
Abstract
This scoping review aims to synthesize existing literature regarding theory of mind (ToM) outcomes, the neuropathology associated with ToM outcomes, and the relationship between ToM outcomes and social functioning in children and adolescents with traumatic brain injury (TBI). We searched MEDLINE® and PsycINFO databases to identify all literature that examined ToM following pediatric TBI until July 2019. A total of 29 articles met inclusion and exclusion criteria and were included in the results. These articles examined a variety of aspects of ToM, which could be broadly grouped into those focused on cognitive, cognitive-affective, and pragmatic factors. The existing literature suggests that children and adolescents with TBI, compared with their typically developing peers and peers with orthopedic injuries, are more likely to have deficits in ToM. The evidence further shows that the age at which brain injury occurs contributes to ToM disruption. Neuroimaging techniques have offered crucial insights into how TBI may impact ToM performance in children and adolescents. Finally, this review provides evidence that disruption in ToM plays a role in the difficulties in social functioning demonstrated by children and adolescents with TBI. Limitations and gaps in the existing literature warrant future research in this field.
Introduction
Traumatic brain injury (TBI) can impact children's social cognitive functioning and social competence. 1,2 Studies have demonstrated frequent social difficulties among children and adolescents who sustained a TBI, 3 including reduced social participation 4,5 and disruptions in social relationships. 6 –8 As a consequence, children with TBI often experience higher mental distress and lower quality of life. 7,9 –11 These difficulties in psychosocial functioning and social competence have been attributed to impairments in social information processing, which involves a series of problem-solving steps that children execute when responding to social sitations. 12,13 In this scoping review, we examine the impact of TBI on social information processing, focusing in particular on the role of theory of mind (ToM), in children and adolescents with TBI.
Previous research has proposed that individual differences in ToM underlie the differences in social information processing between individuals. 14 –17 ToM is the cognitive ability to attribute mental states (i.e., beliefs, desires, intentions, and emotional states) to oneself and others. 18 In everyday social interactions, ToM allows children to consider the diverse perspectives of others, helps them to explain and predict the others' behavior, and enables them to adapt their own social responses accordingly. Once children enter school, ToM becomes an even more essential skill for navigating social interactions, as they develop relationships with a broader set of individuals (i.e., peers, teachers). Longitudinal studies of ToM in typical developing (TD) children have shown that better ToM skills promote peer acceptance, mutual friendships, and prosocial behaviors. 19 –22 Poor ToM understanding, on the other hand, appears to be related to poorer social relationships. For example, ToM skills measured at 5 years of age predicted becoming a bully and/or a victim at 12 years of age. 23
ToM is a multidimensional ability acquired across development, and therefore, different tasks have been developed for its assessment (see Wellman 24 for a review). These tasks are considered valid measures of developmental changes in social information processing in both TD children and in clinical populations. 25,26 ToM tasks can be organized into three different groups depending on the skills required to perform the task: cognitive, cognitive-affective, and pragmatic factors (see Fig 1). Most ToM research has focused on tasks measuring cognitive aspects of ToM; that is, tasks that primarily draw upon cognitive skills to infer others' mental states. In this domain, research has identified a developmental progression in children's understanding of different mental states. That is, children are successful on tasks measuring their understanding of others' intentional actions, desires, beliefs, and knowledge states before they pass false-belief (FB) understanding tasks. 27,28 FB tasks, considered a litmus test for ToM, are the most common way to assess cognitive ToM, and measure whether children can track another's FB about an event (e.g., the location of an object) in order to accurately predict their subsequent behavior (e.g., where a character will search for a desired object). By age 4.5–5 years, many children consistently pass a variety of FB tasks. 18 Children's understanding of cognitive ToM beyond the pre-school period is measured using the second-order FB task, which requires children to reason about someone's FB about another's thoughts and beliefs. 29 Although some studies (e.g., Sullivan and coworkers 30 ) have shown that younger children pass this task when linguistic demands are reduced, development of the second-order ToM is commonly accepted to occur in middle childhood at approximately 6–10 years. 31
ToM tasks in the other domains involve more demands in terms of pragmatic and emotional understanding (see Fig. 1). These tasks typically measure more advanced ToM inferences in children beyond pre-school years, including the understanding of non-literal communicative intent such as irony or white lies (e.g., strange stories 32 ), recognizing social faux pas, 33 and attributing affective and non-affective metal states from pictures of eye areas (the eyes test 34 ). These tasks require more sophisticated understanding of the meaning of messages in social settings, social knowledge, or more difficult inferences about mental states using a subtle visual cue. Emotional information involved in the stimuli also contributes to delayed success on those tasks. 16 Research from lesion and neuroimaging studies has suggested that affective ToM, involving the comprehension of others' affective states and emotions appears to emerge slowly in development, as it requires the integration of both affective and cognitive processing of emotional states. 35
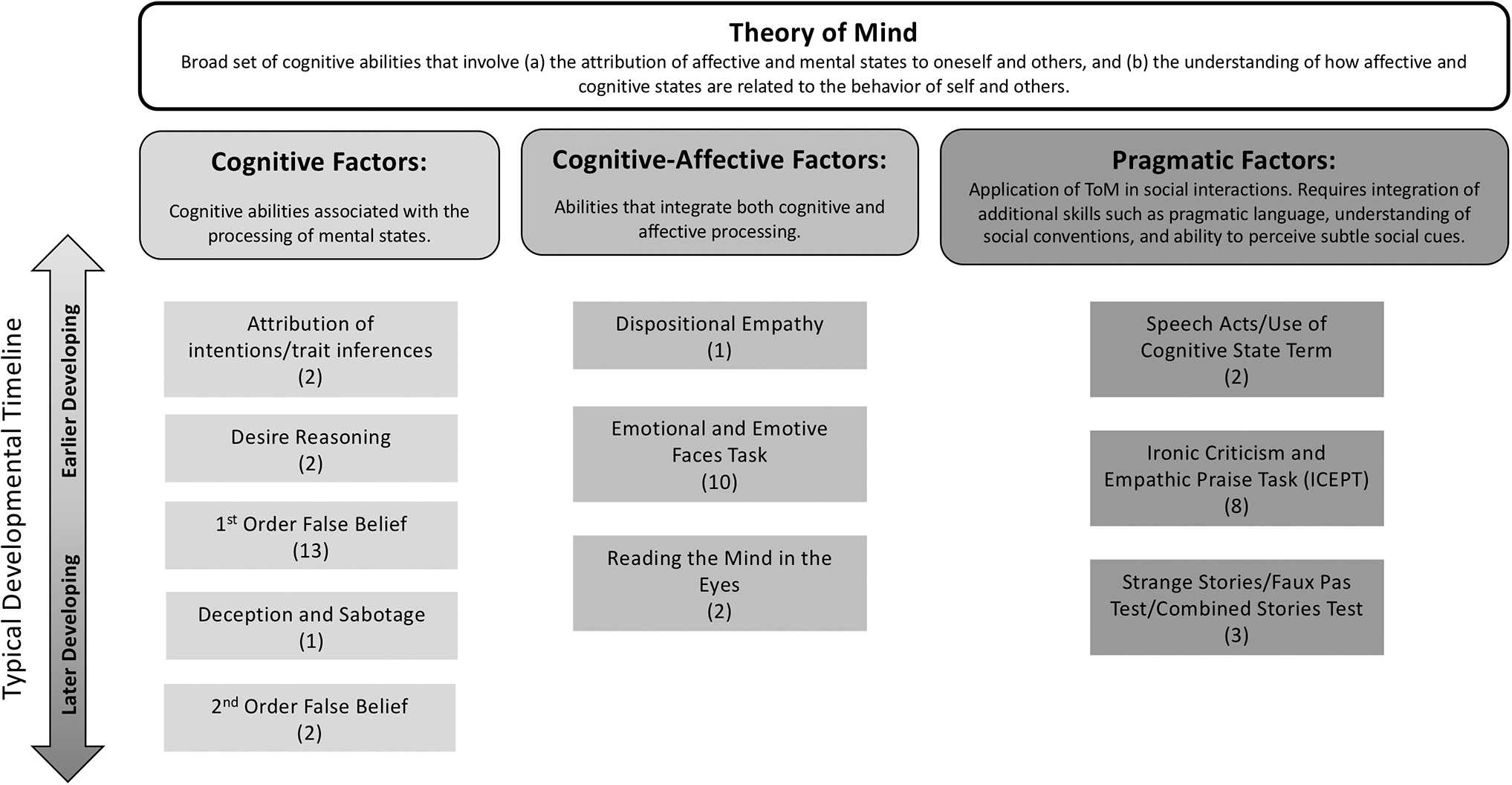
A conceptual framework of the multidimensional nature of theory of mind (ToM) organized into three groups. Cognitive measures primarily draw upon cognitive skills to infer others' mental states, whereas cognitive-affective and pragmatic measures require other skills and knowledge for mental inferences (e.g., skills to detect and process affective information and social cues, and social knowledge). The bar indicates a typical developmental timeline. A progression from reasoning about the construct at the top to applying the construct at the bottom is well established. Note that this framework depicts typical tasks and categories appearing in the developmental literature. Depending on the task design or the degree of conceptual knowledge required, tasks could be grouped in another factor or require a longer period for children to demonstrate their use of ToM. Numbers indicate the number of studies in this review that measured the construct.
Using the tasks described, ToM development has been shown to follow a consistent and fixed order of reasoning abilities. 24 Therefore, using these tasks to assess the extent to which children and adolescents with TBI have ToM deficits, and whether their ToM development varies over time, is reasonable. Indeed, a meta-analysis of studies of ToM deficits in adults with acquired brain injury found that adults show deficits on tasks measuring first-order FB, second-order FB, indirect speech intent, and social faux pas compared with healthy controls. 36
To date, a number of narrative reviews have described social cognition following TBI, reporting impairments in various aspects of social cognition (e.g., empathy, emotion perception, ToM, and pragmatics 37 –39 ). No reviews, however, have focused on ToM skills in children and adolescents with TBI. As such, our objective was to conduct the first scoping review to synthesize existing empirical evidence regarding ToM outcomes, the neuropathology associated with ToM outcomes, and the relationship between ToM outcomes and social adjustment in children and adolescents with TBI. We identify gaps in research that need to be addressed, and recommend future directions.
Methods
We conducted a scoping review following a framework designed by Arksey and O'Malley 40 and refined by Levac and coworkers, 41 with recommendations of Colquhoun and colleagues 42 to synthesize evidence and identify gaps in the literature. We performed all six steps of the framework.
No restrictions were placed on publication year in the search, with a final updated search conducted in July 2019. We searched Ovid, MEDLINE®, and PsycINFO to identify relevant research. The search strategy included terms related to theory of mind (i.e.,
Study selection
We selected studies meeting the following criteria: (1) pediatric and/or adolescent population; (2) measured ToM as either primary or secondary outcome; (3) defined TBI as resulting from closed head trauma; (4) study cohort included children: either child only or child and adult, but in the latter case, the outcomes must be stratified by age (child vs. adult); and (5) full abstract available. We included studies of injuries ranging from mild to severe TBI, with the term “concussion” included as a form of mild TBI. For ToM measurements, we included all tasks described as assessing ToM, mentalizing, perspective-taking, or attribution of mental states (e.g., intention).
Studies were excluded for the following reasons: (1) if the sample was limited to adults with TBI or adults after pediatric TBI; (2) if studies included mixed populations and did not report separate results by injury type (e.g., open vs. closed head) or age; or (3) if studies validated therapeutic programs or assessment tools, used no quantitative measurements, or were reviews or case studies.
Charting the data
We extracted the data and charted the following information: (1) author(s), year of publication, (2) sample (e.g., sample size and age), (3) sample source, (4) study design, (5) study groups (e.g., TBI by severity, comparison group if any, and sample size), (6) age at injury, (7) time since injury, (7) assessments and tasks used to measure ToM outcome, (8) behavioral findings, and (9) neuropathological findings.
The quality of the included articles was assessed by two independent raters (S.B., K.W.L.) using the Newcastle-Ottawa Scale. 43 For our scoping review, the modified version of Newcastle-Ottawa scale for cross-sectional studies 44 was adapted to reflect our main interest (see Table S1). The original Newcastle-Ottawa scale for cohort studies was also adapted so that studies earned a star when the outcome measurements were conducted using objective validated laboratory methods.
Results
The initial search yielded 307 articles. Two authors (N.J. and S.G.) independently assessed the eligibility of the articles for inclusion. The number was reduced to 235 after removing duplicates, and then to 34 after screening the title and abstract, respectively. Of the 34 articles, a total of 29 fulfilled inclusion criteria (see Fig. 2). A hand search of reference lists of these articles conducted by one of the authors did not yield any additional ones.
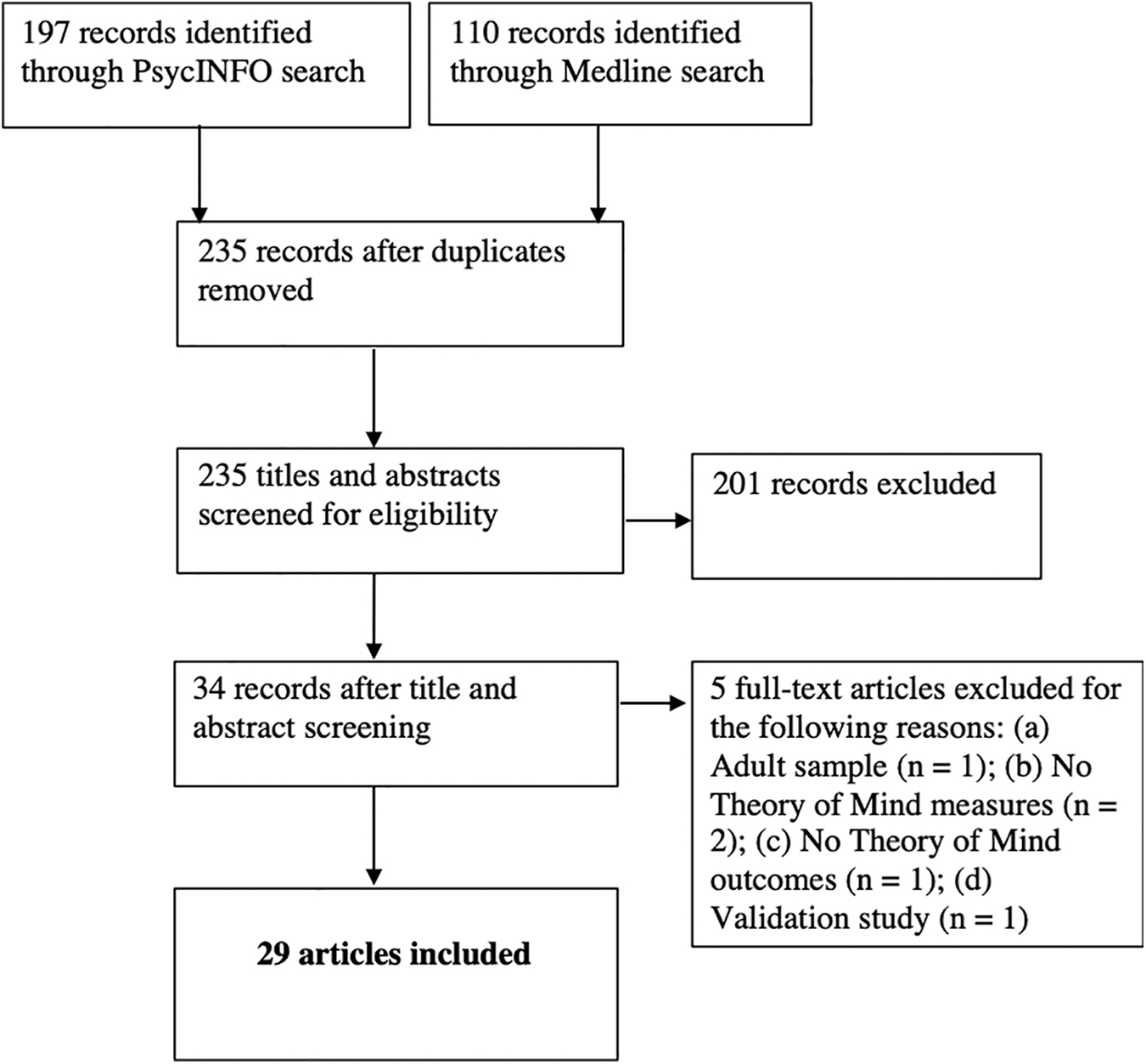
Summary of research and selection of articles.
An overview of data obtained from the 29 articles that met inclusion criteria is shown in Table 1. Of the 29 articles, 19 were identified from four parent studies: eight studies from the Social Outcomes of Brain Injury Kids (SOBIK) study, seven studies from the sample recruited in Melbourne, Australia, two studies from the sample recruited in Montreal, Canada, and two studies from the sample recruited in Ohio, in the United States. The most commonly used study design was cross-sectional (n = 20), with the remaining nine studies using prospective and longitudinal designs. Of the 20 cross-sectional studies, 16 received quality scores of ≥6, as did all prospective and longitudinal studies (Table 2). The average rating of quality was 6.70 (out of 9) for the cross-sectional studies and 7.40 (out of 10) for the prospective and longitudinal studies. The majority of the cross-sectional studies (n = 18) included comparison groups of children with orthopedic injuries (OI) or TD children. Among the prospective studies, eight articles included TD controls and one included both OI and TD controls. A total of 632 unique children with TBI and 546 unique children in control groups (OI: n = 267; TD: n = 546) were included across studies. TBI severity ranged from mild to severe, with more in the mild category; however, totals in each category cannot be reported because of inconsistent categorizing across studies. Age at injury varied from 3 years to 20 years, and time since injury ranged from 1 month to 12 years.
Overview of Studies Included in the Review and ToM Outcomes
ToM, theory of mind; TBI, traumatic brain injury; TD; typical developing (control group); IRI, Interpersonal Reactivity Index; WM, working memory; EEFT, Emotional and Emotive Faces Task; MRI, magnetic resonance imaging; OI, orthopedic injury (control group); FBU, False Belief Understanding Task; ICEPT, Ironic Criticism and Empathic Praise Task; SES, socioeconomic status; ABAS, Adaptive Behaviour Assessment System; DMN, default mode network; CCMN, cerebro-cerebellar mentalizing network; MNEN, mirror neuron empathy network; EF, executive function; SBN, social brain network; STS, superior temporal sulcus; mPFC, medial prefrontal cortex; OFC, orbitofrontal cortex; CBCL, Child Behavior Checklist; SWI, susceptibility-weighted imaging; SOBIK, Social Outcomes of Brain Injury in Kids (study); GM, total gray matter; WM, total white matter; ACQ-Friend, Attribution and Coping Questionnaire – Friends; CT, computed tomography; GCS, Glasgow Coma Scale; SAT, Social Attribution Task; FA, fractional anisotropy; MD, mean diffusivity; IQ, intelligence quotient.
Quality Assessment Scores for Studies Included in the Review
A total of 23 ToM measures were identified in the literature. See Table 3 for a list of measures and a description of each task, as well as the number of studies using each task. In reviewing these studies, we categorized ToM tasks into three groups: those requiring mostly cognitive abilities associated with inferring others' mental states, cognitive-affective abilities that require inferences about both cognitive and emotional states, and pragmatic abilities necessary to apply ToM in social interactions (Fig. 1). ToM tasks used for brain imaging are not included in Figure 1 as they were originally developed to assess brain activation during ToM tasks and therefore do not readily fit within the framework outlined.
ToM Measurements Used in Studies
ToM, theory of mind.
We begin by reviewing findings regarding ToM outcomes in children and adolescents with TBI, followed by a review of the neuropathology associated with ToM outcomes. Finally, we review research describing the relation between ToM outcomes and social functioning in children and adolescents with TBI.
ToM outcomes after pediatric TBI
Cognitive measures
Desire reasoning
Two articles examined children's desire reasoning; that is, whether children understand that someone's desire can be different from their own and whether children appreciate that someone's emotional state (i.e., happy or sad) is a consequence of fulfilled or unfulfilled desire. 45,46 Pre-school children between 18 and 60 months of age with mild TBI showed poorer desire reasoning than TD controls, even when controlling for a pre-existing group difference on externalizing behavior. 45 The significant impact of pediatric TBI on desire reasoning was observed both at 6 months and at 18 months post-injury, when compared with both TD and OI controls. 46 Both studies showed that injury characteristics (e.g., degree of neurological or post-concussive symptoms) were not associated with deficits in understanding of diverse desires in children with mild TBI, and other pre-injury (pre-injury global adaptive scores and social skills), individual (intelligence quotient [IQ] and verbal ability), and environmental factors (parental education and socioeconomic status [SES]) were not different between the mild TBI and the control groups. 45,46
First-order FB
First-order FB refers to the ability to understand others' FBs about the current state of the world. 47 Three key tasks are used to measure first-order FB understanding: false location, false content, and unexpected-identity tasks. These tasks all require children to predict the response of another person whose belief directly conflicts with the child's knowledge about the true state of reality (e.g., children must predict where a character will search for a secretly displaced object or what a character will say is the content/identity of a deceptive-looking object).
When examining first-order FB in children with TBI, studies have yielded inconsistent results. That is, two studies found no differences in first-order FB on a false location and a social cognition tasks in school-aged children and adolescents with TBI compared with TD controls. 48,49 Other studies, however, have reported alterations in this skill following pediatric TBI. That is, Walz and colleagues 50 reported that 3-year-olds with TBI had more difficulty understanding the discrepancy between the appearance and actual identity of a deceptive object (e.g., a candle that looks like an apple) than their OI peers. Further, children with severe TBI between 3 and 5 years were more likely to show knew-it-all-along errors (e.g., claiming that they had known that there were crayons in a candy box). Similarly, Bellerose and colleagues 45 demonstrated that pre-school children with mild TBI showed poorer understanding of another's FB about an object identity compared with their TD peers. This group difference between children with mild TBI and TD controls remained after controlling for pre-existing externalizing behavior. In a subsequent study, however, these authors failed to find a significant effect of mild TBI for FB understanding from 6 months to 18 months post-injury. 46
Alterations in first-order FB following TBI have also been reported in school-aged children, with performance varying as a function of injury severity. That is, ∼1–1.5 years post-injury, children with severe TBI showed a deficit in FB understanding measured by the false location task, whereas children with moderate TBI and OI did not differ in performance on this task. 51 Findings from the SOBIK study, a large multi-site observational cohort study on pediatric TBI, reported that school-aged children with TBI performed poorly on an FB understanding task (i.e., Jack and Jill task) relative to OI controls ∼2.5 years postinjury. 52 –54 Dennis and colleagues 53,54 found that children with severe TBI specifically showed a deficit in FB understanding that was not attributable to differences in attention or motivation. Similarly, another large pediatric TBI research conducted in Australia found that children with severe TBI performed poorly on FB understanding compared with children with mild-moderate TBI and TD controls at 6 months post-injury, even after controlling for sex, age at assessment, and SES. 55 These group differences in FB understanding were not detected in the same sample at 2 years post-injury when controlling for the same variables as well as pre-injury social functioning measured by the Adaptive Behaviour Assessment System-II (ABAS 56 ). 57
In summary, the literature suggests that children with TBI may have poorer first-order FB compared with their peers. For school-aged children, poorer understanding of first-order FB was found among children who sustained TBI compared with their peers. The effect of TBI on first-order FB was more salient in children with severe TBI.
Deception and sabotage
The development of FB understanding is closely related to understanding deception. Successful deception requires individuals to understand their own as well as a listener's mental states, and make a deliberate effort to induce a FB in the listener. 58,59 Indeed, testing children's ability to detect deception has been considered as a way of assessing their ToM development. 47 Using a deception versus sabotage test, 59 Snodgrass and Knott 48 found a significant group difference between severe/moderate TBI and TD groups in sabotage, but not in deception. When children were required to deceive a puppet, both children with TBI and TD controls similarly told a lie to the puppet. When the task, however, required children to sabotage the puppet, children with TBI were more likely to fail to inhibit their pre-potent behavior and thus hinder the puppet than their TD peers.
Second-order FB
Second-order FB tasks 29,30 involve understanding embedded mental states (i.e., attributing beliefs about beliefs). For example, a typical test requires children to track the mental state of two protagonists over the course of a narrative so that they can infer at the end of the story what one agent believes about another agent's mental state (e.g., “What does Maria think Sam thinks…”). Typically developing 6–7-year-olds accurately solve second-order ToM tasks. 29 Walz and colleagues 51 found that 6–7-year-old children with severe TBI showed poorer performance on the second-order ToM tasks than children with moderate TBI and OI. The effect of severe TBI remained after controlling for age at assessment, verbal abilities, and cognitive demands of the task. Similarly, Turkstra and colleagues 49 demonstrated that adolescents with moderate to severe TBI performed worse on second-order ToM questions than TD controls. No relation was found between injury-related factors (e.g., age at injury, injury severity) and performance on the second-order FB.
Attribution of intentions/trait inferences
Two studies examined children's ability to reason about others' intentions based on the outcome in a given situation. 4,60 Anderson and colleagues 4 presented children with hypothetical situations in which the behavior of a child's close friend causes a negative outcome, but the friend's intention is ambiguous. Children and adolescents with TBI and their TD peers did not differ in attribution about their friend's intention. In another study, Levy and Milgram 60 presented children with animated stories in which an agent's behavior (e.g., a suggestion to watch a particular movie) with either positive (e.g., want someone to be happy) or negative (e.g., want someone to be upset) motive leads to either a positive (e.g., happy) or negative (e.g., upset) outcome for another character. They then asked participants to infer the agent's emotion (e.g., whether the agent is happy or sad) and evaluate the agent (e.g., whether the agent is good or bad). Children with TBI performed worse on this task overall and seemed to give more weight on the outcome to attribute the emotion and trait of the agent than their TD peers. When the agent had a negative motive but the outcome was positive, children with TBI rated the agent's emotion more positively and gave higher evaluations than TD controls. On the contrary, when the agent's motive was positive but the outcome was negative, children with TBI rated the agent lower than TD controls did. The group differences remained significant after controlling for executive functioning (EF) as reported by parents, but not after controlling for facial emotional recognition, abstract reasoning, working memory, or verbal fluency.
Cognitive-affective measures
Dispositional empathy
Empathy is considered to include both affective (the ability to share others' emotions) and cognitive (the ability to take others' perspective) components. 61,62 The Interpersonal Reactivity Index assesses diverse dimension of empathy including empathic concern, perspective-taking, fantasy, and personal distress. 63 Using this self-reported questionnaire, Tousignant and colleagues 64 found no significant group effect in any subscales, except perspective-taking. Adolescents with TBI reported lower perspective-taking skills than their TD peers. This group difference remained after controlling for EF (working memory and inhibition) and parents' education.
Affective ToM
Affective ToM refers to the ability to infer others' feelings. 35 The Emotional and Emotive Faces Task (EEFT) 54,65,66 was developed to measure this facet of ToM. In this task, children are presented with short vignettes in which, for social purposes, a character does not express his or her real emotion. Children are then asked to provide a reason for why the character concealed the real emotion and asked to identify the character's real as well as expressed emotions. Differentiating between real and expressed emotions emerges in the late pre-school years and continues to develop into adulthood. 28
Investigations from the SOBIK study found that children with TBI performed more poorly on affective ToM than children with OI. 52,54,66 For example, Bigler and colleagues 52 found that more than half of children with TBI (6 out of 11) had difficulties identifying others' apparent emotions, indicating their poorer understanding of adjusting facial expressions in social interactions. With larger sample sizes, Dennis and colleagues 54,66 found that children with mild/moderate and severe TBI showed poorer affective ToM than their OI peers. Children with TBI used less socially mature strategies to adjust facial expressions for social purposes in that they were more likely to choose the milder manifestation for expressed emotion (e.g., very happy to less happy) rather than a contrasting emotion or a neutral face. 54
In contrast to the above-described results, five studies from a pediatric TBI cohort in Australia have reported inconsistent findings in the domain of affective ToM. That is, Anderson and colleagues found no group differences among children with mild TBI, moderate/severe TBI, and TD controls in affective ToM at 6 months post-injury 4 as well as at 24 months post-injury. 3 Children's performance on affective ToM was predicted by older age at assessment, but not by other cognitive, injury-related, and environmental factors. 3 Contrary to these findings, Ryan and colleagues 57,67,68 found significant group differences in affective ToM following childhood TBI, when controlling for factors known to influence social outcomes following pediatric TBI, such as age at assessment, pre-injury adaptive functioning, and SES. Poorer affective ToM was associated with mild-complicated and moderate TBI. 57,68 Interestingly, in both studies, children with severe TBI showed comparable affective ToM relative to their TD peers.
Evidence suggests that these inconsistent findings on relation between injury severity and affective ToM may be attributed to other factors. Ryan and colleagues 69 demonstrated differential effects of age-at-injury and brain pathology on affective ToM. They found that children who were injured in middle childhood (between 5 and 9 years of age) showed comparable affective ToM skills at 6 and 24 months post-injury to their TD peers. The late childhood TBI group (injured at ∼10 and 11 years of age) performed more poorly on affective ToM at 24 months post-injury than TD controls, whereas the adolescent TBI group (injured between 12 and 15 years of age) showed deficits of affective ToM at both time points.
In summary, the current evidence suggests that TBI negatively affects children's affective ToM in that children with TBI showed poorer understanding of modulating emotions in social contexts. The dose-response relationship between injury severity and affective ToM deficits was inconsistent. Children's age of brain injury may play a role in their acquisition of affective ToM.
Reading the Mind in the Eyes
This test measures whether children can infer affective and non-affective mental states from non-verbal cues, including the eye region of the face. 34 Children are presented with photos of eye areas and asked to choose one depicting a particular mental state. This task has been validated with adult populations. 70,71 Two studies found that children with TBI performed poorly on this task compared with TD controls. 48,60 Furthermore, Snodgrass and Knott 48 found a relationship between children's performance on the eyes test and their emotion recognition abilities. A subsequent study, however, found that group differences on the eyes task were no longer significant after controlling for facial emotion recognition, working memory, verbal fluency, or abstract reasoning skills. 60
Pragmatic measures
Speech acts/use of cognitive state term
These two tasks, unlike other ToM tasks, measure whether children produce proper speech acts or terms to describe cognitive states. In the speech acts task, 72 children are presented a series of pictures in which two people are interacting and asked to generate an intentional speech act reflecting a listener's need in a context. Using this task, Dennis and colleagues 73 found that children with TBI exhibited significantly lower performance than the standard norm. This ability to produce a proper speech act was predicted by individual cognitive inhibition, which was mediated through working memory. Another study measured the number of cognitive stated terms (e.g., think, know, guess) used during a conversation 74 as an index of ToM ability. Adolescents with moderate to severe TBI were divided into high ToM and low ToM groups based on their performance on a ToM task. 75 It was reported that the TBI group with poor ToM understanding was less likely to use cognitive state terms than were children with TBI with intact ToM understanding and their TD peers. 74
Ironic Criticism and Empathic Praise Task (ICEPT)
This task measures conative aspects of ToM, an understanding of others' feelings and intentions associated with indirect speech (ironic criticism and deceptive praise) in social communication. 76,77 Participants are presented with pictures of everyday situations (e.g., building a block tower) accompanied by scenarios that include a speaker's utterances in a neutral, sarcastic, or comforting tone of voice. They are also told the goal of the event, the outcome, the character of the speaker, and the speaker's utterance. In each situation, participants are asked to identify the speaker's beliefs about the event and the addressee, as well as the speaker's intentions regarding what the speaker wants the addressee to think about his/her work and him/her self. Using this task, four studies demonstrated deficits in conative ToM following pediatric TBI. 52,54,67,77 Three studies from SOBIK found conative ToM deficits in school-aged children with TBI compared with the OI group. 52,54,77 Although both the severe and mild/moderate TBI groups showed difficulties in understanding conative communication, 54 evidence suggested that the mild/moderate TBI group had a specific deficit in ironic criticism. 77 Dennis and colleagues 77 showed that these group differences could not be attributed to failures to memorize the speaker's utterance or to comprehend the situation. Among the injury-related factors, only the age at testing successfully predicted children's understanding of both ironic criticism and empathic praise. In line with these findings, Ryan and colleagues 67 found poorer conative ToM in children with mild-complicated and moderate TBI than in their TD peers after controlling for their age at testing and SES. Conative ToM in children with mild-complicated TBI was also found to be lower than that of mild TBI group. No further group differences among mild and severe TBI and TD were detected.
Strange Stories/Faux Pas Test/Combined Stories Test
In these tasks, participants are presented with a series of vignettes that include various indirect statements or faux pas and required to infer the speaker's intention in the context. The Strange Stories Task involves everyday examples from which to infer the speaker's motive and intended meaning of the message (e.g., white lie, joke, irony 32 ). The Faux Pas Test measures children's skill at judging whether a speaker says something that is inappropriate in a social setting. Two studies using the Strange Stories Task did not find group differences between TBI and TD or OI control groups among school-aged children 51 or adolescents. 78 Similarly, Turkstra and colleagues 78 failed to find significant group differences between adolescents with TBI and TD controls in the ability to identify faux pas in short narratives.
Tousignant and colleagues 64 used the Combined Stories Test, which included a set of ToM tasks measuring first-order FB, the Strange Stories Task, and the Faux Pas Test. Adolescents with moderate to severe TBI performed more poorly than their TD peers on the combined measure. After controlling for cognitive abilities and the level of parents' education, the effect of group was only marginally significant, but was still associated with a moderate effect size.
Other measures
Composite ToM
As an indicator of overall ToM skill, three studies used a composite ToM score generated by averaging children's performance on cognitive, affective, and conative ToM tasks. 67,79,80 All three studies reported significant group differences in composite ToM scores. Children with severe TBI showed poorer composite ToM scores than either TD or children with OI. 67,79 However, findings with children with mild TBI were inconsistent. Robinson and colleagues 79 found no significant differences between children with mild-complicated/moderate TBI and children with OI, whereas Ryan and colleagues 67 found that children with mild TBI, but not mild-complicated and moderate TBI, showed lower composite ToM scores than TD controls.
Another study used a composite ToM score calculated from children's performances on first- and second-order ToM tasks as well as the Strange Stories Task. 51 They found an adverse effect of severe TBI on ToM performance compared with moderate TBI and OI. The group difference between children with severe TBI and OI remained after controlling for age at assessment and verbal abilities.
ToM measures for brain imaging
Three tasks were used to assess ToM performance during brain imaging: the social attribution task, the mental attribution task, and the trait attribution task. The first two tasks use a series of short films illustrating movements or interactions among geometric figures (e.g., triangles). The social attribution task measures the ability to attribute social relationships to the figures by asking participants to infer whether or not the figures are friends or enemies, whereas the ability to attribute mental states to those geometric figures is measured based on participants' description about the film in the mental state attribution task. The trait attribution task, which was developed to assess the brain areas activated when people take another's perspective, assesses how participants think about themselves or a significant other from their own or the significant other's perspective. No differences in social attribution 81 or trait attribution 82 were found among children and adolescents with TBI and their TD peers. Levin and colleagues, 83 however, found that children with TBI were less sensitive to the prompt to describe as if the figures were humans compared to the OI controls on mental state attribution task.
Neuropathological characteristics on ToM outcomes
In the following section, we review studies that examined the neuropathological correlates affecting ToM performance in children following TBI. Studies were separated into two main groupings: those that reported clinical lesions and those that used advanced neuroimaging techniques. A variety of neuroimaging techniques were used, including both structural and functional magnetic resonance imaging (MRI) techniques assessing both focal lesions and diffuse injury to large scale brain networks.
Clinical lesions
Findings on the relations between ToM and pathology location in children with TBI are mixed. Focal lesions and diffuse injury to both gray and white matter has been associated with TBI, although less commonly with mild TBI. Initial findings by Snodgrass and Knott 48 indicated that children with known frontal lobe damage showed deficits in ToM compared with TD controls, notably for advanced measures of ToM (i.e., the eyes test) and on a measure of emotional processing, indicating deficits in cognitive and affective ToM. Similarly, Bigler and colleagues 52 found that decreased affective ToM performance was associated with focal lesions in the left frontal and temporal regions with corpus callosum thinning. However, not all individuals who exhibited this pathology displayed this deficit in ToM, and individuals who performed poorly on affective ToM tasks did not all exhibit the expected lesion. In contrast to these findings of a relationship of ToM to focal lesions, Levin and colleagues 83 did not find any focal lesions to be related to ToM performance. In addition, Anderson and colleagues 3,4 found that although the most common lesion site was in frontal regions in children with TBI, the site of injury was not a significant contributor to performance on affective ToM performance at 6 months or at 2 years post-injury. Yeates and colleagues 7 also did not find associations between local volumes and ToM in the TBI group; however, conative ToM was positively associated with global gray and white matter volumes and negatively associated with ventricular volume in both the TBI and OI groups. Collectively, these studies indicate that the relationship between lesion location and ToM outcome varies across children and is more likely to be attributed to global diffuse injuries than focal lesions.
Advanced neuroimaging
The vulnerability of the frontotemporal regions of the brain to TBI may compromise many neural networks. Diffuse injuries to networks associated with ToM such as the social brain network (SBN), salience network (SN), mentalizing network (MN), and mirror neuron/empathy network (MNEN) were observed in many studies in this review using advanced MRI techniques, including susceptibility-weighted imaging (SWI). Five studies in this review examined these relationships. 54,55,57,67,69 Dennis and colleagues 54 found that lesions in the MNEN predicted lower performance on tasks assessing conative ToM, but that cognitive and affective ToM were not significantly affected by lesion location or volume. Specifically, lesions to the posterior cingulate cortex and the hippocampal formation, both integral parts of the limbic system, were associated with poorer conative ToM. Similarly, Ryan and colleagues 67,69 found that more diffuse post-acute neuropathology lesion load was correlated with poor performance on composite ToM tasks. Specifically, reduced volumes of the total SBN, which includes many of the same structures as the MNEN, as well as the cingulate cortex and the superior temporal sulcus, were correlated with poorer performance on composite ToM scores.
Ryan and colleagues 57 sought to further uncover the brain network correlates to different aspects of ToM. As in the study by Dennis and colleagues, 54 the TBI groups showed gray matter volumetric reductions in all networks as compared with TD controls, and performance in conative ToM was correlated with increased lesions to the MNEN. However, they also found that increased lesions in the insula and amygdala as part of the SN predicted deficits in affective ToM and that lesions in the MN were associated with deficits in cognitive ToM. Together, these studies indicate that different types of ToM involve unique brain networks and that injury to these networks may disrupt the higher order processing involved in ToM.
Other methods of MRI have also been used to observe changes in brain pathology and its effects on ToM skill following pediatric TBI. Two studies in this review utilized functional MRI (fMRI) to study brain activation during ToM tasks in children with TBI. 81,82 Newsome and colleagues 82 observed no differences in ToM performance between TBI injured children and TD controls but found differing brain activation patterns. No group differences were found in the frontal regions, but the TBI group showed increased activation in the posterior and subcortical regions while performing composite ToM tasks. Scheibel and colleagues 81 found similar results, with increased bilateral activation in the posterior regions among children with TBI during composite ToM tasks. Increased activation also occurred in clusters in the posterior frontal lobe and in the left occipital lobe extending to the left temporal lobe and cerebellum. These results are generally consistent with neuroanatomical correlates of ToM, as some of these posterior areas have been implicated in social reasoning. Taken together, these studies indicate that these brain regions are more heavily utilized following TBI and may be acting as a compensatory mechanism.
Diffusion tensor imaging (DTI) is another advanced MRI technique used to study pediatric TBI. Only one study in this review utilized DTI to examined correlations between white matter microstructure injury and ToM skill. Levin and colleagues 83 found that the TBI group exhibited lower fractional anisotropy (FA) than OI controls for all regions except the inferior longitudinal fasciculus and the right cingulum bundle, as well as exhibiting higher MD in all regions except the cingulum bundle. The left cingulum bundle and dorsolateral frontal FA was positively associated with ToM performance in both groups, but differences in white matter pathology between the TBI and OI groups did not predict ToM performance.
Contribution of ToM to social adjustment and social interaction
Three studies examined the relationship between ToM and social adjustment. Two studies focused on the association between ToM and post-injury social adjustment in either pre-schoolers or school-age children with TBI. Among pre-school children with mild TBI, poorer performances on desire reasoning and false belief understanding tasks were associated with lower social functioning measured by the ABAS at 6 months post-injury. 46 For school-age children with TBI, those who showed social impairments at 2 years post-injury demonstrated poorer affective ToM, along with other risk factors (e.g., younger age at injury, poorer family function, lower IQ, slower processing speed, and greater pre-injury and current behavioral problems). 3 Levin and colleagues, 83 however, failed to find a significant relationship between the ability to attribute mental states and social functioning on Vineland Adaptive Behaviour Scale (VABS 84 ) in school-aged children and adolescents with moderate-severe TBI.
Recent studies have used mediation analyses to identify the relationship between ToM and social functioning following TBI. One study from SOBIK found that a composite measure of ToM mediated the relationship between severe TBI and social functioning on the ABAS. 79 Ryan and colleagues 67 also showed that a composite ToM score at 6 months post-injury mediated the prospective relationship between abnormal brain morphology at 2 months post-injury and adaptive functioning measured using Child Behaviour Checklist (CBCL 85 ) at 2 years post- injury.
With regard to peer relationships, findings from the SOBIK study demonstrated a possible role of ToM. Among 12 children who sustained a TBI, only two children who showed unimpaired ToM skills had typical friendships; they were liked by their peers and named as friends. 52 Yeates and colleagues 7 found that affective ToM predicted rejection-victimization rated by peers, which was in turn associated with social adjustment in school. Children who had a better understanding of others' actual versus displayed emotions received less rejection-victimization by peers.
One potential reason that children with TBI have poor social adjustment may be poor self-awareness. Wolfe and colleagues 80 examined the role of self-awareness in peer relationships and the contribution of ToM to the relationship. Unexpectedly, they found that higher composite ToM scores were associated with greater discrepancies between peer- and self-ratings of aggression (peer > self). However, ToM was not predictive of discrepancies between peer and self-ratings of other aspects of peer relationships, and the discrepancy between peer- and self-ratings on aggression did not predict children's social functioning with ABAS. Thus, ToM appeared to play a limited role in accounting for self-awareness after TBI.
Discussion
The aim of the current scoping review was to collate the existing literature on ToM outcomes, the neuropathological characteristics related to ToM, and the relationship between ToM and social adjustment in pediatric TBI. Decades of research have expanded our knowledge of the impact of TBI on ToM and its role in social outcomes. To date, however, no review has summarized the impact of pediatric TBI on various aspects of ToM. In this respect, the current review is timely, providing an overview of ToM after TBI in children and adolescents.
We identified 29 studies that varied in study design, sample size, comparison groups, and measurements of ToM, but were mostly considered to be of high quality. In what follows, we review the core findings, and then consider directions for future research.
First, this review confirmed that various aspects of ToM appear to be vulnerable to the effect of pediatric TBI. Overall, children with TBI performed poorly on both first-order FB 51,53 –55 and second-order FB tasks 49,51 relative to children in comparison groups, suggesting a deficit in cognitive dimension of ToM after pediatric TBI. Research has also indicated that children with TBI show deficits in affective ToM, 54,57,66 –68 conative ToM, 53,54,67 and the production of speech acts. 73 Composite measures of ToM, which provide an indicator of overall ToM understanding, have also been reported consistently to be worse in children with TBI than in their peers in control groups, regardless of whether the composite was the average of ToM across different domains (cognitive, affective, and conative ToM) 67,79 or across different levels of complexity (first-order, second-order, or the third-order FB). 51
Second, the review identified that the age at which brain injury occurs contributes to disruption in children's ToM. Pre-school children with TBI show difficulties in understanding different desires between individuals, 45,46 differentiating FB from reality, 45,50 and manipulating behavior to sabotage someone. 48 Adolescents with TBI are at risk of deficits in affective ToM, which were related to more diffuse cerebral damage, whereas affective ToM among those with middle childhood TBI was comparable with that of their TD peers. 69 Moreover, the outcome of late childhood TBI on affective ToM varied as a function of time since injury, such that the effect of late childhood TBI on affective ToM occurred after 24 months post-injury. 69 Taken together, these findings indicate that ToM outcome is dependent on children's neurological and social-cognitive development. That is, early childhood TBI, even when the injury is mild, could negatively affect the acquisition of early developing ToM skills. More advanced forms of ToM, which emerge during late childhood and adolescence when maturation of the medial pre-frontal cortex is still proceeding, 86,87 are a greater risk of deficit in children and adolescents who sustain a TBI later in childhood.
Third, we found moderately consistent evidence of a dose-response relationship between severity of injury and ToM deficits in some domains. That is, disruptions in understanding first-order FB were found in severe TBI groups, but not in moderate or mild-moderate TBI groups. 51,53 –55 Poorer performance on second-order FB was also identified following severe TBI, but not moderate TBI. 51 Another study found worse second-order FB in children with TBI than in their TD peers, but no group differences between those with severe and those with moderate TBI. 49 Overall, these findings indicate that greater TBI injury is associated with poorer cognitive ToM.
In contrast, the relationship between injury severity and performance in other domains of ToM was more inconsistent. One group of studies reported a negative impact of severe and mild-moderate TBI on affective ToM, 54,66 whereas another group of studies failed to find an impact of severe TBI and instead found poor affective ToM following mild-complicated and moderate TBI. 57,68 Regarding conative ToM, evidence suggests that severe TBI is associated with widespread deficit in conative ToM, whereas a specific deficit in understanding irony is associated with mild-moderate TBI. 54,77 An effect of injury severity, however, was not found in another study in which children with mild-complicated and moderate TBI showed poorer conative ToM than the control group, and the poorest conative ToM performance was associated with mild-complicated TBI. 67 Two potential reasons may account for these inconsistent findings. One is the inherent heterogeneity of TBI population, in terms of age at injury, mechanism of injury, and the complexity of the underlying neuropathology. Children at different stages of development are more susceptible to different mechanisms of brain injury, which may cause different neuropathological effects and subsequent behavioral outcomes. A second possible reason may be the small sample size in each injury group. For example, the number of children with severe TBI in the study by Ryan and colleagues 67 was only 10. This sample size may limit the power to detect the relationship between severe TBI and ToM. Future research would therefore benefit from larger sample sizes in each injury group.
Fourth, neuroimaging techniques have offered crucial insights into how TBI may disrupt ToM performance in children. Several studies in this review confirmed that frontal lesions are the most common focal lesion in more severe cases of TBI. 4,83 Only one study, however, found that these focal lesions were related to deficits in cognitive and affective measures of ToM as compared with TD. 48 More evidence indicates that observed deficits in ToM are related to diffuse global injuries to both gray and white matter, which may disrupt major neural networks. 7,55,57,66,67,69 Although large-scale neural networks have been identified to be important for affective, conative, and cognitive ToM, the mechanisms underpinning these relationships are still unclear. Only one study in this review utilized a task-based functional imaging technique, and identified differences in brain activation in children with TBI while they were performing ToM tasks. 82 Further investigation using functional imaging is needed to determine these precise mechanisms. These studies also reveal the potential prognostic value of using advanced neuroimaging techniques to assess neuroanatomical abnormalities to predict ToM outcome and recovery. Future studies using more sensitive structural imaging analysis techniques such as DTI are needed to assess the brain-behavior relationships involving ToM.
Finally, this review demonstrated that disruption in ToM plays a role in difficulties in social adjustment, including social relationships, among children and adolescents with TBI. ToM understanding appears to affect post-injury social adjustment 3,46 and to mediate the effect of severe TBI or brain morphology on social functioning. 67,79 Moreover, children with poor affective ToM are more likely to show higher levels of rejection-victimization, which in turn, negatively affects their friendships following childhood TBI. 7 Given the importance of understanding others' minds in social contexts, the finding that deficits in ToM relate to poor social functioning and mediate the relationship of injury severity and the social outcome is unsurprising. These findings highlight the need for clinical assessment to include consideration of children's ToM to identify critical targets for interventions to promote social adjustment. That is, some children may struggle to understand other's thoughts, whereas others may be unable to recognize subtle social or emotional cues. Further, as few interventions target deficits in social information processing in children with TBI, these findings signal the need for future research in this area. 39
Several limitations and methodological issues were noted in the existing literature. The first limitation is the reliance on cross-sectional designs. We identified only nine studies with a prospective, longitudinal design, which were from two parent studies. More studies employing prospective, longitudinal designs are necessary to better understand the process involved in the long-term effects of pediatric TBI on ToM. Further, because most studies employed a retrospective design, imaging occurred along different points of recovery, and less is known about the post-acute neuropathological effects of pediatric TBI. Another limitation lies in the small sample sizes of the studies reviewed. Across 20 cross-sectional studies, 8 included sample sizes of <50 participants, and more than half of the studies included <20 participants in at least one of the injury groups. As discussed, small samples reduce the power to detect a significant effect, and may account for inconsistent findings among studies. Findings may also have been inconsistent because there were varying comparison groups between studies. Most studies have compared children with TBI with TD children. This is problematic, especially in milder cases of TBI, as it does not account for pre-injury characteristics or post-injury factors such as stress caused by general trauma or pain. A recent DTI study found that adolescents with mild TBI and OI had similar white matter microstructure characteristics, but differed from TD, perhaps making the OI group a more suitable comparison group. 88
We note that many studies did not control for confounding factors such as age (e.g., age at testing) or other affective-cognitive factors (e.g., emotion recognition, EF) in their analysis. The disruption in ToM among children with TBI is likely to be related to deficits in other domains; EF, in particular, is closely related to ToM, 89 and is often negatively affected by pediatric TBI. 90,91 Thus, deficits in EF may hinder children's performance on ToM tasks. Future studies should therefore consider these covariates and aim to establish the contributions of each to ToM outcomes following pediatric TBI. Further, no studies reviewed here examined the potential role of sex or reported ToM outcomes separately by sex. A regent review noted evidence suggestive of gender differences in social cognition among adults with TBI. 92 Therefore, we highlight the need to consider the possible effects of sex on ToM outcomes and the possible role of gender as a moderator between ToM outcome and social functioning following pediatric TBI as a critical direction for future research. The last limitation is the relative dearth of research with pre-school children. Only four studies were identified involving children <7 years of age; therefore, this population would benefit from future research.
The current scoping review, of course, has limitations as well. The first pertains to the article selection process. Although we believe that the review successfully identified and included articles with a variety of measures of ToM, it may have not captured all relevant articles. In our literature search, we found additional studies that measured pragmatic ability instead of ToM. We excluded these articles, because the current work primarily focuses on ToM, and ToM and pragmatic skills are two distinct constructs, although they can overlap. 93 Further, a recent scoping review provided an overview of the relationship between pragmatic language and TBI. 37 Another limitation is that we did not conduct a meta-analysis to quantify the effect of pediatric TBI on ToM. The significant heterogeneity in study designs and ToM measurements, and the small number of studies with non-overlapping participant samples within each task, precluded such an analysis. Finally, the proportionally large number of studies drawing upon two large cohort studies (SOBIK and studies from Melbourne) may introduce a bias in the observed effect of pediatric TBI on ToM outcomes.
Conclusion
In conclusion, the collective evidence indicates that children and adolescents who sustain a TBI, likely because of damage to major brain networks involved in social cognition, are at an increased risk for disruption of various aspects of ToM, which in turn increases the risk of difficulties in their social adjustment and interactions. However, the existing studies are characterized by significant heterogeneity in sample characteristics, study designs, and ToM measurements, hampering strong general conclusions. Future studies are required to reconcile the varied results from the existing literature and to expand our knowledge of ToM skills, their neural basis, and their contributions to social outcomes following TBI in children and adolescents.
Footnotes
Acknowledgments
We thank Summer Abdalla for her assistance with manuscript preparation.
Funding Information
Preparation of this manuscript was supported by funding from a Ronald and Irene Ward Chair in Pediatric Brain Injury, funded by the Alberta Children's Hospital Foundation, to Dr. Keith Yeates, and funding from Alberta Children's Hospital Foundation through the Owerko Centre to Dr. Susan Graham. Narae Ju was funded by an Eyes High Doctoral Scholarship at the University of Calgary.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.