
Abstract
Clinical trials have shown that intravenous albumin and decompressive craniectomy to treat early refractory intracranial hypertension can cause harm in patients with severe traumatic brain injury (TBI). The extent to which these treatments remain in use is unknown. We conducted a multi-center retrospective cohort study of adult patients with severe TBI admitted to five neurotrauma centers across Australia between April 2013 and March 2015. Patients were identified from local trauma and intensive care unit (ICU) registries and followed until hospital discharge. Main outcome measures were the administration of intravenous albumin, and decompressive craniectomy for intracranial hypertension. Analyses were predominantly descriptive. There were 303 patients with severe TBI, of whom a minority received albumin (6.9%) or underwent early decompressive craniectomy for treatment of refractory intracranial hypertension complicating diffuse TBI (2.3%). The median (intequartile range [IQR]) age was 35 (24, 58), and most injuries were caused by road traffic accidents (57.4%) or falls (25.1%). Overall, 34.3% of patients died while in the hospital and the remainder were discharged to rehabilitation (44.6%), other health care facilities (4.6%), or home (16.5%). There were no patient characteristics significantly associated with use of albumin or craniectomy. Intravenous albumin and craniectomy for treatment of intracranial hypertension were used infrequently in Australian neurotrauma centers, indicating alignment between best available evidence and practice.
Introduction
Severe traumatic brain injury (TBI) is a global public health problem with considerable socioeconomic impact. Worldwide the incidence of severe TBI is estimated to be 73 cases per 100,000 population, or a total of 5.48 million people per year. 1 Outcomes remain poor, with more than 50% dying or suffering long-term severe disability; a minority survive to live independently, and a small proportion return to work. 2 The direct and indirect lifetime costs for all TBI are estimated to be $400 billion annually. 3
Effective treatments to improve survival and functional recovery remain elusive. 4 High-quality randomized controlled trials (RCTs) have been conducted of a variety of interventions in TBI including steroids, fluid resuscitation, erythrocyte-stimulating agents, therapeutic hypothermia, and decompressive craniectomy. 5 –12 Among these trials, the Saline versus Albumin Fluid Evaluation Traumatic Brain Injury (SAFE TBI) and Decompressive Craniectomy in Diffuse Traumatic Brain Injury (DECRA) studies found significant differences in outcomes between the interventions and the alternative standard therapies. In SAFE TBI, the administration of intravenous 4% albumin when compared with saline in severe TBI led to increased mortality at 24 months (42% in patients receiving albumin vs. 22% in patients receiving saline). 11 In DECRA, among patients randomized to early surgical craniectomy for treatment of intracranial hypertension complicating diffuse TBI 30% had favorable functional outcomes (as measured by the Glasgow Outcome Scale-Extended [GOS-E]) at 6 months, compared with 49% of those receiving medical management. 8 These trials represent a high level of evidence to clinicians to guide the management of their patients with severe TBI. Further, the findings have been confirmed in systematic reviews and incorporated into international clinical practice guidelines. 13 –16
Cohort studies have not shown improvements in outcomes following severe TBI since publication of these trials. 17,18 Previous Australian and international studies in critical care, trauma, and other disciplines have shown that even high-level evidence frequently fails to translate into practice, 19,20 meaning patients are not benefiting from available research knowledge. Such failures of implementation have been associated with worse outcomes. 21 Since their publication there have been no studies examining the impact of the SAFE TBI and DECRA trials on practice; therefore, we undertook a retrospective cohort study of patients with severe TBI admitted to neurotrauma hospitals in Australia.
Methods
Study design
We undertook a retrospective cohort study at five major trauma teaching hospitals across Australia. Eligible hospitals were those that provided comprehensive neurosurgical services and contributed to institutional or state-wide trauma registries. Human research ethics approval was granted by Monash University and the local institutional ethics committees, with a waiver of patient consent.
Sequential patients with severe TBI aged 15 years or older were included if they were admitted to a participating hospital between April 2013 and March 2015 (2 years after publication of the DECRA trial, and 6 years after SAFE TBI). The main outcomes of interest were the administration of intravenous albumin and use of surgical craniectomy in their early management, and hospital outcomes.
Patients were identified from local trauma and intensive care registries using a combination of the Abbreviated Injury Scale (AIS)-head and pre-intubation Glasgow Coma Scale (GCS). Ambulance and hospital records, including fluid orders, intensive care unit (ICU) observation charts, and surgical reports were reviewed and data were collected by local hospital research personnel using REDCap (Research Electronic Data Capture) tools hosted at the Alfred Hospital. 22 Data were checked using encoded rules at time of entry with subsequent queries referred back to data collectors. In cases where data were missing no assumptions have been made and results are presented as a percentage of available data, expressed as % (n/N).
Data extracted included demographics, brain injury mechanism and severity, pre-hospital occurrence of secondary insults (hypoxia and hypotension), pre-hospital GCS score, and pre- and in-hospital therapies including details of the use of albumin or craniectomy surgery and their reported indications. Craniectomy was defined as intracranial surgery without replacement of the skull bone flap. Pre-surgery computed tomography (CT) Marshall classifications were reported by local institutional radiologists for patients who underwent craniectomy. Due to variability in treatment thresholds and measurement standards, whether surgery was indicated for treatment of intracranial hypertension was decided by site investigators' review of medical records. Lengths of stay and hospital outcome data were obtained from hospital records, and for patients managed in Victoria 12-month functional neurological outcomes in the form of the GOS-E were obtained from the Victorian State Trauma Registry (VSTR), a prospectively collected, population-based trauma registry.
Statistical analysis
Categorical data are presented as numbers and proportions (%); continuous data are presented as mean (± standard deviation) for normally distributed data, and median (interquartile range [IQR]) for skewed data.
To identify those to whom the DECRA trial results should apply, patients were classified according to whether intracranial mass lesions were present, or in diffuse injury whether decompressive craniectomy was performed for pre-emptive life-saving decompression, for treatment of early refractory intracranial hypertension (within 72 h of injury, as in DECRA), or as rescue therapy for intracranial hypertension (after 72 h). The SAFE TBI results were considered to apply to all patients in an ICU with severe TBI up to 14 days after injury.
Multi-variable logistic regression analyses were planned to explore possible associations between patient characteristics (age, GCS score, pupil responses, and CT appearances) and albumin infusion or use of decompressive craniectomy for intracranial hypertension.
The 12-month functional outcomes for patients in Victoria were analyzed to ensure consistency with previous cohort studies of patients with TBI.
All statistical analyses were performed using Stata version 16.0 (StataCorp LLC, TX, USA).
Results
Of seven major trauma centers invited to participate, five contributed data for a total of 303 patients (Supplementary Table S1). All sites were located in capital cities of Australian states.
Figure 1 shows grouping of patients by use of albumin or craniectomy, and indications.
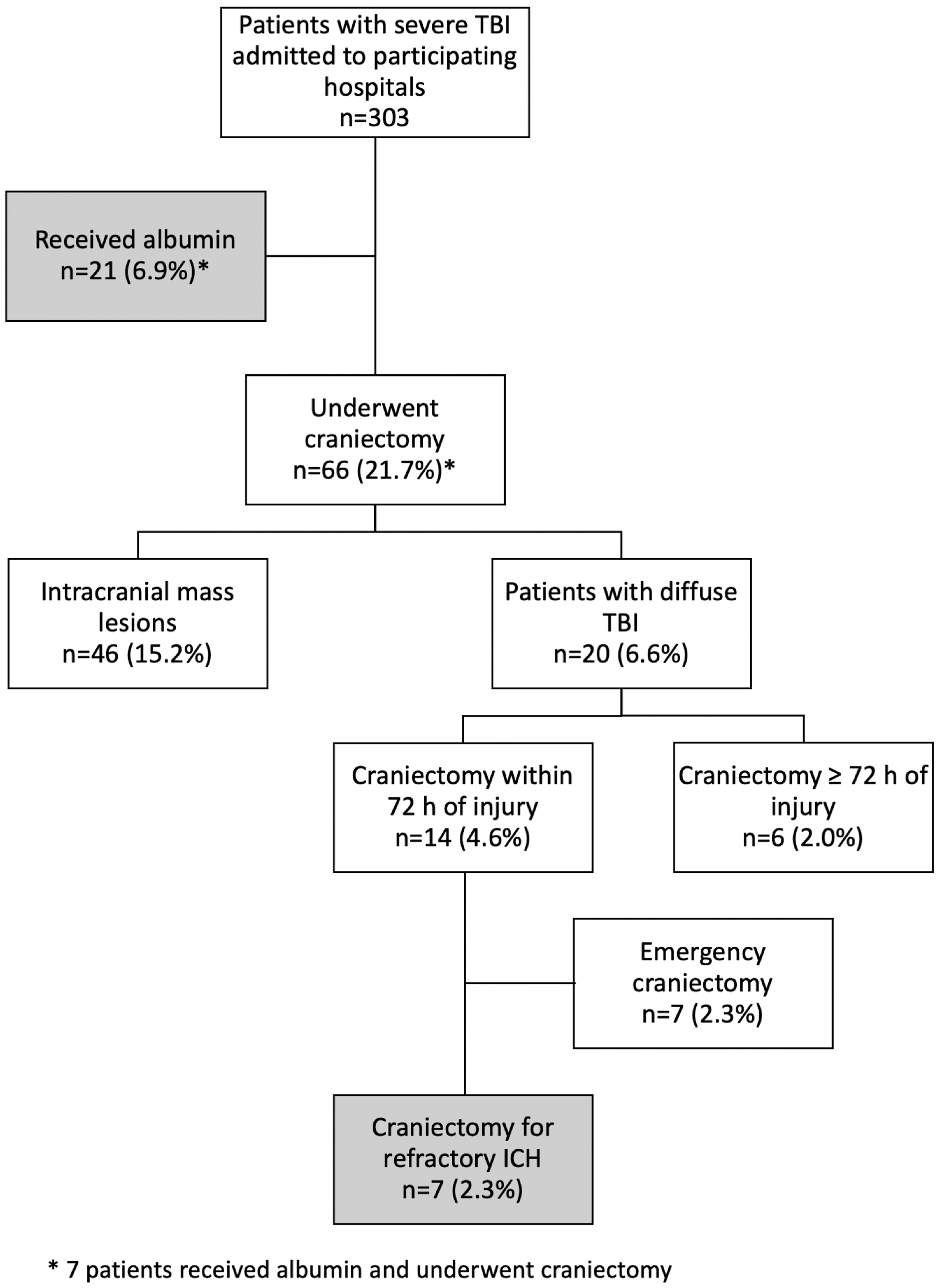
Distribution of patients. ICH, intracranial hypertension; TBI, traumatic brain injury.
Patient characteristics
The demographic, mechanism of injury, and injury severity characteristics were similar between groups (Table 2). The median age was 35 (24, 58) years; most patients were male (76.9%). The main causes of injury were road traffic accidents (57.3%) followed by falls (25.1%); vehicle crashes were more frequent in those who received albumin. Median GCS score was 5 (3, 7). One or both pupils were unreactive in 35.3%. Pre-hospital secondary insults were recorded in 33.0%. Intracranial mass lesions (Marshall classification 5–6) were present in 40.0% (26 of 66) when reported by site radiologists; an additional 20 patients underwent evacuation of lesions. Twenty-one patients (6.9%) received albumin, whereas 66 (21.8%) underwent craniectomy; 7 patients (2.3%) received both interventions.
Patient Characteristics
Seven patients received albumin and underwent craniectomy.
Median Glasgow Coma Scale (GCS) motor score was inconsistently reported except in one jurisdiction; however, the median motor of 2 (1, 4) was unchanged with exclusion of other jurisdictions indicating similar patient characteristics.
Computed tomography (CT) appearances are reported for 65 patients who underwent craniectomy; appearances were not available for 1 patient. The Marshall classification of CT abnormalities in brain trauma ranges from 1 to 6: a score of 1 indicates normal findings, 2 diffuse injury, 3 or 4 radiologic signs of increased intracranial pressure, and 5 or 6 an intracranial mass lesion. The first CT scan was categorized for each patient. Patients who had surgery to evacuate a hematoma <24 h after injury but whose first CT was conducted before surgery were classified as having a Marshall score of 5.
IQR, interquartile range.
Albumin Administration
Five patients received more than one episode of albumin administration; a total 29 episodes were reported.
In some cases more than one indication was reported.
CPP, cerebral perfusion pressure; ICU, intensive care unit; IQR, interquartile range.
Processes of care are shown in Supplementary Table S2. A minority of patients underwent craniotomy (bone flap replaced during surgery) for mass lesion evacuation (19.1%), or received barbiturate infusions (3.8%) or therapeutic hypothermia (7.9%) for intracranial hypertension. One-third of patients (34.3%) died in the hospital; most survivors were discharged to rehabilitation (44.6% overall), and the remainder to home (16.5%) or another health care facility (4.6%). At 12 months, three of four patients (73%) whose data were available in VSTR were dead or had severe disability (GOS-E score 1–4); and just under 10% had a good recovery (GOS-E score 7–8; Supplementary Fig. S1). The small patient numbers precluded presentation of GOS-E by subgroup.
Use of albumin
Twenty-one patients (6.9%) received intravenous albumin (Table 2). Albumin was administered in the operating theater (n = 8) and ICU (n = 13) and was prescribed by doctors of all seniority. Five patients received more than one episode of albumin resuscitation in the ICU: two patients in two discrete episodes, and three patients in three episodes. No patients received albumin pre-hospital or in the emergency department. Median time to first administration was 14.5 h, and volumes corresponded to the sizes of the available bottles (i.e., multiples of 500 mL). In most cases the indication for administration was not discoverable retrospectively; the most commonly reported indication was hypotension (47.6%). Length of stay in the ICU was longer for surviving patients who received albumin, and a greater proportion of those who received albumin infusions died in the hospital (47.6% vs. 33.3%).
Use of craniectomy
The use of craniectomy is described in Table 3. Of patients with diffuse injury, 7 (2.3%) underwent decompressive craniectomy for refractory intracranial hypertension within 72 h of injury (the eligibility criteria for the DECRA trial). A further 7 underwent “emergency” decompression prior to placement of intracranial pressure monitoring, ICU admission, or mechanical or pharmaceutical attempts to lower intracranial pressure, and another 6 patients with diffuse injury underwent “rescue” procedures at 72 h or more. Bilateral surgery (either bifrontal or bitemporal) was used in a majority of craniectomies performed for refractory intracranial hypertension. The remaining 46 patients (69.7%) who underwent craniectomy had mass lesions (either a radiologist-scored Marshall classification of 5–6, or neurosurgical opinion), of whom most underwent unitemporal craniectomy (89.1%). Median lengths of stay in the ICU and hospital for survivors varied between groups according to indications for craniectomy. The highest hospital mortality was observed in patients undergoing emergency craniectomy (57.1%).
Characteristics of Patients Undergoing Craniectomy
Early hypothermia was undertaken in some patients as part of a concurrent clinical trial.
CSF, cerebrospinal fluid; ICU, intensive care unit; IQR, interquartile range.
Factors associated with use of albumin and craniectomy
The small numbers of patients who received albumin or underwent craniectomy for intracranial hypertension precluded multi-variable analyses looking for associations with patient or site characteristics. Exploratory univariable analyses are presented in Supplementary Table S3. There were no characteristics significantly associated with the use of craniectomy or administration of albumin, and practice appeared similar between sites.
Discussion
Key findings
In this multi-center, observational cohort study of early management of severe TBI in multiple jurisdictions around Australia we observed low proportions of patients receiving therapies demonstrated in randomized trials to cause harm. These findings suggest that choice of resuscitation fluid and use of decompressive craniectomy for intracranial hypertension within these neurotrauma centers is highly consistent with the evidence generated by their encompassing clinical trial network.
Comparison with previous studies
Patient characteristics
Most patients included in this study would have been eligible for SAFE TBI. Many fewer would have been eligible for the DECRA trial as that trial restricted enrollment to a specific group of TBI patients with diffuse injury, and early intracranial hypertension. Demographic and clinical characteristics were similar to both trial populations, with the exceptions that median age was 32 years in our cohort of patients who underwent craniectomy versus 24 years in patients in DECRA (which excluded patients 60 and older), and the median GCS score was 5 in our cohort versus 7 in patients in SAFE TBI (which included both moderate and severe TBI).
Further, the characteristics of patients included in this study were consistent with other observational cohorts of severe TBI and therefore likely represent the spectrum of hospitalized patients with severe TBI. A longitudinal, population-based registry study conducted between 2006 and 2015 in Australia reported demographics, mechanisms, and severity of injury similar to those in our study (median age 41.5; male 72.5%; traffic accident as cause 49.0%); functional outcomes were also equivalent. 17
Use of albumin
Although intravenous fluid resuscitation is universally administered to hypovolemic patients following major trauma, few other studies have reported types of fluid used in patients with TBI. One exception was a recent international multi-center trial of early hypothermia for severe TBI, conducted from 2010 to 2017 (commencing 3 years after publication of SAFE TBI) in which the use of albumin infusions in the 10 days following injury was comparably infrequent (8.6% vs. 6.9% in our study). 7
Comparing these data with the available pre-SAFE TBI data suggests there has been a reduction in the use of colloid-containing fluids including albumin in patients with TBI. In 2000, sizeable proportions of Australian and New Zealand patients received colloid fluids in the pre-hospital (22.7%) and emergency department (39.1%) setting, 23 compared with our findings of exclusive use of crystalloid and blood. In a cross-sectional study of all ICU fluid resuscitation in 25 countries conducted in 2007 (prior to publication of SAFE TBI) 58% of patients admitted with TBI received colloid; among all patients albumin was used in 30% of colloid resuscitation episodes. 24 Overall, use of colloids in Australia and New Zealand in the intervening period has elsewhere been noted to have decreased in response to SAFE TBI and other non-TBI randomized controlled trials (RCTs), 25,26 whereas in the 5-year period prior to publication of SAFE TBI overall albumin use appeared static in Australia, New Zealand, Canada, and northern Europe. 27
Use of craniectomy
No studies published since DECRA have reported the incidence of refractory intracranial hypertension in patients with severe TBI or the proportions of patients undergoing decompressive craniectomy. In the DECRA trial (conducted between 2003 and 2010, published in 2011), 4.5% of screened patients with severe TBI (155 of 3478) had developed intracranial hypertension refractory to medical therapies within 72 h and were therefore eligible for enrollment and early craniectomy. The results of the RESCUEicp trial (published in 2016, after our study period) are difficult to compare due to different screening and eligibility criteria (unlike DECRA, patients with traumatic mass lesions were included). 9
Other historical data suggest there was an increase in use of craniectomy for intracranial hypertension prior to publication of DECRA. Between 1995 and 2005 several non-randomized studies supported its use. 28,29 Observational studies in the United States and Australia reported craniectomy for refractory intracranial hypertension in 4.1% of patients between 2000 and 2004, 30 and 8.2% between 2004 and 2008. 31 By comparison, our study (2013–2015) found early decompressive craniectomy for intracranial hypertension used in only 2.3% of patients (7 of 303), consistent with a change in practice in Australian neurotrauma centers following publication of the DECRA results.
Comparison with studies of translation
Several studies have examined adherence to neurotrauma guidelines. Recent systematic reviews found that across jurisdictions (not including Australia) the median observed adherence to the Brain Trauma Foundation guidelines for general management of TBI was 61%, with an apparent improvement between 1997 (40%) and 2007 (60%) but no improvement since. 32 Median adherence rates ranged from 0 to 100% with greater variability in low-income countries, and improved adherence was associated with guidelines based on higher levels of evidence. Our data on two individual practices compare favorably with these previous studies, for reasons that require further examination.
Clinical trial networks and translation
It is plausible that evidence may translate into practice more efficiently within clinical trial networks, which are made up of teaching hospitals employing key opinion leaders. 33 In contrast to our findings of low proportions of patients receiving albumin or undergoing decompressive craniectomy in centers that participate in the Australian and New Zealand Intensive Care Society Clinical Trials Group (ANZICS CTG) network, which undertook the SAFE TBI and DECRA studies, in recent surveys of European neurotrauma centers 23% of neurocritical care staff reported they would consider the use of albumin-containing fluids in patients with TBI, and 47% considered craniectomy as “general policy” for the treatment of refractory intracranial hypertension. 34,35 The centers involved were variably located in higher- and low-income countries and were not part of established clinical trial networks.
Other studies have examined de-adoption of individual practices found to be harmful. An interrupted time series analysis conducted in 195 American ICUs found that de-adoption of tight glycemic control was more likely to occur in teaching facilities relative to other sites in the years following publication of definitive evidence showing harm. 36 Allowing for methodological differences, our findings appear consistent with a greater alignment of practice with evidence within the ANZICS CTG member institutions.
Association with outcomes
Although a low proportion of patients received interventions shown to be harmful, outcomes in Australia do not appear to have improved over a period that encompasses publication of SAFE TBI and DECRA, and data collection for our study. 17 Possible explanations include a change in patient characteristics, such as increasing age, which may have masked improvements in outcomes that would otherwise be expected with improved quality of care. 17 Alternatively, although we accounted for different indications for craniectomy, it is possible that the proportions of patients with mass lesions and diffuse injury has changed resulting in fewer patients being eligible for this intervention.
Strengths and limitations
This study is among the largest longitudinal cohort studies conducted to date of the acute management of patients with severe TBI, and one of the few to assess adherence to discreet elements of the neurotrauma evidence base. We captured all patients hospitalized in neurotrauma centers from jurisdictions representing most of the Australian population, providing data that are more reflective of the broader population than that reported in RCTs. The collection of granular individual patient data including radiology, and emergency department and pre-ICU management, allowed precise description of care processes, complications, and indications for interventions received. Given the complex, overlapping indications for craniectomy following TBI, this approach was essential to identifying a cohort of patients to whom the evidence should apply.
Limitations relating to data availability should be considered. The effect of the SAFE TBI and DECRA studies on clinical practice would be more clearly distinguishable by interrupted time series analysis; however, data as detailed as ours are no longer available for the period prior to publication of these studies. Our data pre-dates the publication of a subsequent large trial of decompressive craniectomy for intracranial hypertension, but this trial provides further opportunity for evaluation of ongoing translation, currently underway. Additionally, we chose not to record intracranial pressure measurements because these are invariably confounded by treatments received, the thresholds for treatment of intracranial hypertension remain poorly defined, and the focus of our study was the choices of therapies. Finally, some potential confounders were not recorded including frailty scores, any advanced care directives, substitute decision making, and timing of withdrawal of life-sustaining therapy. These factors are important considerations for clinicians when judging appropriateness of aggressive therapies that have the potential to generate more survivors with a greater burden of disability.
Conclusion
In neurotrauma centers from a clinical trials network within a high-income country, two interventions reported to cause harm are infrequently used in patients with severe TBI. Use of these interventions appears to be lower compared with studies conducted prior to publication of the trials reporting their potential for harm. Clinical trial networks may support more rapid translation of research findings into clinical practice, but the key drivers of alignment of practice with evidence remain unclear. Exploring factors responsible for high levels of translation can inform implementation efforts in these and other treatment areas.
Footnotes
Acknowledgments
The Victorian State Trauma Registry (VSTR) is a Department of Health and Human Services, State Government of Victoria and Transport Accident Commission funded project. We thank the Victorian State Trauma Outcome Registry and Monitoring (VSTORM) group for the provision of VSTR data.
Site research coordinators: Alfred Hospital: Shirley Vallance, Emma Martin; Royal North Shore Hospital: Elizabeth Yarad, Anne O'Connor, Naomi Hammond, Frances Bass; St. George Hospital: Jennene Miller, Deborah Inskip; Royal Perth Hospital: Sharon Waterson; Royal Brisbane and Women's Hospital: Paul Jarrett.
Funding Information
This study was supported by a fellowship grant (N-M-12-036) provided to D.G. by the Centre of Excellence in Traumatic Brain Injury Research at the National Trauma Research Institute, Victoria, Australia.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.