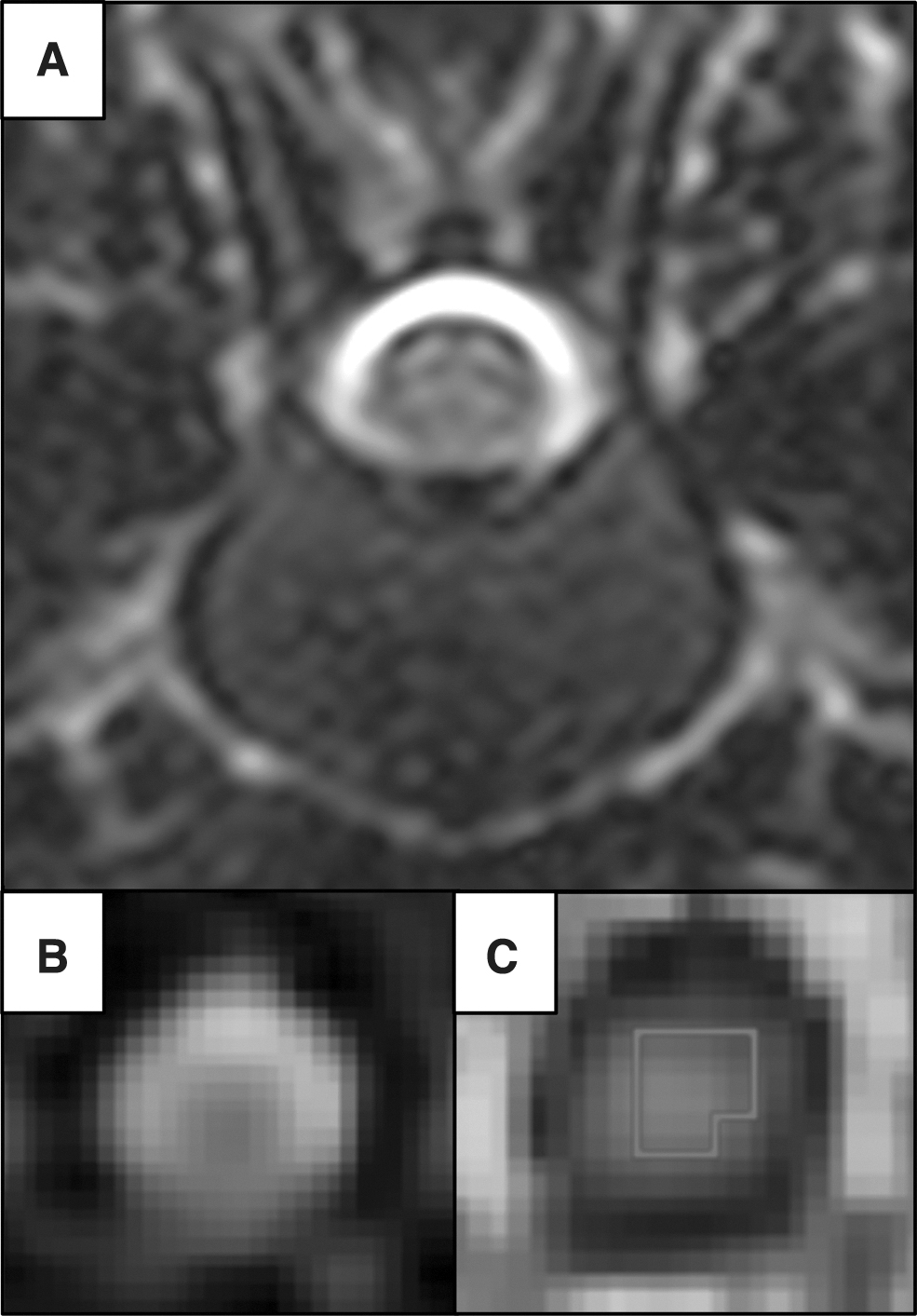
Example of diffusivity maps and region of interest (ROI) placement. (
Statistical analysis
Analyses were performed using Jmp 13 Pro (SAS Institute, Cary, NC, USA) and R (version 3.6.3). Summary statistics for continuous data were calculated and reported as mean and standard deviation or median and range based on the Shapiro-Wilk test for normality. Intraobserver reliability was performed on a randomly selected subset of cases (n = 8, approximately 30% of cases). For those cases, placement of cranial, middle, and caudal ROI were repeated, and then the measurements were compared with the originals by calculating the intraclass correlation coefficient.
Relationships between DTI values and duration of injury were determined by regression analysis and analysis of covariance (ANCOVA) using a model that incorporated age and neurological grade. To investigate associations between DTI values and injury severity, Wilcoxon rank sum or analysis of variance (ANOVA) was performed. Among severely affected dogs, defined as paraplegic with or without pain perception (MFS Grade IV and V), relationships between DTI values and outcome (successful or unsuccessful) were explored using Wilcoxon rank sum. p < 0.05 was considered significant.
Results
Twenty-six dogs with IVDH were enrolled with a median age of 6.8 years (range: 3–13 years) and median body weight of 9.5 kg (range: 5.2–47.3 kg). There were eight Dachshunds, six mixed breed dogs, and nine other breeds represented by two or fewer dogs. Median duration of injury was 1.5 days (range: 1–9 days) and ranged from less than or equal to one day (n = 13), one to two days (n = 6), three days (n = 3), five days (n = 1), seven days (n = 2), to nine days (n = 1). The MFS neurological grade ranged from grade II (n = 2), grade III (n = 11), grade IV (n = 8) to grade V (n = 5). Of the dogs that were designated as severely affected (grade IV or V), follow-up information was available in 12. Ten had a successful outcome (n = 7 grade IV, n = 3 grade V) and two had an unsuccessful outcome (all grade V). One dog (grade IV) was euthanized at the time of imaging and eliminated from outcome analysis. Lesion location ranged from T7 to L5 and was noted to be cranial to L1 in 17 dogs and caudal to L1 in nine dogs.
Diffusion images were of adequate quality with a mean SNR of 29.8 (standard deviation [SD] 7.6) and a minimum value of 20.8. Intraobserver repeatability was excellent with intraclass correlation coefficients >0.93 (95% confidence interval [CI] 0.77–0.99) for all measurements. Mean FA and MD values for each ROI (cranial, lesion epicenter, and caudal) are presented in Table 1. Mean FA and MD values for each ROI divided according to duration of injury (≤1 day, 1–2 days, >2 days) are presented in Table 2.
Mean Diffusion Tensor Imaging Values Across All 26 Dogs
DTI, diffusion tensor imaging; ROI, region of interest; FA, fractional anisotropy; SD, standard deviation; MD, mean diffusivity.
Mean Diffusion Tensor Imaging Values Categorized by Injury Duration
DTI, diffusion tension imaging; ROI, region of interest; FA, fractional anisotropy; SD, standard deviation; MD; mean diffusivity.
Accounting for age and neurological grade, FA of the caudal ROI was inversely associated with duration (p = 0.02) (Fig. 2c). No relationships were identified between MD and duration for any ROI (p > 0.05) (Fig. 2d–f). Mean FA and MD values for each ROI for each neurological grade are presented in Table 3. Across all dogs, no significant relationships were identified between FA and injury severity.
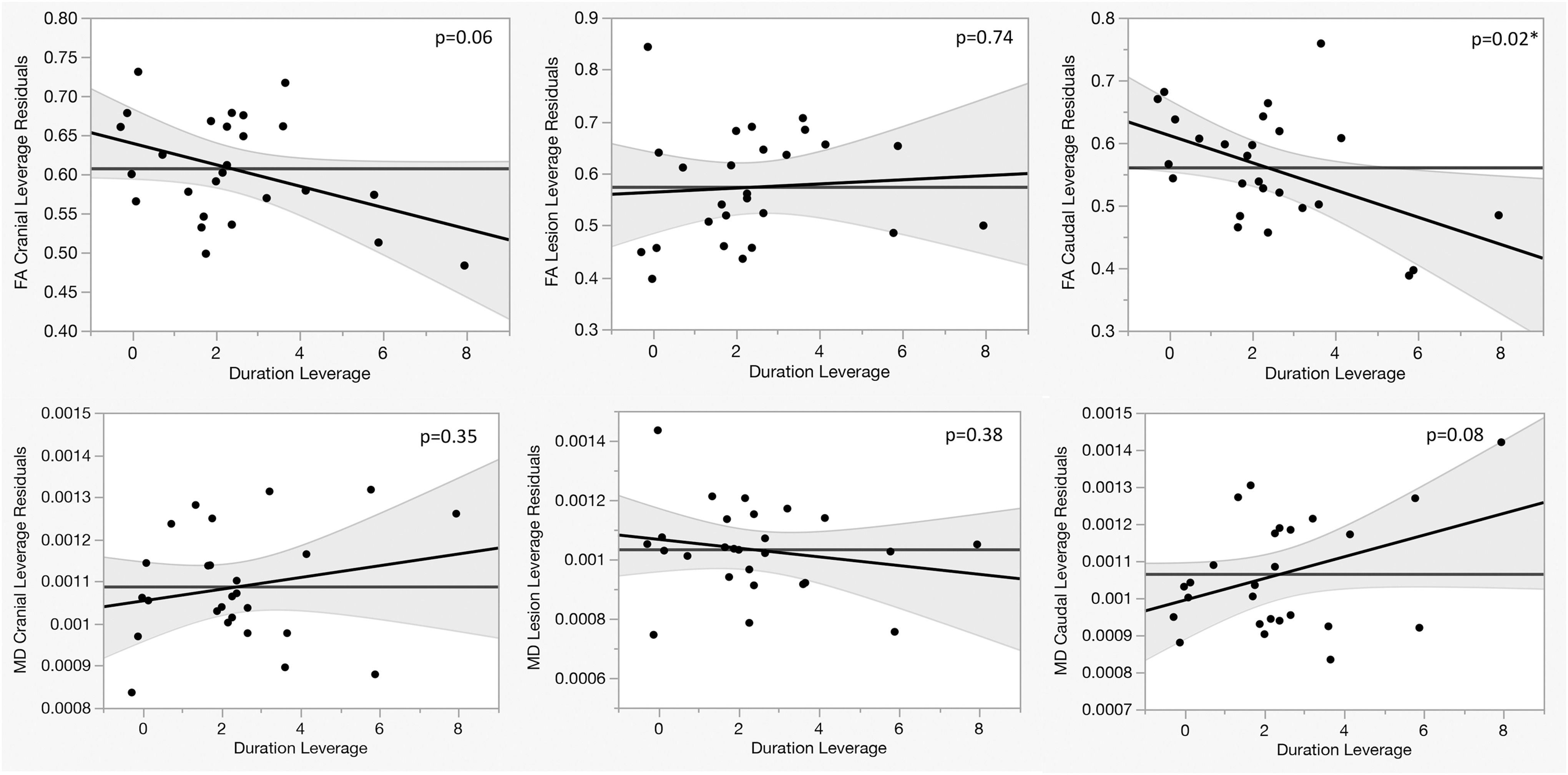
Leverage plots depicting the influence of duration of injury on diffusion tensor imaging indices in dogs imaged within the first 10 days after acute thoracolumbar intervertebral disc herniation. FA, fractional anisotropy; MD, mean diffusivity. p < 0.05 significant.
Mean Diffusion Tensor Imaging Values Categorized by Injury Severity
DTI, diffusion tensor imaging; MFS, modified Frankel Scale; ROI, region of interest; FA, fractional anisotropy; SD, standard deviation; MD; mean diffusivity.
The MD of the lesion epicenter decreased with greater severity of injury, but the difference was not significant (p = 0.07). When injury was categorized as mild (grades II/II) or severe (grades IV/V), however, MD of the lesion epicenter was significantly lower for more severely affected dogs (p = 0.01) (Fig. 3). In addition, when considering dogs imaged within 48 h of onset of signs, MD for the lesion epicenter ROI remained significantly lower for more severely affected dogs (p < 0.04). Among the severely affected dogs for which follow-up information was available (n = 12), mean FA and MD for each ROI are presented in Table 4 grouped by the 10 that improved (successful outcome) and the two that did not recover function (unsuccessful outcome). The MD of the lesion epicenter was significantly lower in dogs with an unsuccessful outcome (p = 0.03).
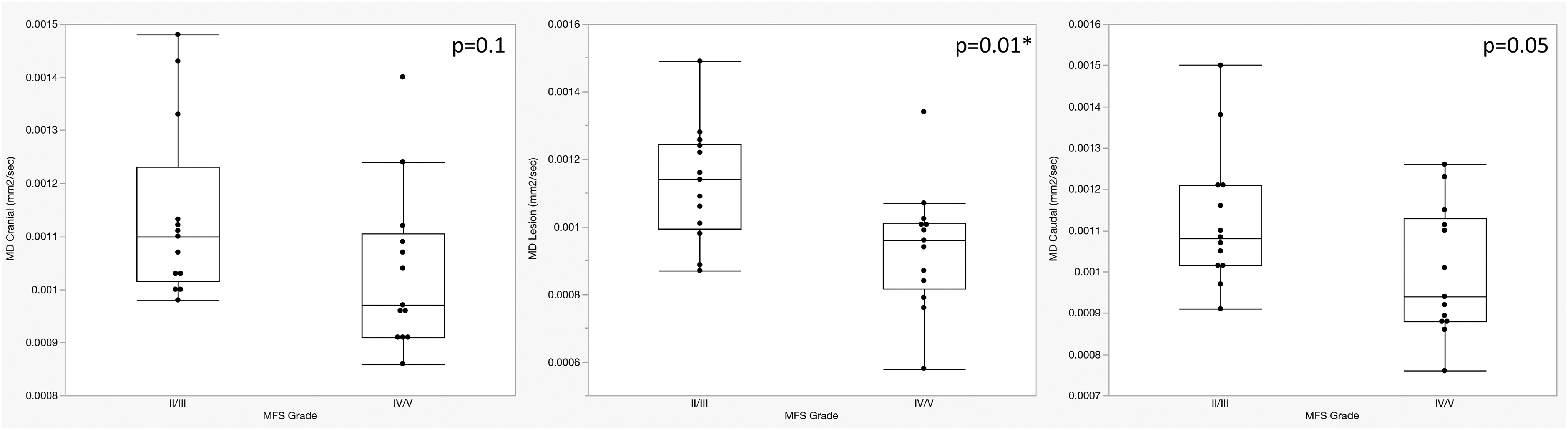
Mean diffusivity (MD) compared between different neurological severity (modified Frankel Scale [MFS] grades II/III vs. grades IV/V) for dogs with acute thoracolumbar intervertebral disc herniation. p < 0.05 significant.
Mean Diffusion Tensor Imaging Values in Severely Affected Dogs (Modified Frankel Scale Grade IV and V) Categorized by Outcome *
DTI, diffusion tensor imaging; ROI, region of interest; FA, fractional anisotropy; SD, standard deviation; MD, mean diffusivity.
Success was defined as improved neurologic function.
of interest, MFS: Modified Frankel Scale. P < 0.05 significant.
Discussion
Our results demonstrated an inverse relationship between the duration of SCI and FA values caudal to the lesion epicenter for dogs with IVDH imaged within 10 days of injury. The decrease in FA over time in the acute setting indicates that the interval from injury to imaging should be considered when interpreting DTI values in dogs with acute thoracolumbar IVDH. We also showed that MD might differentiate injury severity while FA demonstrated no consistent relationship with neurological grade. This suggests that MD might be useful in determining initial injury severity and be worthy of further evaluation as a non-invasive marker of injury and a potential prognostic indicator in this population.
The DTI is being incorporated increasingly into the imaging evaluation of acute SCI in people and dogs. To maximize the utility of DTI, the impact of the timing of injury relative to imaging acquisition needs to be established. In an experimental rodent model, an optimal imaging time of one to three days post-injury has been reported to best determine initial lesion severity and predict subsequent outcome. 29 While the current study was not designed to establish optimal imaging timing in dogs with acute SCI, we did demonstrate decreases in FA without consistent trend in MD over the first 10 days after injury.
This is in contrast to a previous study in dogs where FA values were increased at the lesion epicenter in acute SCI relative to healthy controls, although changes over time were not investigated. 8 Consistent with our findings, however, mean FA values in persons with traumatic cervical SCI imaged between one hour and five days post-injury have been shown to be significantly lower than healthy controls. 21 Further, FA values have been reported to decrease steadily in persons over the first three weeks after injury. 4 Longitudinal evaluation of FA in persons with traumatic brain injury (TBI) has also showed decreases in FA from the acute (up to seven days) to subacute (greater than seven days from injury) stages. 30
In an experimental canine contusion injury model with imaging studies performed at three hours, 24 h, six weeks, and 12 weeks post-injury, FA values within or near the epicenter showed significant decreases between the time of injury and 12 weeks, although there was some variability in the values over the first 24 h. 31 In the same study, MD values at the lesion epicenter declined during the first three hours post-injury and then remained stable or increased over the course of the 12 week study, but the changes in MD were not significant. 31
The MD has also been shown to increase from two weeks to a maximum at 15 weeks post-injury in a rat model of SCI, but changes before two weeks were not evaluated. 32 In dogs with spontaneous injury, MD previously has been shown to be significantly higher in the chronic setting compared with acute SCI or healthy controls, but the timing of this change has not been investigated. 8,10 Overall, broad trends across studies of SCI include general decreases in FA with more variable initial changes in MD followed by increases chronically. These studies, however, also serve to highlight the variability in DTI data and underscore the importance of considering factors such as timing of imaging acquisition when interpreting or comparing results.
Our results suggest that FA decreases but that MD might be less subject to variation within the acute, post-injury setting in dogs with naturally occurring thoracolumbar SCI secondary to IVDH. This initial lack of change over time in MD might reflect a delay in the histological changes underlying this calculation or that the complexity of acute SCI includes factors that variably increase and decrease diffusivity, thus canceling each other out. Serial imaging within the acute and subacute time frame as well as evaluation of diffusivity along individual axes (i.e., axial and radial diffusivity in addition to mean diffusivity) are needed to further delineate how DTI changes over time and to help to determine the optimal time for imaging in this population.
We also explored the association between injury severity and DTI in acute canine SCI. We did not find any associations with FA for any ROI. The MD was noted to decrease, however, as severity worsened, and this change was most pronounced when measured at the lesion epicenter. Among dogs imaged within 48 h of their injury, MD within the lesion epicenter remained significantly lower in paraplegic dogs with or without pain perception (MFS grades IV or V) compared with less severely affected dogs. The underlying cause of a lower MD within the lesion in the acute setting is not clear, but might relate to acute factors restricting diffusivity such as hemorrhage, edema, inflammation, and extradural compression. While this has not been reported previously in dogs with IVDH, it is consistent with reports in persons with acute SCI. 21
Higher MD and lower FA at the injury site have each been correlated strongly with better initial American Spinal Injury Association (ASIA) motor scores in persons with acute, non-hemorrhagic traumatic cervical SCI imaged between one hour and five days post-injury. 21 In another cohort of patients with acute, traumatic cervical SCI imaged between 0 and 10 days from their injury, higher FA rostral to the injury site was associated with better ASIA grade and thoracic limb motor function at the time of imaging. 23 In addition, in persons and dogs with chronic SCI, FA but not MD has been associated with completeness of injury ASIA impairment scores, tibial somatosensory evoked potential values, and pelvic limb motor function. 10,33 –36
These findings suggest that while FA (reflecting the degree of loss of longitudinally aligned axons) appears to correlate well with clinical severity in chronic SCI, this affiliation remains unclear and inconsistent in the acute setting. In contrast, a lower MD (quantifying restricted diffusivity) at the site of acute injury might indicate more severe initial injury, although this relationship might not be maintained in the chronic setting. Therefore, MD might be most useful in determining initial injury severity in dogs with acute SCI secondary to IVDH. The ability to identify differences in clinical status might allow this imaging modality to be developed as a non-invasive outcome measure capable of correlating structural and functional changes in clinical trials of dogs with SCI.
Among severely affected dogs with IVDH, our results provide preliminary data to suggest that DTI in the acute setting might be associated with outcome. While there were only a small number of severely affected dogs in the current study (paraplegic dogs with or without pain perception), lower MD values were noted in the dogs that ultimately had an unsuccessful outcome, most notably MD at the lesion epicenter. In a previous report of DTI in dogs with sensorimotor complete injury performed between 0 and 22 days after onset of signs (median one day), higher FA caudal to the lesion was associated with a lower likelihood of return of motor function. 7
The FA, however, was not shown to be a better predictor of outcome compared with clinical neurological evaluation, and MD or other DTI indices were not evaluated. 7 In addition, in human patients with TBI, FA values in the acute setting were variably associated with prognosis while higher FA in the subacute time frame was predictive of better outcomes; MD was not evaluated. 30
In persons with acute cervical SCI, lower MD on pre-operative imaging was associated with a greater risk of subsequent spinal cord cavitation and limited functional recovery. 22 Our results indicate that MD might be useful in predicting recovery in acute SCI while FA appears more variable. We were not able to standardize treatments or follow-up, however, and results should be interpreted with caution pending further validation. Additional studies in a large number of severely affected dogs are needed to clarify these findings and further explore the prognostic utility of DTI.
Limitations of this study include those inherent to spinal cord DTI, such as the potential for anatomical distortions, low SNR, and partial volume averaging. In addition, specific quantitative values might not be generalizable beyond the specific magnet and protocol utilized. This study also included a relatively small number of dogs, especially among the most severely affected group, and only one disease type. This limited the ability to draw conclusions about the relationship between DTI parameters, injury severity, diagnosis, and prognosis. While our results are intriguing and in line with other published studies, our findings should be considered preliminary and interpreted judiciously, especially with regard to establishing prognostic relationships.
Further evaluation in a larger number of severely affected dogs is needed to confirm and expand these findings, ideally in independent cohorts using their own imaging protocols. In addition, imaging was acquired at only one time point in each dog and, as such, this study was not intended to determine the optimal time to perform DTI in the acute setting. Longitudinal studies are needed to establish the ideal timing for such imaging and to monitor changes over time within an individual animal.
Overall, we demonstrated temporal changes in DTI values in dogs with acute IVDH imaged within the first 10 days of injury indicating that the interval between injury and imaging should be considered when interpreting DTI results. We also determined that DTI, specifically MD, was associated with injury severity and might be useful to explore as a potential predictor of outcome. Development of DTI as a non-invasive imaging biomarker in acute canine SCI will enhance global understanding of the recovery potential in SCI and expand the ability to utilize dogs as a spontaneous disease model.
Footnotes
Funding Information
No funding was received to perform this project.
Author Disclosure Statement
No competing financial interests exist.