
Abstract
High-level spinal cord injury (SCI) can disrupt cardiovascular autonomic function. However, the evolution of cardiovascular autonomic function in the acute phase following injury is unknown. We evaluated the timing, severity, progression, and implications of cardiovascular autonomic injury following acute SCI. We tested 63 individuals with acute traumatic SCI (aged 48 ± 2 years) at five time-points: <2 weeks, and 1, 3, 6–12, and >12 months post-injury. Supine beat-to-beat systolic arterial pressure (SAP) and R-R interval (RRI) were recorded and low-frequency variability (LF SAP and LF RRI) determined. Cross-spectral analyses were used to determine baroreflex function (low frequency) and cardiorespiratory interactions (high frequency). Known electrocardiographic (ECG) markers for arrhythmia and self-reported symptoms of cardiovascular dysfunction were determined. Comparisons were made with historical data from individuals with chronic SCI and able-bodied controls. Most individuals had high-level (74%) motor/sensory incomplete (63%) lesions. All participants had decreased LF SAP at <2 weeks (2.22 ± 0.65 mm Hg2). Autonomic injury was defined as high-level SCI with LF SAP <2 mm Hg2. Two distinct groups emerged by 1 month: autonomically complete SCI with sustained low LF SAP (0.76 ± 0.17 mm Hg2) and autonomically incomplete SCI with increased LF SAP (5.46 ± 1.0 mm Hg2, p < 0.05). Autonomically complete injuries did not recover over time. Cardiovascular symptoms were prevalent and worsened with time, especially in those with autonomically complete lesions, and chronic SCI. Baroreflex function and cardiorespiratory interactions were impaired after SCI. Risk of arrhythmia increased immediately after SCI, and remained elevated throughout the acute phase. Acute SCI is associated with severe cardiovascular dysfunction. LF SAP provides a simple, non-invasive, translatable, quantitative assessment of autonomic function, and is most informative 1 month after injury.
Introduction
It is well appreciated that the cardiovascular autonomic dysfunction that accompanies spinal cord injury (SCI) has profound effects on activities of daily living, 1,2 and can manifest with life-threatening cardiovascular conditions. 3 Of particular concern for individuals living with high-level SCI (at or above the sixth thoracic level [T6]), is the inability to regulate autonomic cardiovascular control due to loss of descending control of efferent sympathetic nerves. 4 This often manifests with poor heart rate and blood pressure control through disruption of sympathetic outflow to the heart and key peripheral vasculature beds that mediate vascular resistance and capacitance responses. 3,4 Accordingly, these individuals are prone to episodes of autonomic dysreflexia (AD; sudden profound hypertension triggered by sensory stimuli from below the lesion level), 5 orthostatic hypotension (OH; hypotension in the upright position), 6 fatigue, 7,8 and cardiac arrhythmia. 9 –11 However, the progression and evolution of cardiovascular autonomic dysfunction during the first year (acute phase) of SCI is not known. This makes it difficult to predict the severity and time course of the complex cardiovascular consequences of SCI, and complicates their management.
One contributing factor to this gap in the literature may be the lack of a gold standard quantitative method to assess cardiovascular autonomic dysfunction following SCI. Any such tool would need to be suitable for use in individuals in the acute post-injury phase, able to accurately quantify the severity of injury to autonomic pathways, able to provide meaningful information concerning the extent of autonomic dysfunction an individual is likely to experience, and able to track changes in function over time. 3 The quantitative evaluation of beat-to-beat fluctuations in heart rate and blood pressure (and their interactions) using spectral and cross-spectral analysis can potentially satisfy these criteria for assessing autonomic dysfunction after SCI. Such analyses permit quantitative evaluation of cardiac sympathetic and vagal control, 12 sympathetic control of the vasculature, 10 the sensitivity and delay of the cardiac baroreflex, 13,14 and the interactions between respiratory and cardiovascular parameters. 14,15 These analyses are of particular interest because they are well-established measures of cardiovascular autonomic function in the able-bodied, 14 –16 and have already been applied to both human 10 and experimental 17 SCI. This provides a useful means to apply results from bench to bedside, thus promoting translational discovery science. Other benefits are the low cost, non-invasive nature, and minimal participation required. 15
Assessment of autonomic function in the acute period after SCI is particularly challenging because of the potential for discordance between motor, sensory, and autonomic injury 18,19 accompanying neurogenic shock (global loss of sympathetic outflow to the peripheral vasculature associated with profound hypotension) initially after injury, 3,12,20 and the potential for spontaneous recovery of autonomic pathways due to plasticity. 21,22 We aimed to evaluate whether spectral and cross-spectral analyses of cardiovascular function would be: (1) suitable to track the progression and evolution of injury to cardiovascular autonomic pathways over the first year after injury; (2) able to identify individuals with severe lesions to cardiovascular autonomic pathways; and (3) associated with symptoms or signs of cardiovascular dysfunction.
Methods
Ethical approval
This study was approved by the Department of Research Ethics at Simon Fraser University and Vancouver Coastal Health Research Institute. All aspects of this study conform to the principles outlined in the Declaration of Helsinki. 23 All participants provided written informed consent at the time of testing.
Participants
Eligible participants were at least 18 years of age, had recently sustained a traumatic SCI, and were inpatients in the Acute Spine Unit at Vancouver General Hospital. Individuals were excluded from the study if they had known cardiovascular or neurological diseases prior to sustaining their injury, cauda equina or conus lesions, diabetes mellitus, and/or were involved in other research studies with clinical interventions. Additional exclusion criteria included medical/psychiatric conditions or substance abuse disorders that were likely to affect their ability to consent to or complete the study, inability to communicate in English, and pregnancy.
Experimental protocol
In this longitudinal study, participants were tested at four time-points during the first year (acute phase) following SCI (Fig. 1): Visit 1, 2–14 days post-injury; Visit 2, 2–4 weeks post-injury; Visit 3, 2–3 months post-injury; and Visit 4, 6–12 months post-injury; as well as at a fifth visit (Visit 5), 12–18 months post-injury (subacute phase; Fig. 1). During each test visit, participants were fitted with a standard three-lead electrocardiogram (ECG; lead 2) and a non-invasive beat-to-beat finger blood pressure monitor (Finometer Midi, Finapres Medical Systems [FMS], Amsterdam, The Netherlands). Blood pressure and ECG were recorded supine for 15-min (sampling rate 200 Hz). Data were stored for offline analysis of beat-to-beat blood pressure and ECG signals.
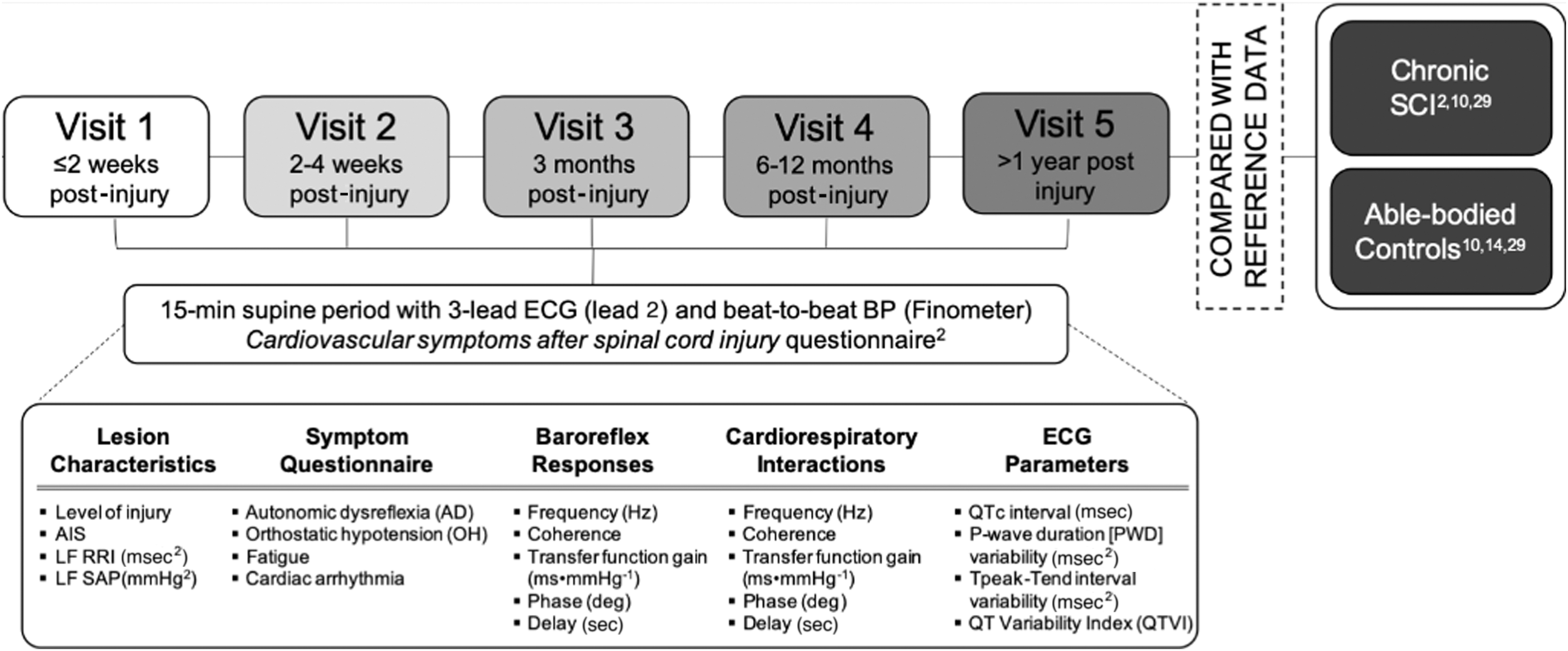
Study protocol. AIS, American Spinal Injury Association Impairment Scale; LF RRI, low-frequency R-R interval; LF SAP, low-frequency systolic arterial pressure; SCI, spinal cord injury.
Following this recording, participants were asked to complete a questionnaire about their cardiovascular symptoms (including OH, AD, arrhythmia, and fatigue). 2,24
Neurological level and severity of injury to motor and sensory pathways at each time-point were determined using the American Spinal Injury Association (ASIA) Impairment Scale (AIS). 25 Based on level criteria, individuals with injuries at or above T6 were considered “at risk” for cardiovascular dysfunction. Based on AIS grade, individuals with AIS A injuries were considered motor/sensory complete.
Data analyses
Autonomic completeness of injury
Autoregressive monovariate models were fitted to time series generated from beat-to-beat systolic arterial pressure (SAP) and R-R interval (RRI) to determine both blood pressure and heart rate variability. 14,15,26 Occasional ectopic beats were removed using linear interpolation of adjacent normal beats, and significant trends were removed by subtracting the best polynomial function fitted to the data using low pass filtering. 15 Three peak frequencies were identified for each power spectrum: very low frequency (<0.03 Hz), low frequency (LF, 0.5–15 Hz), and high frequency (HF, >0.15 Hz). The central frequency, as well as both absolute and percent power at each frequency domain, were determined by computation of the residuals. 27 We focused our analyses on the key autonomic parameters of interest: LF RRI (reflecting oscillations in vagal outflow generated through the baroreflex and driven by sympathetically induced LF SAP) 15,28 and LF SAP (reflecting sympathetic control of the vasculature 14 arising from the sympathetic centers in the rostral ventrolateral medulla 29,30 ).
Autonomic completeness of injury was inferred from LF SAP variability according to our standard approach. 10 An injury was considered autonomically complete (severe injury to cardiovascular autonomic pathways) where LF SAP variability was <2 mm Hg 2 and injuries were at or above T6 at Visit 2. Autonomic completeness was not determined from Visit 1 because of the high likelihood of neurogenic shock, with global, temporary loss of sympathetic control immediately following injury that might confound estimates of injury to descending sympathetic pathways. In cases where Visit 2 data were not available, autonomic completeness was inferred from a LF SAP <2 mm Hg 2 at the subsequent visit.
Baroreflex function and cardiorespiratory interactions
Baroreflex function was assessed by cross-spectral analysis of LF SAP and LF RRI. Frequency-related squared coherence, phase shift, and transfer function gain (TFG) between SAP and RRI signals were quantified by fitting a bivariate autoregressive model to the time series.
14
Discrete values of these variables were taken at the frequency corresponding to the maximal coherence value for the frequency range of interest, where the estimated error is minimal.
14,31
Coherence indicates the strength of the relationship between SAP and RRI covariance, with 0 indicating no relationship and 1 indicating complete interdependence; coherence >0.5 indicates statistically significant correlations between the two signals.
32
Cross-spectral analyses in the LF range were taken to describe properties of the arterial baroreflex, where spontaneous oscillations in LF SAP induce oscillations in LF RRI mediated by the baroreflex.
10,17
Phase (deg) represents the time delay between input signal (LF SAP) and output response (LF RRI), and is negative where changes in LF SAP precede changes in LF RRI. Phase was converted to time delay in seconds by the following formula:
TFG (msec·mm Hg−1) indicates the sensitivity or magnitude of the reflex response. Cardiorespiratory interactions were calculated in exactly the same way, but with determination of central frequency, phase (time delay), coherence, and TFG at the respiratory frequency, that is, in the HF range.
ECG markers of arrhythmia risk
ECG parameters (RRI, p-wave duration [PWD], QT interval corrected for heart rate using Bazzett's method [QTc], Tpeak-Tend interval [TpeakTend], and QT variability index [QTVI]) were determined using customised software (LabView 2010, National Instruments) as described previously.
33
The variability for each ECG interval parameter was determined using autoregressive spectral analyses. QTVI was determined by the following formula:
33,34
where v and m denote the variability and mean, respectively. Typically, QTVI is a negative number. The more positive (closer to zero) the QTVI, the greater the risk of ventricular arrhythmia.
Symptoms of OH, AD, and fatigue
Symptoms of OH, AD, and perceived arrhythmias (palpitations) were quantified as described previously. 2 Higher reported values indicate increased symptom frequency and severity. A fatigue severity score was calculated using a linear visual-analog scale (0, no fatigue; 10 severe fatigue) from an average of three sample questions from the Fatigue Severity Scale. 8,35
Comparisons with historical data from individuals with chronic SCI and healthy able-bodied controls
Where applicable, data from these individuals with acute/subacute SCI were compared with existing historical data from individuals with chronic SCI 2,10,33 and healthy able-bodied controls. 10,15,33 These data were collected previously by our research group, using the same techniques and analysis, and provide perspective on the evolution of cardiovascular dysfunction over time after SCI, and in the context of able-bodied normative data.
Statistical analysis
Data processing was performed using R (version 3.3.3) and RStudio (version 1.1.453). Statistical analyses were performed using Sigmaplot 14 (Systat Software Inc., San Jose, CA, USA). Data were tested for normality and parametric or non-parametric assumptions were used as appropriate. Comparisons for whole group data over time were performed using one-way analysis of variance (ANOVA). Comparisons of outcomes measures over time-points and between subgroups were performed using two-way ANOVA. Spearman rank correlations and linear regressions were used to assess the relationships between variables. Statistical significance was assumed where p < 0.05. Where appropriate, data are represented as mean ± standard error, unless otherwise stated.
Results
Demographic and injury information
Information on participant demographics and injuries can be found in Table 1. We tested 63 individuals on at least one occasion (51 males) who had injuries ranging from C1 to L1, and a range of injury severities based on AIS scores. Forty-seven participants (74%) were at risk for developing autonomic injuries based on level criteria (injuries at or above T6). Assessment of LF SAP at Visit 2 revealed that 40% of participants met criteria for autonomically complete injuries, that is, some of those with high-level injuries had at least some preservation of cardiovascular autonomic function.
Participant Characteristics
Data are presented as mean ± standard error or n (%) as appropriate.
AIS, American Spinal Injury Association (ASIA) Impairment Scale; F, female; M, male.
Autonomic assessment
We have previously used LF SAP criteria to distinguish autonomic completeness of injury in individuals with chronic SCI. 10 However, we were interested to see whether this classification also applies in the acute phase of SCI, and whether LF RRI criteria could also be used to identify different subgroups of SCI based on the severity of impairment to autonomic parameters. We compared the evolution of LF RRI and LF SAP with time after injury for the group as a whole and subdivided according to lesion characteristics (Fig. 2). There were no significant differences in either LF RRI or LF SAP over time or between subgroups when classified according to severity of injury based on AIS scores. Discrimination based on level criteria for risk of autonomic injury revealed lower LF SAP and LF RRI in those who were at risk, but a limited ability to distinguish subgroups at any given time-point. There was a significant increase in LF SAP over time in those who were not at risk (p = 0.021).

Evolution of LF SAP and LF RRI over time after injury.
When considering subgrouping based on autonomic completeness of injury, there was a significant main effect of group for both LF RRI (p = 0.002) and LF SAP (p = 0.002), where they were reduced in individuals with autonomically complete lesions. Based on post hoc testing, the ability to discriminate between individuals with autonomically complete and autonomically incomplete lesions was present from Visit 2 onward when using LF SAP criteria, but not until Visit 5 based on LF RRI criteria. When compared with reference data from individuals with chronic SCI (1.84 ± 0.5 mm Hg2, n = 26) 10 and healthy able-bodied controls (5.18 ± 1.0 mm Hg2, n = 43), 10,15 LF SAP tended to be reduced in all participants compared with able-bodied controls, regardless of injury characteristics, at Visit 1 (2.22 ± 0.65 mm Hg2, n = 22, p = 0.064). By Visit 2, the resolution of autonomic function in participants with autonomically incomplete lesions rendered this the first time-point from which autonomic function could be accurately discriminated. From this point onward, LF SAP was significantly higher in those with autonomically incomplete lesions, and normalized compared with control data. LF SAP remained reduced compared with control data at all time-points in those with autonomically complete SCI. These results confirm the utility of discrimination between those with severe autonomic injury and those who have autonomically incomplete lesions using LF SAP criteria. Accordingly, all subsequent analysis will focus on discrimination between subgroups based on autonomic completeness of injury using LF SAP criteria.
Relationships between autonomic assessment and AIS score
As noted above, autonomic parameters could not be distinguished between subgroups based on severity of injury to motor and sensory pathways determined using the AIS score. This disconnect between injury to autonomic, motor, and sensory pathways is underscored in Figure 3. These data show representative examples of LF SAP data in individuals with varying levels and severities of injury based on AIS score. In one example, an individual with a high-level incomplete lesion according to classification of motor and sensory pathways (C4 AIS D) is seen to have near-abolition of LF SAP at all time-points—a severe autonomic injury—despite relative preservation of motor and sensory function (Fig. 3A). In another example, an individual with a low-level injury, in whom autonomic pathways would not be expected to be impaired, shows blunted LF SAP at Visit 1, which is then recovered in all subsequent visits (Fig. 3B). These data also show the various profiles of LF SAP at Visit 2, the time-point at which autonomic completeness is determined (Fig. 3C). This example shows an individual with a low-level lesion and accordingly the expected preservation of normal LF SAP, as well as two individuals with very similar (high-level motor and sensory incomplete) lesions based on AIS criteria but very different severities of injury to autonomic pathways.
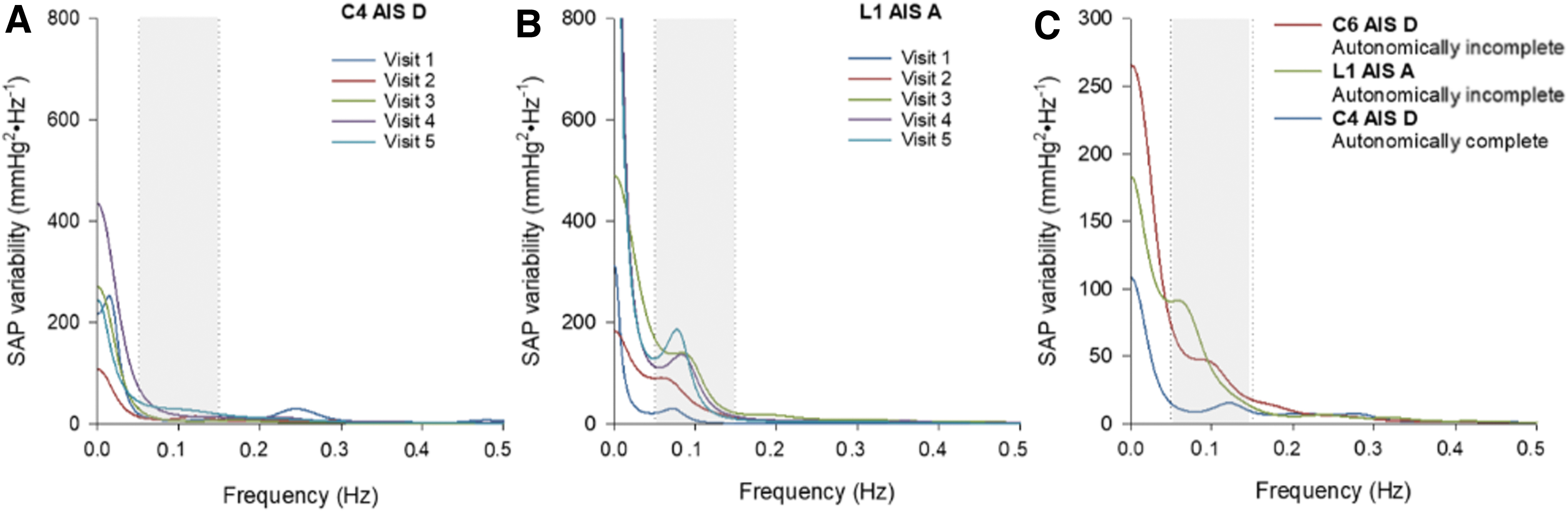
Example power spectra showing typical blood pressure variability profiles.
Symptoms
Cardiovascular autonomic symptoms were prevalent and did not improve with time after injury; in fact, symptoms of AD, OH, and fatigue became worse over time, with particularly high scores in individuals with chronic SCI (Table 2). There was a main effect of autonomic completeness of injury, whereby symptoms of arrhythmia (p = 0.013) and fatigue (p = 0.012) were worse in individuals with autonomically complete than autonomically incomplete lesions. This also tended to be the case for symptoms of AD, although this did not quite achieve statistical significance (p = 0.088).
Symptoms of Cardiovascular Dysfunction
Statistical significance: *denotes significant difference between individuals with autonomically complete and incomplete SCI; Vn denotes significant difference between visit n. Data for individuals with chronic SCI are taken from Inskip and colleagues. 2 Data are presented as mean ± standard error (n). Bold text highlights statistical significance (p < 0.05).
AD, autonomic dysreflexia; OH, orthostatic hypotension; SCI, spinal cord injury.
We considered whether self-reported symptoms were correlated, based on the visit most likely to represent late symptomatology (Visit 5). In individuals with autonomically complete lesions, self-reported symptoms of AD and OH were highly correlated with each other (r = 0.729, p = 0.0016), and symptoms of both AD and OH were correlated with fatigue (r = 0.668, p = 0.006; and r = 0.682, p = 0.005), indicating a high combined symptom burden within the first year post-injury. Interestingly, quantification of autonomic severity of injury using LF SAP at Visit 2 (or equivalent) tended to be significantly correlated with late (Visit 5) symptoms of OH (r = −0.436, p = 0.09) and was significantly correlated with late symptoms of fatigue (r = −0.857, p = 0.006) in those with autonomically complete lesions.
In addition, quantification of autonomic severity of injury using LF SAP at Visit 5 was significantly correlated with late symptomatology in those with autonomically complete lesions: symptoms of OH (r = −0.695, p = 0.017) and symptoms of fatigue (r = −0.668, p = 0.047), and tended to be associated with symptoms of AD (r = −0.515, p = 0.09).
Baroreflex function
For the group as a whole, LF central frequency was left-shifted (0.08 ± 0.01 Hz, p = 0.019) and coherence was low at Visit 1 (0.41 ± 0.05, p < 0.001), but these did improve over time (Table 3). TFG was low compared with individuals with chronic SCI and able-bodied controls at all time-points (all p < 0.001), and did not improve over time. LF phase was low initially but increased over time (p = 0.004), with an associated decrease in the time delay between oscillations in SAP and RRI (p = 0.005). When considering data from only those in whom coherence criteria were met, TFG was statistically smaller compared with both able-bodied controls and individuals with chronic SCI at Visit 3 (p = 0.007 and p < 0.001) and Visit 5 (p = 0.041 and p = 0.005; Fig. 4A). Phase was significantly less negative compared with individuals with chronic SCI at Visit 4 (p = 0.045), with a significant main effect of time (p = 0.009), but there were no significant differences in the delay over time (Fig. 4B).
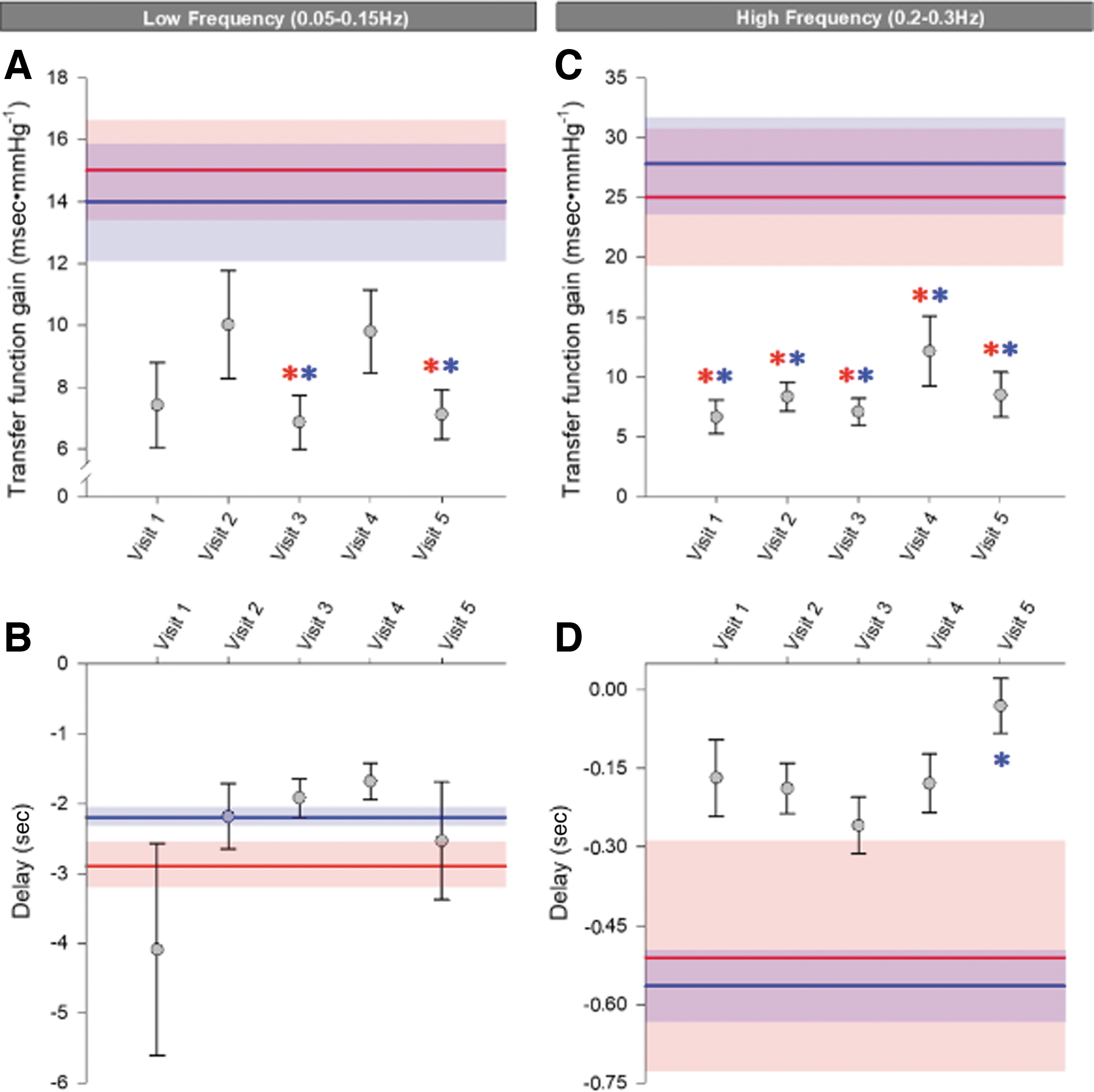
Cardiovascular (low frequency) and respiratory (high frequency) cross-spectral parameters in individuals with coherence ≥0.5.
Cross-Spectral Analyses of Cardiovascular and Respiratory Parameters over Time
Statistical significance: *denotes significant difference between individuals with autonomically complete and incomplete SCI; Vn denotes significant difference between visit n. Statistical significance (p-values) are also presented for the main effects of visit, subgroup classification based on autonomic completeness of injury, and their interactions. Data for individuals with chronic SCI and for healthy able-bodied controls are from Claydon and Krassioukov. 10 Data are presented as mean ± standard error. Bold text highlights statistical significance (p < 0.05).
SCI, spinal cord injury; TFG, transfer function gain.
Given the low coherence, particularly in the early time-points, we only considered subgroup analyses on data for which coherence was >0.5 (56% of all recordings). There were no significant differences between subgroups distinguished by level, AIS, or autonomic completeness at any time-point.
Cardiorespiratory interactions
For the group as a whole, HF central frequency was right-shifted at Visit 1 (0.28 ± 0.02 Hz, p = 0.045), particularly compared with individuals with chronic SCI, but did normalize over time. TFG was also reduced in all visits compared with individuals with chronic SCI and able-bodied controls (p < 0.001) (Table 3). Phase was negative and increased compared with individuals with chronic SCI and able-bodied controls (p = 0.004), corresponding to a reduced delay that did not increase over time (p = 0.002). When considering data from only those in whom coherence criteria were met (56% of all recordings), again TFG was reduced at all time-points and did not improve over time (Fig. 4C). Phase was significantly more positive at all time-points compared with healthy able-bodied controls, corresponding to a tendency to a smaller time delay compared with controls that reached statistical significance at Visit 5 (Fig. 4D). There was a main effect for the HF central frequency to be significantly higher in those with autonomically incomplete lesions, but there were no other significant differences between subgroups distinguished by level, AIS, or autonomic completeness of injury at any time-point.
ECG analyses
Interval analyses
ECG interval parameters were compared over time (Visit 1–Visit 5) and to reference data from individuals with chronic SCI and healthy able-bodied controls. 33 Resting RRI lengthened over time for all participants (p < 0.0001), indicating slowing of heart rate. This effect was more pronounced in individuals with autonomically incomplete injuries than those with autonomically complete injuries (p = 0.042), in whom heart rate tended to be slower initially. PWD was longer in the late acute period (Visit 3: 124 ± 14 msec; Visit 4: 129 ± 15 msec) compared with chronic SCI (102 ± 4 msec) and controls (100 ± 4 msec) (all p < 0.01). There were no significant differences in Tpeak-Tend, between subgroups categorized by either lesion level, AIS, or autonomic completeness of injury, or compared with those with chronic SCI or healthy able-bodied controls.
Additionally, when assessing total variability of RRI within the first five visits, variability was increased in those with autonomically incomplete injuries compared with those with autonomically complete injuries (p = 0.014). Within those with autonomically incomplete injuries, variability increased over the first year (Visit 1 vs. Visit 4, p = 0.012) consistent with the resolution of autonomic dysfunction. There were no significant differences in RRI variability between subgroups defined by level of injury, or AIS classification.
Markers of arrhythmia risk
Mean QTc, as well as QTVI, PWD variability, and Tpeak-Tend variability for all participants were compared both over time and with reference data for individuals with chronic SCI and able-bodied controls 33 (Fig. 5). Mean QTc was significantly increased at Visit 1 and Visit 3 compared with both healthy controls and individuals with chronic SCI, but did decrease over time (p = 0.0001), becoming normalized compared with reference data. PWD variability was significantly increased over all five visits (all p < 0.01), compared with both individuals with chronic SCI and healthy controls, with no significant improvement over the five visits. QTVI was significantly increased at Visit 1 and 3 compared with individuals with chronic SCI (p = 0.082 and p = 0.006) and at Visits 1–4 compared with healthy controls (all p < 0.001) but did significantly decrease over time (p < 0.001). Tpeak-Tend variability was not significantly different compared with controls or individuals with chronic SCI and did not change over time, although there was a trend, for higher Tpeak-Tend variability at Visit 3 compared with able-bodied controls (p = 0.075).

Evolution of electrocardiographic predictors of cardiac arrhythmia over time after injury.
There were no significant differences in these markers for arrhythmia (Mean QTc, QTVI, PWD variability or Tpeak-Tend variability) between subgroups classified according to lesion level, AIS, and autonomic completeness of injury over the five experimental visits (p all >0.05). We considered whether the severity of autonomic impairment, based on LF SAP at Visit 2 (or equivalent), was correlated with these markers of arrhythmia based on the visit most likely to represent late outcomes (Visit 5). There were no significant correlations between autonomic completeness of injury and markers of risk for arrhythmia either for the group as a whole, or in a subanalysis of only those with autonomically complete lesions. Of note, in those with autonomically complete injuries, late (Visit 5) markers of risk of ventricular arrhythmia were significantly correlated with each other (QTVI was correlated with mean QTc r = 0.745, p = 0.007; Tpeak-Tend variability was correlated with mean QTc r = 0.587, p = 0.042; and QTVI and Tpeak-Tend variability tended to be correlated: r = 0.527, p = 0.09).
Discussion
This is the first study to assess the timing, severity, progression, and implications of cardiovascular autonomic injury in the acute phase after SCI. We have demonstrated that LF SAP is a feasible and applicable method for the quantitative assessment and classification of severity of cardiovascular autonomic (sympathetic) injury in the acute care setting. LF SAP (as a direct measure of peripheral sympathetic activity) was a more discriminate tool than LF RRI (which incorporates sympathetic and vagal influences on the heart), AIS injury severity (which assesses motor and sensory function), and level of injury (which does not discriminate injured pathways) for the assessment of autonomic function post-injury.
Quantification of LF SAP was able to discriminate individuals with autonomically complete and autonomically incomplete lesions within the first month post-injury, as well as identify significant differences in the severity of symptoms of cardiovascular dysfunction between those with different severities of lesions to cardiovascular autonomic pathways. In general, the symptom burden was high and did not improve over time—in fact symptoms of AD, OH, and fatigue worsened over time. Symptoms of arrhythmia, fatigue, and AD were higher in individuals with blunted LF SAP, and thus autonomically complete lesions. These data highlight the need for aggressive management of cardiovascular dysfunction in individuals with SCI, particularly those with autonomically complete lesions, and in light of the profound impact of cardiovascular dysfunction on quality of life for individuals with SCI. 1,2 Further, these symptom profiles challenge prior dogma that OH improves over time, 36 as well as previous notions that AD is rare in the first weeks after SCI. 37,38
We have once again demonstrated that there is a disconnect between the severity of injury to cardiovascular autonomic pathways and severity of injury to motor and sensory pathways as determined by AIS scores. Although this has been reported many times by our research group 2,10,39 and others, 18,19 there are still numerous reports in which AIS A injuries are considered to be “severe” and accompanied by profound injury to cardiovascular autonomic pathways 10 ; this assumption should continue to be challenged as it may not always be the case.
Obviously, individuals with lesions below T7 are at low risk for cardiovascular autonomic concerns, and should be reassured. 40 Individuals with injuries above this level, even those with motor and sensory incomplete lesions, can also have profound autonomic impairment, thus rationalizing the use of LF SAP to identify risk of cardiovascular dysfunction after SCI. Recently, ASIA and the International Spinal Cord Society (ISCoS) released the first guidelines for scoring autonomic function following SCI. 19 Although this is a major improvement to the pre-existing impairment scale (which previously assessed motor and sensory function alone), this new addition fails to accurately quantify autonomic function following SCI. Although we have shown a connection between quantitative and qualitative markers of autonomic dysfunction, we, like the Autonomic Standards Committee responsible for the creation of the International Standards to document remaining Autonomic Function after Spinal Cord Injury (ISAFSCI), 19 recognize that there is no current clinical standard with which to accurately quantify the degree of autonomic dysfunction after injury. We believe the addition of LF SAP to the assessment of autonomic function post-injury provides a robust quantitative tool, allowing clinicians and researchers to accurately describe autonomic impairments post-injury. In addition, use of LF SAP represents an ideal tool to assess changes in autonomic function in clinical trials, with the additional benefit that it can be used in pre-clinical research, 17 facilitating translation of results from bench to bedside, and back.
Although we advocate for the use of LF SAP to assess autonomic function after SCI, there are some caveats to this approach. We found that it was not possible to discriminate between individuals with autonomically complete and autonomically incomplete lesions until Visit 2 (approximately 1 month post-injury). Prior to this time-point there was global suppression of sympathetic function irrespective of later autonomic severity of injury in all participants. We suspect that this reflects the numerous autonomic insults occurring during this time, including the presence of neurogenic shock, other accompanying trauma, blood loss, surgery, medication use, deconditioning, sleep-disordered breathing, etc. However, after the first few weeks we were able to document the emergence of two distinct groups: one with the resolution of LF SAP (autonomically incomplete) and one where LF SAP remains absent or blunted (autonomically complete).
We were keen to determine whether LF RRI would also provide a useful tool for discrimination of cardiovascular autonomic function after SCI. Although we did detect a reduction in LF RRI in those with autonomically complete injuries, the ability to discriminate between groups was weaker, and did not emerge until later time-points after injury. This presumably reflects that LF RRI is not a direct measure of sympathetic function, and also incorporates vagal (parasympathetic) influences on heart rate, 41,42 which would not be expected to be affected by SCI. 43 This highlights the need for a pure assessment of sympathetic function when considering autonomic completeness of injury after SCI.
Irrespective of autonomic injury, it is likely that all participants displayed marked cardiovascular deconditioning consistent with their traumatic spinal injuries. 12 Indeed, the high levels of fatigue, impaired baroreflex sensitivity, and blunted LF SAP and LF RRI are hallmark features of deconditioning. 10,12,42 However, many of these markers of deconditioning were more severely impaired in participants with autonomically complete injuries, presumably because their additional autonomic dysfunction further exacerbates the deconditioning process in addition to directly contributing to these abnormalities. Of note, we observed particularly high levels of fatigue in those with autonomically complete lesions. This is concerning because chronic fatigue is known to negatively impact participation in rehabilitation and quality of life after SCI. 2,7,8 In community-dwelling individuals with SCI, high levels of fatigue have been linked to polypharmacy, 44 and this may be one factor that contributes to the high levels of fatigue we observed. 2
Our cross-spectral analyses revealed profound impairments in baroreflex function in the acute phase after SCI, with low coherence between changes in blood pressure and heart rate, reduced baroreflex sensitivity, and a tendency to longer reflex delay. There are many factors that might play a role in impaired baroreflex function in the acute phase after SCI, including blunted blood pressure variability, which would reduce the input stimulus to the baroreflex, 10,45 the inability to activate baroreflex-mediated sympathetic modification of heart rate in those with high-level autonomically complete lesions, 46 cardiovascular deconditioning, 12,42,47 vascular stiffening, 48 and medication use. 49 The increased baroreflex sensitivity in those with chronic SCI suggests that baroreflex function does improve with time after injury, presumably due to reductions in deconditioning and reliance on intact cardiac vagal modulation. 42 We did not see a greater degree of impairment in baroreflex function in participants with autonomically complete injuries, which may be attributed to the predominance of vagal influences on cardiac baroreflex function during supine rest. 42 Of interest, baroreflex sensitivity decreases in individuals with cervical SCI when vagal tone is reduced following the assumption of a seated posture, suggesting there is indeed a reliance on efferent vagal baroreflex modulation in those at risk for severe autonomic injuries. 10
When considering cardiorespiratory interactions, we found profound reductions in response gain along with a shortened time delay between respiratory-associated changes in blood pressure and heart rate. We also observed a higher central frequency of these respiratory oscillations that normalized over time and likely reflects the tendency to rapid, shallow breathing after SCI secondary to paralysis of the accessory muscles of breathing and the presence of neurogenic shock. 50 There are two main theories as to the mechanisms underlying these cardiorespiratory interactions: (1) respiratory-induced changes in intrathoracic pressure in the HF range introduce baroreflex-mediated, predominantly vagal, modifications in heart rate 51 ; and (2) respiration-induced changes in intrathoracic pressure generate HF oscillations in blood pressure, and with similar timing, generate oscillations in heart rate (respiratory sinus arrhythmia) perhaps mediated by vagal activation via the Hering-Breur reflex. 52 A baroreflex-mediated mechanism requires a sufficiently long latency for a reflex response to occur 53 ; the short response delay (−70 msec to −35 msec) and profound impairments in baroreflex function observed in individuals with acute SCI favor the latter explanation. In individuals with chronic SCI and able-bodied controls the response delay is increased (−530 msec and −570 msec) and baroreflex function improved, and this might suggest greater reliance on a baroreflex-mediated mechanism.
There is one previous study that examined cardiorespiratory interactions in the subacute period after SCI and the researchers also found low cardiorespiratory sensitivity with a similar phase in their cohort of individuals with SCI. 54 However, there were some discrepancies between our data and the earlier report, which reported greater interdependence of cardiorespiratory interactions (higher coherence) in individuals with SCI compared with controls as well as longer response time delays in individuals with subacute SCI (−241 msec) and a feed forward pattern of heart rate into pressure in able-bodied controls (+443 msec). 54 The reasons for these discrepancies are unclear, but may reflect that in the present study participants were breathing spontaneously, and in the earlier study participants were asked to pace their breathing to a metronome, which was noted to be poorly tolerated in those with SCI. 54 Indeed, previous reports have documented that fixed breathing in healthy controls produces inconsistencies in the phase shift, without impacting the gain. 55 Interestingly, manipulation of breathing rates with mechanical ventilation also produces positive phase shifts. 56 Given the impact of SCI on respiratory function, difficulties for participants with SCI in adhering to metronome breathing protocols, and documented effect of altering breathing patterns on these cardiorespiratory interactions, we advocate that these analyses be conducted with spontaneous breathing where possible.
This study is also the first to assess ECG parameters and their evolution with time during the first year after SCI. A key finding of these analyses is the immediate impact SCI has on pro-arrhythmic cardiac activity. We showed blunted heart rate variability in individuals with acute SCI, which is known to carry an adverse cardiovascular risk profile. 57 We also showed adverse changes in numerous ECG-based markers of risk of both atrial and ventricular arrhythmia. Our data support our previous findings that markers of arrhythmia risk are increased following SCI. 33,34,39 However, what was not appreciated in previously reported studies is the timing and magnitude of these changes in cardiac electrical function over the first year of injury: these pro-arrhythmic changes occur almost immediately after sustaining an SCI and persist in individuals with chronic SCI when compared with able-bodied controls, even in the face of some improvements when comparing those with acute and chronic SCI. These data are consistent with the detrimental impact of neurogenic shock, cardiovascular deconditioning, and loss of the ability to regulate cardiac sympathetic outflow on cardiac electrical function. 3,6,10,20
We did not show relationships between markers of arrhythmia risk and autonomic completeness of injury in the acute phase, even though greater impairments in ECG parameters have been reported in those with autonomically complete lesions in the chronic phase after SCI. 33 This may reflect the numerous additional challenges to cardiac function, such as medication use, surgery, other trauma, etc., in the acute phase of SCI, which obscure the relationship with autonomic function at this early time-point and/or that electrical remodeling secondary to impaired autonomic function takes time to develop. It is also important to appreciate that these recordings were taken during supine rest, and thus participants were not under sympathetic challenge. We have previously shown that individuals with severe autonomic injuries have a greater propensity to develop cardiac arrhythmias during increased sympathetic activation (i.e., during bouts of AD) compared with at rest. 39
Interestingly, we found that symptoms of arrhythmia were more pronounced in those with autonomic injury, and might reflect a greater propensity to induce arrhythmia in these individuals with provoking stimuli. One key aspect to note is that given the clearly abnormal ECG findings during resting conditions in this cohort of individuals with acute SCI, it is likely that the risk of developing cardiac arrhythmia during provoking autonomic stimuli such as during AD is actually underestimated. Certainly, the increased risk of developing cardiac arrhythmias seen in all participants in the acute phase after SCI underscores the need for periodic ECG monitoring, and careful attention to reports of palpitations.
There were several limitations to this study. The primary challenge was that, as with many longitudinal studies, there was a loss to follow-up over the course of the five experimental visits. This might increase the statistical likelihood of failing to detect differences between groups or time-points. Despite this, we show robust statistical significance across all measures. We did not assess the effect of medication administered during acute care on our recordings, apart from those considerations taken on testing days. It has recently been shown that polypharmacy contributes to high levels of fatigue, 44 and use of baclofen, commonly prescribed after SCI, is associated with marked neurological (motor/sensory) recovery 49 ; the effects of baclofen on recovery of autonomic function are unknown. We did not power this study to examine interaction effects with medication use, but do consider that our results reflect the clinical reality of acute care after SCI, where polypharmacy is inherently common and might affect cardiovascular autonomic function, especially given the aggressive hemodynamic management that occurs in the acute phase of injury.
We also recognize that the connections we have made to data from individuals with chronic SCI are based on historical data from our research group, 10,15,33 and would be further strengthened with a continuation of this longitudinal study into the chronic phase. At the present time these data are not available, and the challenges with loss to follow-up render them difficult to obtain. The benefit of the present comparison with historical data is the ability to place these data in context with the longer-term outcomes after SCI, and with data from healthy able-bodied controls, using identical data collection and analysis approaches.
Conclusion
We have shown that spectral and cross-spectral analyses of cardiovascular function can be used to track the progression and evolution of injury to cardiovascular autonomic pathways after SCI. Severity of injury to autonomic pathways can be discerned by 1 month post-injury and autonomically complete lesions are associated with a high cardiovascular symptom burden. Acute SCI is also marked by severe deconditioning, persistent baroreflex and cardiorespiratory dysfunction, and abnormal ECG characteristics, regardless of stratification according to AIS scores, risk for cardiovascular injury based on level criteria, and autonomic injury. We propose the use of LF SAP as a simple, effective translatable tool for the measurement of cardiovascular autonomic function after SCI. Given these results, consideration of cardiovascular dysfunction after acute SCI should be prioritized when considering the most appropriate rehabilitation and management approaches for individuals with SCI.
Footnotes
Acknowledgments
We are grateful for the help and support of all the team members at the Vancouver Acute Spine Unit, including Allan Aludino, Lise Belanger, RN, and Janelle Pennington, RN. We also thank Erin Williams, Simran Sangha, Sargun Bajaj, Olivia Sandberg, and Dave Borrel for their assistance with data analysis.
Funding Information
This work was funded by the Heart and Stroke Foundation of Canada (BC and Yukon; Grant No. G-13-0002836). B.K.K. is the Canada Research Chair in Spinal Cord Injury and the Dvorak Chair in Spine Trauma.
Author Disclosure Statement
No competing financial interests exist.