
Abstract
Evidence suggests that pediatric traumatic brain injury (TBI) may be causally related to alcohol misuse later in life; however, the nature and extent of the association has not been well described. This study examined the relationship between pediatric TBI and adult alcohol misuse in a population sample ≥20 years of age. We sought to determine (1) whether first self-reported incidence of TBI with loss of consciousness (LOC) before the age of 20 increased the risk for alcohol misuse later in life; and (2) whether sex, injury severity, and age at time of injury modified the association. We found a greater likelihood of binge but not heavy drinking for those whose first self-reported TBI with LOC occurred before the age of 20 when compared with those whose first self-reported TBI with LOC occurred later in life (28.5% vs. 20.4%, p = 0.003). When limited to those with only mild TBI, the relationship to binge drinking remained significant (31.9% vs. 19.3%, p < 0.001) and was evident for both males (38.4% vs. 25.6%, p = 0.016) and females (20.9% vs. 12.4%, p = 0.044). When controlling for sex, age, and race/ethnicity, reporting a first TBI with LOC before age 20 was associated with binge drinking only for those with mild TBI (adjusted odds ratio [AOR] = 1.32; 95% confidence interval [CI] = 1.00–1.74). Results also showed that those with first TBI with LOC occurring between the ages of 10 and 19 years were more likely to binge drink as adults than those first injured earlier in life, regardless of TBI severity. Further research is needed at both the epidemiological and pre-clinical levels to better understand this relationship.
Introduction
Prior studies suggest that childhood events, such as traumatic brain injury (TBI), may precipitate the development of substance use and other behavioral health disorders in later life. 1 –4 Studies designed to investigate the relationship between pediatric TBI and alcohol abuse can be generally categorized into two groups: (1) population surveys in which systematic canvasses were conducted and weighted to the characteristics of the specific population 5 –7 ; and (2) birth cohort studies in which children from a specified geographical area were prospectively followed and data were extracted periodically. 1 –4,8,9 These approaches yield advantages and disadvantages. Population surveys are limited by their reliance on self-reported TBI history and substance abuse outcomes. Birth cohort studies generally do not capture injuries that are not treated in a healthcare setting. Therefore, the patterns of injuries reported in these studies may not represent a full picture of TBI incidence. TBIs do not always result in contact with a healthcare provider, 10 and even if one does occur, TBI diagnoses are commonly missed. 11 Birth cohorts are generally limited in time and therefore may not detect the emergence of sequelae later in life. Despite these limitations, evidence from a number of studies have lent support to the general relationship between childhood TBI and substance use disorders; 1,5,12 for example, Bogner and colleagues reported that persons with at least one TBI with loss of consciousness (LOC) were 50% more likely to binge drink and 70% more likely to be heavy drinkers than persons without that injury history. 7 However, the evidence for alcohol use disorders is more modest than other adult consequences. 4,5,7 Additionally, other psychological variables that can result from TBI, including risk-taking and impulsivity, can obscure the relationship. A birth cohort reported by Kennedy and colleagues, 3,4 which indicated such a causal relationship between TBI and alcohol abuse, also appears to be independent of the above mentioned confounds. Interestingly, this relationship appeared to be specific to alcohol because there was no association of TBI with cannabis or nicotine use at least when measured at 17 years of age. 3
Pre-clinical studies have attempted to reveal the neural substrates that underlie the development of substance-abuse-related behaviors following early life injuries. We have demonstrated previously that mild TBIs increase alcohol self-administration behavior in mice. 13 However, this phenomenon was specific to the age of injury and sex of the animals. Female mice injured early in life drank more alcohol than did sham-injured females, or females injured only as adults. In all cases, females drank more than males and injury had no effect on self-administration behavior among males. This increase in alcohol self-administration behavior among females injured early in life was associated with increased conditioned place preference responses to intraperitoneal alcohol. Despite methodological differences among animal studies, these data largely agree with other pre-clinical data, although most studies have focused on adult males. 14 –16
Therefore, epidemiological and pre-clinical data support the possibility that childhood brain injury can cause alcohol misuse. 17 Although the specifics of this relationship remain unspecified, the pre-clinical and epidemiological data suggest that key variables including sex, age, and severity of injury could be critical determinants of substance abuse risk. The present study aimed to evaluate the relationship between pediatric TBI and adult alcohol misuse in an Ohio population sample ≥20 years of age. Specifically, we hypothesized that incurring one's first TBI with LOC before the age of 20 increased the risk for alcohol misuse (i.e., binge drinking or heavy drinking) later in life, relative to first exposure at or after age 20. We further hypothesized that sex, severity of injury, and age at injury would modify these relationships.
Methods
Sample
Survey respondents were a random sample of Ohio non-institutionalized adults ≥20 years of age who completed the core component questions and the lifetime history of TBI optional module of the 2014, 2016, or 2017 Ohio Behavioral Risk Factor Surveillance System (BRFSS) survey and who self-reported a lifetime history of at least one TBI with LOC (n = 2935). There were 66 respondents who did not report their age at first injury, resulting in a final cohort of 2869 cases. To ensure that results were representative of the Ohio adult, non-institutionalized population, the sample was reweighted. The final weight was calculated by multiplying the sample weight for each individual year by its sample size proportion of the combined data set (Table 1).
Demographic and Injury Related Characteristics by Age at First TBI
LOC, loss of consciousness; TBI, traumatic brain injury; GED, General Education Development.
More than three fourths of the sample had experienced mild TBI with LOC. Almost two thirds had experienced their first self-reported incidence of TBI with LOC before the age of 20. Those first injured in childhood or adolescence were relatively evenly distributed among those with the first self-reported TBI before age 10 (18.3%), between the ages of 10 and 14 years (21.6%) and between the ages of 15 and 19 years (25.6%). The majority of the cohort were male (58.4%), white non-Hispanic (86.4%), and <65 years of age (85.2%). The departure of other demographic characteristics from the general population were consistent with previous findings, including that they were less likely to be married, had more children in the household, had lower educational attainment and lower income, and were less likely to be employed. 18
Procedures
The study used de-identified, archival data provided by the Ohio Department of Health (ODH) BRFSS program, and therefore was considered exempt from human subjects review by the host institutional review board. The Ohio BRFSS is an annual, cross-sectional state-based random telephone survey of non-institutionalized adults, ≥18 years of age, regarding their health-related risk behaviors, chronic health conditions, and use of preventive services. 19 The Ohio BRFSS, which is federally funded and jointly administered by the Centers for Disease Control (CDC) and the ODH, contains core component questions used nationally to collect demographic and health-related data. In 2014, 2016, and 2017, the Ohio BRFSS also included a state-added module on lifetime history of TBI.
The BRFSS utilizes design weighting and iterative proportional fitting, incorporating telephone ownership (land line and/or cell phone), education level, marital status, and renter versus owner status, in addition to known proportions of age, race/ethnicity, sex, and geographic region in Ohio. 19 Applying the sample weights, the Ohio BRFSS can be representative of the Ohio adult, non-institutionalized population. The state-added module on lifetime history of TBI included on the Ohio BRFSS is adapted from The Ohio State University (OSU)-TBI ID, a validated tool with strong inter-rater reliability (intraclass correlation coefficients [ICC] 0.85–0.96) and acceptable to excellent test/retest reliability (κ = 0.60–0.91). 20 –23 Criterion-related validity is supported by relationships between indicators of lifetime history and measures of cognitive performance and affective functioning, as well as structure and function of the brain observed via neuroimaging. 20,22,24 –27 Questions asked in the lifetime history of TBI module include the number, cause, and severity of TBIs with LOC experienced in their lifetime, and age at which they sustained their first TBI with LOC.
Measures
The main outcome variables of interest were: (1) self-reported binge drinking during the preceding month (“binge drinking”) and (2) self-reported heavy drinking during the preceding month (“heavy drinking”). The main exposure variables were: (1) age at first TBI with LOC (< 20 years vs. ≥20 years) and (2) sex (female vs. male).
Alcohol misuse was measured using two items: (1) self-reported binge drinking during the preceding month, defined as ≥5 drinks on one occasion for men or ≥4 for women, and (2) self-reported heavy drinking during the preceding month, defined as >14 drinks per week for males and >7 drinks per week for females. A binary response category was used for these two items.
Age at first TBI with LOC was measured as the age at which the individual sustained his/her first TBI with LOC, which was coded as a dichotomous variable (i.e., first TBI with LOC at <20 years vs. ≥20 years).
Sex was coded as male or female.
TBI severity was measured based on the self-reported length of LOC and categorized into one of three groups: (1) LOC for <5 min, (2) LOC for 5–30 min, or (3) LOC for >30 min. The response categories of LOC for <5 min and LOC for 5–30 min were combined to capture all “mild TBIs”) (i.e., TBI with LOC for ≤30 min).
Other variables included in the analyses were study year (2014, 2016, or 2017), age at time of survey completion (20–44 years, 45–64 years, or ≥65 years of age), and race/ethnicity (white non-Hispanic, black non-Hispanic, or all others). These variables were treated as potential covariates in the analyses.
Statistical analysis
Descriptive statistics (means and standard deviations or frequencies and percentages) were examined for key variables. All variables were compared between individuals with the first self-reported TBI with LOC at <20 years versus those with the first self-reported TBI with LOC at ≥20 years using χ 2 tests.
Adjusted logistical regression models were constructed to ascertain the odds ratios (OR) for binge (or heavy) drinking between individuals with their first self-reported incidence of TBI with LOC at <20 years and those with their first self-reported incidence of TBI with LOC at ≥20 years. We used the same logistical modeling to examine sex with the addition of an interaction term (sex by age at first TBI with LOC). Variables adjusted in the logistical regression models were sex, age, and race/ethnicity. Analytical models were repeated for the subgroup of the sample who sustained a mild TBI (i.e., LOC for ≤30 min). Complex survey design variables (strata, clusters, and weights) were incorporated into the analyses. To calculate unbiased confidence intervals (CIs) and p values, domain analysis was utilized (keep all non-TBIs in the analysis).
Results
As shown in Table 2, a higher prevalence of current binge drinking was observed among adult Ohioans whose first self-reported incidence of TBI with LOC occurred before the age of 20 than in those whose first self-reported TBI with LOC occurred at or after age 20 (28.5% vs. 20.4%, p = 0.0029). When examining alcohol-related outcomes among adult Ohioans whose most severe TBI was mild, the prevalence of current binge drinking was significantly higher among those who experienced their first self-reported TBI with LOC before age 20 than at or after age 20 (31.9% vs. 19.3%, p = 0.0004). This association was also observed when stratified by sex. The relationship between age at injury and heavy drinking was not significant for all TBI with LOC (p = 0.5382) or mild TBI (p = 0.5388).
Adult Alcohol Misuse and Age at First TBI with LOC by Injury Severity and Sex
LOC, loss of consciousness; TBI, traumatic brain injury; CI, confidence interval.
After adjusting for sex, age, and race, no significant differences in the odds of current binge drinking (adjusted odds ratio [AOR] = 1.04, 95% CI = 0.83, 1.30) or heavy drinking (AOR = 0.89, 95% CI = 0.65, 1.22) were observed among adult Ohioans whose first self-reported incidence of TBI with LOC occurred before the age of 20 as compared with those whose first TBI with LOC occurred at or after age 20 (Table 3). However, among adult Ohioans whose most severe TBI was mild, those whose first self-reported TBI with LOC occurred before the age of 20 had 32% greater odds of reporting binge drinking (AOR = 1.32, 95% CI = 1.00, 1.74) than Ohioans who experienced their first TBI with LOC at or after age 20. Such age effects were not observed for self-reported heavy drinking (AOR = 0.96, 95% CI = 0.65, 1.42).
Adjusted Odds Ratios (AOR) of Binge and Heavy Drinking by Injury Severity
AOR was based on logistic regression with age of first TBI, sex, age, and race mutually adjusted.
CI, confidence interval; TBI, traumatic brain injury; LOC, loss of consciousness.
Sex and current age were significantly associated with binge drinking and heavy drinking, with females and older age having significantly lower odds of binge drinking and heavy drinking, regardless of the severity of worst TBI. The relationship between current age and drinking raised the possibility of a confound resulting from reverse causation: younger people were more likely to misuse alcohol and were closer in time to childhood, which might improve recall of early life TBIs. We conducted a sensitivity analysis in which all participants <30 years old were eliminated from the modeling. The resulting odds ratios were essentially unchanged from those found for the entire cohort (Table S1)
When examining binge drinking by specific child and adolescent age groups at first self-reported incidence of TBI with LOC, we found that significantly higher proportions of binge drinking were associated with first TBI with LOC at ages 10–14 or 15–19 years (p = 0.0102) (Fig. 1a). This association held true among adults whose most severe TBI was mild (p = 0.0009) (Fig. 1b). Interestingly, when stratified by sex, females whose first TBI with LOC occurred at ages 10–14 years or 15–19 years were significantly more likely to report binge drinking than those whose first TBI with LOC occurred before the age of 10 (p = 0.0229). This relationship was also observed among females whose most severe TBI was mild (p = 0.0301). No significant effects of age group at first TBI with LOC on binge drinking were found for males, among all TBI (p = 0.3959) or among mild TBI (p = 0.0808).
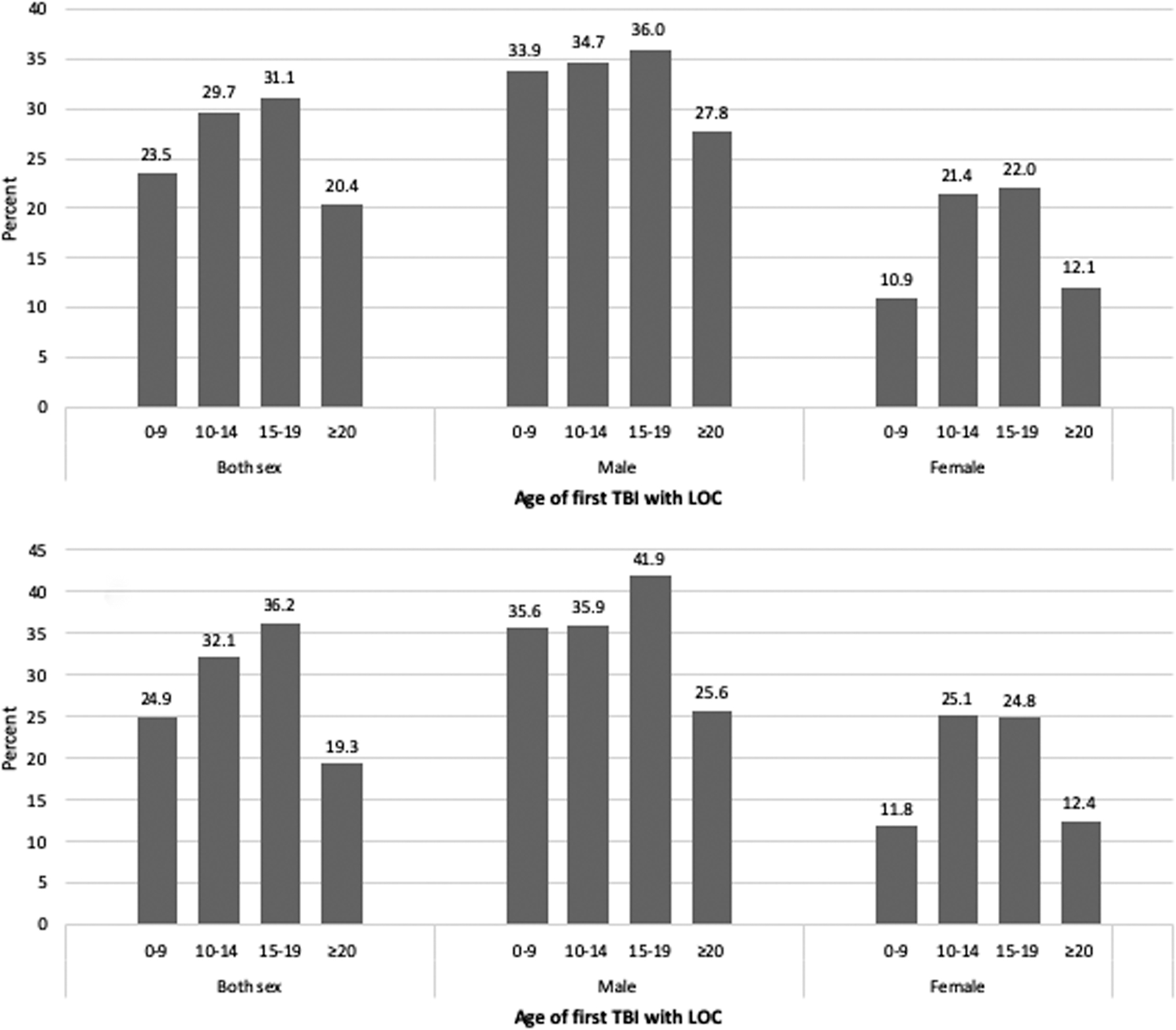
Proportion of binge drinking by childhood age at first traumatic brain injury (TBI) with loss of consciousness (LOC).
Discussion
In this population-based cohort study we observed a greater likelihood of binge drinking for those who incurred their first TBI with LOC before the age of 20 when compared with those who experienced their first TBI at or after 20 years. This relationship was apparent for both males and females. This relationship was not evident when controlling for sex, age, and race/ethnicity. This relationship was not observed for heavy drinking. However, when history of TBI was limited to a respondent's worst lifetime injury being mild (i.e., resulted in LOC ≤30 min), this observed relationship remained evident for binge drinking and was persistent even after controlling for sex, age, and race/ethnicity. The relationship for binge drinking was apparent for both males and females whose worst lifetime TBI was mild. Our results further revealed that participants whose first self-reported TBI with LOC occurred when they were between 10 and 19 years of age were more likely to report binge drinking as adults than those whose first TBI with LOC occurred earlier (when they were <10 years of age) or later (when they were ≥20 years of age) in life. This relationship was evident regardless of the severity of one's worst lifetime TBI. These findings appeared to be primarily because of results for female respondents, as males injured before age 10 were as likely to report binge drinking as males first injured at 10–19 years of age.
There is a question as to why early life injury would increase vulnerability to adult alcohol misuse. Injury to the developing nervous system not only damages existing structures and functions, but can also impact nervous system elements that manifest later in the neurodevelopmental trajectory. 28,29 TBIs to developing brains both directly damage tissue and disrupt a series of tightly coordinated neurodevelopmental processes that could be relevant to addictive behaviors, including myelination, synapse formation, and circuit maturation. 30,31 Precise neurobiological mechanisms that underlie these phenomena are currently being explored and are not fully understood. We have previously described a series of potential links between pediatric brain injuries and the subsequent development of alcohol-related pathology. 14,17,32 For example, pediatric TBI can persistently alter the reactivity of the central neuroinflammatory system. 33 This increase in inflammatory reactivity can initiate a vicious cycle because alcohol is proinflammatory, and neuroinflammation seems to promote alcohol intake. 34 –36 Further alterations in neurochemical homeostasis, particularly in the brain reward circuitry, have been demonstrated following TBI. 37 From a psychosocial perspective, the use of alcohol and other drugs among individuals with a history of TBI can be conceptualized as a self-medication phenomenon that may be used to attenuate negative emotional states and/or facilitate social interactions. 38 Whether these factors contribute to the incidence of drinking behavior or the transition from alcohol use to misuse is a critically important question.
There is a question as to why a relationship between early life injury and adult binge drinking would be more pronounced for mild than for more severe TBI. Several studies have reported a protective effect of more severe TBI on alcohol consumption. 7,39,40 For some individuals with more severe injuries, impaired community mobility may limit access to alcohol. Clinically, patients report more frequent, and more painful, headache as a consequence of drinking after TBI. Seizure disorders arising from the injury, including the use of seizure prophylaxis, are also commonly cited as the reason a person stops drinking. For others, the consequences of a more severe TBI may serve as a warning of the negative effects of excessive drinking. Without other key risk factors being controlled, reasons for the effect observed in the current study are speculative.
Although adult Ohioan males were more likely than females to report both binge and heavy drinking, we found that females first injured in adolescence were more likely to binge drink than females first injured either earlier or later in life, whereas no such association was found among males. No previous studies have observed this differential effect of age at injury in either sex. Previous findings regarding sex differences in alcohol-related behaviors may be informative; however, the results from human and rodent studies have been contradictory. Female rodents self-administer more alcohol than males under continuous and binge-like conditions and in operant procedures. 41 –43 Additionally, female rodents appear to find ethanol more rewarding, as indicated by greater conditioned place preference and dopamine efflux following ethanol administration. 44,45 In contrast, human men generally drink more than women. That said, although there are fewer women who meet the diagnostic criteria for alcohol use disorders than men, the rate appears to be increasing, and women are vulnerable to the medical consequences of heavy drinking, including liver disease, infertility, and mortality. 46,47 In the current study, we found more overall alcohol misuse among males. The increased vulnerability among females who only had a mild TBI and experienced their first TBI in adolescence may not have been evident in males simply because the greater baseline levels of alcohol misuse among males generally reduced the potential for an additional, TBI-induced increase. Quite clearly, the specific mechanisms for this sex difference remain unspecified.
Several limitations of the methodology employed in this study should be considered when interpreting these results. The study reports on data gathered via self-report, which is influenced by the respondents' ability to understand the questions, accurately recall pertinent information, and match what is recalled to the response options. The self-report measure used to detect TBI in the current study has been validated extensively; however, the extent to which answers are a veridical representation of lifetime exposure are unknown. Given the importance of age at first TBI with LOC, injuries before age 4 are less likely to be reported in adulthood, although TBIs with LOC occurring later in childhood are highly likely to be recalled. 48 Additionally, the questions used in this module to determine lifetime history of TBI slightly changed from the 2014 survey to the 2016 and 2017 surveys. The authors do not feel that this change was significant enough to impact the ability to combine data and produce valid estimates. As discussed, the findings cannot be interpreted as representing a causal effect. Although childhood injury precedes adult alcohol use, confounding variables could account for both a TBI and the adult use. We did not control for confounders beyond basic demographics (e.g., household income, parental influences). Further studies are needed to understand the role of potential confounders in the relationship between lifetime history of TBI and unhealthy adult behaviors. The current study also did not evaluate the relationship between TBI without LOC and adult alcohol misuse, as less severe injuries were excluded in 1 year of the data utilized in the current study. Therefore, for the purposes of this study, persons whose only lifetime exposure was a TBI without LOC were excluded.
The relationship between pediatric brain injury and the subsequent development of alcohol misuse disorders has been described epidemiologically, and modelled in pre-clinical settings. 33,49,50 The results of the current study add to epidemiological studies showing an association between childhood injury and adult drinking, at least for those with only mild TBI, and binge but not heavy drinking. Critically, the mechanisms that underlie the link between TBI and the development of alcohol misuse are not currently known and are likely to be complex and multifactorial in any case. We have previously described potential neurobiological substrates that could link TBI to substance abuse in animal models, and similar processes seem likely to exist in humans. 32,51 Although there are strong indications in the current report and other previous epidemiological and pre-clinical studies of the relationship described, much work at all levels of analysis are required to fully understand this critical phenomenon.
Footnotes
Author Contributions
Each of the authors shared in planning the research, in conducting and interpretation of analyses, and in reporting of the work described in the article. All authors have approved the final version submitted here and take responsibility for all aspects of the work.
Funding Information
Drs. Corrigan, Weil, and Bogner's effort on this project were funded in part by a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR # 90DPTB0001). NIDILRR is a Center within the Administration for Community Living (ACL), Department of Health & Human Services (HHS). Dr. Hagemeyer's effort on this project was funded in part by the Centers for Disease Control and Prevention (U17 CE924827). The contents of this report do not necessarily represent the official views or policy of NIDILRR, ACL, CDC, or HHS, and endorsement by the federal government should not be assumed.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.