
Abstract
The purpose of this study was to assess the frequency of structural lesions on conventional magnetic resonance imaging (MRI) of the brain in a large prospective cohort of post-concussion syndrome (PCS) patients. Conventional 3T MRI was used to evaluate 127 prospectively enrolled PCS patients and 29 controls for non-specific white matter hyperintensities (WMH) and traumatic structural lesions, including encephalomalacia, atrophy, microhemorrhage, subarachnoid hemorrhage, and cortical siderosis. All PCS patients had a clinical diagnosis of one or more concussions based on the Concussion in Sport Group (CISG) consensus statements. Patients with recognized intracranial hemorrhage on prior head computed tomography (CT) and MRI were excluded. The differences between the PCS and control groups were analyzed. Four patients in the PCS group (3.1%) had positive findings, which included microhemorrhages in two patients and encephalomalacia in another two patients. None of these lesions was present in the control group, but there was no statistical difference between the two groups (p = 0.5 for microhemorrhage and p = 0.5 for encephalomalacia). In the PCS group, 28 patients (22%) had WMH (15.7% had 1–10 lesions and 6.3% had >10 lesions), and these results did not differ from the age-matched control (20.6%, all with 1–10 lesions; p = 0.9) The location of the WMH showed no significant difference in the number of juxtacortical WMH between the PCS and control groups (p = 0.5). Structural lesions were rare in PCS in this study, and the presence of such findings suggests a more severe form of traumatic brain injury. Our data support the role for MRI in the diagnosis of PCS by exclusion of atrophy, encephalomalacia, and all forms of intracranial hemorrhage. The presence of WMH irrespective of number is not an exclusion. This is the first description of the MRI criteria for PCS.
Introduction
Traumatic brain injury (TBI) is the most common cause of neurological debility in young adults, and accounts for 30% of all injury deaths in the United States. 1 Approximately 2% of the United States population is affected by TBI, resulting in annual healthcare costs of $76.5 billion. 2 Concussion and mild TBI are the most common forms of TBI, accounting for 75% of all reported TBIs. 3,4 Although the term “concussion” is often used interchangeably with “mild traumatic brain injury” (mTBI), concussions are at the lower end of the spectrum of clinical severity. 5,6 In 1997, the American Academy of Neurology defined concussion as “trauma induced alteration in mental status that may or may not result in loss of consciousness.” 7 However, most clinicians now use the definition of concussion of the Concussion in Sport Group (CISG), which has held the International Conference on Concussion in Sport since 2001, and has published periodic consensus statements on concussion, the last two of which were published in 2013 and 2017. 6,8 Sport and recreation are the major causes of concussion in adolescents and young adults, but other etiologies include motor vehicle collisions, falls, work accidents, assault, and military combat. 9,10 Approximately 80% of patients with concussion achieve neurological recovery within 1–4 weeks following the traumatic event. However, ∼20% with concussion do not fully recover and will have persistent symptoms beyond the initial 1–3 months. These individuals are said to have post-concussion syndrome (PCS). 11 –13 The exact incidence of PCS is uncertain, mainly because of lack of agreement about definitions for the clinical and radiological criteria for PCS, and has ranged from 5% to 58%. 14 –18 Indeed, Mayer and coworkers 19 recently examined the criteria for 10 definitions of concussion and found radiological criteria for only 2. For PCS, the situation is similar, with no agreed-upon inclusion and exclusion criteria for the neuroradiological aspects of this condition. The definition of PCS is critical, as this condition can have a profound impact on long-term well-being 20 and quality of life because PCS often affects neurocognitive and emotional domains, 20,21 which can cause long-term disability. Therefore, the purpose of the present study was to examine the structural magnetic resonance imaging (MRI) findings in a large sample of PCS patients selected according to a consistent clinical definition of PCS.
Although computed tomographic (CT) scan of the head is the usual radiological procedure employed in the acute stage of concussion management because of reduced cost and availability, MRI is the preferred method for investigating patients with PCS, because it is more sensitive for detection of structural lesions and has no ionizing radiation. Conventional MRI is well suited for detection of traumatic structural lesions including contusion, encephalomalacia, and hemorrhages. Specifically, microhemorrhages are best depicted using iron-sensitive sequences such as T2 gradient echo (GRE) and susceptibility weighted imaging (SWI). 19 Although a recent article reported the prevalence of acute, trauma-related MRI structural findings and clinically significant, non-specific MRI findings in athletes with or without sports-related concussion, there are no reports in the literature describing in detail, the role of MRI in PCS. 22 Although the CISG consensus statements have indicated that structural lesions should be absent in PCS, there has been no agreement on the precise MRI criteria for PCS, and, therefore, there has been great variability in the reported incidence of MRI structural lesions in PCS patients in the literature. 23 –25 Also, the variability of the reported incidence of structural lesions in concussion and mTBI relates partly to the difference in the clinical diagnostic criteria published by different societies. To date, there has been no published study of the incidence of structural lesions on MRI in PCS using the CISG definition of concussion. The aim of this study was therefore to: (1) investigate the incidence of structural lesions on conventional MRI in a large prospectively enrolled cohort of PCS patients, and (2) to propose an integrated clinical and neuroradiological MRI definition of PCS.
Methods
A prospective study was employed to investigate the incidence of structural lesions on conventional MRI in patients with PCS compared with age- and sex-matched healthy controls. The study was approved by the University Health Network Research Ethics Board, and consent from all included participants was obtained. This study was funded by the Ontario Brain Institute, Canada, and the Canadian Concussion Centre, Toronto Western Hospital.
Patient selection
A cohort of consecutive patients from January 2013 to December 2015 who were referred to the Concussion Clinic of the Canadian Concussion Centre, Toronto Western Hospital, and were seen by two concussion team physicians including one of the authors who is the director of the Centre (C.H.T.). Clinical inclusion criteria were as follows: (1) must have had at least one concussion with at least one persisting symptom from that concussion, (2) minimum period for persisting symptom(s) >1 month since the last concussion, and (3) diagnosis of PCS was based on clinical criteria for concussion alone using the 2012 Zurich and 2016 Berlin guidelines formulated at the 4th and 5th International Conferences on Concussion in Sport. 6,8 Exclusion criteria included: (1) age <13 years, (2) having any other brain disease, (3) having a recognized intracranial hemorrhage of any type on prior CT and/or MRI scan of the head. Twenty-nine volunteers (19 males, 10 females, mean age = 36.8 ± 9.8 years) were prospectively enrolled as controls. Inclusion criteria for controls were age being >13 years of age without a history of head trauma, not being engaged in contact sports, and without any neurological condition. Any participant with a contraindication to MRI was excluded. Individuals with metallic dental or surgical implants that would excessively degrade the images were also excluded. A total of 134 patients with PCS as described and no recognized hemorrhagic or other lesions were recruited from the concussion clinics. Of these, seven patients were excluded because of incomplete or non-diagnostic imaging, such as absence of an iron-sensitive sequence.
MRI protocol
MRI scans were performed at the University Health Network, Toronto Western Hospital, on a 3T MRI scanner (Signa HDx, GE Healthcare, Milwaukee) with an eight channel phased array head coil. MRI brain protocol included the following sequences: three dimensional (3D) T1-weighted (T1-W) inversion recovery (IR)-prep fast 3D-GRE (repetition time [TR]/echo time [TE] 7.00/2.50 msec; 1 mm 3 voxels); T2-weighted fluid attenuated inversion recovery (FLAIR) (TR/TE/TI 11,000/150/2250 msec; 0.86 × 1.33 × 3 mm voxels); echo planar imaging (EPI) GRE sequence (TR/TE 2000/25 msec, echo train length [ETL] = 12; 0.83 × 0.86 × 4 mm voxels).
Imaging analysis
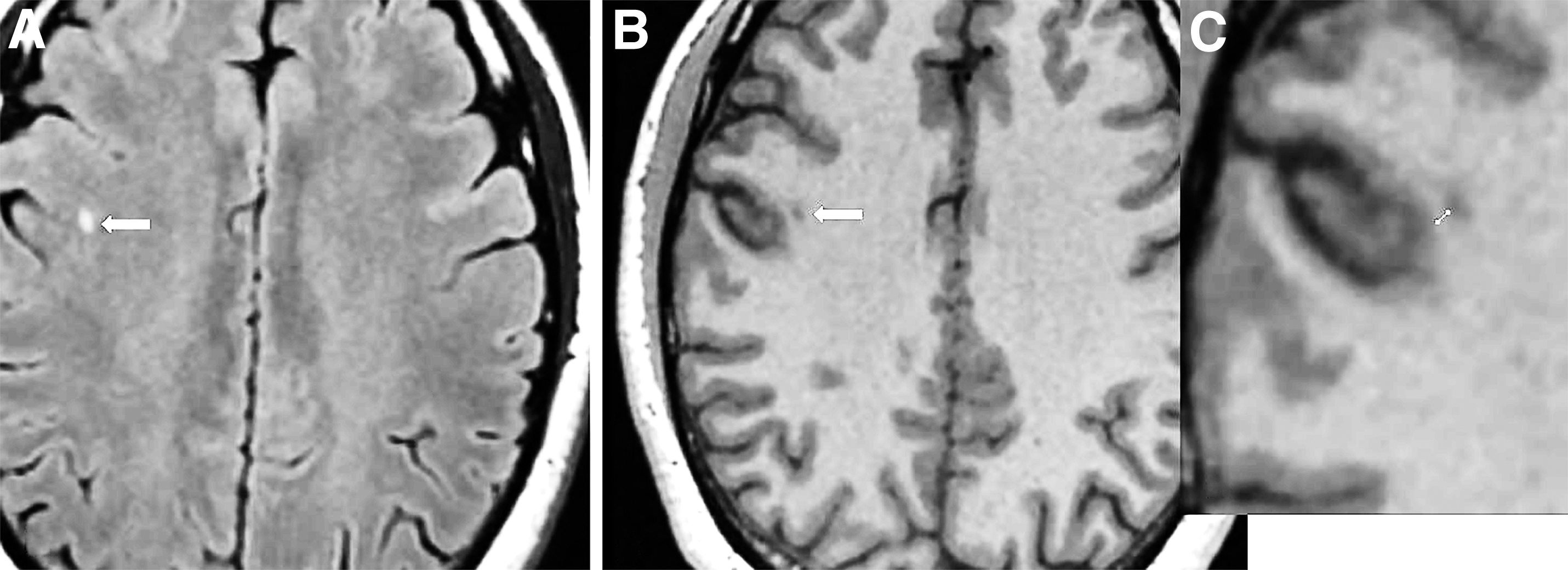
All acquired images were transferred to our picture archiving and communications system (PACS) (Coral PACS/RIS). Annotations including patient identity were removed to facilitate blinded analysis. Two neuroradiologists (J.P. and C.C.-T.H.) independently evaluated each study with final agreement by consensus. Each MRI was evaluated for the presence of encephalomalacia, all intracranial hemorrhages including microhemorrhages, cortical siderosis, white matter hyperintensities (WMH), gross atrophy, and any relevant incidental findings such as arachnoid cysts and Chiari malformation. WMH were counted and recorded categorically as 1–10 and >10. Location of the WMH was also recorded as either juxtacortical (< 3 mm from cortex) or deep (> 3 mm from cortex); the measurement was made from the shortest gray matter–white matter junction to the lesion on both the FLAIR and 3D T1WI as described by Jarrett and coworkers 26 (Fig. 1).
Statistical analysis
Statistical analysis was performed using SAS University Edition (SAS Institute, Inc, Cary, NC) statistical software. The differences in participant demographics between patients and controls were tested for statistical significance using the Student's t test for age and the χ 2 test for gender. Continuous variables were reported as mean and standard deviation. We used the χ 2 or Fisher exact test to evaluate the statistical differences between the PCS and control groups for the following categorical variables: encephalomalacia, microhemorrhages, WMH (1–10 or >10) and WMH locations (juxtacortical or deep). Statistical significance was defined as p < 0.05.
Results
Patient characteristics
A total of 127 patients (77 male and 50 female) with PCS were evaluated with a mean age of 33.6 years and an age range of 13–63 years. There were 29 age-matched controls (19 male and 10 female) with a mean age of 36.8 years and an age range of 20–59 years. There was no significant difference between the ages and sexes of the patients in the PCS group and those in the control group (p = 0.15 and p = 0.63, respectively). Table 1 shows the baseline demographic and clinical data from the concussed patients and controls.
Baseline Demographic and Clinical Data for PCS Patients and Controls
PCS, post-concussion syndrome; SD, standard deviation; MRI, magnetic resonance imaging; MVC, motor vehicle collision.
MRI findings
Two PCS patients (1.57%) had microhemorrhages (right occipital periventricular white matter and central pons), and no significant difference was found between the two groups (p = 0.5) (Fig. 2). There were no other patients with any intracranial hemorrhages. Two PCS patients (1.57%) had encephalomalacia (left orbitofrontal and right anterior temporal lobes), and no significant difference was found between the two groups (p = 0.5). There was no gross regional or generalized brain atrophy in either of the groups.

The WMH burden in the PCS group was as follows: 15.7% 1–10 lesions, and 6.3%> 10 lesions. The WMH burden in the control group was as follows: 20% 1–10 lesions and 0%> 10 lesions. Although the frequency of WMH in the PCS group was slightly higher than in the control group (22% vs. 20.6%), this was not statistically significant (p = 0.9). Analysis of the location of the WMH showed no significant difference in the number of juxtacortical WMH in the PCS group (18%, 24/127) compared with the control group (10%, 3/29) (p = 0.5). Incidental findings in the PCS group included developmental venous anomaly (7.8%, 10/127) and arachnoid cyst (1.5%, 2/127). Incidental findings in the control group included a small parafalcine meningioma in one patient (3.4%, 1/29).
Discussion
Almost all the PCS patients in this study had a normal MRI brain scan (96.8%) and only four patients (3.1%) had positive structural lesions (two patients had microhemorrhages and two patients had encephalomalacia). No gross brain atrophy was evident. Our results are similar to those reported by two prior publications detailing the low frequencies of structural lesions (0.5–1.5% in concussed pediatric and young patients based on the Zurich 2012 definition of concussion). 25,27 The clinical criteria used to select concussion patients can be expected to affect the incidence of structural lesions in patients with PCS. Most importantly, the clinical criteria for mTBI used by the World Health Organization (WHO), 28 American Academy of Pediatrics, 29 and Department of Defense 30 include patients with an abnormal Glasgow Coma Scale (GCS) of 13 or 14 and focal neurological deficits. Therefore, patients with mTBI represent a more heterogeneous population in terms of neurological deficit including patients with more severe forms of TBI. In contrast, patients with the diagnosis of concussion are more homogeneous and do not have focal neurological deficits. Indeed, the incidence of structural lesions on MRI in patients with mild TBI has been reported to range from 15% to 20% and includes microhemorrhages and WMH. 31,32 Importantly, the presence of structural lesions on conventional MRI is known to correlate with greater clinical severity of TBI. 32 –37
The prevalence of microhemorrhages depends on the MRI sequences employed. SWI has an inherently higher sensitivity than the T2 GRE sequence. 38 Because SWI was not part of our imaging protocol, it is likely that additional microhemorrhages would have been detected had SWI been included in the applied imaging protocol. However, this difference in the sensitivity of GRE versus SWI does not alter our view that patients with any detected microbleeds with either sequence should be excluded from studies of PCS. Prior mTBI studies have shown that microhemorrhages are typically located at the gray matter–white matter junction, indicating that the pontine and periventricular microhemorrhages we observed were atypical and not necessarily related to head trauma. Hasiloglu and coworkers showed that amateur boxers had a higher number of microhemorrhages than controls, but the difference was not statistically significant. Interestingly, their results showed that all the microhemorrhages were located exclusively in the gray matter–white matter junction of the frontal and temporal lobes. 39
Hasiloglu and coworkers 39 also showed a higher prevalence of microhemorrhages (in 10% of the subjects) in amateur boxers than in the control group on 3T MRI; however, the prevalence was not significantly different between boxers (3 cases) and controls (0 cases). Huang and coworkers also showed that there were significantly more microhemorrhages at the gray matter–white matter interface in mTBI patients than in controls. 37 Microhemorrhages in mTBI are also known to become smaller in number and size over time. A recent study by Liu and coworkers showed a 35% reduction in the number of microhemorrhages and a volume reduction of 0.85 mm3/day from baseline (mean 205 days after mTBI) to follow-up imaging (mean 270 days after mTBI). 40 The reduction of susceptibility signals from the microhemorrhages over time is likely attributed to the innate iron clearance mechanisms of the microglia. 36 The incidence of microhemorrhage in our PCS cohort was low. Jarrett and coworkers supported our finding that hemorrhagic lesions including microhemorrhages are not a predominant feature of concussion even with the more sensitive multi-echo SWI technique. 26
WMH is a perplexing imaging pathology in PCS. Although WMH have been reported to be associated with mTBI, 32 WMH has been associated with a myriad of other non-traumatic causes including migraines and chronic microangiopathy. 32 It is also well known that WMH are seen in healthy aging individuals. In fact, it has been shown that healthy subjects in the 30–50 year age range typically have between zero and seven WMH, with the numbers increasing beyond the fifth decade. 41 These confounding variables makes WMH a non-specific indicator of head trauma, although there may be a causal association. In a study of mTBI that included patients with an initial reduction of GCS to 13 and 14, Trifan and coworkers showed a significantly higher rate of WMH (42% vs. 22%) than in controls. 32 In contrast, in our study we found no statistically significant difference in WMH between the PCS and control groups. The location of WMH is purported to be a discriminator between traumatic and non-traumatic causes with a higher incidence of juxtacortical WMH in mTBI and sport-related concussion. 26,42,43 However, in our study we did not find a significant difference in the number of juxtacortical WMH between the PCS and control groups, although there was a trend that showed more WMH in the PCS group.
We must emphasize that the absence of structural lesions in PCS does not imply an absence of neuronal or axonal injuries. For example, more advanced MRI techniques have uncovered non-structural or functional abnormalities. MRI diffusion tensor imaging (DTI) has shown reduced fractional anisotropy, which may represent subtle early microstructural changes within the white matter tracts following mTBI. 44 However, currently there is no established standard DTI biomarker for PCS diagnosis or prediction. 45 Future advances in structural and functional imaging may achieve this goal.
Prior studies have shown that increased severity of TBI is associated with increased cerebral atrophy. 46,47 Trauma associated with loss of consciousness (LOC) results in a greater reduction in brain volume than trauma without LOC. 47 Goswami and coworkers reported significant cortical thinning of the anterior temporal lobe and orbitofrontal cortex in football athletes with a history of multiple concussions (n = 19) as compared with controls (n = 17). 48 Koerte and coworkers also identified decreased cortical thickness in former professional soccer players. 49 In the present study, cerebral atrophy was assessed subjectively and no atrophy was reported. However, subtle atrophic changes might have been detected if brain volumes had been assessed quantitatively
The present study has some limitations, including the use of GRE with a lower sensitivity for detecting microhemorrhages than SWI. 50,51 Therefore, we must caution that the interpretation of the specific incidence of hemorrhages is only applicable to our MRI protocol and magnet field strength. Further, our study was not longitudinal, and this is important because microhemorrhages can fade over time. Nevertheless, MRI serves as an important tool for differentiating more severe TBI, such as those with hemorrhages, from those with a concussion and subsequent PCS. Our recommendation for brain MRI in this population includes the use of either T2* GRE or SWI sequences, and when possible obtaining the scan during the 1st month of injury. On the other hand, WMH can increase over time, as is seen in athletes when comparing serial MRI studies from preseason to post-season. 26 In contrast, we studied only one time point and included a variety of concussion causes. The sample size of the control group was also relatively small, and, therefore, some of the group comparisons lacked statistical power. Finally, image analysis was performed using qualitative evaluation of the WMH and atrophy instead of measuring volumes. This could account for a lack of sensitivity for detecting relevant between-group differences.
Conclusion
The diagnosis of PCS has been challenging because of the lack of a consensus concerning the clinical definition and the absence of strict, well-defined neuroimaging criteria. In our study, structural lesions such as contusion, atrophy, and microbleeds are rare in PCS, indicating that the presence of such lesions represents a more severe form of TBI. Because WMH are as common, or nearly as common, in healthy controls as they are in individuals with PCS, their presence offers no increase in specificity. Therefore, WMH should not be used as an indicator of trauma-related axonal injury in this patient group. We therefore propose that the neuroradiological criteria for the diagnosis of PCS be as follows: (1) a structurally normal MRI with no evidence of generalized or focal cerebral tissue loss (atrophy and/or gliosis) but with the caveat that WMH are permitted, and (2) no evidence of intracranial hemorrhage. These imaging criteria therefore enable the use of strict clinical and MRI definitions for obtaining homogeneous patient cohorts for examination of the consequences of concussion such as PCS. It should also be kept in mind that the dependence on microhemorrhages for indicating brain injury is most useful in the 1st month after injury, as the hemorrhage can fade thereafter.
Footnotes
Funding Information
This study was funded by the Ontario Brain Institute, Canada, and the Canadian Concussion Centre, Toronto Western Hospital.
Author Disclosure Statement
No competing financial interests exist.