
Abstract
Traumatic brain injury (TBI) produces microstructural damage to white matter pathways connecting neural structures in pre-frontal and striatal regions involved in self-regulation (SR). Dorsal and ventral frontostriatal pathways have been linked to cognitive (“cool”) and emotional (“hot”) SR, respectively. We evaluated the relation of frontostriatal pathway fractional anisotropy (FA) 2 months post-TBI on cool and hot SR assessed 7 months post-TBI. Participants were 8–15 years of age, including children with uncomplicated mild TBI (mTBI; n = 24), more severe TBI (complicated-mild, moderate, severe [cms]TBI; n = 60), and typically developing (TD) children (n = 55). Diffusion tensor tractography was used to map frontostriatal pathways. Cool SR included focused and sustained attention performance, and parent-reported attention, whereas hot SR included risk-taking performance and parent-reported emotional control. Multivariate general linear models showed that children with cmsTBI had greater parent-reported cool and hot SR difficulties and lower dorsal and ventral FA than TD children. Focused attention, risk taking, and emotional control correlated with FA of specific dorsal and ventral pathways; however, only the effect of TBI on focused attention was mediated by integrity of dorsal pathways. Results suggest that frontostriatal FA may serve as a biomarker of risk for SR difficulties or to assess response to interventions targeting SR in pediatric TBI and in broader neurodevelopmental populations.
Introduction
Children and adolescents with traumatic brain injury (TBI) often experience difficulties with self-regulation (SR) that contribute to long-term problems in social and academic settings. 1,2 Disruption has been noted in both cool (e.g., attention, vigilance, cognitive control) and hot (e.g., risky decision making, emotional control) aspects of SR. 3 –7 Frontostriatal structures and connected pathways are vulnerable in TBI, 8 and also contribute to SR processes. 7,9,10 For example, difficulties in cool and hot SR have been linked to dorsal (e.g., pre-frontal, anterior cingulate, caudate) and ventral (e.g., orbitofrontal, rostral cingulate, ventral striatum) frontostriatal dysfunction, respectively, in children with attention-deficit/ hyperactivity disorder (ADHD) and conduct disorder. 10 –13 However, no known studies have investigated whether integrity changes to dorsal and ventral frontostriatal pathways in children with TBI might differentially relate to cool versus hot SR, which are critical to everyday functioning. The present study therefore seeks to understand the interrelations of frontostriatal pathways and SR; doing so is highly relevant to addressing issues related to prediction and management of altered SR following TBI.
“Cool” and “hot” self regulation and frontostriatal pathways
Nigg 14 proposed the terms “SR of cognition” and “SR of emotion” that map onto cool and hot top-down processes, 12,15 respectively. SR of cognition, or cool SR, which involves conscious control of thought and actions, includes focused attention (e.g., ability to concentrate on a specific stimuli) and sustained attention (e.g., ability to attend to a stimuli for an extended period of time). 12,14,16 In contrast, SR of emotion, or hot SR, includes top- down processes moderating control of emotions and risk-taking propensity. 15,17 Even in healthy populations, developmental influences such as age and sex have potential implications for cool and hot SR outcomes. Risky decision making and difficulties with emotional control increase from early childhood to middle adolescence. 10 Further, boys tend to show higher levels of externalizing behavior problems, demonstrate greater risk-taking propensity, and may be more susceptible to peer pressure to engage in risky behaviors than girls. 18 –20
Dorsal and ventral frontostriatal circuitry are dissociable and related to aspects of cool and hot SR, respectively. Dorsal frontostriatal pathways supporting cool SR connect ventrolateral pre-frontal (VLPFC), dorsolateral pre-frontal (DLPFC), and dorsal anterior cingulate cortices (dACC) to the caudate. 21,22 Structural differences in the VLPFC, DLPFC, and dACC are related to attentional problems. 23,24
Synthesizing past decades of literature with recent empirical revisions on developmental theories of self-control, Casey 10 presents a model of the neural network central to the SR of emotion. In Casey's model, neural correlates of hot SR such as risk-taking and emotional control include specific ventral frontostriatal regions. The ventral striatum (including the nucleus accumbens), orbitofrontal, and medial pre-frontal regions are heavily linked to reward and emotion processes. 7 Medial pre-frontal and rACC functional activation has also been linked with regulation of emotional decision making and inhibition. 25,26
Cool and hot self-regulation and white matter pathways after tbi
Difficulties with cool and hot SR may develop or worsen following pediatric TBI. Cool SR, such as focused and sustained attention, is negatively impacted following pediatric TBI. 3,5,27 Difficulties in attention are reflected in the high rate of acquired, or secondary ADHD following TBI, 28 and place children at elevated risk for compromised attention and executive functions including planning and working memory. 29 Hot SR problems may be manifested by increased emotional dysregulation, risky decision making, and increased risk for externalizing behaviors such as oppositional and conduct disorders. 5,6,30 Although greater severity of TBI has generally been linked to more significant problems in cool and hot SR, 5,31 there are inconsistencies. 4,29,32 These inconsistencies may be related in part to the inherent heterogeneity of TBI and the challenges of using the Glasgow Coma Scale (GCS) as a marker of severity. Therefore, improved characterization of clinical markers and predictors of impairment, including markers such as neuroimaging, would assist in determining those at greater risk.
Despite the emerging literature on SR deficits following pediatric TBI, there is a lack of research on how injury to neural structures affects SR in general, and how white matter changes to dorsal and ventral frontostriatal pathways differentially relate to cool and hot SR in particular. The advent of structural neuroimaging techniques such as diffusion tensor imaging (DTI) allows quantification of disruption in white matter pathways. DTI provides a sensitive measure of microstructural changes to white matter by measuring the diffusion of water molecules in the brain. 33 Fractional anisotropy (FA) is a measure of diffusion such that higher FA values generally indicate more dense and consistent ordering of axons, and greater myelination. 34 White matter FA is often reduced following pediatric TBI. 8,35
In relation to cool SR, a recent meta-analytic review of studies using DTI following pediatric TBI showed that attention difficulties were related to lower FA at least 1 month post-injury in frontal and cingulate regions. 36 School-age children with moderate to severe TBI demonstrated reduced cognitive control that was related to lower FA in the cingulum. 37 In relation to hot SR, Johnson and colleagues 38 found that, in comparison with children with orthopedic injury, children with moderate to severe TBI had lower FA in the uncinate fasciculus, white matter extending from the orbitofrontal cortex (OFC) to the anterior temporal pole, which predicted subsequent emotion dysregulation.
The only study investigating white matter integrity of frontostriatal pathways found that higher diffusion of ventral striatum was correlated with greater executive functioning difficulties in children and adolescents 5–15 years of age, following TBI. 8 However, hot SR measures were not included in this research, and analyses targeted ventral striatum pathways. Therefore, it is unclear if injury effects on ventral striatum are related to hot SR or if the dorsal striatum also mediates SR differences.
The present study
It is unknown whether microstructural changes in dorsal and ventral frontostriatal pathways after TBI are differentially related to cool versus hot SR, or how pathways and behavior interact longitudinally. Moreover, how demographic and TBI markers influence pathway integrity and its relation to SR are also unknown. Therefore, the present study investigated whether integrity of specific dorsal and ventral frontostriatal pathways (see Fig. 1), assessed 2 months after injury, predicted SR in children and adolescents with differing severity of TBI assessed 7 months after injury, relative to a healthy comparison group. SR was assessed using both direct test and parent report.
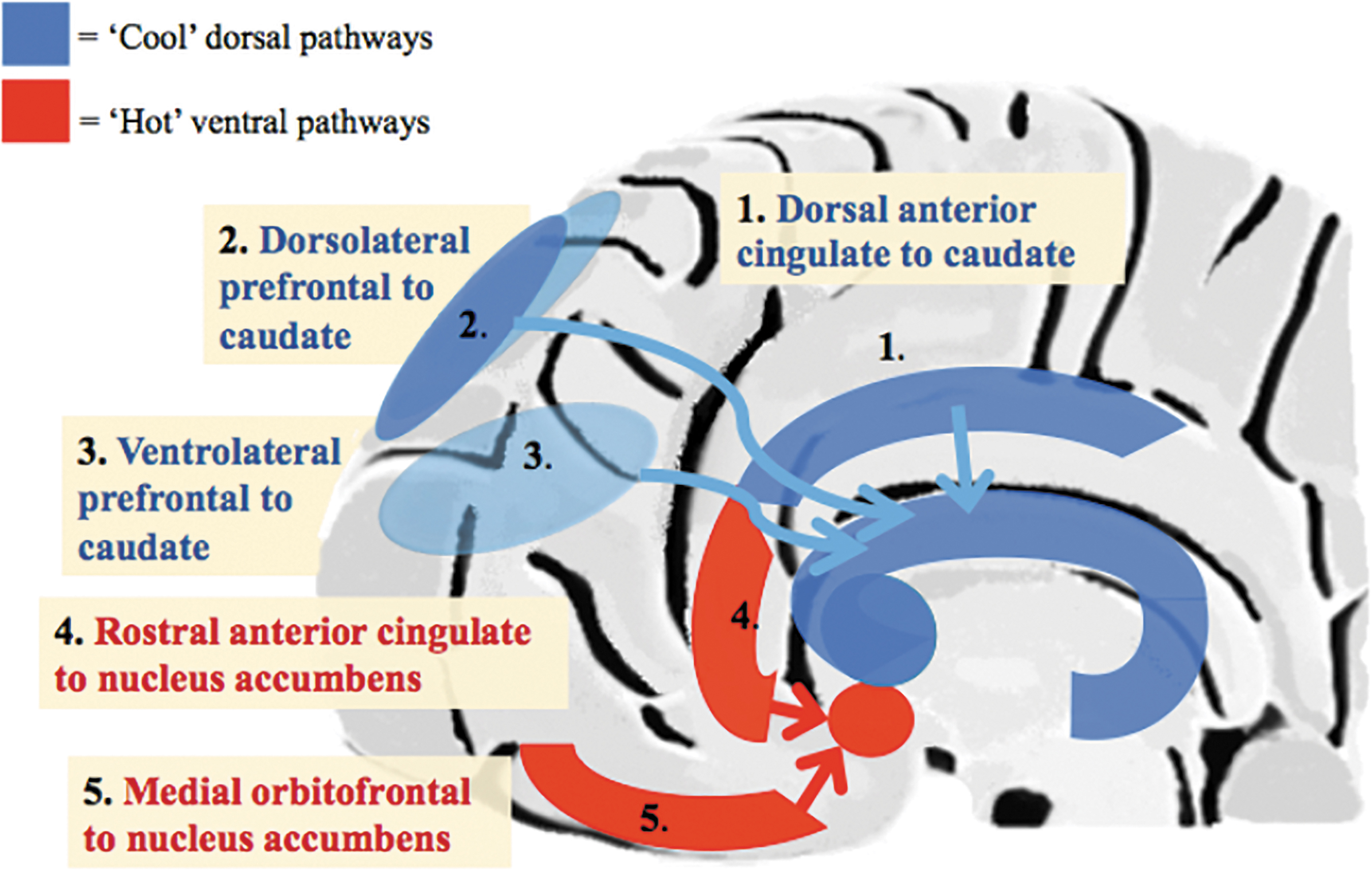
Frontostriatal pathways of interest. Schematic representation showing sagittal view of dorsal and ventral frontostriatal pathways regulating cool and hot self-regulation (SR), respectively. Anterior (left) to posterior (right) orientation. Color image is available online.
We expected that (1) greater TBI severity would be associated with greater SR difficulties and lower FA in both dorsal and ventral frontostriatal pathways, (2) boys would have greater difficulties than girls on measures of hot and cool SR, and (3) dorsal and ventral frontostriatal FA would mediate the effect of injury group on cool and hot SR, respectively.
Methods
Participants
Participants were drawn from a longitudinal prospective TBI study. Inclusionary criteria for TBI included admission to the emergency department or level 1 trauma center at a major urban hospital. The comparison group of typically developing (TD) children was recruited through posting flyers throughout the community. All participants in the study were 8–15 years of age at enrollment. Exclusionary criteria for both groups included: previous history of brain injury, severe developmental or learning disability, hospitalization for a psychological disorder, or penetrating brain injury. Of the 147 (56 TD, 91 TBI) participants originally enrolled in the study, 98 (41 TD and 57 TBI) contributed to imaging data at 2 months and 128 (52 TD and 76 TBI) contributed behavioral data at 7 months (see flow chart Fig. S1). TBI severity was classified into uncomplicated mild TBI (mTBI) with no intracranial lesions and complicated-mild, moderate, and severe TBI (cmsTBI) using the admission GCS
39
and acute computed tomography (CT) findings. The Injury Severity Score (ISS) assessed bodily injury severity and was calculated by summing the squares of the three most severely injured body regions as rated by the Abbreviated Injury Scale (AIS).
40
In subjects with mild or moderate TBI, skeletal or body AIS scores were
Behavioral measures
Validated direct test and parent report measures of SR were used to evaluate SR. All measures have adequate split-half or test–retest reliability.
Regarding cool SR, the Conners’ Continuous Performance Test (CPT-II) 41 was used to assess focused and sustained attention. The CPT-II is a computerized go/no go task. Omission errors, or the number of times a participant fails to respond to a target, were used as a measure of focused attention. Hit reaction time change by block, or the slope of change in reaction time over the six blocks as the task progresses, measured sustained attention. Higher T scores represent greater difficulty.
Parent-report from the Strengths and Weaknesses of ADHD and Normal Behavior measure (SWAN) assessed behavioral attention. 42 The Inattentive Behavior subscale is the average of Items 1–9 rated on seven-point Likert type scale, with ratings ranging from −3 to +3; lower scores indicate greater inattention.
Regarding hot SR, the Balloon Analogue Risk Task (BART) is an established task assessing risk-taking propensity. Participants were told that after the task, the number of points earned would determine the size of their prize reward. In each of 30 trials presented in the same order, participants choose how many times to pump an empty balloon that could explode on an unpredictable schedule at any point from 1 to 128 pumps. Cashing out prior to explosion is a safe option and increases payout; continuing to pump for greater reward is a riskier option. This measure has consistently correlated well with self-report measures of risk-taking. 43 The average number of adjusted pumps for unexploded balloons predicts risk-taking propensity. A greater number of pumps represents a higher level of risk taking.
The Behavior Rating in Executive Functioning (BRIEF) 44 is a parent report of everyday executive functioning problems. The Emotional Control subscale assessed emotion regulation. Higher T scores (mean = 50, standard deviation [SD] = 10) indicate greater difficulty with emotion regulation.
The Pubertal Development Scale 45 is a validated and reliable self-report measure of pubertal status. Child and parent independent ratings of changes associated with puberty were collected, including growth in height, body hair, and skin, and sex-specific changes. Parent and child ratings were averaged to yield a consensus score from 1 (pre-pubertal) to 4 (post-pubertal).
Procedure
Data on retrospective pre-injury functioning for the TBI groups and baseline functioning for the TD group were gathered at a baseline clinical visit. Participants were scanned ∼2 months following injury (for the TBI group). Trained research assistants administered the CPT-II and BART at 7 months. Parents completed the BRIEF measure, and SWAN ratings were obtained via clinical interview as part of a structured Diagnostic and Statistical Manual of Mental Disorders (DSM) interview at baseline and 7-month visits. Behavioral outcome data were collected from all participants who attended their baseline and 7-month follow-up. All procedures were approved by the participating institutions’ respective institutional review boards (IRBs).
Regarding image acquisition, the current study used data acquired on a Philips 3T magnetic resonance (MR) scanner with a 32 channel head coil. Participants were scanned at the University of Texas McGovern Medical School. An echo planar imaging sequence (repetition time [TR] = 8700 ms; echo time [TE] = 67 ms; 65 slices total; square field of view [FOV] = 240 mm; slice thickness = 2.5 mm) was used for diffusion weighted data collection. High resolution T1-weighted anatomical scans were collected (TR = 8.1 ms, TE = 3.7 ms, flip angle = 6 degrees, matrix = 256 × 256, slice thickness = 1 mm, and voxel size = 1 mm3). Toward the end of data collection, the scanning facility upgraded the scanner with a Philips 3T Ingenia, and 45 of our participants with valid DTI data were scanned after the upgrade. We performed fidelity analysis to match diffusion-weighted and T1-weighted scanning protocols; however, some variations may remain. To account for differences in scanner, scanner change was included as a covariate in all DTI analyses.
FreeSurfer 5.3.0 (
Dorsal pathways included DLPFC to caudate, VLPFC to caudate, and dACC to caudate parcellations. Freesurfer divisions included: DLPFC = rostral middle frontal and caudal middle frontal; VLPFC = pars triangularis, orbitalis, and opercularis; and dACC = caudal anterior and posterior cingulate cortex. Ventral pathways included medial OFC (mOFC) to nucleus accumbens and rostral anterior cingulate cortex (rACC) to nucleus accumbens. We generated exclusion masks for DTI analysis corresponding to ventricular regions using the same image-processing pipeline.
FMRIB Software Library (FSL) 5.0.1 (
Diffusion tensor tractography (DTT) maps white matter pathways using DTI voxel-based values by reconstructing fibers by inferring directional information from acquired diffusion metrics, allowing for a fully reformed assessment of white matter pathway integrity. The current study used probabilistic methodology to determine fiber orientation and to designate voxels in white matter pathways. This method is particularly suitable in studying children with TBI or other neurological insults, given that pathway structure and relations to the rest of the cortical and subcortical network may not be as expected. Probabilistic tractography algorithm (FSL: probtrackx) uses voxelwise probability distributions to generate a distribution of pathways connecting specified regions, and this was applied for seed to target fiber tracking. This algorithm has been used for recent investigations of pre-frontal to subcortical white matter in children. 49 We initiated one-way direction fiber tracking from each voxel in a seed mask to track all paths connecting to the target mask and discarding paths in contact with exclusion masks. Three dorsal pathways were constructed as the seed to termination points of DLPFC to caudate, VLPFC to caudate, and dACC to caudate. Two ventral pathways were constructed with seed to termination points: mOFC to nucleus accumbens, and rACC to nucleus accumbens. Thus, for each of the five seed-to-target combinations, we calculated the average FA for each hemisphere along the entire pathway. Fiber tracking within a diffusion space generated 5000 streamline samples (step length = 0.5 mm; curvature threshold = 0.2). Because tract volume varies based on the size of seed regions, we normalized tract maps in order to account for voxel count in seed masks by dividing the number of streamline samples present in the voxels of the tract maps by the way-total. The way-total consisted of the total number of generated tracts from each seed mask that reached at least one of the other masks and had not been rejected by mask inclusion/exclusion criteria. Tracts were thresholded to voxels with FA values >0.2 in order to ensure pathways included only white matter.
Statistical analysis
Data screening strategies, assumptions, and goodness-of-fit checks were conducted before behavioral and DTI analyses were run. Multivariate general linear models (GLMs) were conducted to examine the effect of group (TD, mTBI, cmsTBI), age, and sex, and their interactions on the right and left pathway FA with scanner change as a covariate. One multivariate GLM was run with each of the five pathways of interest as the dependent variable (DV) (dorsal pathways to caudate: dorsal ACC, ventrolateral pre-frontal cortex [PFC], dorsolateral PFC; ventral pathways to nucleus accumbens: rostral ACC, medial OFC). Non-significant interaction terms were trimmed. Significant multivariate effects were followed up using Bonferroni-adjusted pairwise comparisons. In order to minimize the number of analyses using correlated metrics, initial study design focused on FA as our primary DTI metric. However, considering the use of multiple DTI metrics may expand our understanding of underlying mechanisms; 50 –53 therefore, we conducted post-hoc GLM on mean, axial, and radial diffusivities for pathways showing significant group differences in FA using Bonferroni corrections. This methodological approach is similar to recent published research on white matter changes in pediatric TBI. 35
The same approach was used with SR measures as the DV (Cool SR: focused and sustained CPT scores, parent inattention ratings; Hot SR: risk taking and parent emotional control ratings). Pre-injury parent ratings of inattention and emotional control were included as a covariate in models evaluating post-injury SWAN and BRIEF ratings, respectively.
Effect sizes benchmarked against Cohen's criteria were evaluated using partial eta squared (η p 2 ) for multivariate and univariate models (small = 0.01, medium = 0.06, and large = 0.14) and Hedges g for follow-up pairwise comparisons between groups. Imaging analyses were run for participants with and without behavioral data, and behavioral analyses were run for those with and without imaging data.
Multicategorical mediation analyses were conducted through PROCESS with 10,000 bootstrap re-samplings and 95% confidence intervals 54 to examine whether the effect of group on SR outcomes was mediated through pathway FA. From five right and five left hemisphere pathways, target pathways were selected if FA varied significantly by group or if partial (age) Spearman or Pearson correlations identified significant relations of pathway FA with SR outcomes. Four mediation models were run with group as the independent variable (IV) (with the TD group as the reference group) and scanner change as a covariate; DVs were 7-month CPT omission errors, BART pumps, and BRIEF emotional control with pathway FA at 2 months as the mediators.
Results
Preliminary analyses
Table 1 compares clinical and demographic data for the TD (n = 55), mTBI (n = 24), and cmsTBI groups (n = 60). Demographic variables, including age, sex, race/ethnicity, socioeconomic status, and pubertal status were all comparable across groups (all ps > 0.17). Scanner update was equally distributed in participants with valid DTI data. GCS distribution for the 84 subjects with TBI included 26.2% in the 3–8 range (n = 22), 7.1% in the 9–12 range (n = 6), and 66.7% in the 13–15 range (n = 56).
Demographics and Clinical Characteristics by Group
mTBI, uncomplicated mild traumatic brain injury; cmsTBI, complicated mild, moderate, and severe
traumatic brain injury; M, mean; SD, standard deviation; ISS no head, Injury Severity Score excluding score for head injury.
Group differences in frontostriatal white matter
For all multivariate GLMs, group by age and group by sex interactions were non-significant and therefore trimmed. Table 2 provides final multivariate models for dorsal and ventral pathways. Table S1 provides descriptive statistics for FA of dorsal and ventral pathways by hemisphere. The main effect of age was non-significant across models.
Multivariate Models for Dorsal and Ventral Frontostriatal Pathways
ACC, anterior cingulate cortex; PFC, pre-frontal cortex; η p 2 , partial eta squared effect size.
Bonferroni adjusted pairwise comparisons revealed: a, cmsTBI < TD; b, cmsTBI < mTBI;
Multivariate group differences were demonstrated for dACC cortex to caudate pathway (bilaterally), with a medium effect size. Follow-up pairwise comparisons showed that the cmsTBI group had significantly lower left and right FA than the mTBI group and the TD group, while FA in the mTBI group did not significantly differ from in the TD group. The main effect of sex was significant with a medium to large effect size, such that males had lower pathway FA across groups. To investigate whether the significant effect of sex was related to pubertal status, post-hoc analyses included the Pubertal Development Score, which did not alter findings. Post-hoc GLMs of dACC to caudate were non-significant for mean diffusivity (MD) and axial diffusivity (AD) and did not survive correction for radial diffusivity (RD) (Table S2).
Bilateral VLPFC to caudate pathway FA differed significantly across groups, demonstrating a medium effect size. Adjusted pairwise comparisons showed that the cmsTBI group had significantly lower left and right FA than the mTBI group, but not the TD group. Post-hoc analyses examining diffusivities demonstrated that MD and RD differed across groups, with medium effect sizes. Adjusted pairwise comparisons showed that the cmsTBI group had significantly greater left-sided MD than the mTBI and TD groups. Regarding RD, the cmsTBI group had significantly greater RD than the mTBI group, but not the TD group. The DLPFC to caudate pathway failed to demonstrate significant group differences. For the ventral pathways, multivariate models did not identify significant effects of group, age, or sex.
Group differences in cool and hot self-regulation
Descriptive data and group comparisons are presented in Table 3 for baseline/pre-injury and 7 month cool and hot SR variables. SWAN, but not BRIEF scores, differed at baseline. On the SWAN, the mTBI group showed worse baseline attention than the TD group (p = 0.012). Intercorrelations among SR variables are provided in Table S3.
Descriptives for Baseline and 7 Month Cool and Hot Self-Regulation
mTBI, uncomplicated mild traumatic brain injury; cmsTBI, complicated mild, moderate, and severe traumatic brain injury.
SWAN, Strengths and Weaknesses of Attention-Deficit/Hyperactivity Disorder and Normal Behavior measure; CPT, Conners’ Continuous Performance Test; BRIEF, Behavior Rating in Executive Functioning; T, T score; RT, reaction time.
Two multivariate GLMs examined the effects of TBI group, age, sex, and their interactions on cool and hot SR, controlling for baseline SWAN ratings (Table 4). Group by age and group by sex interactions were non-significant and were trimmed. Cool SR differed significantly across groups; univariate analyses demonstrated group differences to be driven by parent report of attention at 7 months, but not by child performance on tasks of sustained and focused attention. Subjects with more severe TBI had significantly greater parent-reported inattention than TD subjects, with a large effect size (p < 0.001; g = 0.769). Younger children across groups demonstrated a greater number of errors on age-normed cool SR tasks of focused and sustained attention, with small (η p 2 = 0.04) and medium (η p 2 = 0.07) effect sizes, respectively. No significant effect of sex was detected.
Multivariate Models For Cool And Hot Self-Regulation
Bonferroni adjusted pairwise comparisons revealed: a, cmsTBI < TD group; b, cmsTBI < mTBI group;
Multivariate GLMs investigating behavioral outcomes in hot SR showed significant group differences, with a medium effect size (Table 4). Group differences were driven by parent-reported emotional control at 7 months, with a large effect size (η p 2 = 0.42), with no group differences in risk-taking task performance. Bonferroni-adjusted follow-up analyses showed that subjects with more severe TBI had significantly greater emotional control difficulties than both subjects with mTBI, with a small effect (p = 0.012; g = 0.32), and TD subjects, with a medium effect (p < 0.001; g = 0.67). As expected, the effect of age was significant, with a medium effect size. Specifically, older participants across groups displayed a greater number of adjusted pumps on the BART, indicative of higher levels of risk-taking with a medium effect size (η p 2 = 0.05).
Mediation models examining white matter and group effects on behavior
Multi-categorical mediation models were run to examine whether frontostriatal white matter integrity mediated the direct effects of group (TD, mTBI, cmsTBI) on 7 month cool and hot SR difficulties, using the TD group as a reference group. 54 Given that FA in four pathways related to various cool and hot SR measures (Table S4), four multi-categorical mediation models were conducted. The indirect effect of cmsTBI group on CPT omission errors through the (right) dACC to caudate FA was significant (B = 0.115; Fig. 2a and b), such that lower FA accounted for a greater number of omission errors. Additionally, for the mTBI group, but not the cmsTBI group, the relationship between group and CPT omission errors at 7 months demonstrated a significant indirect effect through the VLPFC to caudate pathway FA (B = 0.060; Fig. 2b). Lower FA in this model also accounted for higher omission errors. Although the total effect was non-significant for these two models, findings meet the guidelines for mediation effect, given the significant indirect effects. 55 Contrary to expectations, there was no indirect effect of mean FA of rACC or mOFC to nucleus accumbens pathways on the relationship between group and BART pumps at 7 months. An exploratory model examining whether the effect of group on BRIEF Emotional Control was mediated by DLPFC to caudate FA failed to demonstrate a significant indirect effect.
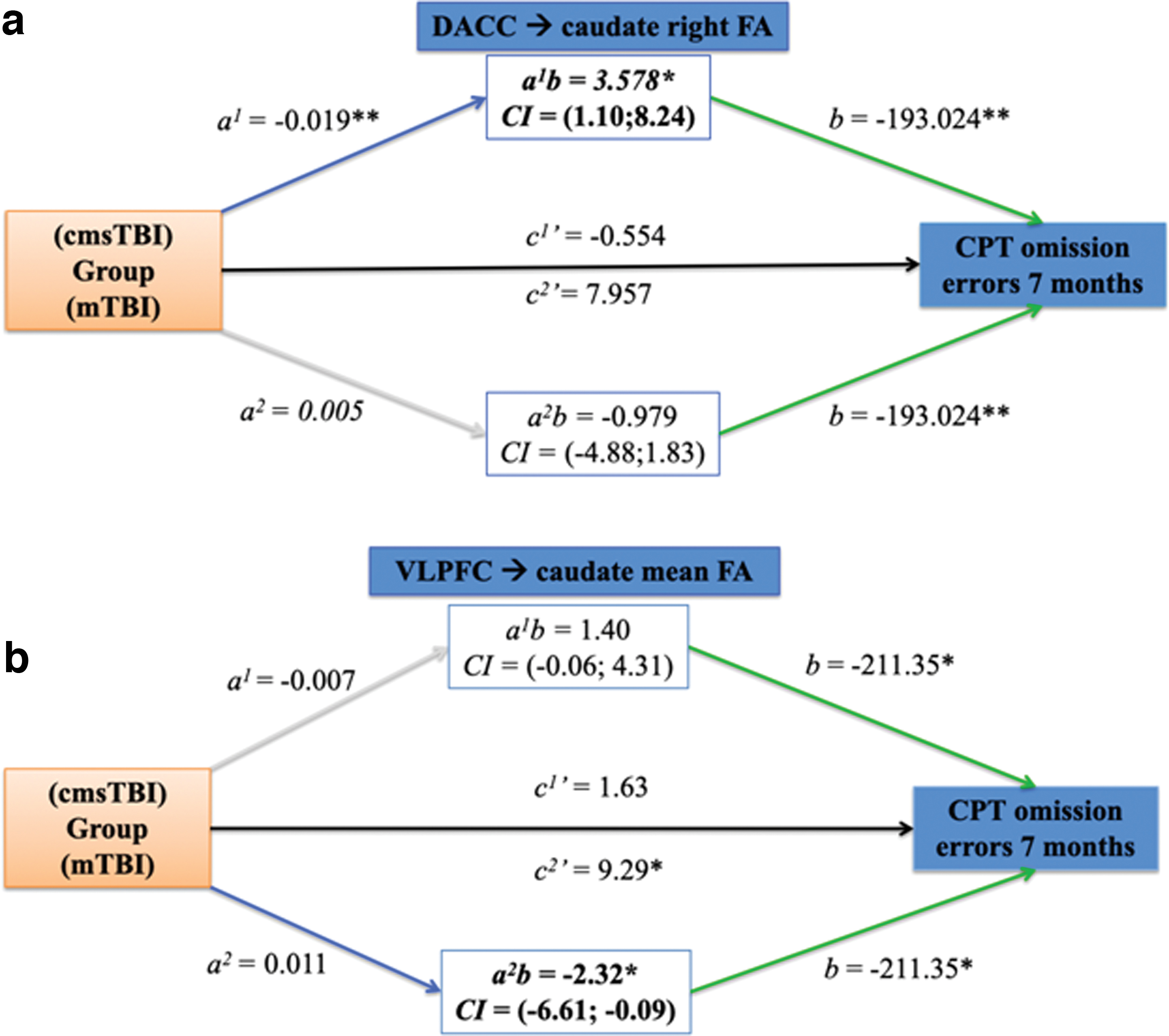
Multicategorical mediation models examining direct (c’) and indirect (ab) effects of group on Conners’ Continuous Performance Test (CPT) omission errors at 7 months through pathway fractional anisotropy (FA). Group variable consisted of two dummy coded levels (mild traumatic brain injury [mTBI], complicated-mild, moderate, severe [cms]TBI), with the typically developing group as the reference group. Path a1 and c1’ indicate cmsTBI, path a2 and c2’ indicate mTBI, path a1b shows indirect effect of cmsTBI on CPT omission errors, path a2b shows indirect effect of mTBI on CPT omission errors. Confidence intervals for both indirect effects are shown. The 95% confidence interval for the indirect effects was obtained through bootstrapping with 10,000 re-samples.
Discussion
The present study is the first to examine both dorsal and ventral frontostriatal white matter integrity in core pathways 2 months following TBI using clinically relevant and theoretically based models of SR. Relative to TD subjects and/or those with uncomplicated mild TBI, white matter integrity was reduced following more severe TBI in bilateral pathways connecting dACC and VLPFC to the caudate, as well as in the pathway connecting the right mOFC with the nucleus accumbens. Subjects with TBI showed more difficulties than healthy subjects with parent-reported cool SR (inattention); more severe TBI was also associated with greater hot SR difficulties (emotional control) than other groups. Direct measures of sustained or focused attention and risk taking did not differ across groups. Although lower FA in bilateral rACC to nucleus accumbens pathways was associated with greater risk taking, pathway integrity did not mediate the relationship between group and risk taking. However, dorsal frontostriatal white matter integrity at 2 months partially mediated the relation of TBI severity to differences in direct measures of attention at 7 months post-injury. Specifically, lower dACC to caudate pathway FA predicted worse focused attention in subjects with more severe TBI (Fig. 2a), while lower FA of the VLPFC to caudate pathway predicted worse attention following uncomplicated mild TBI (Fig. 2b). As such, this study illustrates the importance of dorsal frontostriatal white matter for regulation of attention in TBI, similar to other disorders associated with attentional difficulties. 56,57 Findings can guide future research on neural correlates of self-regulatory difficulties following pediatric TBI and can inform theoretical understanding of attention and frontostriatal neural circuitry in broader neurodevelopmental populations.
Impact of TBI on white matter integrity and self-regulation
The lower white matter integrity in subjects with more severe TBI relative to those with mTBI and TD subjectst in several core pathways is consistent with the few prior structural imaging studies examining change in frontostriatal structures and pathways. For example, DTI findings following pediatric TBI show white matter differences in regions overlapping the current study's pathways of interest, including the anterior corona radiata, cingulate, and orbitofrontal white matter. 37,58,59 Current findings extend this line of research by showing bilateral reductions in dACC and VLPFC to caudate FA as well as right mOFC to nucleus accumbens FA following more severe TBI. Post-hoc investigations showed alteration in diffusivity (MD and RD) in the VLPFC to caudate pathway. This further indicates diminished white matter integrity in more severe TBI, potentially via compromised myelin sheath integrity or neuronal loss. 52,60 Overall, findings highlight the importance of DTI to serve as a potential biomarker to detect selective changes in frontal and subcortical brain regions following more severe TBI and suggest underlying pathophysiological mechanisms contributing to white matter disruption.
After accounting for pre-injury functioning, subjects with more severe TBI showed greater difficulties on parent-reported measures of cool and hot SR assessing inattention and emotional control 7 months post-injury than healthy subjects and those with mTBI. These findings add to a body of research demonstrating attention, emotional control, and other SR difficulties in children and adolescents with TBI in comparison with those with orthopedic injury and healthy controls. 2,3,6,27,30,38,61,62 These cool and hot SR difficulties have significant implications for everyday functioning and predict social, academic, and adaptive behavioral performance across home, school, and community settings, 2,63 and predict lower educational outcomes. 64 Similarly, problems with attention and emotional control in uninjured children and adolescents create clear barriers to academic achievement, and put subjects at risk for negative outcomes in adulthood, including lower graduation rates, substance use, and sexual risk taking. 65 –67 Further, a recent review of intervention following pediatric acquired brain injury reported greater effects occurred when specific types of executive functioning were targeted, 68 rather than cool and hot SR targeted together, consistent with our differential findings in these domains.
Age and sex effects on white matter and cool and hot self-regulation
Frontostriatal pathway integrity did not interact with age or sex to influence SR outcomes. Contrary to expectations and prior research on normal development and DTI in children an adolescents with TBI, 35,69 main effects of age were not demonstrated for white matter FA. The latter study found robust age effects in school-age children but not adolescents for several pathways; however, pathway changes were assessed over 2 years, and the study used a younger sample with fewer children with mTBI. Therefore, age effects may be more salient in samples containing younger children with more severe injury. Considering the mediational analyses that combined behavioral and imaging data, the current study included a smaller DTI sample overall, used tractography, and examined different pathways. Future work with larger samples across wider age ranges and longitudinal spans may clarify the trajectory of frontostriatal pathway development using more specific indices of myelination, axonal packing, and tract coherence, 70 as well as the impact of different types of injury on pathway microstructure.
Interestingly, boys across groups demonstrated lower white matter FA than girls along dorsal pathways; differences that were not attributable to age or pubertal stage of development. This falls in line with recent work on typically developing children, 71,72 which demonstrated that males had later maturation of white matter than females, including lower whole brain FA and more protracted white matter development in frontal regions involved in cognitive control. 69,73 Overall, findings support past work showing that sex and age effects in injured and uninjured children play a role in white matter and behavioral functioning, respectively. Together, findings suggest potential sex differences across development of frontostriatal circuitry.
In relation to behavioral outcomes, older participants across groups showed signs of greater risk-taking, and younger children had more difficulty with focused and sustained attention. This is consistent with what is known about developmental improvement in attention and executive functioning capacity across childhood. 74 –76 In contrast, greater risk taking demonstrated in older participants follows the U-shaped slope of reward-seeking and risky behaviors illustrated across development, as risk taking and impulsivity increase from early childhood to middle adolescence. 10,77,78 Although sex differences were identified in frontostriatal circuitry in the current study, behavioral measures of SR did not vary in boys and girls.
White matter integrity predicted selected self-regulation outcomes
Dorsal frontostriatal white matter integrity 2 months post-TBI accounted for changes in the relationship between group and cool SR task performance at 7 months (Fig. 2 and b). Worse focused attention was mediated by lower FA of the right dACC to caudate in subjects with more severe TBI and of bilateral VLPFC to caudate in subjects with uncomplicated mild TBI. In sum, findings support prior work showing reduced integrity and overall microstructural differences in frontostriatal regions relating to attentional and cognitive control outcomes post-TBI, including frontal white matter, cingulum bundle, 37,79 caudate, and ventral striatum. 8 In contrast, FA of mOFC to nucleus accumbens DLPFC to caudate FA tracts failed to mediate the relationship of group to risk taking and emotional control, respectively, despite correlations between pathways and outcomes. Potential mediation findings were likely precluded by FA not varying by group in those model pathways. Indeed, recent work has suggested that cool executive functioning relies on dorsal regions, whereas hot executive functioning may rely on both dorsal and ventral regions. 80
Limitations and future research
The current study is not without limitations. Sample sizes likely restricted the power of multivariate and meditational analyses. Future work with tighter age bands and larger samples may be better able to stratify and examine age or pubertal stage relations along with brain-behavior outcomes following TBI. The constructs of cool and hot SR encompass broad sets of cognitive and emotional capacities; therefore, future work can further refine constructs and expand on measures used to assess different domains. Our study did not examine the contribution of other risk factors for SR difficulties, such as sleep disturbances, 81 which are common following TBI 82 and may significantly influence SR in everyday contexts. We used DTT to specifically evaluate frontostriatal pathway FA. Future work might also incorporate novel structural imaging methods such as graph theory, which use a network approach to examinations of brain–behavior relations and high-definition fiber tracking that may better characterize microstructural indices of myelination, axonal packing, and communication efficiency. 70,83 –85 This would allow delineation of microstructural changes related to injury and better characterize how key factors, such as age and sex, influence pathway development and link to behavioral outcomes in healthy children and adolescents and in those with TBI.
Conclusion
The current study advances knowledge of frontostriatal relations with behavioral outcomes and provides clinical implications by longitudinally linking post-acute compromised white matter microstructure to worse attention and risk taking 7 months after TBI. Results support findings that post-acute frontostriatal white matter integrity predicts chronic behavioral outcomes in children and adolescents with TBI 8,79 and may inform brain–behavior relations for uninjured populations. For example, frontostriatal structures and white matter connections between them are centrally involved in SR difficulties associated with ADHD 11 –13,86 and social functioning. 87 Considering the prominent role of frontostriatal circuitry in children and adolescents with TBI, ADHD, and other acquired and neurodevelopmental disorders, 88 this growing line of research may guide pharmacological 89,90 or behavioral treatment 68 by highlighting potential biomarkers for those most likely to respond or those most at risk. In future studies, interventions targeting SR may enhance white matter microstructural changes in associated pathways of interest. 91
Findings from this investigation demonstrated that lower FA in specific frontostriatal pathways was associated with differences in cool and hot SR following pediatric TBI. Dorsal pathways were more vulnerable to disruption than ventral frontostriatal pathways after more severe TBI, and dorsal pathway integrity predicted later attention performance. Educators and clinicians have key opportunities to screen for worsening attention and emotional control difficulties in the year following pediatric TBI, as well as to tailor interventions to target specific cool and hot SR problems. 68 More broadly, an enriched understanding of frontostriatal brain–behavior relations will inform future research and can lead to improved intervention for children and adolescents with both developmental and acquired neurological disorders.
Footnotes
Acknowledgments
We thank the children and families who participated in this study. We also thank the research team at the Children's Learning Institute that was responsible for data collection, including Gerardo Duque, Leticia Gomez, Denise Orellana, and Elizabeth Stamps.
Funding Information
This work was funded in part by National Institutes of Health R01 NS046308. The content is solely the responsibility of the authors and does not necessarily represent the official views of the granting institute.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.