
Abstract
Pediatric traumatic brain injury (TBI) can lead to adverse emotional, social, and behavioral consequences. However, outcome is difficult to predict due to significant individual variability, likely reflecting a complex interaction between injury- and child-related variables. Among these variables are genetically determined individual differences, which can modulate TBI outcome through their influence on neuroplasticity mechanisms. In this study, we examined the effect of Val66Met, a common polymorphism of the brain-derived neurotrophic factor gene known to be involved in neuroplasticity mechanisms, on behavioral symptoms of mild TBI (mTBI) sustained in early childhood. This work is part of a prospective, longitudinal cohort study of early TBI. The current sample consisted of 145 children between ages 18 and 60 months assigned to one of three participant groups: mild TBI, orthopedic injury, or typically developing children. Participants provided a saliva sample to detect the presence of the Val66Met polymorphism, and the Child Behavior Checklist was used to document the presence of behavioral symptoms at 6- and 18-months post-injury. Contrary to our initial hypothesis, at 6 months post-injury, non-carriers of the Val66Met polymorphism in the mTBI group presented significantly more internalizing symptoms (e.g., anxiety/depression and somatic complaints) than Val66Met carriers, who were similar to orthopedically injured and typically developing children. However, at 18 months post-injury, all children with mTBI presented more internalizing symptoms, independent of genotype. The results of the study provide evidence for a protective effect of the Val66Met polymorphism on internalizing behavior symptoms 6 months after early childhood mTBI.
Introduction
Pediatric traumatic brain injury (TBI) can lead to impaired functioning in a range of neurocognitive and psychosocial domains, 1,2 and typically follows a dose–response relationship with regard to injury severity and the extent or chronicity of consequences. 3 In the case of milder forms of TBI (concussion or mild TBI [mTBI]), adverse consequences are transient and resolve within a few weeks for most children. 4,5 However, there is evidence that some children are more vulnerable to the effects of mTBI and display significant and persistent problems after injury, especially in social and behavioral domains. 6,7
Differential recovery outcomes and trajectories are likely the result of a complex interplay between injury characteristics, child factors such as age at injury and pre-injury functioning, 8,9 and environmental factors such as socio-economic status and parenting practices. 10,11 In addition, some authors suggest that genetically determined individual differences may modulate TBI outcome through their influence on neuroplasticity mechanisms. 12 -14 Neuroplasticity consists of the ability of the brain to change and adapt as a result of experience (i.e., experience-dependent plasticity), or to reorganize following an acquired brain injury (i.e., lesion-induced plasticity). These changes and reorganization processes occur at molecular, synaptic, and cellular levels, as well as through more global network changes. 15
The brain-derived neurotrophic factor (BDNF), encoded by the BDNF gene, is of particular interest when studying neuroplasticity mechanisms and has received considerable attention with respect to lesion-induced plasticity and acquired brain injury outcome. BDNF is the most abundant neurotrophin present throughout the brain and plays a key role in neuronal survival, synaptic plasticity and neurogenesis. 16 –19 Animal models of experimental brain injury reveal acute up-regulation of neurotrophic factors, such as BDNF, in the central nervous system. 20 In keeping with this, in a study of children age 3 months to 16 years with severe TBI, BDNF levels in cerebrospinal fluid and plasma showed a sharp peak acutely after injury. 21 This increase is thought to reflect an endogenous attempt of neuroprotection against biochemical and molecular changes induced by the brain insult, while contributing to synaptic reorganization processes, thus protecting against neurological damage and cognitive deficits. 21 -23
The BDNF gene has several polymorphisms, of which the Val66Met (also known as rs6265) variant is the most studied. BDNF Val66Met is common in humans, with an allele frequency of 20 to 30% in Caucasian populations. 21 -23 Its prevalence makes it possible to study its impact without requiring very large samples and this partly explains why it has been extensively studied in healthy controls, as well as in clinical populations. BDNF Val66Met is the result of a valine (Val) to methionine (Met) substitution at codon 66 of the gene. This substitution leads to alterations in intracellular trafficking of BDNF, which decrease protein regulated secretion by about 25%. 24,25 Taking these mechanisms into account, it is assumed that the Val66Met polymorphism (in other words, the presence of the Met allele) is associated with reduced potential for neuroplasticity, and thus a diminished capacity for functional recovery after neurological insult. 26
Genetic association studies exploring the role of the BDNF Val66Met polymorphism in TBI functional recovery are rare and only target adults. Moreover, results of the few existing adult studies are conflicting and difficult to reconcile, in part because of methodological differences (e.g., injury severity level and type of outcome evaluated). For example, some studies report that after severe forms of TBI (i.e., focal penetrating head injuries), the Met allele (i.e., Val66Met polymorphism), but not the hypothesized Val allele, promotes recovery of executive functioning 27 and general intelligence. 28 Conversely, the Met allele seems to be a risk factor for socio-emotional problems after milder forms of TBI. A recent study showed a strong association between the presence of the Val66Met polymorphism and depressive symptoms in the first week after mTBI in adults. 29 Similarly, another study found that in adults with a history of multiple concussions (defined as a head injury that resulted in post-concussive symptoms), increased brooding rumination and elevated symptoms of depression are reported among Met-allele carriers. 30
Despite these emerging findings on the role of BDNF Val66Met in recovery after TBI, the results of studies conducted in adults have limited applicability to the pediatric population because of the distinctive neurobiology of the immature brain. Further, natural concentrations of BDNF throughout the brain vary across development, such that the reduced protein expression conferred by the Met allele may constitute a protective factor in some developmental periods (e.g., during adolescence when BDNF levels peak) while representing a risk factor during others. 31 Thus, to better understand the role of the BDNF Val66Met polymorphism on TBI outcome, studies targeting well-defined developmental periods are needed.
In sum, genetic predispositions are thought to play an important role in functional recovery after TBI. However, there is a paucity of genetic association studies specific to TBI in children. 32 In particular, there are no candidate gene studies that investigate the role of BDNF gene polymorphisms on the functional outcome of pediatric TBI, even though BDNF is believed to play an important role in neuroplasticity after a brain insult. The current study aimed to explore the association between the presence of the Val66Met, a common polymorphism of the BDNF gene, and behavioral symptoms after mTBI sustained in early childhood (i.e., between 18 and 60 months), a period during which TBI is highly prevalent 33 and during which the brain undergoes major and rapid changes through brain plasticity mechanisms. In accordance with the results found in adults, it was hypothesized that Met-allele carriers would display more behavioral problems than Val/Val homozygotes.
Methods
The data presented here constitute a sub-study of a larger prospective longitudinal cohort study investigating cognitive, behavioral and social outcomes of preschool TBI 9,34 –38 and approved by the local institutional ethics review board. The current analyses focus on BDNF Val66Met polymorphism and behavioral symptoms after early mTBI.
Participants and recruitment
The current sample constitutes a sub-group of participants from the larger aforementioned cohort study, who agreed to participate in an additional and optional genetic sub-study. This sub-group consisted of a total of 145 children assigned to one of three participant groups: mild TBI (mTBI; n = 47), orthopedic injury (OI; n = 42), and typically developing children (TDC; n = 56; see descriptive variables in Table 1). Children from the two injury groups were between ages 18 and 60 months at the time of the injury and were recruited in a single, tertiary care pediatric emergency department. The mTBI group comprises children who sustained a closed-head injury with a score between 13 and 15 at admission on the Glasgow Coma Scale (GCS). Children who had a diagnosis of complicated mTBI (score between 13 and 15 on the GCS with evidence of an intracranial lesion on clinical computed tomography or magnetic resonance imaging) were also included (n = 8). The OI group comprises children who sustained a limb trauma, leading to a final diagnosis of simple fracture, sprain, contusion or unspecified trauma to an extremity. To compose the TDC group, non-injured children of equivalent age were recruited via information pamphlets left for parents in urban daycare centers. To ensure that the three groups were of comparable age at the first assessment time-point (i.e., 6 months post-injury for the two clinical groups), children in the TDC group were between ages 24-66 months at the time of recruitment.
Participants' Sociodemographic and Descriptive Characteristics
Parental education was obtained by averaging both parents' educational qualifications on an 8-level scale ranging from “Doctoral degree” to ‘Less than 7 years of school, unless the information was only available for one parent.
mTBI, mild traumatic brain injury; TDC, typically developing children; M, mean; SD, standard deviation.
Exclusion criteria for the three groups were: 1) diagnosed congenital, neurological, developmental, psychiatric, or metabolic condition; 2) gestational age <36 weeks; 3) child and parent not fluent in French or English; 4) history of prior TBI serious enough to warrant a visit to the ED; and 5) suspicion of a non-accidental injury (for the mTBI and OI groups). More detailed information on the recruitment procedure and inclusion criteria were provided previously. 9
Measures and materials
Descriptive variables
For the mTBI and the OI groups, a research nurse completed a standardized case report form immediately after recruitment for descriptive purposes (e.g., nature and severity of the injury, neurological signs and symptoms, GCS) and to confirm inclusion/exclusion criteria. Parents of all three groups completed an in-house socio-demographic questionnaire to collect information regarding demographics (e.g., sex, ethnicity, parental education, family living arrangement).
Behavioral outcome
At 6-months (T1) and 18-months post-recruitment (T2), mothers were asked to complete the age-appropriate version (i.e., preschool version for ages 1.5-5.0 years or school-age version for age 6-18 years) of the Child Behavior Checklist (CBCL). 39 For each version, items are rated using a 3-point scale (0 = not true; 1 = somewhat or sometimes true; 2 = very true or often true). There are 100 items in the preschool CBCL version and 113 items in the school-age version. Items are combined in empirically based syndrome subscales and these subscales are combined in two higher order factors: Internalizing Problems including four subscales (emotionally reactive, anxious/depressed, somatic complaints, and withdrawn), and Externalizing Problems including two subscales (attention problems and aggressive behavior). T scores were used in all analyses.
Saliva collection and analysis
Participants were invited to provide a saliva sample (0.75 mL) during the course of the study, either in person or via mail. The sample was collected using Oragene OG-575 kits (DNA Genotek, Ottawa, Canada) by collecting saliva with a sponge moved along the child's gums and inner cheeks, and then squeezed into a collection tube when saturated with saliva. To detect the presence of the polymorphism Val66Met, the amplification was performed using a thermal cycler (Biometra Tprofessional) using a polymerase chain reaction (PCR) approach, with the following oligonucleotide primer pairs: 5′-biotin before GGACTCTGGAGAGCGTGAAT-3 and 5′-reverse CCGAACTTTCTGGTCCTCATC-3′. In addition to buffers, nucleotide components and a dose of 0.01 U of Taq polymerase supplier of PCR Master Mix (Qiagen), the amplification reactions contained 1 μg of DNA derived from saliva, 1 μM each primer, 0.4 mM of dNTP, 1.0 mM MgCl2, in a final volume of 50 μL. The PCR conditions included 35 cycles: 30 sec at 95°C; 30 sec at 61.2°C; and 1 min at 72°C. These 35 cycles of amplification were preceded by an initial heating step of 3 min at 95°C and followed by a final extension of 4 min at 72°C. The PCR products were visualized on a 1.2% agarose gel. The Val66Met polymorphism was sequenced wiyh a pyrosequencing protocol 40 with a slight modification using the oligomer: 5′- GCTGACACTTTCGAACA -3′. The sequence analyzed was: CA / GTGATAGAAGAG.
Statistical analysis
All analyses were conducted using IBM SPSS Statistic (version 21.0). First, preliminary analyses were performed to ensure that groups were equivalent in terms of socio-demographic factors. Chi-squared analyses were conducted on categorical variables (i.e., sex, ethnicity, family living arrangement), and analyses of variance (ANOVAs) or Student's t-tests were conducted for continuous variables (i.e., age at assessment, age at injury, parental education). Where significant group differences were found for any of these socio-demographic variables (or even a statistical trend), the main analyses detailed below were conducted including the potentially confounding variable as a covariate.
In the main analyses, three-way mixed analyses of variance were performed for both the Internalizing Problems score and the Externalizing Problems score on the CBCL, with Group (mTBI, OI, TDC) and Genotype (Val/Val homozygotes, Met-Allele carriers) as between-subject factors and Time (T1, T2) as a within-subject factor. In the case of a significant interaction, planned follow-up analyses (ANOVAs or Student's t-tests) were conducted to determine simple main effects. An alpha level of p ≤ 0.05 was considered significant. Effect sizes were calculated using Cohen's d (small effect d = 0.2, medium effect d = 0.5, large effect d = 0.8; Cohen, 2013). 41
Results
Follow-up details and participant characteristics
Information on recruitment and follow-up details for all three groups are presented in Figures 1 and 2. There were no differences between families who agreed to participate in the overall study and those who refused participation, in terms of child age [mTBI: t(217) = 0.81, p = 0.42; OI : t(216) = -0.39, p = 0.70; TDC : t(111) = 0.61, p = 0.55] and sex [mTBI: χ2 (1) = 0.59, p = 0.44; OI : χ2 (1) = 0.43, p = 0.51; TDC : χ2 (1) = 2.28, p = 0.13]. Concerning attrition, 19 mTBI (16%), 27 OI (27%), and 1 TDC (1%) initially agreed to participate in the study but dropped out before the first assessment time-point (T1). More families from the injury groups than the TDC group dropped out before T1 because 6 months elapsed between recruitment and T1 for the clinical groups, whereas for the uninjured TDC group, T1 was completed immediately after recruitment. Twenty-four mTBI (27%), 11 OI (18%), and 17 TDC (20%) were excluded from analyses because they had missing CBCL data for either T1 or T2 (e.g., parents never returned the questionnaire booklet).
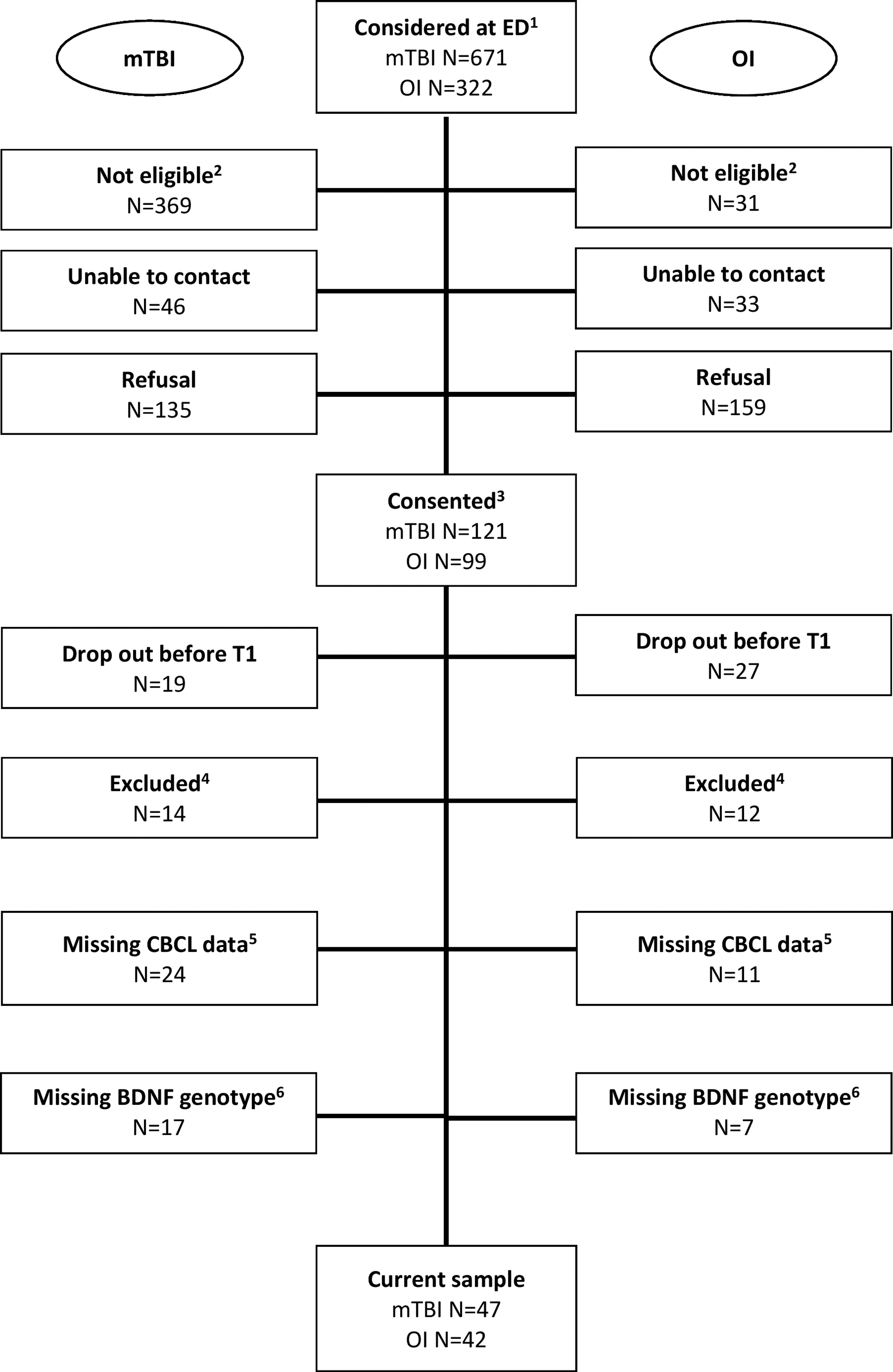
Recruitment and follow-up flowchart of the mild traumatic brain injury (mTBI) and orthopedic injury (OI) groups.

Recruitment and follow-up chart for the typically developing children.
Finally, among the children with complete CBCL data for both assessment time-points, there were 17 mTBI (27%), 7 OI (14%) and 11 TDC (16%) with missing BDNF genotype. The main reasons for missing genetic data were: 1) the parent did not want to participate in the genetic sub-part of the study (n = 13); 2) parent was no longer reachable or had abandoned the project at the time the data collection for the genetic sub-part of the study was in progress (n = 13); and 3) the parent did not return the sample that had been sent by mail with instructions for collection (n = 4). The proportion of children with missing BDNF genotype was similar across groups (χ2 (2) = 3.3, p = 0.19). There were no differences between families who agreed to participate in the genetic sub-study and those who refused, in terms of child age t(156) = 0.55, p = 0.55) and sex (χ2 (1) = 2.85, p = 0.58).
The final sample consisted of 145 children: 47 mTBI (29 boys, 62%), 42 OI (21 boys, 50%) and 56 TDC (30 boys, 54%). As detailed in Table 1, there were no between-group differences for the following demographic variables: child age at each assessment, age at injury (for the two clinical groups), sex ratio, ethnicity, and family living arrangement. However, a between-group difference was observed for parental education level (p = 0.01), with parents in the mTBI group having significantly lower educational qualifications than parents in both the OI and the TDC group.
In the overall sample, 91 participants carried the wild-type Val66Val polymorphism (Val/Val homozygotes) and 54 participants carried at least one copy of the Met allele (Val66Met or Met66Met), representing 37% of the study sample. Participants with Val/Met and Met/Met genotypes were combined for statistical analyses into a Met-allele carriers group. The proportion of Val/Val versus Met-allele carriers was similar for each participant group: mTBI (62% Val/Val vs. 38% Met carriers), OI (62% Val/Val vs. 38% Met carriers) and TDC (64% Val/Val vs. 36% Met carriers).
Main analyses
Externalizing problems
For the Externalizing Problems score, there was a significant main effect of Group [F(2, 139) = 4.71; p = 0.01], regardless of Genotype or Time. Contrasts revealed that children with mTBI (M = 54.04; SE = 1.21) had higher reported rates of externalizing symptoms than TDC [M = 49.04; SE = 1.12; p = 0.003, 95% CI (1.75 – 8.26)]. It is noteworthy that although there was a significant group difference, mean scores remained in the average range (i.e., below the clinical significance level cut-off) for all three groups. There was no main effect of Genotype or Time, nor was there a Group x Genotype × Time interaction.
Internalizing problems
Results for the Internalizing Problems score are presented in Figure 3. There was a significant main effect of Group, [F(2, 139) = 4.39; p = 0.014], with children in the mTBI group (mean [M] = 53.58; standard error [SE] = 1.42) having higher reported rates of internalizing problems than children in both the OI [M = 49.13; SE = 1.50; p = 0.033, 95% CI (0.36 – 8.54)] and the TDC groups [M = 48.07; SE = 1.32; p = 0.005, 95% CI (1.68 – 9.34)]. However, there was no main effect of Time (p = 0.13) or Genotype (p = 0.26).

CBCL Internalizing problems 6 and 18 months post-injury. At T1, the difference between Val/Val and Met-allele carriers in the mTBI group was significant. At T2, Val/Val and Met carriers who sustained mTBI had similar rates of internalizing problems. However, regardless of genotype, children with mTBI had significantly more internalizing symptoms than children in the OI and the TDC groups. Color image is available online.
The Group × Genotype × Time interaction was significant [F(2, 139) = 3.05; p = 0.05]. Visual inspection of the means and interaction graph indicate that at T1, Val/Val participants who sustained mTBI presented more internalizing problems (M = 57.48, standard deviation [SD] = 10.08) compared with Met-allele carriers who sustained mTBI (M = 47.61, SD = 11.42), the latter being comparable to all others groups (Val/Val and Met-allele carriers in the OI and TDC groups). Accordingly, a planned follow-up analysis indicated that at T1, the difference between Val/Val and Met-allele carriers in the mTBI group was significant [t(50) = 3.19; p = 0.002] and represented a large-sized effect d = 0.90. At T2, however, Val/Val and Met carriers who sustained mTBI had similar rates of internalizing problems [t(45) = 0.99; p = 0.33]. At T2, regardless of genotype, there was a significant Group difference [F(2, 142) = 4.52; p = 0.01], with mTBI children (M = 55.04; SE = 12.35) presenting more internalizing symptoms than children in both the OI (M = 49.43; SE = 8.73; p = 0.02, 95% CI (0.99 − 10.24)] and the TDC groups (M = 48.98; SE = 11.37; p = 0.01, 95% CI (1.75 – 10.37)].
Note that a more conservative model including parental education level as a covariate was conducted and yielded similar results; the Injury Group × Genotype × Time interaction was still significant [F(2, 138) = 3.06; p = 0.05].
Discussion
This prospective cohort study examined the role of BDNF Val66Met, a naturally occurring polymorphism in the BDNF gene, with respect to behavioral outcomes after early mTBI. This BDNF polymorphism is thought to represent a risk factor for poorer functional outcome after brain injury, given that the Met allele is associated with decreased activity-dependent BDNF release, and therefore less neurotrophic support for neuroplasticity. Contrary to our initial hypothesis, the results of the study provide evidence for a protective effect of the Met allele on internalizing behavior symptoms 6 months after mTBI sustained during early childhood. As such, in the mTBI group, Val/Val homozygotes presented significantly more internalizing symptoms than Met-allele carriers. The latter had similar levels of symptoms as orthopedically injured and non-injured control participants, for whom there was no differential effect of genotype. The protective effect of the Met allele in the mTBI group disappeared over the following 12-month period. That is, at 18 months post-injury, all children with mTBI continued to show more internalizing symptoms compared with orthopedically injured and non-injured peers, independent of genotype.
The results obtained at 6 months post-injury contrast with those of two prior adult mTBI studies showing greater internalizing behavior problems for Met-allele carriers. 29,30 Discrepancies between pediatric and adult findings are perhaps not surprising, given that the structure and function of the pediatric brain is rarely analogous to that of the adult brain, 42 but the current pattern of results contrasts with those typically found in adults. In typical development, gene- or environment-related alterations in BDNF levels have different effects on behavioral phenotypes across development. 31 During the preschool period, the immature brain develops rapidly due to normal mechanisms of brain plasticity. This plasticity is considered beneficial in the context of healthy development because it drives brain growth through the creation of new neurons and synaptic connections, which are refined as new learning occurs. However, mechanisms of brain plasticity that occur in response to brain injury could instead be detrimental in the developing brain.
There is evidence of TBI-induced altered developmental plasticity mechanisms after pediatric TBI, including for example faulty neurotransmission, enhanced apoptotic injury-induced cell death, and perturbations in neuronal connectivity. 43 These types of maladaptive plasticity contribute to making the developing brain more vulnerable to the effects of injury and may explain why young children show poorer functional recovery compared with older children and adults, despite the fact that they have a higher potential for plasticity. This adds to the fact that sustaining brain injury during early childhood may disrupt the pre-determined sequence of brain maturation and the resulting developmental processes. In other words, an increased potential for TBI-induced plasticity allowed by greater availability of BDNF neurotrophins in Val/Val homozygotes can interfere with the normal developmental blueprint and thus may not translate into better functional recovery. 44 Together, these developmental factors may explain why Val/Val homozygotes are at greater risk for poor behavioral outcome in the first few months after sustaining a mTBI during early childhood.
Another hypothesis to explain the disparity between the results obtained in our study of early childhood compared with those observed in adults is that natural concentrations of BDNF in the central nervous system vary with age. Consequently, an allele that confers reduced release of BDNF may represent a risk factor at a particular age, while offering protection during another developmental period. 31 In a developmental period during which natural expression of BDNF protein is already abundant, the overabundance of BDNF in response to TBI could trigger biochemical reactions leading to neuronal death, thereby compromising post-TBI recovery. In line with these explanations, findings from a study of older TBI patients and with more severe injuries revealed Gene × Age interactions with BDNF in relation to TBI mortality. 45 The authors suggest that age-specific risk profiles may be related to differential expression patterns in the relative balance of pro-survival/pro-apoptotic BDNF target receptors across aging. It is not clear, however, whether this explanation could apply to milder forms of TBI, or even within a developing, immature brain.
Prior studies in other clinical populations have demonstrated the maladaptive effect of an overexpression of BDNF, in particular with regard to the development of neuropathic pain 46 and epileptogenesis. 47
Impact of BDNF Val66Met on long-term recovery
All children with mTBI, independent of genotype, presented more internalizing symptoms than orthopedically injured and non-injured peers at 18 months post-injury. Compared with the 6 months post-injury time-point, this suggests a persistence of internalizing behavior symptoms in Val/Val homozygotes, and an increase in symptoms in Met-allele carriers, who were initially comparable to orthopedically injured and non-injured peers 6 months post-injury, as seen in Figure 3. This long-term persistence of symptoms is somewhat surprising after mTBI, which is usually associated with more transient effects. 4,5 The fact that there is no longer any differential effect of genotype 18-months post-injury suggests that the etiology of behavioral symptoms in the long-term may no longer be neurological.
For example, at 18-months post-injury, parents may perceive and report behavioral difficulties that are real, but that may be a result of environmental changes related to the accident (e.g., changes in parenting practices) that may affect all children with mTBI, independent of their genotype. It is possible that child behavior problems that have a neurological basis have a detrimental impact on parenting quality, impeding behavioral recovery. 37,48 In short, it can be assumed that at 6 months post-injury, children show internalizing symptoms related to a combination of neurological processes (mediated by BDNF genotype) and non-neurological factors, but that over time, symptoms crystallize due to family-related or other environmental factors, nonetheless related to TBI, but non-neurological.
Limitations and future studies
The main limitation of this work is the reliance on a sole informant (the mother) for providing post-injury behavioral ratings. As with any parent-report questionnaire, it is not possible to blind to group status and this could introduce personal bias and confounds related to parental perception and mental state, for example. However, with regard to the difference observed between Val/Val homozygotes and Met-allele carriers in the mTBI group, genotype is unknown to mothers and therefore cannot be influenced by parental bias. Another limitation of the study is the absence of potential environmental risk factors (e.g., related to parenting sensitivity and socio-economic status) known to contribute to TBI outcome to assess their interplay with BDNF genotype. Indeed, in non-injured populations, it has been shown that BDNF interacts with environmental risk factors and adversity to predict neuroanatomical and behavioral phenotypes. 49 -51
An additional limitation of the study is the small sample size for a genetic study, as well as the candidate gene approach that was used. Results of candidate gene studies are not always replicated by follow-up studies or by genome-wide association studies and should be interpreted with caution. Future studies should reproduce the results of this study in independent cohorts, as well as consider genome-wide approaches. A study conducted by Kurowski and colleagues 52 shows promise using a genomic approach, informed by systems biology, to study combinations of genes underpinning an array of biologic processes involved in TBI. The current project nevertheless makes a novel contribution given the paucity of genetic association studies specific to pediatric TBI and especially in early childhood. 32 Finally, another limitation of the study is that Caucasians are over-represented in the cohort studied (i.e., almost 90% in the mTBI group). Given that it is possible that a particular genotype confers different cognitive and behavioral phenotypes depending on ethnicity, 53 future studies should seek to include a larger and more varied sample and to analyze the results according to ethnic differences.
Future studies could also investigate the role of other genes and polymorphisms that may influence pediatric TBI outcome. Promising gene candidates could be those potentially involved in pre-injury risk factors for TBI, response to neurotrauma, repair, and plasticity processes, or pre- and post-injury cognitive capacity and reserve. 13 In fact, a recent study used a polygenic risk scores approach to examine the differential cumulative influence of candidate genes involved in the inflammatory response on pediatric TBI outcomes. 54 Finally, future studies should also explore the role of BDNF Val66Met on cognitive functions that could underlie behavioral problems after pediatric TBI, such as executive functions, decision-making and social cognition.
Conclusion
The current study provides support for a transient protective effect of the Val66Met polymorphism on internalizing symptoms after early mTBI. In the particular context of early childhood mTBI, it appears that enhanced potential for neural plasticity in Val/Val homozygotes might be more deleterious than beneficial for internalizing behaviors in the first 6 months post-injury. Future studies of pediatric TBI should investigate combined and interactive effects of genetic variants and environmental risk factors, thus providing a better understanding of the wide variability in outcomes.
Footnotes
Acknowledgments
We are grateful for the work of the members of the LION project. We also thank the Emergency Department team at Ste-Justine Hospital, in particular, Dr. Jocelyn Gravel, pediatric emergency physician, as well as Maryse Lagacé, Ramona Cook, and the PIEUVRES group for their assistance with recruitment.
Funding Information
This work was supported by the Canadian Institutes of Health Research (grant number MOP111036).
Author Disclosure Statement
The authors report no conflicts of interest.