
Abstract
Individuals classified clinically as having a motor-complete spinal cord injury (mcSCI) should lack voluntary motor function below their injury level. Neurophysiological assessments using electromyography (EMG) and transcranial magnetic stimulation (TMS), however, have demonstrated that persons with mcSCI retain limited cortical descending innervation and voluntary activation of muscles below their level of injury, including muscles of the trunk and lower limb. We explored the possibility of whether there is also preserved innervation of the pelvic floor muscles (PFM) in persons with mcSCI. The PFM are controlled by widespread cortical and subcortical areas and typically coactivated with trunk and gluteal muscles to maintain continence and regulate intra-abdominal pressure. Nine mcSCI and eight control subjects participated in this cross-sectional study. Surface EMG was used to record activity in the PFM. Data were recorded while participants attempted various maneuvers of the trunk and pelvis. We also applied TMS at incrementing levels of intensity over the primary motor cortex area to record motor evoked potentials (MEPs) in the PFM. When performing the maneuvers, activation of the PFM was possible in all controls and the majority of SCI participants. However, the PFM were only activated in the SCI participants during maneuvers that engaged other trunk muscles, however. MEP responses in the PFM were also elicited in all controls and SCI participants, but MEP response characteristics were significantly altered in the SCI group. Our results suggest that persons with mcSCI retain some residual innervation of the PFM after injury, possibly via indirect cortical descending pathways.
Introduction
Spinal cord injury (SCI) is a devastating neurological disorder that arises from damage to the spinal cord and may result in irreversible sensory and motor deficits. The accurate classification of an individual's level of injury and degree of sensorimotor impairment is critical for medical and rehabilitation management. In a clinical setting, SCI is classified using the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) examination. 1 The motor portion of this examination is used to classify the injury as motor-incomplete or motor-complete, which reflects whether the person has residual voluntary motor control below the injury level. 1 Neurophysiological examinations complement the ISNCSCI because they can provide a more detailed picture of spared motor activity post-injury. 2,3
While clinical examinations such as the ISNCSCI rely on manual palpation of a muscle to determine the degree of motor activity, neurophysiological examinations using electromyography (EMG) can capture even the smallest amount of contractile activity that may be unpalpable. 4 Indeed, studies using EMG have shown that persons classified with a motor-complete SCI (mcSCI) can voluntarily contract muscles below their level of injury; in a majority of cases, individuals showed some level of voluntary activation of their leg and/or trunk musculature, regardless of the duration of injury or the proximity of their injury level to the level of innervation for the targeted muscle. 5 –10
Transcranial magnetic stimulation (TMS) offers a non-invasive approach to explore in more detail the integrity of descending pathways from the primary motor cortex to muscles innervated below the injury level. 2,11 The presence of a motor-evoked potential (MEP) elicited by TMS over the primary motor cortex has been used to indicate at least partial preservation of the corticospinal tract in persons with SCI. Indeed, previous studies using TMS have reported preserved corticospinal innervation to the trunk and some lower limb muscles in individuals with high-thoracic or cervical mcSCI, even in persons who were >10 years post-injury. 6,7,12
Beyond the binary assessment of MEP presence/absence, other attributes of the MEP waveform are altered post-SCI, providing further insights into the nature of pathological changes after injury. 13 –17 For example, the latency of MEPs elicited in persons with SCI is typically prolonged. Axonal demyelination could explain this, but the finding that the delays in MEP latencies are not associated with time post-injury 18 suggests other explanations such as reduced number or degeneration of corticospinal axons. 2,16 –20
Recruitment curves, where MEP amplitude is plotted against incrementing levels of TMS, 21 are also affected post-SCI and indicate reduction in the gain of the input-output relationship of corticospinal networks compared with controls. 13 The input-output relationship can be fit with a sigmoid curve, and several curve parameters can be extracted, including the maximum slope of the rising portion of the sigmoid function, which is considered to represent cortical representation and corticospinal excitability. 21,22 To our knowledge, recruitment curves have only been characterized in persons with incomplete SCI, and only in muscles of the upper or lower limb. 13 –15,23
While studies using neurophysiological assessments have provided some evidence for the residual integrity of descending motor pathways to leg and trunk musculature in persons with mcSCI, 6,7,12 these types of examinations have yet to be conducted on the pelvic floor muscles (PFM) in this population. The pelvic floor plays a critical role in urinary function, and interventions to strengthen these muscles are the first line treatment for incontinence in able-bodied males and females. Despite more than 80% of persons with SCI experiencing lower urinary tract dysfunction, 24 –26 interventions targeting the PFM have not been explored, possibly because of uncertainty around the degree of voluntary motor control maintained over the PFM post-injury. Considering the evidence for voluntary activation in the trunk muscles in persons with mcSCI, 5 –10 this raises the question of whether the PFM can be similarly activated.
While the PFM can be contracted in isolation (forming the core element of PFM exercise programs in various able-bodied populations 27 ), PFM activation is largely involuntary because this muscle group serves an important functional role in maintaining continence 28,29 and regulating intra-abdominal pressure required for everyday tasks, including postural and respiratory tasks. 30 –33 Indeed, multiple EMG studies have demonstrated that the PFM are co-activated during various activities (e.g., coughing, postural adjustments) that also engage the trunk and gluteal muscles. 31 –35 Co-activation of the PFM with other postural muscles in these functional tasks is thought to be mediated via multiple cortical and subcortical regions. 30,35,36
Further, neurophysiological investigations in able-bodied controls have revealed the presence of corticospinal innervation to the PFM by recording MEPs in response to TMS over the medial wall of the precentral gyrus. 35 –41 Two studies have shown the possibility of eliciting MEPs in the PFM or anal sphincter in response to TMS in persons with multiple sclerosis 42 or motor-incomplete SCI, 41 but MEP responses were only observed in about half of the study participants.
In this study, we sought to evaluate the presence of residual innervation of the PFM in persons with mcSCI, with able-bodied control subjects providing reference data. In the first part of this study, we determined whether the PFM can be activated in isolation, and/or coactivated through maneuvers targeting the trunk and gluteal muscles. In addition, we wanted to explore the consistency with which the PFM are activated in response to the maneuvers, and whether injury characteristics may play a role in the ability to engage the PFM.
In the second part of this study, we sought to determine whether MEPs may be elicited in the PFM in response to TMS over the primary motor cortex. We also aimed to evaluate the characteristics of the MEP response utilizing a recruitment curve, and by exploring the relationship between MEP response and injury characteristics. We hypothesized that persons with mcSCI would be able to engage the PFM by the various maneuvers, regardless of level of injury and chronicity. We also hypothesized that MEPs in the PFM could be elicited, but the recruitment curves constructed from their MEP response would show signs of decreased corticospinal connectivity and excitability depending on injury characteristics.
Methods
Participants
Participants with SCI recruited for this study were between 19–60 years of age, at least 12-months post-injury, and had an injury classified as motor-complete (American Spinal Injury Association Impairment Scale [AIS] A or B) at or above the neurological level of L1. Healthy control participants of the same age range were recruited to provide reference data. Individuals were excluded from participation if they had been pregnant, given birth, or had urogenital/abdominal surgery within the past year; if they had received a diagnosis of PFM injury or impairment; or if they experienced neurological impairment other than SCI. Participants were also screened for TMS contraindications including recurring severe headaches; history of seizures/epilepsy either personally or in an immediate family member; consumption of medications that lower the seizure threshold; metal fixtures within the head; history of skull fracture or brain/head injury; presence of psychiatric disorders or sleep deprivation; or electrodes implanted within the nervous system.
All procedures in this study were approved by the University of British Columbia's Clinical Research Ethics Board, and all participants provided informed written consent.
Procedures
All measurements took place during a single session. Participants were asked to report their age, sex, height, weight, and females were asked about previous pregnancy and childbirth. Participants with SCI were also asked about their date and cause of injury, and a registered nurse conducted the ISNCSCI examination with each SCI participant to confirm the classification of their injury. 1
We used surface electrodes to record EMG signals from the PFM. Disposable surface electrodes connected to snap lead EMG sensors (Trigno Snap Lead sensor, Delsys Inc., Boston, MA) were placed perianally to record bilaterally from the PFM. To monitor EMG activity from other muscles of the trunk and pelvis during the maneuvers, we also affixed surface electrodes (Trigno Avanti sensors) bilaterally over the rectus abdominis (RA; 1 cm lateral and 3 cm superior of navel), external oblique (EO; 2 cm inferior of the lowest rib on the anterior side), erector spinae (ES; 2 cm lateral of the vertebral column at L4), and gluteus maximus (GM; 2 cm inferior and lateral to the line drawn between the posterior superior iliac spine and the third sacral spine). The EMG data were recorded at 2000 Hz and stored for offline analysis.
Attempted maneuvers
Participants attempted a series of maneuvers targeting the abdominal, paraspinal, gluteal, and PFM muscles to determine whether coactivation or isolated activation of the PFM was possible. To account for possible effects of intra-abdominal pressure on EMG activation, participants' breathing pattern was timed to each maneuver. 4,7 Before each maneuver, participants were given the following instructions: “breathe out (2 sec), breathe in (2 sec), breathe out (4 sec) while [performing the requested maneuver].” Correct breathing was verified using a thermocouple affixed below one of the nostrils to record changes in temperature related to inhalation and exhalation.
Participants were asked to attempt six maneuvers, of which five were tasks previously shown to induce coactivation of the PFM, 31,32,34,35 and one task was to perform an isolated activation of the PFM. Participants were instructed to attempt to hold each position for approximately 4 sec. (1) Trunk Flexion (TF) was attempted while participants lay supine with their knees flexed, feet flat, and arms crossed at the chest; (2) Side Bend/Lateral Flexion (right and left; RSB, LSB) was attempted while participants lay supine with legs extended and arms at their sides; (3) Trunk Extension (TE) was attempted while participants were prone with their arms by their sides; (4) Abdominal Hollowing (AH) was attempted while participants lay supine with their knees flexed and feet flat; participants were asked to compress their abdomen, drawing the naval toward the spine; (5) Hip Extension/Bridging (HE) was attempted while participants lay supine and asked to maximally contract their gluteal muscles; (6) Isolated PFM contraction/”Kegel” (isolPFM) was attempted while participants lay supine with their knees flexed and feet flat, and asked to contract their pelvic floor by imagining they were attempting to stop the flow of urine or prevent flatulence.
For each maneuver, research team members ensured correct positioning (e.g., bent knees with feet flat on the plinth) and stabilized the participants as necessary. For trunk flexion, side bending, and trunk extension, a member of the research team provided manual cues to the participant (e.g., “try to press up against my hands”) to prevent any movement; however, in no case was movement elicited. Each maneuver was repeated twice.
TMS
For the TMS trials, participants rested supine on a plinth with a small foam block underneath the head to allow for proper coil positioning. Stimuli were delivered using a MagStim 200 Stimulator (The MagStim Company Ltd, Dyfred, UK) with a double cone coil (Magstim Double Cone Coil, P/N: 9902-00). Surface anatomy was used to locate the optimal point of excitability (hot spot) of the primary motor cortex representation of the PFM. 35,36,38,41
The coil was positioned initially along the midsagittal line, drawn from the bridge of the nose to the occipital protuberance, at the intersection 2 cm anterior to the auricular plane, which was the anticipated hot spot location. To verify hot spot location, stimuli were delivered initially at 60% of the maximum stimulator output (MSO) while MEP presence was verified by real-time monitoring of the EMG signal. The coil was then moved in increments of approximately 0.5 cm along the sagittal plane to find the location that consistently delivered the largest MEP. If a response could not be determined at 60% MSO, the same protocol was repeated at incrementing levels of 5% MSO until a response was found and a hot spot determined.
To ensure that the coil position was maintained consistently on the identified hot spot between trials, rigid bodies with infrared-emitting diodes were secured on the coil and over two bony landmarks on the participant's skull (zygomatic arch and frontal bone). The positions of these rigid bodies were streamed in real-time from an Optotrak Certus position sensor (Northern Digital Inc, Waterloo, Canada) into a custom-made navigation program (Unity Technologies, San Francisco, CA) that tracked the linear and angular position of the rigid bodies relative to each other. Real-time visual feedback from this program was monitored by the research team, and the coil was adjusted as necessary between each trial to ensure the trial-to-trial consistency of coil position was within ∼2 mm.
To generate a recruitment curve of the MEP responses, a range of stimulation intensities were delivered to each participant in blocks. Stimuli of the same intensity were delivered in blocks of five pulses, with 10 sec between each stimulus, and up to 3 min between each block. Stimuli began submaximally at approximately 30% of the maximum stimulator output (% MSO) for all participants, and increased in intensity by 5–10% MSO each block. The test ended when 100% MSO was reached, the MEP amplitude reached a plateau (no significant increase in average MEP amplitude over three consecutive levels of % MSO), or if the participant requested to discontinue the experiment.
To control for background variability in cortical and motoneuron pool excitability, 43 participants were instructed to attempt to maintain a slight activation of the PFM while MEPs were recorded. Before stimulation, participants were asked to complete three maximal, isometric trunk flexion attempts using the same technique as described above (Attempted maneuvers). The amplitude of these responses was averaged, and 10% of maximum effort was determined. During each stimulus, participants were asked to maintain a submaximal contraction of their PFM by attempting trunk flexion at the threshold of 10% of maximum effort, and to maintain this engagement for approximately 2 sec during which the stimulation was delivered. Visual feedback of the smoothed rectified RA EMG signal was provided to assist participants in maintaining this contraction level, and all participants were given time to practice repeatedly achieving a 10% contraction until they felt confident in doing so.
To control for changes in intra-abdominal pressure, participant's breathing was timed to the TMS pulse. 7 Before each stimulus, participants were asked to “breathe in (2 sec), breathe out (2 sec) while gently contracting your abdominal muscles without moving your head.” The stimulation was delivered during the exhalation, and correct breathing pattern was verified using the thermocouple.
Data analysis
All data were analyzed using custom-written MATLAB routines (Mathworks Inc, Natick, MA).
Two variables were extracted from the attempted maneuvers trials: the average root mean square (RMS) and the maneuvers score. All EMG data were band-stop filtered at 60 Hz and then high-pass filtered at 30 Hz with an eighth-order dual-pass Butterworth filter and rectified. The mean RMS of the PFM EMG amplitude over a 2-sec window for each muscle during the attempted voluntary contraction (maneuver) for each participant in each trial was then calculated. To calculate average RMS, RMS amplitude of the right and left EMG signals were averaged together for each participant in each maneuver.
The maneuvers score for each participant was calculated using the PFM EMG signal. For this measure, activity in right and left PFM EMG recordings were analyzed separately. First, the RMS EMG amplitude over a 2-sec window for the PFM during the rest period preceding each voluntary contraction was calculated. The mean and standard deviation of the resting PFM data across all trials were used to create a threshold for each participant. If the mean RMS amplitude during a given attempted contraction phase exceeded two standard deviations above the global mean of this resting threshold, muscle activity was considered “present” for this maneuver. 4,6,7
The participant was given a score of 0 (no activity on either trial), 1 (activity present in only one of the trials), or 2 (activity present in both trials) for the right and left PFM for each maneuver. The maneuvers score for each participant was then calculated and reported as a percentage by summing the total score for right and left PFM and dividing by 28 (seven maneuvers, two trials each, bilaterally).
For the TMS data, peak-to-peak MEP amplitude from the PFM EMG signal was calculated from both the right and left sides from each trial at each stimulus intensity. To determine MEP presence, we first defined a threshold based on the background EMG signal, which was quantified by averaging the rectified EMG signal over a 100-msec window 50 msec before the TMS pulse. If the EMG data after the stimulation exceeded two standard deviations of the mean of the background EMG sample, and surpassed this threshold for at least 2 msec, then the MEP was considered present. The MEP latency was defined as the instance at which the EMG first crossed this threshold. 6,7
To construct recruitment curves, we first measured the peak-to-peak amplitude of the raw EMG activity after MEP latency.
6,7
Because the PFM MEPs sometimes had irregular waveforms, especially from the SCI participants (
Motor-evoked potentials (MEP) in the pelvic floor muscles (PFM) from spinal cord injury (SCI) participants with (
If the variance in MEP amplitude accounted for by % MSO (R 2 ) was greater than 0.80, 44 MEPslope, representing the steepness of the function, 44 was extracted from the equation. Absolute amplitude-related parameters from the sigmoid function, such as the maximum value (plateau), were not extracted because we could not normalize PFM EMG amplitude for an appropriate comparison across participants.
Statistical analysis
Statistical analyses were performed using SPSSv20 (IBM, Armonk, NY), and statistical significance was evaluated at an alpha of 0.05. Note that the data from the control group are presented to provide reference data, but no formal statistical analyses were performed to compare controls with the SCI group.
To evaluate which maneuvers successfully activated the PFM in the SCI participants, the average RMS during each maneuver was compared using separate one-way within-subjects repeated measures analysis of variance. Pairwise comparisons using a Bonferroni-corrected alpha were used to compare each maneuver against rest (total of seven pairwise comparisons; adjusted alpha of 0.007). The same analysis was conducted for the control group.
To explore how participant characteristics may relate to the ability to activate the PFM, the maneuvers scores of individual participants were reported descriptively along with their injury characteristics.
To assess the integrity of the cortical descending pathways to the PFM, MEP presence, MEP latency, and MEPslope of individual SCI and control participants were reported using descriptive statistics.
Formal subgroup analysis by chronicity or level of injury within the SCI group was not pursued because of the small sample size. In all figures and tables where possible, however, SCI participants were grouped by level (≥T5 vs. ≤T6, because abdominal muscles are innervated by the lower six thoracic segments) and organized by chronicity to allow for visual examination of any trends between these characteristics with the maneuvers and MEP responses.
Results
Participants
There were nine participants (three females) with mcSCI enrolled in this study (Table 1), with a mean age of 43 years (range 24–54 years). Of the three females, SCI08 was nulliparous, SCI05 was multiparous (three cesareans), and SCI06 was primiparous (one vaginal delivery). Injury levels ranged from C6–T10, and two participants were classified as having AIS B injuries. Eight able-bodied control participants also enrolled in this study including four males and four females (all nulliparous) with a mean age of 24 years (range 19–31 years). The EMG data from the left PFM in one control participant (C08) were excluded from all analyses, and left PFM data from one SCI participant (SCI06) were excluded from the maneuvers analysis because of technical problems.
Characteristics of Spinal Cord Injury Participants
M, male; F, female; Light touch, the results for the light touch sensory test of the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) examination, maximum score of 112 where higher score represents better light touch sensation; Pinprick, the results for the pin- prick sensory test of the ISNCSCI examination, maximum score of 112 where higher score represents better sharp/dull discrimination; Total motor score, the results for the motor assessment of the ISNCSCI examination, maximum score of 100 where a higher score represents better motor control; AIS, American Spinal Cord Injury Association Impairment Scale: A, motor and sensory complete; B, motor complete and sensory incomplete.
Maneuvers
Example EMG data from one control and one SCI participant during the attempts of the different maneuvers are plotted in Figure 1. Individual data of all the muscles from each participant in the SCI group are also available in Supplementary Figure 1.

Individual elecromyography recordings from (
All maneuvers elicited significant PFM activity in the control group, but only three maneuvers (RSB, LSB, TE) elicited significant PFM activity in the SCI group (Fig. 2). In the control group, there was a statistically significant difference in PFM EMG amplitude among the maneuvers (F(7,49) = 18.234, p < 0.0001, Fig. 2A), with pairwise comparisons confirming significantly larger PFM EMG amplitude during all maneuvers compared with rest (p < 0.0001). There was also a statistically significant difference in PFM EMG amplitude among the maneuvers in the SCI group (F(7,56) = 8.204, p < 0.001, Fig. 2B). Pairwise comparisons revealed significant increases in PFM EMG amplitude between rest and right side bending (p = 0.0069), left side bending (p = 0.003), and trunk extension (p = 0.006), while trunk flexion showed a trend toward significant activation of the PFM compared with rest (p = 0.008).

Average root mean square (RMS) electromyography amplitude of the pelvic floor muscles in (
The maneuvers generally elicited a consistent response in PFM activation across the control participants, but more a variable response in the SCI group. In the control group, maneuver scores ranged from 64–100% with an average of 90% (Fig. 3, right panel). Hip extension and the isolated PFM contraction were the most effective maneuvers for eliciting full score. In the SCI group, one participant did not demonstrate PFM activity with any of the maneuvers and thus received a score of 0% (however, left PFM data were missing). In the other SCI participants, maneuvers scores ranged from 4–61%, with an average score of 31%
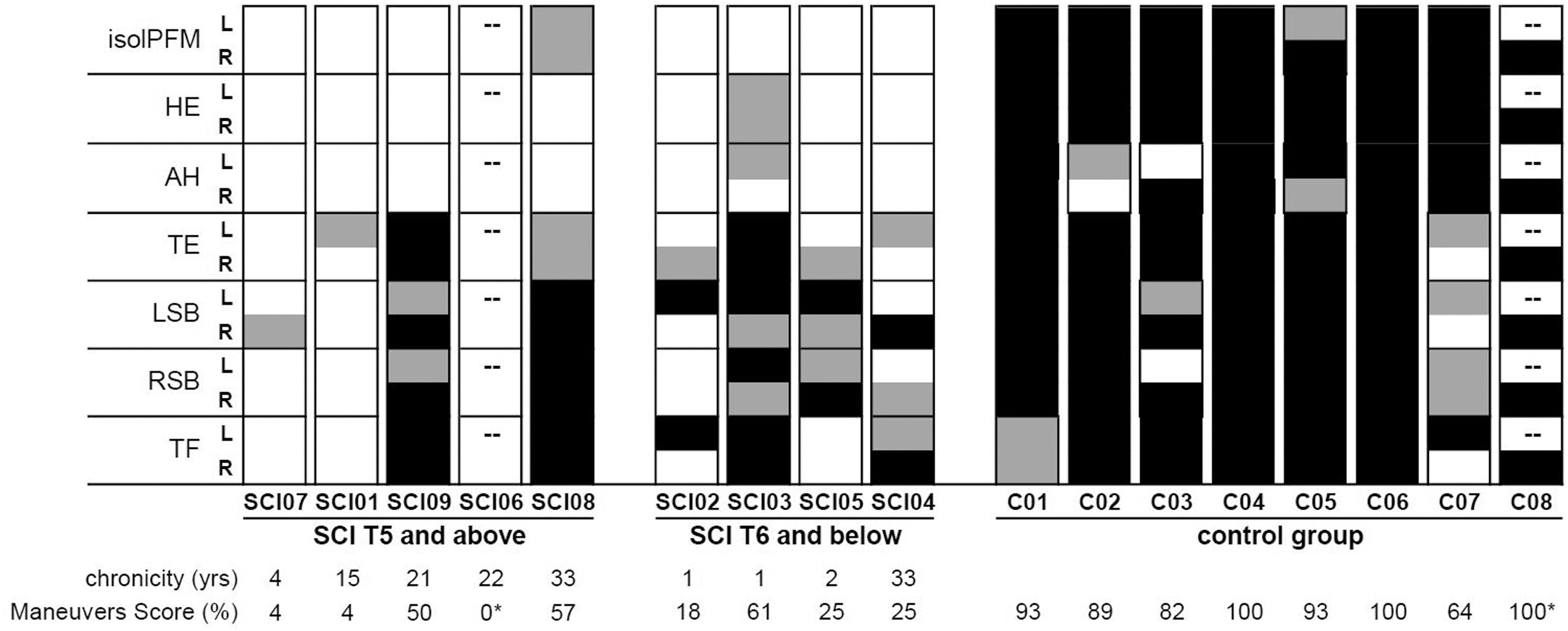
Frequencies of activation of the left (L) and right (R) pelvic floor during the attempted maneuvers in each spinal cord injury (SCI) and control participant. Each participant completed two trials per maneuver and was awarded a score of 2 if the right/left pelvic floor was active during both trials (black), 1 if the right/left pelvic floor was active during one of the trials (gray), or 0 if the right/left pelvic floor was not active in either trial (white). Cells with dashed lines represent data that were discarded from analysis. Chronicity (SCI only) and each participant's maneuvers score (their activation divided by total possible score) are indicated in the bottom rows (asterisks indicate that there were missing data from the maneuvers score). isolPFM, isolated pelvic floor muscle contraction; HE, hip extension; AH, abdominal hollowing; TE, trunk extension; LSB, left side bend; RSB, right side bend; TF, trunk flexion.
The trunk flexion, trunk extension, and the right and left side bending maneuvers were the most successful among the other maneuvers in eliciting some PFM activation. These responses were inconsistent, however. For example, despite trunk flexion eliciting one of the highest scores overall, four participants had no PFM activation with this maneuver. In contrast with the control group, hip extension and isolated PFM contraction were the least effective in eliciting PFM activation in the SCI group; only two participants with SCI showed PFM activation during either the isolated PFM (SCI08) or hip extension (SCI03) maneuvers, and the activation was inconsistent.
On visual inspection, participants with SCI at T6 and below generally seemed to have better success at coactivating their PFM with the different maneuvers compared with those with SCI at T5 and above (Fig. 3, cf. left and middle panels). There was no apparent pattern with chronicity.
TMS
The % MSO delivered in this study ranged from 30–100% among the controls and SCI participants. The total number of stimuli delivered to each participant, excluding the initial mapping, varied from 25 to 138. No adverse events were reported as a result of the TMS stimulation, but four SCI participants (SCI01–90% MSO; SCI03–80% MSO; SCI04–70% MSO; SCI05–65% MSO) and one control (C08–70% MSO) requested to stop the TMS recruitment curve early.
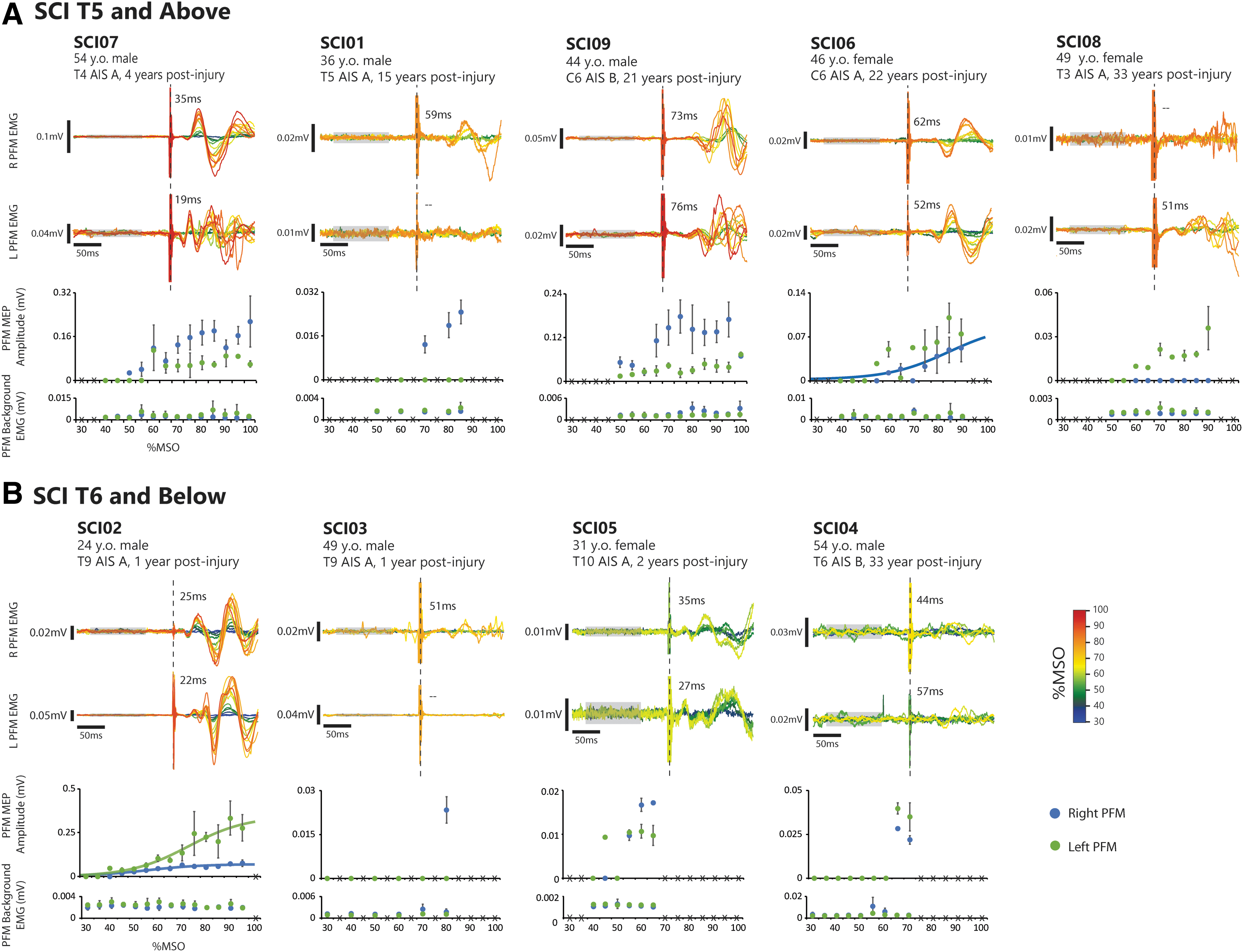
The TMS elicited bilateral PFM MEPs in all control participants (Fig. 4). In the SCI group, PFM MEPs were also present in all participants, but could be elicited only unilaterally in three individuals (SC101, SCI03, SCI08) (Fig. 5). Also, it should be noted that the EMG amplitude of the MEP responses of some SCI participants (SCI01, SCI03, SCI04, SCI05, SCI08) may be considered negligible (∼<0.05 mV), 17,23 even if they exceeded the threshold for MEP presence based on their background EMG. The average latency of the PFM MEP response in the control group was 22.1 msec (SD = 3.7 msec; range = 17.7-30.2 msec). Visually, we also noted late-latency responses appearing in some control participants (notably C02, C03, C05, C06; Fig. 4). In the SCI group, response latencies were prolonged compared to controls (average latency = 45.8ms; SD = 19.6 msec; range = 18.9-76.7 msec).
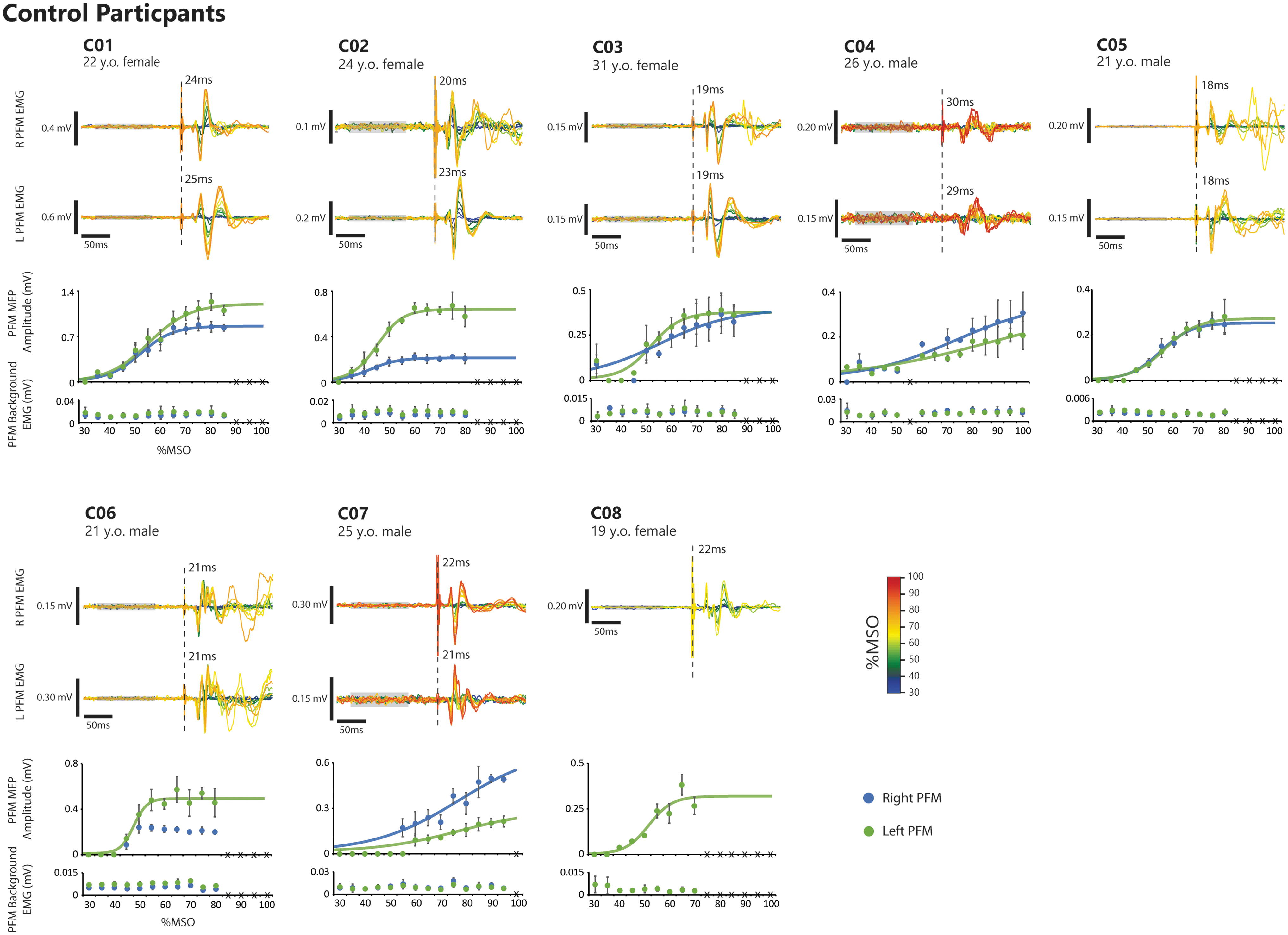
Motor-evoked potentials (MEP) in the pelvic floor muscles (PFM) from each control participant.
There appeared to be a pattern between MEP latency and chronicity when visually inspecting the data. Except for SCI03, participants who had MEP latencies more than double control values were all more than 15 years post-injury (Fig. 6).

Average pelvic floor muscle motor evoked potentials (MEP) latency in relation to chronicity. Visual inspection reveals an apparent pattern between MEP latency and chronicity where MEP latencies of participants who were injured more recently (<4 years post-injury; open symbols) tended to be closer to the control group average (vertical solid line). No pattern was noted between MEP latency and level of injury (circle vs. square symbols). Each symbol represents the average PFM MEP latency of each participant. Error bars represent the standard deviation calculated across all transcranial magnetic stimulation trials in each participant. The solid and dashed lines represent the control average and one standard deviation, respectively.
Sigmoid functions fit well to the recruitment curves of MEP amplitude versus % MSO of each control participant (average R2 = 0.92, range = 0.79–0.98), except the right PFM in C06. The average MEPslope was 10.2 (range = 2.7–26.4). In contrast, sigmoid functions fit well only to the right and left PFM MEP recruitment curves of SCI02 (right R2 = 0.85; left R2 = 0.88) and right PFM of SCI06 (R
2
= 0.92)
Discussion
In this study, we examined the presence of residual innervation to the PFM in individuals with mcSCI. Despite their clinical injury classification, we found evidence in most of our SCI participants of PFM activation during one or more of the attempted maneuvers. Although we could also detect the presence of MEPs in the PFM in each of the SCI participants, indicating some degree of connectivity between the motor cortex and PFM, several features of the response to TMS were disordered.
Activation of PFM is possible after mcSCI, but only through coactivation
We found that the SCI group members were unable to activate their PFM in isolation, and instead could only engage this muscle group through coactivation, particularly with the superficial abdominal and paraspinal muscles. 31 –35 In contrast, we were generally unable to elicit the expected PFM coactivation with abdominal hollowing 31,34 or hip extension. 33,35 Because we did not record from the transverse abdominis muscle, we cannot confirm that participants were able to perform abdominal hollowing, but we can note that none of the participants showed gluteal muscle activation during the hip extension maneuver (see Supplementary Fig. S1).
Conversely, if activation of the rectus abdominis, erector spinae, and/or external oblique was elicited during trunk flexion, extension, or side bending, this was typically accompanied by PFM activation. This was observed even in two participants with high-thoracic or cervical mcSCI, indicating preservation of portions of descending pathways from motor cortical areas mediating activation of the superficial trunk muscles, as shown in previous studies. 5,7,8,10 Any co-activation that we observed in the PFM with the abdominal musculature is unlikely attributed to changes in intra-abdominal pressure and possible contribution from short-latency spinal stretch reflexes because we asked participants to maintain an open glottis and exhaling while performing the maneuvers. 4,45
The coactivation responses in the SCI group were also notably inconsistent across the participants. The maneuvers were selected based on previous research that demonstrated these movements should elicit PFM activity. 31 –35 As such, we expectedly saw PFM activation during these maneuvers in the majority of control participants. Each SCI participant, however, had a unique pattern of PFM activation with the attempted maneuvers that did not correspond to their level of injury nor chronicity. Indeed, even within participants, activation of the right and left sides of the pelvic floor was inconsistent between maneuvers. It is unclear what mechanism underlies this variation, or if practice performing the different maneuvers may strengthen the response. Future work exploring how to best elicit PFM activity in this population may need to incorporate a considerable number of exercises so as not to overlook the potential for coactivation.
None of the SCI participants was able to demonstrate consistent voluntary activation of the PFM in isolation. We also cannot discount the possibility that the inability of the SCI participants to perform an isolated PFM contraction may be because performing this maneuver is challenging, even for some able-bodied individuals. Previous work has shown that slightly less than half of able-bodied females are able to perform an isolated PFM contraction effectively after brief verbal or written instruction, and as many as 25% of respondents display a technique that would potentially promote incontinence, such as a Valsalva maneuver. 46,47 Providing only a brief instruction, such as what we did here, may be inadequate to encourage isolated PFM contractions.
This difficulty is likely further compounded for persons with mcSCI who are unable to use sensory feedback to confirm if their attempt is correctly targeting their PFM. In comparison, abdominal maneuvers such as trunk flexion, extension, and side bending are simpler to understand, easier to perform, and are more likely to have been performed by the participants previously.
Integrity of cortical descending pathways to the PFM in persons with mcSCI
We were able to elicit MEPs in the PFM in all control and SCI participants in response to the TMS. In the SCI group, the presence of MEPs suggests some degree of preserved descending connectivity from the motor cortex to the PFM. Further, our success in eliciting MEPs in the SCI group is in line with earlier studies that reported 90–100% success rates of observable MEPs in the abdominal muscles 6,7 and 65% success rate of MEPs elicited in at least one lower limb muscle 6 in persons with mcSCI.
Although we could detect MEPs in all of the SCI participants, the features of their MEP response were very different from what we observed in the controls. First, the PFM MEP latencies recorded in our control group were within the range of that reported in previous studies. 35,40,48,49 Interestingly, the latencies of MEPs recorded in the external anal sphincter in a group of males with motor-incomplete SCI were also within the range of normative values, although responses could only be elicited in half of the group. 41 In contrast, PFM MEP latencies in our mcSCI participants ranged from being within to more than double that of control values.
Many studies have reported prolonged latency of MEP responses in various upper and lower limb muscles, mainly in participants with incomplete SCI, 16 –18,20 but we noted only one study showing data indicating latencies approaching more than double of control values. 17 It is interesting that in our sample, the SCI participants who had MEP latencies within the range of control values were among the less chronic (Fig. 6). This was not expected because previous work has demonstrated an increase in latency immediately after SCI that persists years into recovery, and that latency does not relate to chronicity, 18 nor was it found to be affected after participation in a rehabilitation intervention. 23 There could be a number of possible explanations for alterations in MEP latency post-injury (e.g., demyelination, reduced axon count), 2,16 –20 and so the lack of relationship between MEP latency and clinical characteristics of SCI should not be surprising.
It is possible that delayed PFM MEP responses we observed could have arisen from sensory feedback, 50,51 such as an increase in intra-abdominal pressure, secondary to activation of the diaphragm or abdominal muscles. Intra-abdominal pressure changes secondary to a diaphragmatic response to motor cortex stimulation, however, are on the order of 80-100 msec, 52 which is beyond the latency range we observed in our participants. In addition, we controlled the timing of TMS delivery to normal exhalation, with an open glottis, which should decrease intra-abdominal pressure. 53
While we were able to generate characteristic recruitment curves for almost all of the control data, we were unable to do so for most of the SCI data. Previous work in individuals with motor-incomplete SCI has demonstrated that the rise of the recruitment curve recorded from thenar muscles is reduced and that the reliability of recruitment curve metrics is poor, especially in more severely affected muscles. 13,14 These changes may represent interruptions in the descending pathways as well as alterations in corticospinal networks.
Our results are in line with these previous findings in that the responses we elicited were variable, and we were only able to fit a Boltzmann sigmoid function to the data of two participants (although we were unable to attempt a full recruitment curve from four SCI participants because of their request to halt the procedure early). Nevertheless, despite the disordered features of the MEP response, the presence of MEPs indicates at least some degree of integrity of the descending cortical pathways accessing the PFM in the SCI participants.
Possible origin of residual PFM innervation in mcSCI
It is unclear whether the delayed onset time of the MEP responses in the SCI group represents the slowing of direct corticospinal transmission to muscles below the level of SCI, as described previously, 16 –18,20 or a preservation of a longer latency component of the PFM MEP response. In able-bodied individuals, the early-latency components of MEPs in the PFM or external anal sphincter have been reported to range from ∼18–36 msec 35,40,48,49 and are generally thought to reflect transmission along direct corticospinal pathways, 37,48 although others have argued for the contribution of polysynaptic spinal relays to this descending pathway. 49
Latencies of the fastest portion of the MEP responses in our control group were in line with previous reports, 35,40,48,49 but we also observed what might be late MEP responses in some control participants. Dimitrijevic and associates 54 (1992) reported late MEP responses that appeared variably across trials and different leg muscles with latencies approximately double that of the typical early-latency response attributed to direct corticospinal pathways. They hypothesized that these later MEP responses could arise from indirect corticospinal or cortico-bulbospinal pathways. 54 Longer-latency MEP responses observed in the external anal sphincter have also been hypothesized to arise from the interaction of cortical circuits to brainstem or spinal polysynaptic pathways. 49
In our study, MEP responses were elicited while participants maintained a low-level activation of the PFM by performing trunk flexion, which was the only way we could facilitate responses in the SCI group. In performing this coactivation maneuver, we may have engaged pathways overlapping with those involved in the coordination of anticipatory postural adjustments and the control of intra-abdominal pressure. 30 –34
Functional neuroimaging data in humans have revealed various candidate areas for such synergistic control of the PFM, which include the primary motor cortex and pre-motor areas including supplementary motor area. 35,36,55 Anatomical tracing studies have also provided evidence for PFM motor neurons receiving direct projections from areas in the medulla (nucleus retroambiguus) 56 and motor cortex (area 4). 57 Thus, it is possible that our findings that the PFM could only be recruited by coactivation with a trunk muscle, coupled with the dominance of long-latency MEP responses, represents a preservation of descending connectivity to the PFM favoring indirect corticospinal or corticobulbospinal pathways in our participants with mcSCI.
Methodological considerations
A limitation of this study was the small sample size. With only nine participants with SCI, we were unable to conduct formal, statistical subgroup analyses to determine how injury characteristics such as chronicity and level of injury may impact our findings. Future work should include larger samples to generalize our findings to the broader SCI population and draw conclusions from subgroup analyses.
Differences in age present another possible limitation of this study, because the SCI group, with an average age of 43 years, was older than the control group (average age of 24 years). The prevalence of pelvic floor disorders increases with age, although this may be because of other characteristics (e.g., parity, obesity, other health problems) that are more common with age. 58,59 There is also evidence that the pelvic floor tends to thin with age, but this finding was only noted in individuals 65 years and older, 60 and our oldest participant was 54 years old.
The discrepancy in male:female ratio and parity between our control and SCI groups may have had a more confounding effect on our results. Our SCI group had more males than females (6:3), whereas the control group was balanced between the sexes (4:4). In addition, two of the three females in the SCI group had carried at least one pregnancy to term, yet all the females in the control group were nulliparous. The prevalence of pelvic floor disorders is higher in females, especially in those that have carried pregnancies past 20 gestational weeks. 58,59 Therefore, although there were fewer females in the SCI group, which should, on the whole, reduce the prevalence of PFM disorders in this group, the majority had delivered children, which in turn increases the likelihood of PFM disorders. As such, while we should acknowledge the potential impact of differences in the male:female ratio between the groups, it is difficult to distinguish that from the impact of differences in parity among the females in the two groups.
Recording EMG from the PFM is challenging based on the sensitive location of this muscle group, where participants may experience personal discomfort in exposing their perineum to affix surface EMG sensors. Previous studies of PFM activity have typically used vaginal or anal recording probes. 30 –32,35
We chose to use surface EMG electrodes to minimize participant discomfort and facilitate participant recruitment. Although the PFM are circular, the use of perianal surface EMG allowed us to record independent signals from the right and left aspects of this muscle as it encircles the anal canal, instead of as a singular unit like vaginal/anal probes. Considering that the PFM is unilaterally innervated, the separated right and left sided recordings also allowed us to detect asymmetries in PFM recruitment, as was often observed in the SCI group.
Previous work has shown that the PFM EMG signal is prone to crosstalk from muscles around the hip. 61,62 Among our SCI participants, we did not observe any gluteal activity, but we cannot rule out contamination of the PFM signal from gluteal EMG crosstalk during the hip extension and trunk extension maneuvers in the controls. We did not record EMG from the hip adductors and external rotators, so we also cannot verify whether activation of these muscles might have induced crosstalk to the PFM signal. 61
Clinical implications
Our results reveal the possibility of eliciting coactivation of the PFM along with other muscles of the trunk in some persons with mcSCI. This opens up the question of whether PFM training, a mainstay of treatment for urinary incontinence in other populations, 27,63 –67 could be a viable rehabilitation intervention for managing lower urinary tract symptoms in persons with mcSCI.
The most consistent means to activate the PFM in the SCI group appeared to be trunk flexion, extension, or side bending. As such, development of exercise-based programs for the mcSCI population may have to rely on coactivation strategies as opposed to direct maneuvers such as the isolated PFM contractions. This strategy, however, will have to be undertaken with caution because focusing on abdominal muscle exercises in the absence of ensuring PFM coactivation may result in further exacerbation of lower urinary tract symptoms. 31,68,69 Further research should be undertaken to discover whether more intensive clinical instruction, 65,70,71 or other combinatorial approaches (such as with biofeedback or electrical stimulation 72 ) would help facilitate the ability of persons with mcSCI to perform PFM exercises more effectively.
Conclusion
In this study, we demonstrate that persons classified as having a mcSCI may be able to coactivate their PFM when they attempt various abdominal maneuvers. Further, the presence of MEPs in the PFM in response to TMS indicates possible preservation of descending pathways supplying the PFM in these participants. These results support the growing body of literature that persons with a diagnosis of mcSCI may retain some residual motor function below the injury level, especially in the muscles of the trunk.
Footnotes
Acknowledgments
We would like to thank all of the participants for their time and efforts in this study and to Dr. Lynn Stothers for her valuable feedback. We would also like to thank the anonymous reviewers for their constructive and valuable comments on this manuscript.
Preliminary results from this study were presented at the International Continence Society 2019 Annual Meeting and published in abstract form in the journal Neurourology and Urodynamics.
Funding Information
This work was supported by the Blusson Integrated Cures Partnership. AMMW was supported by a Canadian Institutes of Health Research CGS-Masters award.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.