
Abstract
Pairing vagus nerve stimulation (VNS) with rehabilitation has emerged as a potential strategy to enhance plasticity and improve recovery in a range of neurological disorders. A recent study highlights the therapeutic promise of VNS in promoting motor recovery after spinal cord injury (SCI). We investigated the safety of acute VNS in a rat model of chronic SCI. We measured the cardiovascular response to various VNS paradigms following chronic high-thoracic SCI that is known to deleteriously impact cardiovascular control. Dose-response experiments with continuous VNS revealed an SCI-dependent increase in sensitivity for heart rate (HR) and blood pressure (BP) compared with controls. A clinically relevant intermittent VNS resulted in transient reduction in HR in rats with SCI; however, BP remained unaltered. In all experiments, the effect lasted only while the VNS stimulus train was present, as HR and BP restored to baseline values as soon as VNS ended. No prolonged episodes of persisting hypotension were seen in either group. Further, VNS did not trigger autonomic dysreflexia or exacerbate the severity of autonomic dysreflexia when induced during or after stimulation sessions. Overall, these findings provide initial evidence that intermittent VNS at parameters used for targeted plasticity therapy (30 Hz, 0.8 mA) appears safe and supports further investigation of this potential therapy for use following SCI.
Introduction
Debilitating functional impairments following spinal cord injury (SCI) are often attributed to morphological and physiological maladaptations in neural circuits. With insufficient or maladaptive spontaneous plasticity following SCI leading to potentially permanent disability, meaningful functional recovery remains largely dependent upon appropriate reorganization of neural circuitry. 1 Conventional rehabilitative therapies following SCI have shown modest circuit reorganization, leading to limited functional improvements. 2 However, this principle lays the foundation for pairing a task-specific training with plasticity-augmenting strategies to reinforce the neural connections activated during the task and further enhance the beneficial effect of rehabilitation. 3,4
Recently, vagus nerve stimulation (VNS) has received considerable attention as a means to promote synaptic plasticity in combination with rehabilitation. 5 Short bursts of closed-loop VNS drive rapid, phasic activation of pro-plasticity neuromodulatory networks concurrent with rehabilitation to enhance plasticity. 6 –10 A number of pre-clinical studies demonstrate that pairing VNS with rehabilitation facilitates synaptic plasticity in spared networks and improves recovery of motor function after stroke. 11 –14 Recent clinical findings corroborate these results and highlight the clinical potential of VNS therapy. 15,16
Building upon these findings, our team has recently shown that closed-loop VNS paired with a rehabilitative training for a motor task significantly improves recovery of forelimb function following cervical SCI in rats. 17 Although these results provide a framework for the development of this strategy to augment plasticity in individuals with SCI undergoing rehabilitation, its safety in subjects with SCI remains to be thoroughly investigated. This is crucial due to the predominant role of the vagus nerve in autonomic function and the fact that cervical or high-thoracic SCI leads to disruption of spinal sympathetic control. Further, not only does SCI result in cardiac structural and functional impairments, 18,19 in addition the affected individuals often experience paradoxically unstable blood pressure (BP) that presents as episodes of extreme hypertension (e.g., autonomic dysreflexia) or profound hypotension (e.g., orthostatic hypotension). Autonomic dysreflexia is a condition in which afferent peripheral inputs (e.g., stimuli from bowel routine) result in rapid hypertensive episodes with BP often reaching beyond 300 mm Hg. 20,21 Moreover, the same individuals with SCI are also prone to episodes of abnormally low arterial BP when assuming an upright posture, a condition called orthostatic hypotension. 22,23
Given the myriad cardiovascular consequences of SCI and the direct implications of VNS in modulation of autonomic tone, it is essential to assess the safety of VNS in subjects with SCI. The present study is a preliminary investigation of cardiovascular effects of VNS in rats with high-thoracic (T3 spinal segment) complete transection SCI, an injury model that predisposes them to severe cardiovascular
Methods
Animal surgery and post-surgical care protocols were approved by the University of British Columbia Animal Care Committee and were performed in strict compliance with the policies established by the Canadian Council on Animal Care (institutional approval certificate number A18-0183). A schematic drawing of the surgical procedures is shown in Figure 1.

Schematic representation of surgical procedures.
SCI surgery
Eleven adult (∼300 g), male Wistar rats (Harlan Laboratories, Indianapolis, IN) were used in this study. Six rats received SCI and were euthanized at 1 month post-injury. Five rats received no SCI and served as age-matched uninjured controls.
Surgical procedures and post-operative care were performed as described previously. 24,25 Beginning 3 days prior to SCI, rats received a daily subcutaneous injection of prophylactic enrofloxacin (Baytril, 10 mg/kg; Associated Veterinary Purchasing [AVP], Langley, BC, Canada). On the day of the surgery, animals were anesthetized using 5% isoflurane mixed with oxygen (2 L/min) and maintained under surgical plane at 1.5–2% isoflurane. Subcutaneous injections of enrofloxacin (10 mg/kg), buprenorphine (Temgesic®, 0.02 mg/kg; McGill University, Montreal, QC, Canada), and ketoprofen (Anafen®, 5 mg/kg; AVP) were administered prior to SCI and continued for 3 days post-SCI.
A dorsal midline skin incision was made followed by incisions through the muscles overlying vertebrae C8 to T4. A laminectomy was performed at the T2 vertebra to expose the T3 spinal cord segment. The dura mater was incised using a 30-guage needle and a complete transection was made using micro-scissors and gentle vacuum aspiration. 26 Lesion completeness was confirmed using visual inspection and a pledget of Gelfoam (Pharmacia & Upjohn Company, Pfizer Inc., New York, NY) was transiently placed between the stumps to achieve hemostasis. The dura was closed using 9–0 Prolene sutures. 27 The muscle and skin were closed with 4–0 Vicryl and 4–0 Prolene sutures, respectively. Following surgery, animals received 5-mL subcutaneous injections of warm Lactated Ringer's solution (Baxter Corp., Mississauga, ON, Canada) and were allowed to recover in a temperature-controlled environment (Animal Intensive Care Unit, Lyon Technologies, Los Angeles, CA) before returning to home cages. Urinary bladders were manually expressed two to three times daily until spontaneous voiding returned (∼10 days post-injury).
Implantation of VNS cuff
Surgical procedure for VNS cuff implantation was performed as previously described. 11,14,17 At 30 days post-SCI, rats were anesthetized with isoflurane and placed in a stereotaxic apparatus. An incision was made down the midline of the head to expose the skull. Three bone screws were inserted into parietal bones of the skull along the sagittal suture to act as an anchor for a two-channel head connector that was mounted to the screws using acrylic. The rat was transferred from the stereotaxic apparatus into a supine position. An incision was made on the left side of the neck and the overlying musculature was blunt dissected to expose the left cervical segment of the vagus nerve. The nerve was gently isolated from the carotid artery and placed into a bipolar cuff electrode. 28 The two electrode leads were tunneled subcutaneously and connected to the two-channel connector mounted on the skull. Cuff functionality was visually confirmed by a cessation of breathing in response to a stimulation train of VNS consisting of 0.8 mA, 0.1-msec biphasic pulses at 30 pulses/sec. Once cuff efficacy was confirmed, head and neck incisions were sutured close with 4–0 Prolene sutures and the animals were advanced toward telemeter implantation surgery.
Implantation of wireless telemeter
Immediately following the VNS cuff implantation, the rats were implanted with a wireless solid-state pressure sensing telemeter (TRM54P; Kaha Sciences, Auckland, New Zealand). Prior to implantation, the telemeters were washed in Tergazyme (MilliporeSigma Canada Co., Toronto, ON, Canada) and were gas-sterilized with ethylene oxide. With the rat placed in the supine position, a skin incision was made in the inguinal region. Blunt dissection was performed to separate the connective tissue and expose the femoral artery and vein. The femoral artery was elevated using silk ligatures and punctured using a curved needle. The pressure sensing tip was inserted and advanced medially toward the abdominal aorta. The catheter wire was secured within the artery using a silk ligature. The abdominal region rostral to the incision was blunt dissected under the skin and the body of the telemeter was placed subcutaneously prior to suturing the skin using 4–0 sutures. The rat was allowed to recover at least 1 h prior to physiological experiments.
Hemodynamic monitoring and VNS delivery
All experiments were performed in conscious, freely moving animals without any restraint. Animals implanted with a VNS cuff and wireless telemeter were placed on a telemetry SmartPad (TR181; Kaha Sciences, Auckland, New Zealand). Beat-by-beat BP and HR were recorded at rest for 1 h. Prior to initiation of VNS, the severity of autonomic dysreflexia was tested. Autonomic dysreflexia was induced by colorectal distension (CRD) using a 2-mm latex balloon-tipped catheter, as described previously. 29,30 Following a baseline recording, the balloon was inflated with 2 mL of air over 10 sec, and maintained for 60 sec. Hemodynamic parameters were recorded before (baseline), during (distension), and after (recovery) balloon inflation.
VNS was delivered using an isolated current-controlled stimulator (Model 2100; A-M Systems Inc., Sequim, WA) via the two-channel connecter mounted on the animal's head. Voltage traces were confirmed using a digital oscilloscope (PicoScope® 2204A; Pico Technology, Tyler, TX). Dose-response curves of HR and BP changes in response to VNS were created by delivering 10-sec trains of continuous biphasic 0.1-msec pulses at 30 Hz and multiple intensities ranging from 0.2 mA to 2 mA in steps of 0.2 mA. After each train, the animal was allowed to recover. Following continuous VNS, the animals were subjected to an intermittent VNS protocol. Short 0.5-sec trains consisting of biphasic 0.1-msec pulses at 30 Hz and 0.8 mA were delivered either every 5 sec or every 15 sec. Intermittent stimulation was delivered until at least 240 stimulation trains were delivered (i.e., 1 h of stimulation). To assess the impact of VNS on an accidental autonomic dysreflexia in patients, episodes of experimental autonomic dysreflexia were triggered in rats using CRD during the intermittent VNS as well as after cessation of the VNS protocol.
Statistical analysis
The magnitude of the change in hemodynamic parameters in response to continuous 10-sec VNS was calculated as the difference between the baseline values and the lowest peak obtained during stimulation. For intermittent 0.5-sec VNS, HR during each stimulation was calculated by counting the number of pulses in a 1-sec window centered on the negative peak (identified using the peak finder function in MATLAB [MathWorks Inc., Natick, MA]). BP values at baseline and in response to VNS were calculated by taking the mean value within the same windows. For severity of autonomic dysreflexia, the difference in systolic BP (SBP), mean arterial pressure (MAP), diastolic BP (DBP), and HR from baseline and the peak value during distension was calculated.
Data are reported as mean ± standard error of the mean (SEM). Dose-response curves between SCI and uninjured animals were compared using a two-way repeated measures analysis of variance (ANOVA). Paired t-tests were performed to determine a significant change in hemodynamic parameters in response to VNS. A one-way ANOVA was performed to compare the severity of autonomic dysreflexia before, during, and after cessation of VNS.
Results
Physiological experiments were broadly divided into three stimulation paradigms. First, VNS was delivered continuously to confirm stimulation efficacy as well as to investigate the resting cardiovascular response to VNS doses (Fig. 2). Second, a clinically relevant intermittent stimulation protocol was delivered to animals at rest (0.8 mA for 1 h) to assess the effect of a prolonged exposure to VNS (Fig. 3). Third, to determine the potential influence of VNS on the severity of autonomic dysreflexia, individual episodes of autonomic dysreflexia were experimentally triggered via CRD prior to, during, and after cessation of 1 h of intermittent VNS (Fig. 4). Further, the BP was continuously monitored throughout the experiments to screen for sporadic hypotensive or hypertensive episodes as a consequence of VNS.
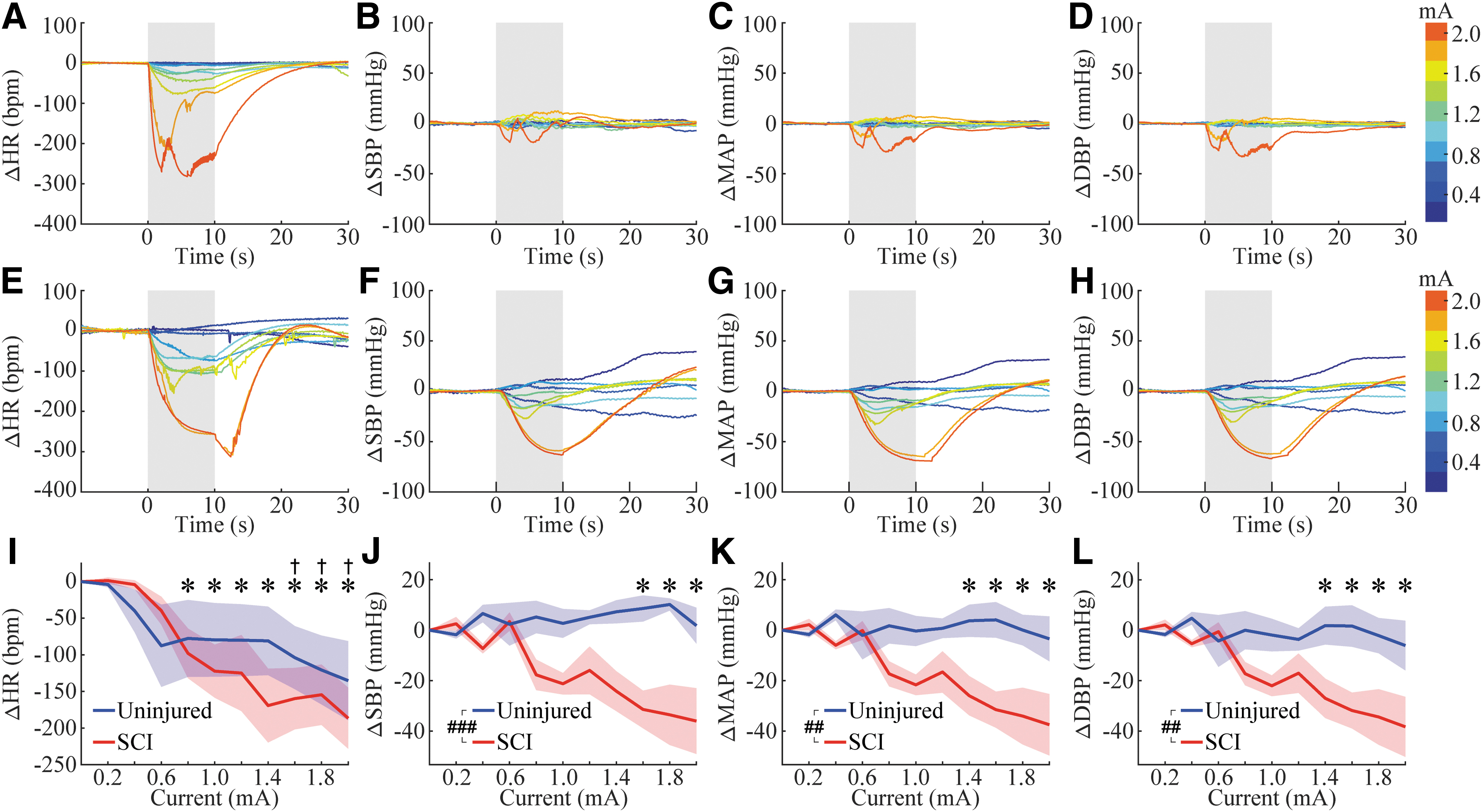
Cardiovascular dose-response to increasing amplitude of continuous VNS. (
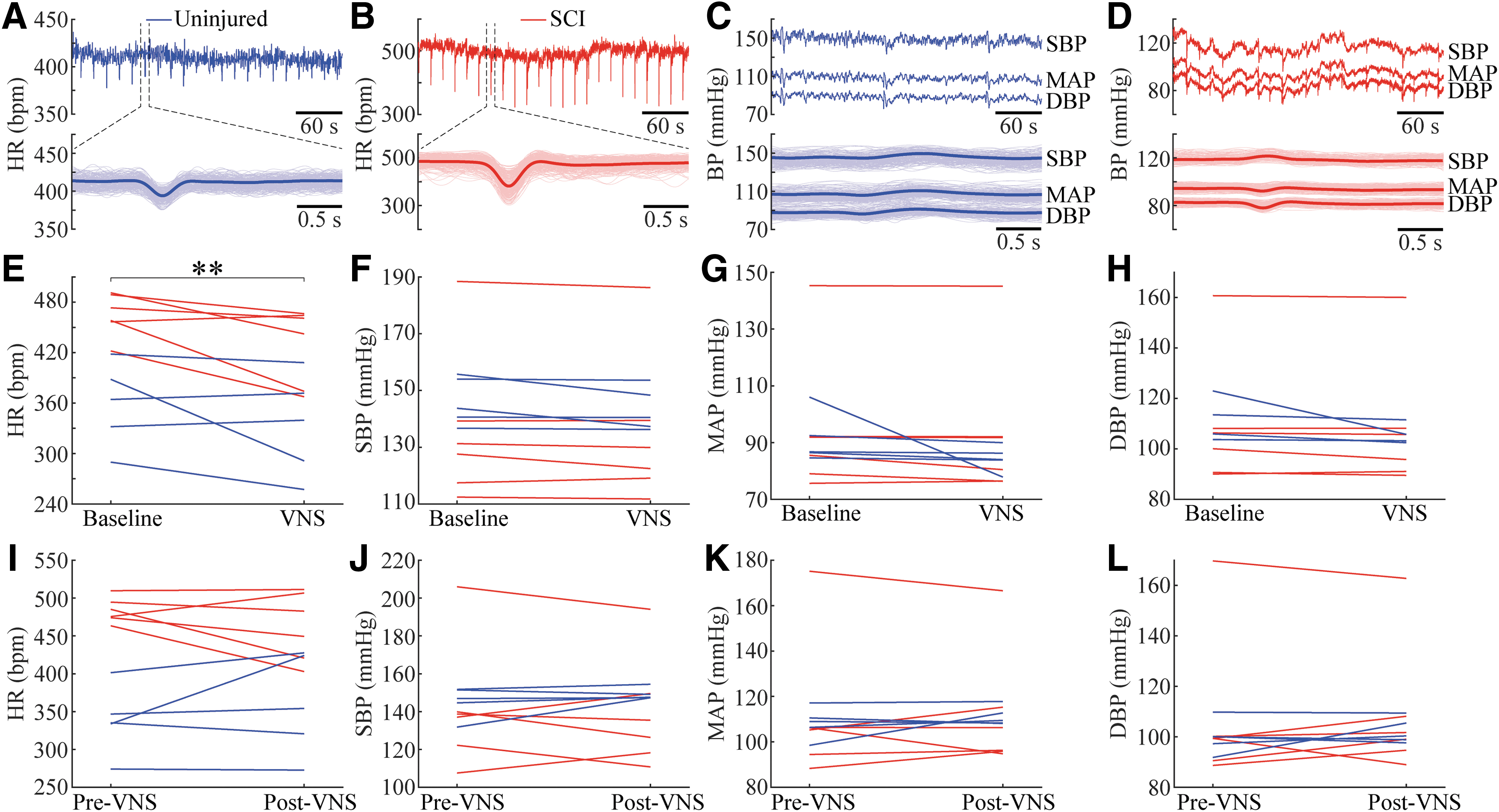
Cardiovascular responses to intermittent 0.8 mA VNS.
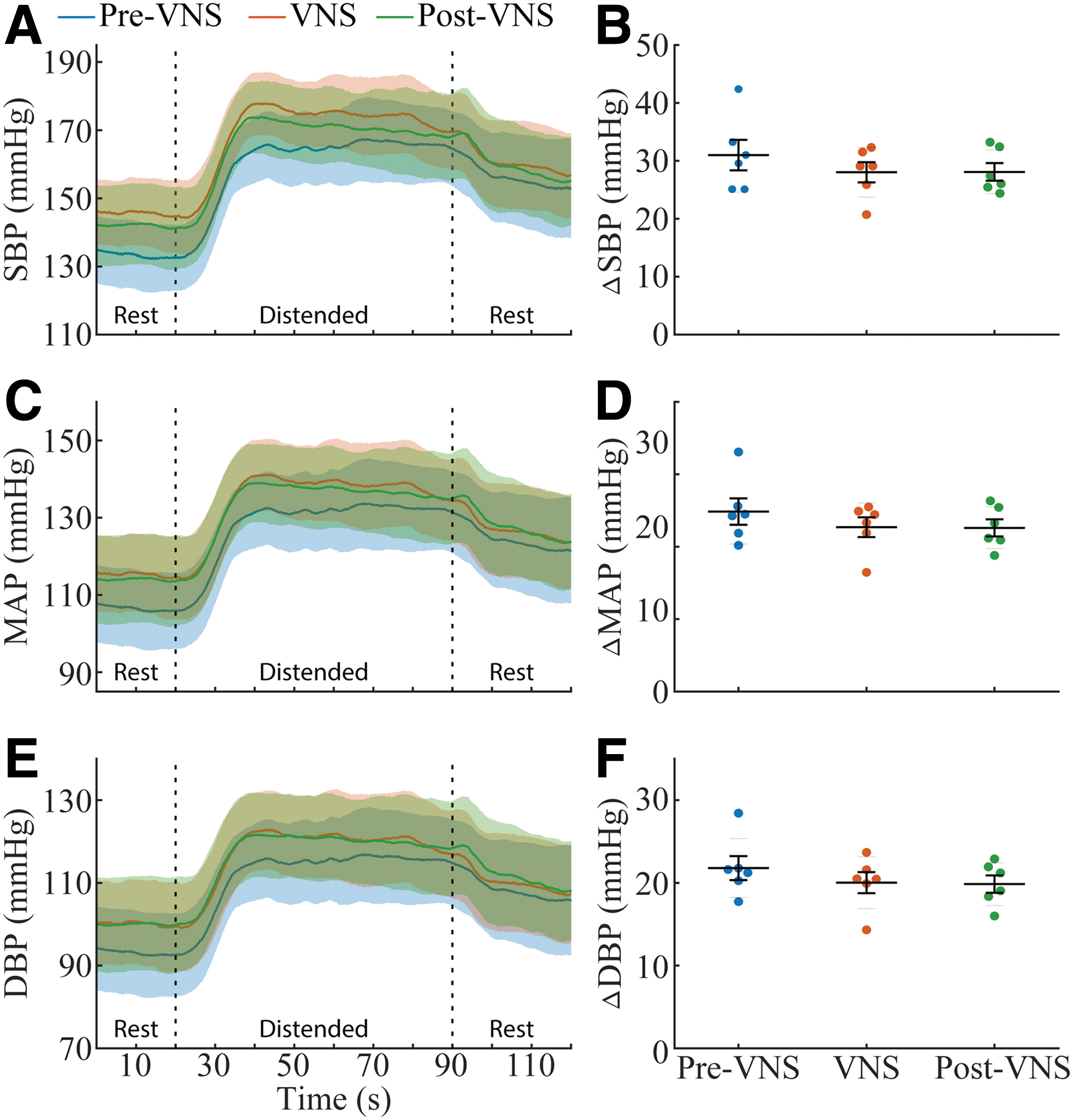
VNS does not affect the severity of autonomic dysreflexia.
Continuous VNS modulates resting cardiovascular response
We first sought to confirm the stimulation efficacy by investigating HR and BP responses to long, continuous trains of VNS. Representative HR and BP traces in response to various current amplitudes (0.2–2.0 mA) are shown for an uninjured rat (Fig. 2A–D) and a rat with SCI (Fig. 2E–H). Overall, as a function of current amplitude, continuous VNS resulted in significant reductions in HR in both SCI and uninjured control groups (Fig. 2I), whereas significant reduction in BP was seen only in rats with SCI (Fig. 2J–L). Two-way ANOVA (group vs. current amplitude) revealed an effect of current in all hemodynamic parameters (Fig. 2I–L; HR: p = 1.45*10^-6, SBP: p = 0.021, MAP: p = 0.0018, and DBP: p = 0.0017). Additionally, there was a negative correlation between stimulation amplitude and the change in HR in both uninjured and SCI animals (SCI: p = 1.187 × 10-6, R2 = 0.3619; uninjured: p = 0.0207, R2 = 0.1066). There was a negative correlation between stimulation amplitude and the change in BP in SCI animals (SBP: p = 2.4865 × 10-6, R2 = 0.3444; MAP: p = 2.8842 × 10-7, R2 = 0.3942; DBP: p = 1.0135 × 10-7, R2 = 0.4171), but not uninjured animals (SBP: p = 0.2831, MAP: p = 0.8569, DBP: p = 0.6532). The raw values for hemodynamic parameters at rest and in response to continuous VNS are shown in Table 1.
Hemodynamic Parameters at Rest and in Response to Continuous VNS
Indicates significantly different from resting state prior to VNS.
Data presented as mean ± SEM.
DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure; SBP, systolic blood pressure; SCI, spinal cord injury; SEM, standard error of the mean; VNS, vagus nerve stimulation.
In all experiments with continuous VNS where a reduction in HR and BP was observed, the effect lasted only while the VNS stimulus train was present. The cardiovascular indices restored to baseline values within seconds after the VNS was turned off. No episodes of low BP were present after cessation of VNS.
Intermittent VNS at 0.8 mA transiently reduces resting HR following SCI
Next, we tested whether short bursts of intermittent VNS, equivalent to those used in studies that pair VNS with rehabilitation, would elicit significant cardiovascular changes. Individual representative HR traces in response to intermittent VNS (0.8 mA, every 15 sec) in an uninjured rat and a rat with SCI are shown in Figure 3A and Figure 3B, respectively. The BP responses from the same individual animals are shown in Figure 3C and Figure 3D, respectively. Intermittent VNS led to a transient, yet significant, reduction in HR (Fig. 3E) in the SCI group (p = 0.0013) but not in uninjured controls (p = 0.1470). No significant effects of VNS were seen in BP for either group (Fig. 3F–H; SCI, Baseline vs. VNS, paired t-test, SBP: p = 0.3575, MAP: p = 0.4172 and DBP: p = 0.1560; Uninjured, SBP: p = 0.1267, MAP: p = 0.2049, and DBP: p = 0.2269). The raw values for hemodynamic parameters at rest and in response to intermittent VNS are shown in Table 2.
Hemodynamic Parameters at Rest and in Response to Intermittent VNS
Indicates significant difference.
Data presented as mean ± SEM.
DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure; SBP, systolic blood pressure; SCI, spinal cord injury; SEM, standard error of the mean; VNS, vagus nerve stimulation.
Similar to continuous VNS, the stimulation-induced reduction in HR was observed only while the stimulus train was present. HR was restored to baseline values as soon as the pulse train ended. No episodes of hypotension were present after the completion of VNS. To examine a potential impact of multiple trains of VNS over time (240 intermittent stimulations every 15 sec; i.e., 1 h duration), mean values of HR and BP were compared before and after 1 h of VNS (Fig. 3I–L). No difference was observed in any parameters before and after prolonged VNS in rats with SCI (HR: p = 0.212, SBP: p = 0.581, MAP: p = 0.977, and DBP: p = 0.723) or uninjured controls (HR: p = 0.305, SBP: p = 0.279, MAP: p = 0.371, and DBP: p = 0.432).
Intermittent VNS at 0.8 mA does not trigger or exacerbate autonomic dysreflexia
In addition to assessing resting hemodynamics, we tested the potential impact of VNS on reflex hypertensive episodes (i.e., autonomic dysreflexia) that occur frequently in response to routine stimuli. CRD was performed prior to VNS experiments, during the 1 h intermittent VNS, as well as between 5 and 10 min after completion of the VNS experiment (Fig. 4A,C,E). The comparison of severity of autonomic dysreflexia revealed no effect of VNS (Fig. 4B,D,F; one-way ANOVA; SBP: p = 0.704, DBP: p = 0.746, and MAP: p = 0.711). Additionally, VNS itself did not result in autonomic dysreflexia throughout the experiments.
Discussion
VNS has emerged to be a widely applicable approach in strengthening synaptic plasticity, with implications for treating sensory, motor, and cognitive dysfunction in various disease conditions. 4 The vagus nerve primarily comprises afferent projections to the brainstem, and VNS drives rapid activation of pro-plasticity neuromodulatory networks. 6 –8 VNS-dependent engagement of these neuromodulatory networks, including the noradrenergic, cholinergic, and serotonergic systems, are coincident with training results in the potentiation of training-specific plasticity. 9,10 Based on this enhancement of plasticity, the use of closed-loop VNS paired with rehabilitative training has been investigated as a means to improve recovery after neurological injury. A number of pre-clinical studies in models of stroke indicate that VNS paired with rehabilitative training enhances plasticity in spared networks and improves motor recovery. 11 –14 Highlighting the clinical potential of this strategy, recent studies demonstrate the safety and feasibility of VNS in chronic stroke patients and a Phase 3 clinical trial investigating its efficacy is underway. 15,16
Building on these studies, a similar implementation of VNS paired with rehabilitation has been employed as a potential therapy to improve motor recovery following SCI. 17 However, in addition to sensorimotor impairments, SCI disrupts sympathetic vasomotor control and presents with severe cardiovascular dysfunctions. With sympathetic and parasympathetic innervations typically functioning antagonistically, a disruption of sympathetic pathways after SCI predisposes an individual to unopposed parasympathetic vagal control, resulting in marked bradycardia and asystolia. 31 Therefore, to determine whether VNS represents a viable therapeutic strategy in the context of SCI, it is critical to characterize whether therapeutic VNS can exacerbate already imbalanced cardiovascular control. Further, individuals with SCI experience hypertension and hypotension (during autonomic dysreflexia and orthostatic hypotension, respectively) numerous times per day. 21,32 These bidirectional oscillations in BP can inversely alter HR via baroreflex-driven changes in vagal tone, making an individual with SCI susceptible to bradycardia, tachycardia, arrhythmia, or even cardiac arrest. 33 Although vagus nerve is primarily afferent in function, it is necessary to examine whether active stimulation of a small proportion of efferent projections during VNS can elicit a more pronounced effect on HR, especially in the absence of an intact, opposing sympathetic control.
With cardiovascular impairments most commonly present in individuals with high paraplegia or tetraplegia (SCI above T6), we investigated the resting and reflex cardiovascular responses in a representative model of chronic SCI. The T3 SCI model has been extensively characterized in terms of cardiovascular dysfunction such as autonomic dysreflexia, 34,35 orthostatic hypotension, 36 and cardiac structural and functional impairments. 18,37
While measuring beat-by-beat BP and HR, rats were subjected to continuous VNS of increasing amplitudes between 0.2 and 2.0 mA, as well as to short bursts of intermittent VNS at a constant amplitude of 0.8 mA. The amplitude of 0.8 mA was chosen for intermittent, long-term VNS because of its known applicability in studies pairing VNS with rehabilitation to promote functional recovery. 15,16 It is noteworthy that VNS parameters being employed in targeted plasticity following SCI administer 100 times less current than those approved by the U.S. Food and Drug Administration (FDA) for treatment of epilepsy and depression. 38 We show that despite an SCI-dependent increase in cardiovascular sensitivity to continuous VNS, the effects are transient and only observed during stimulation. Importantly, prolonged intermittent VNS at therapeutically relevant doses does not instigate aberrant hypotensive or hypertensive episodes similar to orthostatic hypotension or autonomic dysreflexia, which are hallmarks of cardiovascular dysfunction in individuals with upper thoracic or cervical SCI. Finally, autonomic dysreflexia was triggered using CRD, a widely accepted procedure that resembles stimuli (e.g., bowel maneuvers) that commonly instigate AD in individuals with SCI. 39,40 We observed that VNS does not exacerbate or improve experimentally induced episodes of autonomic dysreflexia.
The present study provides initial evidence that VNS does not yield lasting perturbations in cardiovascular function or affect autonomic dysreflexia after SCI. These findings support the safety of VNS as a post-SCI intervention. However, despite the demonstrated safety, it needs to be acknowledged that the present study is a cross-sectional investigation. Future work will be aimed at evaluating the consequences of long-term VNS in acute and chronic SCI.
Footnotes
Funding Information
The present study is supported by funds from Wings for Life Foundation (WFL-US-11-16; PI: Dr. Michael Kilgard). Dr. Hays's laboratory is additionally supported by funds from the National Institutes of Health (R01 NS094384 and UG3 NS109497), and the Defense Advanced Research Projects Agency Targeted Neuroplasticity Training program under the auspices of Dr. Tristan McClure-Begley through the Space and Naval Warfare Systems Center, Pacific Grant/Contract No. N66001-17-2-4011. Dr. Krassioukov's laboratory is supported by funds from the Heart and Stroke Foundation, Canadian Foundation for Innovation, BC Knowledge Development Fund, Craig H. Neilsen Foundation, and Seed grants from the International Collaboration on Repair Discoveries. Dr. Sachdeva is supported by Postdoctoral Fellowships from the Craig H. Neilsen Foundation, Canadian Institutes of Health Research, Michael Smith Foundation for Health Research, and the University of British Columbia (Bluma Tischler Postdoctoral Fellowship).
Author Disclosure Statement
No competing financial interests exist.