
Abstract
Sleep disturbances are commonly reported in children with persistent post-concussion symptoms (PPCS). Melatonin treatment is often recommended, yet supporting evidence is scarce. We aimed to evaluate the efficacy of treatment with melatonin for sleep disturbance in youth with PPCS following mild traumatic brain injury (mTBI). This article is a secondary analysis of a clinical trial of melatonin compared with placebo to treat PPCS. Youth (8–18 years of age) with PPCS and significant sleep-related problems (SRPs) at 4–6 weeks post-injury were eligible. Exclusion criteria: significant medical/psychiatric history; previous concussion/mTBI within 3 months. Treatment groups were: placebo, melatonin 3 mg, or melatonin 10 mg. Primary outcome was change in SRPs measured using the Post-Concussion Symptom Inventory (PCSI) after 2 weeks of treatment. Secondary outcomes included change in actigraphy sleep efficiency, duration, onset latency, and wake-after-sleep-onset. Behavior was measured using Behaviour Assessment for Children (2nd edition). Seventy-two participants (mean age 14.0, standard deviation [SD] = 2.6) years; 60% female) with PPCS and significant sleep disturbance were included in the secondary analysis: placebo (n = 22); melatonin 3 mg (n = 25); melatonin 10 mg (n = 25). Sixty-four participants had actigraphy data. SRPs decreased across all groups over time with a significant effect of melatonin 3 mg (3.7; 95% confidence interval [CI]: 2.1, 5.4) compared with placebo (7.4; 95% CI: 4.2, 10.6) and melatonin 10 mg (6.4; 95% CI: 3.6, 9.2). Sleep duration increased in the melatonin 3 mg (43 min; 95% CI: 6, 93) and melatonin 10 mg groups (55 min; 95% CI: 5, 104) compared with placebo. A per protocol analysis demonstrated improved sleep efficiency in the melatonin 10 mg group (p = 0.029). No serious adverse events were reported. Depressive symptoms significantly decreased with melatonin 3 mg (-4.7; 95% CI: −9.2, −.2) but not with melatonin 10 mg (−1.4, 95% CI: −5.9, 3.2) treatment compared with placebo. Changes in cognition or behavior were otherwise not significantly different between treatment groups. Short-term melatonin is a well-tolerated treatment for sleep disturbance in youth with PPCS following mTBI. In this context, it may also be associated with a reduction in depressive symptoms.
Introduction
Over the last few years, sleep disturbance following mild traumatic brain injury (mTBI) has become increasingly recognized. 1 After mTBI, children and adolescents frequently complain of hypersomnia, insomnia, and fatigue, which may last months or even years after the injury. 2 –4 Sleep disturbance is associated with prolonged recovery, 5,6 and may have a significant impact on learning, mood, and health-related quality of life. 7 As this is a potentially modifiable factor, evidence-based treatments are badly needed. 8
Although the recent Centers for Disease Control (CDC) Guidelines highlight the lack of evidence for any sleep treatments following pediatric mTBI, 9 melatonin is often recommended for the management of sleep disturbance in the presence of persistent post-concussion symptoms (PPCS). 10,11 Melatonin plays a major role in the chronological regulation of the circadian sleep–wake cycle, 12 and is a recognized treatment for sleep disturbance, especially in children with neurodevelopmental disorders. 13 –15 Adults with sleep disturbance following severe TBI have been found to have lower melatonin production, which was associated with disturbances in slow wave sleep. 16 Treatment with melatonin improved both subjective and objective measures of sleep disturbance in this population. 17 The evidence for the use of melatonin for sleep disturbance in children with TBI is scarce; however, in a recent retrospective case series, 67% of children with mTBI and sleep disturbance reported a positive response to melatonin. 5
The current study aimed to evaluate the efficacy of melatonin (3 mg and 10 mg) on sleep-related problems and sleep behavior in youth with PPCS following mTBI in a secondary analysis of the PlayGame Trial. 18,19 We hypothesized that melatonin treatment would be associated with improvements in reported sleep-related problems (SRP) and objective parameters of sleep behavior in children with PPCS. A secondary aim was to explore whether cognition and behavior improved with melatonin treatment in children with PPCS and significant SRP.
Methods
Study design
The PlayGame Trial evaluated the efficacy of melatonin for the treatment of PPCS in youth in a single center double-blinded randomized controlled trial.
19
The trial was approved by local ethical and scientific review boards, and the study protocol, including secondary analyses, has been published previously.
18
Standards of good clinical practices were observed and the Consolidated Standards of Reporting Trials guidelines were followed including registration at
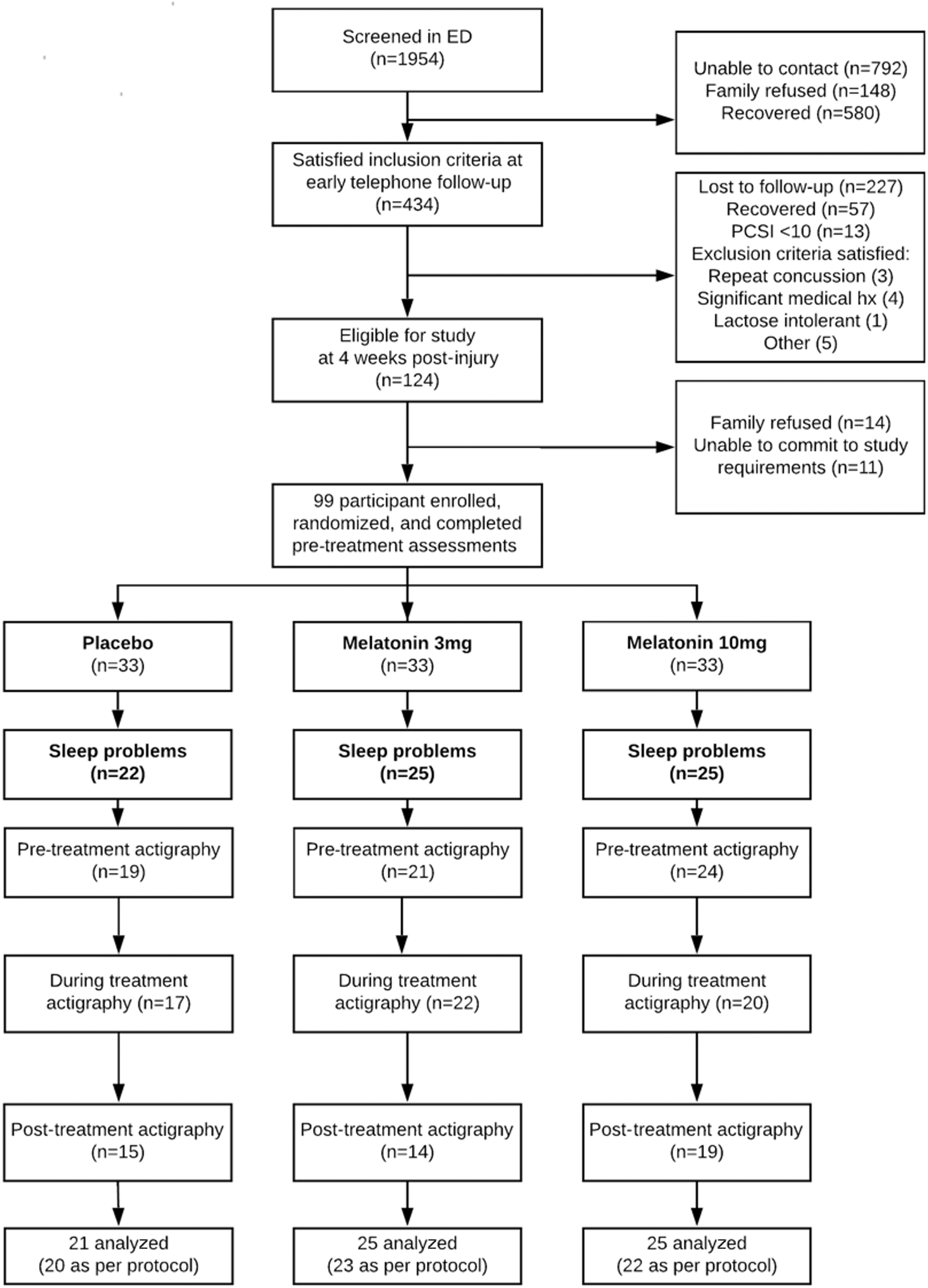
Trial details are demonstrated. A subgroup of participants with sleep disturbance was identified in each treatment group. Wrist actigraphy was performed before, during, and after treatment. Actigraphy was not performed in instances of watch malfunction, unavailability, or refusal.
Intervention
Participants were randomly assigned 1:1:1 to three groups: placebo, melatonin 3 mg, or melatonin 10 mg. Sustained-release sublingual melatonin preparations were used. The study drug was taken sublingually 1 h before night-time sleep for 28 days, and was continued even if symptom resolution occurred. No restrictions were placed on the use of other medications. Compliance and adverse events were monitored and rated weekly using a questionnaire and diary. Participants, parents, and assessors were blinded to treatment allocation. Participants were asked to avoid analgesic overuse, encouraged to undertake light exercise, avoid contact sports, and return gradually to school. Follow-up occurred weekly during treatment, at the end of treatment, and at 3–4 and 6 months post-injury.
Secondary analysis
Only participants with a significant increase in sleep disturbance were included in this study. This was calculated as the pre - post-injury change in the total PCSI sleep domain score. The change in total sleep score at 4–6 weeks post-injury was divided into tertiles. A significant increase in SRPs was considered as an increase in the total sleep score above the 1st tertile (i.e., ≥3). Given melatonin's short half-life and rapid onset of action, the primary outcome in this secondary analysis was the change in sleep-related problems and the secondary outcome was the change in sleep efficiency (measured using wrist actigraphy) during the first 2 weeks of treatment. 21 The trial details are demonstrated in Figure 1.
SRPs
To measure SRPs, the following questions on the validated PCSI were used: trouble falling asleep, sleeping more than usual, sleeping less than usual, drowsiness, and fatigue. 22,23 Each symptom was rated using a Guttmann scale, from 0 (not a problem) to 6 (almost always a problem). These five sleep-related questions were summed to obtain a PSCI “total sleep score” (maximum possible score of 30). Pre-injury scores were assessed retrospectively at trial enrollment. A pre- to post-injury change in the total sleep score of ≥3 was considered to represent a significant increase in SRP. Total sleep scores were assessed before treatment, weekly during treatment, at the end of treatment, 3 months after treatment, and 6 months post-injury.
Wrist actigraphy
Wrist actigraphy provides a valid measure of sleep–wake behavior and was collected using the Actiwatch-2 (Philips Respironics) worn continuously on the non-dominant wrist. 24 –26 The device was removed only when bathing. Data were collected for 5–7 days before treatment, during the 28 days of treatment (watch was recharged midway), and for 5–7 days following treatment. Epochs before and after treatment were set at 15 sec (e15). Epochs during treatment were set at 30 sec (e30) and sensitivity at medium (default setting: 40) to allow 14 days of continuous recording. Participants completed a sleep diary during the same period to document bedtime, sleep time, wake time, number and length of naps, watch removal, and medications used. Information from the sleep diary was used to corroborate the actigraphy data. 27 Periods of watch removal were detected using a non-wear algorithm (periods of no activity for >10 min), manual assessment and cross-referencing with the sleep diary and were excluded from the analysis. Actigraphy/sleep diary assessments and adjustments were made while blinded to study drug and were verified by a second researcher.
Actigraphy data were analyzed using the Respironics Actiware analysis software (version 6.0.2) to score epochs as either “sleep” or “awake.” Sleep onset latency (SOL, in minutes) is the time between start of bedtime rest interval to sleep start, which was the first consecutive series of immobile epochs lasting 10 min with no more than one epoch scored as active or awake. Duration of total sleep time (TST, period from sleep onset to sleep end), sleep efficiency (SE, ratio of sleep duration divided by total duration of sleep episode), SOL, and wake after sleep onset (WASO, total number of “awake” minutes between sleep onset and sleep end) were estimated. These parameters were averaged over pre-treatment assessment, during the first 14 days of treatment, the last 14 days, and for the week following treatment.
Melatonin levels
Participants were not receiving exogenous melatonin before treatment. Overnight urinary 6-sulphatoxymelatonin (aMT6s), the major metabolite of melatonin, was analyzed before treatment, mid-treatment, and after treatment. Urinary aMT6s excretion rates have been found to be a reliable reflection of both salivary and serum melatonin concentration. 28 After bedtime void, the subsequent first morning urine sample was collected and subsequently stored at −80°C once received. Analysis was performed observing Good Laboratory Practices at the Alberta Children's Hospital BioCORE facility using a solid phase enzyme-linked immunosorbent assay with a sensitivity of 1.0ng/mL (ELISA, IBL International, Cat#RE54031). Individual levels of urinary aMT6s were converted to a ratio normalized by using standard laboratory measurement of urinary creatinine concentration. 29,30
Cognition and behavior
Cognition and behavior were assessed immediately before and after treatment. The core CNS Vital Signs neurocognitive assessment battery consisting of seven cognitive tests was used to calculate a global domain score (Neurocognitive Index [NCI]). 31,32 The Behavioural Symptoms Index from the parent proxy version of the Behaviour Assessment System for Children, 2nd Edition (BASC-2) was used as a measure of an overall child behavior problems, and depression and anxiety indices were used to assess mood and anxiety. 33 Problems with daily executive ability were assessed using the Behaviour Rating Inventory of Executive Function (BRIEF, parent report) which has demonstrated validity in children and adolescents with TBI 33 –35 Here, there are eight clinical scales (inhibit, shift, emotional control, initiate, working memory, plan/organize, organization of materials, and monitor) which are used to provide two summary indices, Behavioural Regulation (three scales) and Meta-cognition (five scales), and a summary executive score (Global Executive Composite). The Test of Memory Malingering (TOMM) was administered as a proxy measure of performance validity. 36 Health-Related Quality of Life (HRQL) was assessed using the Child Health Questionnaire, Parent Report (CHQ-PF50). 37 Frequency and severity of bodily pain was assessed using the bodily pain category in the Child Health Questionnaire, Child Report (CHQ-CH87).
Statistical analysis
As this was a secondary analysis of a clinical trial, the sample size was pre-determined. The change in total sleep score at 4–6 weeks post-injury (compared with the pre-injury score) was divided into tertiles. In order to include participants with significant increases in SRPs, only those with an increase in their total sleep score above 1st tertile (i.e., ≥3) were considered in the analysis. Where normalcy assumptions were violated, group differences were analyzed using non-parametric tests (PCSI, SRP, number of previous concussions). Sleep efficiency is a percentage value and was negatively skewed and therefore transformed using log (100 minus efficiency). Onset latency and aMT6s levels were positively skewed and were normalized using a logarithmic transformation.
A random effects mixed-model analysis was used to model total sleep score as a function (negative binomial) of treatment groups (i.e., placebo, melatonin 3 mg, melatonin 10 mg) and time (1, 2, 3, 4 [end of treatment], 12, and 26 weeks) with participant entered as a random factor. Epochs were set at 15 sec before treatment and 30 sec during treatment, precluding the use of a repeated measure design; therefore, pre-treatment parameters were entered as a covariate to account for between-subject sleep behavior differences. Given the rapid onset of action of Melatonin, a random effects mixed-model actigraphy analysis was used to model transformed sleep efficiency (linear) during the first 2 weeks of treatment as a function of treatment groups, with participant entered as a random factor. Fixed factors were group, pre-treatment transformed sleep efficiency, age at injury, body mass index (BMI), and sex. Similar linear mixed-effect models were created to analyze transformed sleep onset latency, total sleep time, and wake after sleep onset as secondary analyses. Mixed linear model assumptions of normality of residuals, linearity, and homogeneity of variance were met. Post-hoc comparisons were corrected using the Scheffe test. Linear regression was used to analyze log aMT6s levels by group controlling for pre-treatment aMT6s level, age, sex and BMI. Exploratory mixed-model estimates of change in HRQL (CHQ-PF50), behavioral change (BASC-2, BRIEF), and NCI as a function of treatment group were performed with age and sex as fixed factors. Missing PCSI data were imputed using the last-observation-carried-forward approach (one participant per treatment group). Otherwise, all data at each time point were used in the mixed models. Statistical analyses were performed using SPSS (IBM SPSS Statistics for Mac, Version 25.0. Armonk, NY: IBM Corp.) and Stata Statistical software Release 15.
Results
Ninety-nine participants were enrolled in the study proper and randomly assigned to treatment groups (33 per group). Two participants withdrew after randomization without starting treatment, and three were lost to follow-up. Ninety-four participants completed assessments immediately after intervention, and 92 completed the trial according to protocol.
In this secondary analysis, 72 participants (mean age 14.0 years, standard deviation [SD] 2.6; 60% female) had sleep disturbance before treatment: placebo (n = 22); melatonin 3 mg (n = 25); and melatonin 10 mg (n = 25); see Figure 1. These participants did not differ significantly in mean age, sex, or average time seen post-injury (38 [SD 5.7] days) from participants without sleep disturbance. Nor did participants with and without sleep disturbances significantly differ on mean NCI, anxiety, depression, headache, or HRQL scores.
Demographic, clinical, and sleep details of the participants are reported in Table 1. The three groups were similar in age, sex, BMI, and family income. Pre-treatment subjective SRPs and objective sleep actigraphy parameters were similar among groups. Eleven participants (placebo, n = 4; melatonin 3 mg, n = 4; and melatonin 10 mg, n = 3) had BASC-2 anxiety scores in the clinically significant range (T-score ≥65). Six participants had BASC-2 depression scores in the clinically significant range (placebo, n = 2, melatonin 3 mg, n = 2, and melatonin 10 mg, n = 2). Mean physical HRQL (34, 95% CI: 31, 37) and psychosocial HRQL (40, 95% CI: 38, 44) were low across groups compared with normative values (mean 50, SD 10).
Demographic, Injury, and Clinical Details of Participants with Persistent Post-Concussion Symptoms and Sleep Disturbance
CI, confidence interval; CA$, Canadian dollar; MVA, motor vehicle accident; PCSI, Post Concussion Symptom Inventory; CNS, central nervous system; BASC-2, Behavioural Assessment for Children, 2nd edition; BRIEF, Behavior Rating Inventory of Executive Function; WASO, wake after sleep onset (min).
SRPs
Model-based estimates of mean total SRPs during treatment and follow-up are shown in Figure 2. Sleep-related problems decreased across all groups during treatment (Supplementary Table 1). There was no effect of age on SRP change (β = -0.01, p = 0.845) or sex (β = 0.26, p = 0.195). There was a significant effect of the melatonin 3 mg group (β = -0.51, p = 0.043), and a group by time interaction for the effect of melatonin 3 mg after 2 weeks of treatment, 95% CIs: −1.08, −0.03, p = 0.038.
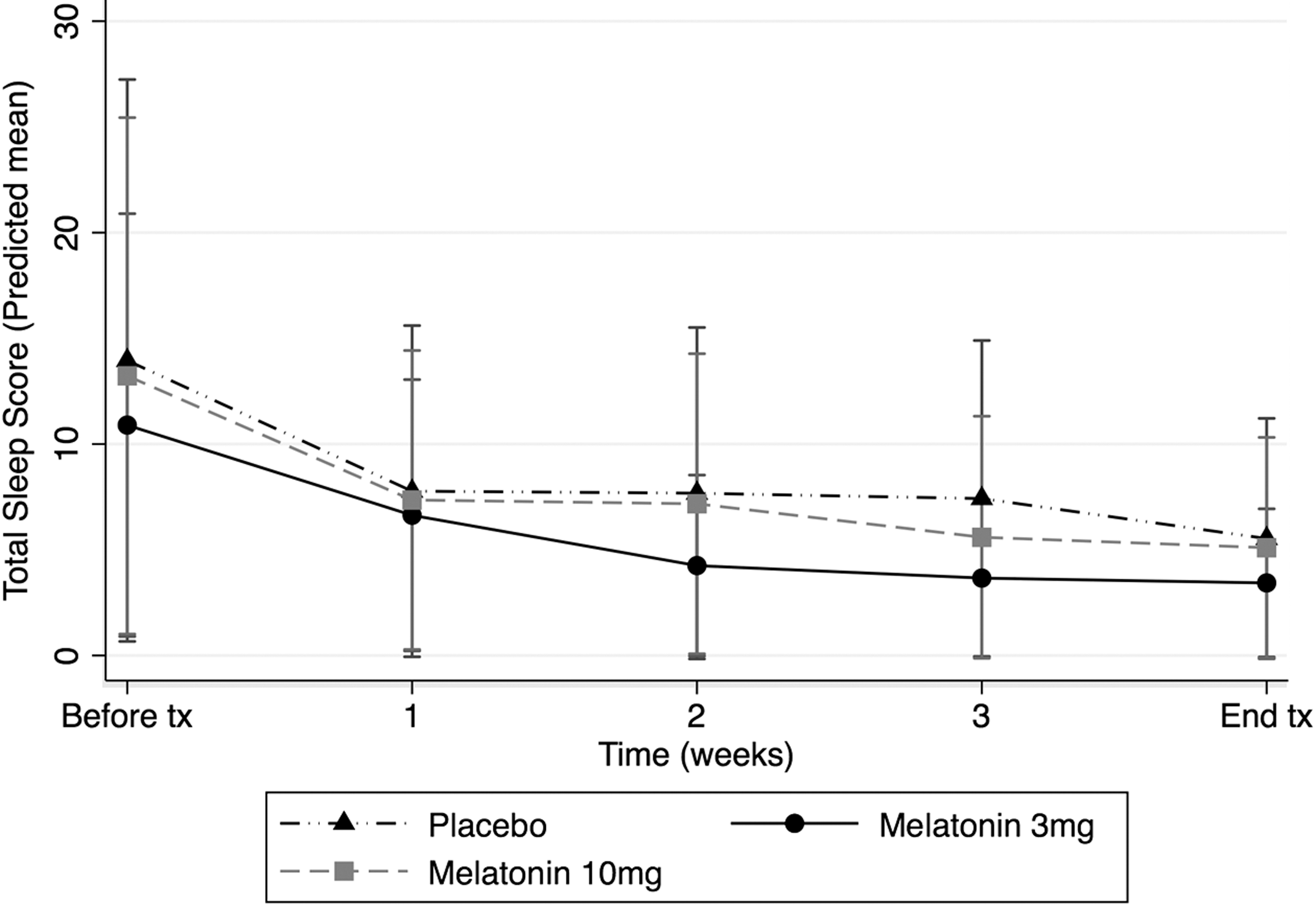
The change in model-based estimated mean total sleep scores over time by treatment group using a non-linear mixed effects model are demonstrated. Sleep-related problems decreased significantly at all time points in all groups (p < 0.01). There was a significant group × time interaction of melatonin 3 mg after 2 weeks of treatment (*β −0.55, p = 0.038).
Sleep activity
Sixty-four participants with increased post-injury SRP had both pre-treatment and on-treatment actigraphy data. Mixed-model analysis demonstrated no significant effect of treatment group on sleep efficiency, F(2,45) = 1.83, p = 0.171. There was a significant effect of treatment group on mean total sleep time, which was increased in both melatonin groups, F(2,45) = 4.04, p = 0.003: 43 min (95% CIs: 6, 93) in the melatonin 3 mg group and 55 min (95% CIs: 5, 104) in the melatonin 10 mg group. There was no effect of treatment group on sleep onset latency, F(2,30) = 0.52, p = 0.60, or WASO, F(2,45) = 0.05, p = 0.95.
Overnight melatonin levels
Overnight melatonin levels are reported in Figure 3 and Supplementary Table 2. Pre-treatment aMT6s levels (mean = 35; 95% CIs: 31, 74) were not significantly different among treatment groups (F[2,45] = 0.01, p = 0.91). Linear regression demonstrated significantly increased transformed mid-treatment aMT6s levels in both melatonin groups (β = 1.88, p < .0001) compared with placebo, F(4, 31) = 7.2, p < 0.001. Five participants chose to continue taking melatonin after the treatment period had ended and were excluded from the post-treatment analysis. After treatment, transformed urinary aMT6s did not differ from pre-treatment levels, paired t = 1.37, p = 0.18.

Overnight urinary melatonin levels (aMT6s, log ng/mg creatinine) before, during, and after treatment in children with persistent post-concussion symptoms and self-reported sleep disturbance. Melatonin levels increased in both melatonin treatment groups, F(4, 31) = 7.2, p < 0.001. After treatment, urinary aMT6s returned to pre-treatment levels.
Per protocol analysis
Six participants had significant protocol deviations (i.e., missed more than five doses of the study drug): placebo (n = 1), melatonin 3 mg (n = 2), melatonin 10 mg (n = 3). A per protocol analysis revealed a significant effect of group on sleep efficiency, F(2,40) = 3.88, p = 0.029 (see Table 2 and Fig. 4). Post-hoc pairwise comparisons revealed that the melatonin 10 mg group had increased sleep efficiency compared with placebo (p = 0.039). Mean total sleep time remained significantly increased in the melatonin groups: Melatonin 3 mg (59 min; 95% CIs: 11, 107) and melatonin 10 mg (70 min; 95% CIs: 22, 118). There was no effect of treatment group on sleep onset latency or wake-after-sleep onset. Changes in SRPs over time were similar to intention-to-treat analyses. Treatment group had no effect on bodily pain (β = -0.02, p = 0.82) or headache (KW[2,66] = 1.8, p = 0.40).
Mean Treatment Effect Estimates (Melatonin Minus Placebo) and Significance Levels from the Mixed Model Analyses
Variable was transformed log(100-efficiency).
Variable was log transformed.
Change assessed at the end of 28 days of treatment.
Bold indicates statistical significance.
WASO, wake-after-sleep-onset; PCSI, Post-Concussion Symptom Inventory; CNS Vital Signs NCI, Neurocognitive Index, Central Nervous System Vital Signs; BASC-2, Behaviour Assessment for Children, 2nd Edition, Parent Report; BSI, Behavior Symptoms Index; BRIEF, Behaviour Rating Inventory of Executive Function Global Executive Function.

A forest plot demonstrating the model-based mean treatment effect estimates of melatonin on sleep-related problems and objective sleep measures (using actigraphy). Melatonin 3 mg and 10 mg had a large significant effect on total sleep duration (p = 0.003). PCSI-Y, total post-treatment post-concussion symptom inventory score; WASO, wake-after-sleep-onset; + log(100-Sleep efficiency); # log(onset latency).
Exploratory analyses
In order to assess any secondary effects of improved sleep on cognition and behavior, exploratory mixed model analyses were performed (see Table 2 and Fig. 5). Mean estimates of treatment effect of melatonin were not significantly different than for placebo for change in non–sleep-related post-concussion symptoms (PCSI-Y), cognition (NCI), overall behavior (Behavior Symptoms Index [BSI]), or anxiety scores. Depression scores decreased significantly in those participants treated with melatonin 3 mg (−4.7; 95% CI: −9.2 to −.2) when compared with placebo. This was not found in the melatonin 10 mg group. There were no significant group differences in the changes in health-related quality of life indices (CHQ).

A forest plot demonstrating the results of exploratory analyses. The model-based mean treatment effect estimates of melatonin on neuropsychological outcome measures are demonstrated. Melatonin 3 mg had a significant effect on depression scores measured using the Behaviour Assessment System for Children, 2nd Edition (BASC-2) (p = 0.038). CNSVS NCI, Central Nervous System Vital Signs Neurocognitive Index; BRIEF, Behaviour Rating Inventory of Executive Function; CHQ, Child Health Questionnaire Parent Version.
Adverse events
Twenty-six participants reported minor adverse events, 16 of which had no impact on daily function (see Supplementary Table 3). There was no statistical difference in the frequency (χ 2 [2] = 1.5, p = 0.47) or severity (χ 2 [6] = 5.6, p = 0.47) of events among groups. Seven events were possibly related to the study drug (i.e., fatigue [n = 2], cognitive complaint, nausea, behavioral change, insomnia [n = 2]). One serious adverse event was recorded in the melatonin 10 mg group (appendicitis) which was not likely to have been related to the study drug.
Discussion
Melatonin improved sleep disturbance in children and adolescents with persistent post-concussion symptoms following mild TBI. SRPs decreased gradually during the study in all treatment groups, plateauing ∼4 months post-injury, which parallels the gradual resolution of PPCS seen over this time period. 19 The melatonin 3 mg group had significantly greater decreases in SRPs, although the effect size was small and was most marked after 2 weeks of treatment. Melatonin also improved the objective sleep-activity measures; total sleep time each night increased by ∼1 h in both melatonin groups, and sleep efficiency increased by 7% in the melatonin 10 mg group (after accounting for non-compliance). There was no effect of melatonin on sleep onset latency or wake-after-sleep-onset. The favorable response to melatonin occurred even though pre-treatment endogenous melatonin levels (54.6; 95% CIs: 46.5, 62.6) were similar between groups, and with age and sex-matched controls with similar sleep schedules. 38 Overall, these results support the use of melatonin for treating significant sleep disturbances in youth with PPCS.
Sleep disturbance is commonly reported by 30–70% of both adults and children across the spectrum of TBI. 39,40 The types of sleep problems are, however, heterogeneous, with insomnia, pleiosomnia, pre-sleep arousal, and circadian rhythm sleep disorders being among the commonest. 41 The type of problem frequently changes over time following the injury. Other sleep disorders, such as sleep-related breathing disorders and rapid eye movement (REM) sleep disorder, are not uncommon in adult chronic TBI. The etiologies are heterogeneous and often multifactorial. Following TBI, sleep problems have been associated with abnormalities in slow-wave sleep production, autonomic dysfunction, neuroinflammation, dysregulation of circadian hormones, and decreased melatonin production. 16,41,42 Their importance should not be underestimated given their impact on recovery, mood, and cognitive function as evidenced by the frequency of these comorbidities in TBI and particularly the associated risk of poor recovery following mTBI. 3,43
This is the first controlled trial to assess the efficacy of melatonin in sleep disturbance in children with PPCS following mTBI. Our results are supported by two earlier pediatric case series 5,44 and a recent clinical trial of melatonin to treat sleep disturbance in adults with moderate-to-severe TBI. 45 Although changes in SRPs achieved statistical significance in our study, the treatment effect on clinical symptoms was small. This could have been because of the insensitivity of the PCSI sleep subscale. The treatment effect, however, on objective sleep-activity parameters (total sleep duration and sleep efficiency) was considerable. Improved overall sleep disturbance in melatonin groups was not mirrored by improvements in other post-concussion symptoms, physical or psychosocial HRQL, or improvements in cognition. Exploratory analyses revealed that depression scores improved in the melatonin 3 mg group over the treatment period, but anxiety scores did not.
As the melatonin doses used in this study are higher than those used in adult TBI populations, this study supports the safety of using melatonin in pediatric populations, which is important, given the frequency of PPCS in childhood. 45 Melatonin production is higher in childhood and decreases later in life. 46,47 A dose of 3 mg was chosen to ensure saturation of melatonin receptors (MT1 and MT2) in the suprachiasmatic nucleus involved in sleep promotion. A 10 mg dose was chosen to reach the supraphysiological levels needed to achieve antioxidant and anti-inflammatory effects to target the complex molecular and pathophysiological processes that lead to secondary injury following TBI, and which may in turn lead to PPCS. 48,49 Despite using higher doses, we observed that melatonin was well tolerated; any side effects were mild and similar between groups, and no serious adverse events related to the study drug were encountered. This is similar to previous reports in the literature. 50 Overall, the 10 mg dose was not superior to 3 mg dose in our study. Although clinically safe, there are concerns that intermediate-term or long-term administration of melatonin may have unforeseen consequences, 51 including decreased endogenous melatonin production/response caused bby melatonin receptor desensitization. 52 We found no evidence of the latter after 28 days of treatment as melatonin levels post-treatment returned to pre-treatment levels.
This study has several limitations. First, we did not evaluate sleep-related problems with a validated pediatric sleep questionnaire. Instead, we used relevant questions from a concussion symptom questionnaire (PCSI), which evaluated the key areas of sleep concerns for our population (i.e., fatigue, drowsiness, trouble falling or staying asleep), but did not assess pre-sleep arousal symptoms. We also used retrospective recollection of pre-injury sleep-related symptoms at the time of enrollment, which could be subject to recall bias. 53 To decrease participant burden, we used parental reports of their child's HRQL and mood and anxiety levels which, although validated in pediatric mTBI, may not accurately reflect the child's mood. As this was a secondary analysis of a clinical trial to treat PPCS and not SRPs, a subgroup of participants with a change in sleep score ≥3 was examined to mimic the clinical scenario in which melatonin might be considered for sleep disturbance. This may have led to an underestimation of the effect of melatonin. Pre-treatment actigraphy was performed using 15 sec epochs, which can underestimate sleep behavior. Therefore, rather than using a repeated measure design, pre-treatment parameters were entered as a covariate to control for between-subject sleep behavior differences. Although the sample size was adequate overall, treatment groups had different sample sizes, which could decrease the power of our study, especially in the assessment of urinary melatonin levels. Overnight melatonin estimation by first void urine collection is an established methodology to assess endogenous melatonin production. We did not measure low-threshold dim-light melatonin onset time or how melatonin production changed during the night, and so cannot comment on changes in circadian melatonin production in our sample or how this might be affected by melatonin supplementation. 54
Although melatonin was effective in treating sleep disturbance and reducing depressive symptoms after mTBI, it did not improve other PPCS symptoms, pain, or anxiety. Other treatments for sleep disturbance have also shown promise in pediatric PPCS and adult TBI, such as cognitive behavioral therapy and ramelteon. 8,55 –57 Behavioral intervention is likely to be a more effective long-term strategy for those children in whom sleep disturbances persist, and may also improve non–sleep-related mood and behavioral problems seen in PPCS. 58 As melatonin may be synergistic with behavioral therapy, 14 future studies examining the use of melatonin in conjunction with cognitive behavioral therapy for sleep disturbance are warranted.
Conclusion
Melatonin is a safe and well-tolerated effective treatment for sleep disturbance in youth with persistent post-concussive symptoms following mTBI. It may also improve depressive symptoms associated with PPCS and sleep disturbance following mTBI.
Footnotes
Funding Information
All phases of the research were funded by Canadian Institutes of Health Research (CIHR) grant number 293375, the Alberta Children's Hospital Research Institute, and the University of Calgary (10006634). Dr. Barlow acknowledges funding from the Motor Accident Insurance Commission, Queensland, Australia (61278).
Author Disclosure Statement
Dr. Brooks previously received in-kind support (free test credits) from the publisher of a computerized cognitive test (CNS Vital Signs, Chapel Hill, North Carolina) for prior studies. The other authors have indicated they have no competing financial interests.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.