
Abstract
In this systematic review, objectives were to investigate dropout rates, adverse events, and effects of exercise-based therapies on urogenital function and quality of life (QoL) in persons with spinal cord injury (SCI). Database searches were conducted on MEDLINE, EMBASE, and CINAHL for studies examining any form of exercise intervention on urogenital function and/or QoL in adults with SCI. Quality of publications was evaluated using the Joanna Briggs Institute critical evaluation tools. When possible, Hedges' g was calculated for overall effect sizes. Subgroup analyses were conducted on sex and injury severity. Ten studies (228 participants) were included in this review. Three studies examined pelvic floor muscle training, and seven studies examined locomotor training. Overall quality of evidence was low because of small sample sizes and non-randomized designs in most studies. Dropout rates ranged from 12% to 25%, and adverse events were reported only in some studies investigating locomotor training. For lower urinary tract (LUT) outcomes, urodynamic findings were mixed despite moderately positive changes in maximum bladder capacity (g = 0.50) and bladder compliance (g = 0.37). Fairly consistent, but small, improvements were observed in LUT symptoms, primarily bladder awareness and incontinence. LUT QoL improved in most cases. Fewer data were available for sexual outcomes, and only minor improvements were reported. Subgroup analyses, based on sex and severity of injury, were inconclusive. There is some indication for the potential benefit of exercise on urogenital outcomes in persons with SCI, but there is insufficient evidence given the number of studies and heterogeneity of outcome measures.
Introduction
A spinal cord injury (SCI) can result in permanent deficits in sensory, motor, and/or autonomic functions, 1 which complicate daily living and undermine quality of life (QoL). 2 Beyond these dysfunctions, persons with SCI also experience a myriad of secondary health complications that impact nearly every physiological system. Critically, recovery of urogenital function has been consistently reported as a health priority by persons living with SCI. 3,4
Although >80% of persons with chronic SCI have neurogenic lower urinary tract (LUT) symptoms (LUTS) and less than one half are able to achieve normal sexual function, 5 rehabilitation programs post-SCI have focused on restoration of motor function and musculoskeletal health (e.g., mobility, locomotion, prevention of muscle atrophy, and decreased bone density), with less attention placed on secondary complications such as urogenital concerns. 6 Early and comprehensive management of LUTS is critical for those living with SCI, given that the majority experience spastic bladder symptoms (e.g., neurogenic detrusor overactivity [NDO] and detrusor-sphincter dyssynergia), which can result in incontinence, an inability to void effectively, and damage to upper urinary tract structures attributable to dramatic and uninhibited increases in detrusor pressure. 5,7,8
Impairments to sexual function are also of great concern post-injury. 9,10 Sexual responses, such as erection, vaginal lubrication, and orgasm, are driven by somatic and autonomic nerves in the pelvic plexus that are under supraspinal control. Impairments to this descending control attributable to SCI impact both the psycho- and reflexogenic potential for arousal, ejaculation, and orgasm. 10,11 Beyond impaired neural control, the interplay of other LUTS (e.g., incontinence) can also negatively affect the sexual experience and act as a barrier to engaging in sexual activities. 6
Therapeutic options for treating and managing urogenital complications are limited for those living with SCI. Catheterization and pharmaceutical interventions remain the primary approaches for bladder management, 5,7,8,11 but these approaches are associated with increased rates of urinary tract infections (UTIs) 7,11 and other adverse effects. 7 When considering sexual health, the vast majority of research and rehabilitation programs have focused on fertility and reproduction, whereas the sexual needs in persons with SCI remain underappreciated. 6,11
Treatment options for urogenital dysfunction are further complicated by sex and injury characteristics given that each person may have unique challenges and experiences when receiving the same treatment. With respect to sex considerations, males and females have different pelvic anatomy (e.g., the urethra being a shared structure for both the urinary and reproductive system in males, but not in females), which results in potentially different experiences and perceptions about urogenital symptoms, and the necessity for sex-specific treatment options. In terms of bladder management, for example, sex differences in the expression and distribution of certain receptors may impact a person's responsiveness to anticholinergic medications, 12 which are a mainstream therapy for NDO. 7 For sexual health, pharmacological, surgical, and prosthetic strategies have been explored as means to manage erectile dysfunction (ED) in males after SCI, but there are considerable gaps in treatment options for other elements of sexual dysfunction. 11,13 For females with SCI, there is even less research exploring rehabilitation strategies specific to their sexual experiences. 13
When considering injury characteristics, level of injury, and degree of residual functioning are important factors in determining catheterization options, 5 whereas certain catheters (indwelling urethral or suprapubic) are not compatible with surgical and prosthetic treatments for ED because of increased risk of infection. 11 In addition, males with motor-incomplete injuries are more likely to have preserved reflexo- and psychogenic erection suitable for sexual intercourse compared to persons with motor-complete injuries. Similarly, having motor-complete SCI (especially when affecting the sacral segments) also means reduced vaginal lubrication and less chance to achieve orgasm in females. 5
Given the insufficiency of current urogenital management options, safer, less-invasive alternatives are being actively sought, which has directed attention toward exercise-based approaches. In the able-bodied population, pelvic floor muscle (PFM) training (PFMT) programs that aim to increase strength and tonicity of the PFMs have become a popular conservative management strategy for both urinary and sexual impairments. 14 –18 With respect to incontinence, strengthening PFMs increases the amount of pressure these muscles can apply to the urethra to prevent leaks. 19 Further, there is evidence that reflexive contraction of PFMs results in decreased detrusor activity, thereby facilitating bladder filling. 20 Previous work has also demonstrated a link between PFM health and sexual function, where stronger PFMs have been associated with improved sexual desire, lubrication, and orgasm in females, 21,22 as well as more rigid erections, better ejaculation control, and improved orgasm in males. 16,23 Whereas classic PFMT programs consist only of exercises that directly target PFMs (so-called Kegels), PFMs are also engaged with a variety of maneuvers requiring regulation of intra-abdominal pressure.
PFMs coactivate with the abdominal 24 –26 and gluteal 24,27 muscles and are therefore active during exercises that target these muscles (e.g., trunk flexion, abdominal hollowing, and hip extension). Further, evidence has shown that PFMs are engaged during ambulation and other dynamic movements. 28 –31 Although there is little evidence so far that programs focusing on ambulation or coactivation of PFMs improve urogenital outcomes, 19,32 it is possible that activation of PFMs during these tasks may serve as a means to strengthen this muscle group, especially in a population where direct and isolated contraction of PFMs may be difficult.
Whereas the role of exercise on recovery of urogenital function specifically to SCI remains poorly understood, the successful implementation of exercise-based rehabilitation programs (primarily PFMT) in other neurological groups, such as those with multiple sclerosis (MS) or in post-stroke rehabilitation, 33 suggests the possibility for investigation in the SCI population. Given the fact that exercise training is cost-effective, associated with minimal adverse effects, and capable of improving symptoms as opposed to simply managing them, this review aimed to summarize the feasibility (adverse events, dropout rate) and effects of exercise-based therapies as a treatment for urogenital dysfunction and QoL in persons with SCI.
Methods
This review was guided by Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 34 and registered on The International Prospective Register of Systematic Reviews (PROSPERO; CRD42020168080).
Study eligibility criteria and selection
Eligibility criteria were established a priori by identifying participants, interventions, and outcomes. Studies were included if they recruited a sample of adult(s) (>18 years of age) with SCI, delivered an exercise or rehabilitation intervention, and reported pre- and post-intervention measurements of any outcome that assessed LUT function and/or QoL or sexual function and/or QoL (e.g., urodynamic studies, bladder diaries, and questionnaires such as Qualiveen-30, Female Sexual Function Index [FSFI], and International Index of Erectile Function [IIEF]). Exercise and rehabilitation interventions were defined as any structured, activity-based training occurring repeatedly over a period of time with the aim of promoting functional recovery from an impairment attributable to SCI. Examples included, but were not limited to, PFMT, locomotor training (LT), resistance training, and/or aerobic training. Studies were excluded if 1) their participant population included minors (<18 years of age), 2) they only recruited participants with lower motor neuron injuries (e.g., cauda equina or conus injury), or 3) they only reported qualitative outcomes. To enable quality assessment, conference abstracts were excluded unless they provided sufficient data. Otherwise, no restrictions were placed on study type or study design.
Search strategy
Searches were conducted on MEDLINE (Ovid, 1946 to present), EMBASE (Ovid, 1974 to present), and CINAHL (EBSCOhost, 1982 to present). Unpublished studies were not sought. In addition, the CINAHL search was restricted to exclude MEDLINE results. Searches were limited to records published in the English language and with human participants. The last search was run on May 21, 2020, and a sample search strategy for MEDLINE is listed in Table 1.
Search Strategy: MEDLINE (Ovid)
The first author (X.Z.) conducted the search and exported results into Zotero for duplicate screening. After merging duplicates, two reviewers (A.M.M.W., X.Z.) independently conducted an initial screening of titles and abstracts for inclusion according to the eligibility criteria described above. Next, results were compared between the reviewers, and full-text screening was conducted for potentially eligible studies. Disagreements were resolved by consensus. If consensus was not reached, a third reviewer (T.L.) was involved to make a final decision.
Risk of bias analysis
Quality of individual studies was assessed at the study level using the Joanna Briggs Institute (JBI) critical evaluation tools. 35 Study characteristics were assessed based on study design as per JBI guidelines. Results of the JBI evaluation were presented descriptively by summarizing answers to each checklist question. In addition, we searched for registered protocols of included studies on ClinicalTrials.gov, the Health Canada Clinical Trial Database, the European Union Clinical Trials Register, and the Brazilian Clinical Trials Registry to examine biases attributable to selective reporting of outcome measures. Two reviewers (X.Z., A.M.M.W.) conducted the risk of bias assessment, and disagreements between reviewers' judgements were resolved by consensus.
Data extraction
Data were extracted to Microsoft Excel (Microsoft Corporation, Redmond, WA), where we recorded the following information from each study: 1) authors; 2) participant and injury characteristics (including age, sex, and injury level and severity, etiology, and duration); 3) study design (including setting, sample size, interventions, comparison groups, and timeline); 4) feasibility measures; and 5) urogenital outcomes and relevant results. We contacted nine authors 36 –44 for unreported data and/or additional details. Three 37,43,44 of the five authors who replied 37,38,41,42,44 provided the required data within the pre-specified 30-day period. Otherwise, only the data available from the published study were used. One reviewer (X.Z.) independently extracted the data, and a second reviewer (A.M.M.W.) reviewed and verified the extracted data.
Synthesis of evidence
Distinct exercise modalities have been used in persons with SCI, and a variety of outcome measures reflect distinct aspects of urogenital function and QoL. In addition, participant characteristics tended to vary substantially across studies. We therefore undertook the meta-analysis by considering different interventions with individual outcome measures separately. Studies were considered ineligible for the meta-analysis if they 1) reported no common outcome measures; 2) had insufficient sample sizes (e.g., involving only 1 or 2 participant[s]) or insufficient data to calculate effect sizes despite efforts to contact the authors; or 3) had non-comparable interventions. As a result, meta-analysis was only possible for pre-post studies and on two outcomes, both from urodynamics (maximum bladder capacity, bladder compliance). Hedges' g was selected as a summary measure for overall effect sizes considering the adjustment for small sample sizes, and Comprehensive Meta-Analysis version 3 (Biostat Inc., Englewood, NJ) was used to perform the calculations and generate the forest plots. Overall, I2 values were used to evaluate heterogeneity across studies.
Other data summarizing the percentage of participants reporting presence of bladder awareness and urinary incontinence were synthesized descriptively using pre-post plots with weighted averages and standard deviations (when applicable). For subgroup analyses, dropouts, adverse events, and pre-post changes in measurement outcomes were examined descriptively based on sex (male vs. female) and severity of injury (motor-complete vs. motor-incomplete), when possible. Formal statistical analysis was not conducted on these subgroup data because of small sample sizes. We were unable to conduct the analysis based on intervention setting (inpatient rehabilitation program vs. community-based exercise program), as stated in our PROSPERO registration, because of lack of available data. Given that the scope of this review focused on post-intervention changes from baseline, two randomized controlled trials (RCTs) 37,45 were reported and plotted to examine each arm, as opposed to comparing the two arms against one another.
Results
Study selection
The initial search resulted in a total of 6257 records, with 4995 remaining after checking for duplicates. After preliminary screening of titles and abstracts, 300 articles were included for full-text review to determine eligibility. From these, 10 studies 36 –45 fully met the inclusion criteria, and data were extracted for qualitative synthesis, of which two studies 39,42 were included in the meta-analysis. Forty-eight studies were not retrievable, and the remainder were discarded because they did not meet our inclusion criteria. A flow diagram of the study selection process is shown in Figure 1. Among the 10 included studies, there were three RCTs 36,37,45 (including one conference abstract 45 ), two quasi-experimental studies, 39,40 three cohort studies, 41 –43 and two case reports. 38,44 In addition, after personal contact with the author, Baunsgaard 46 provided a previously published study on feasibility reports of their training protocol.
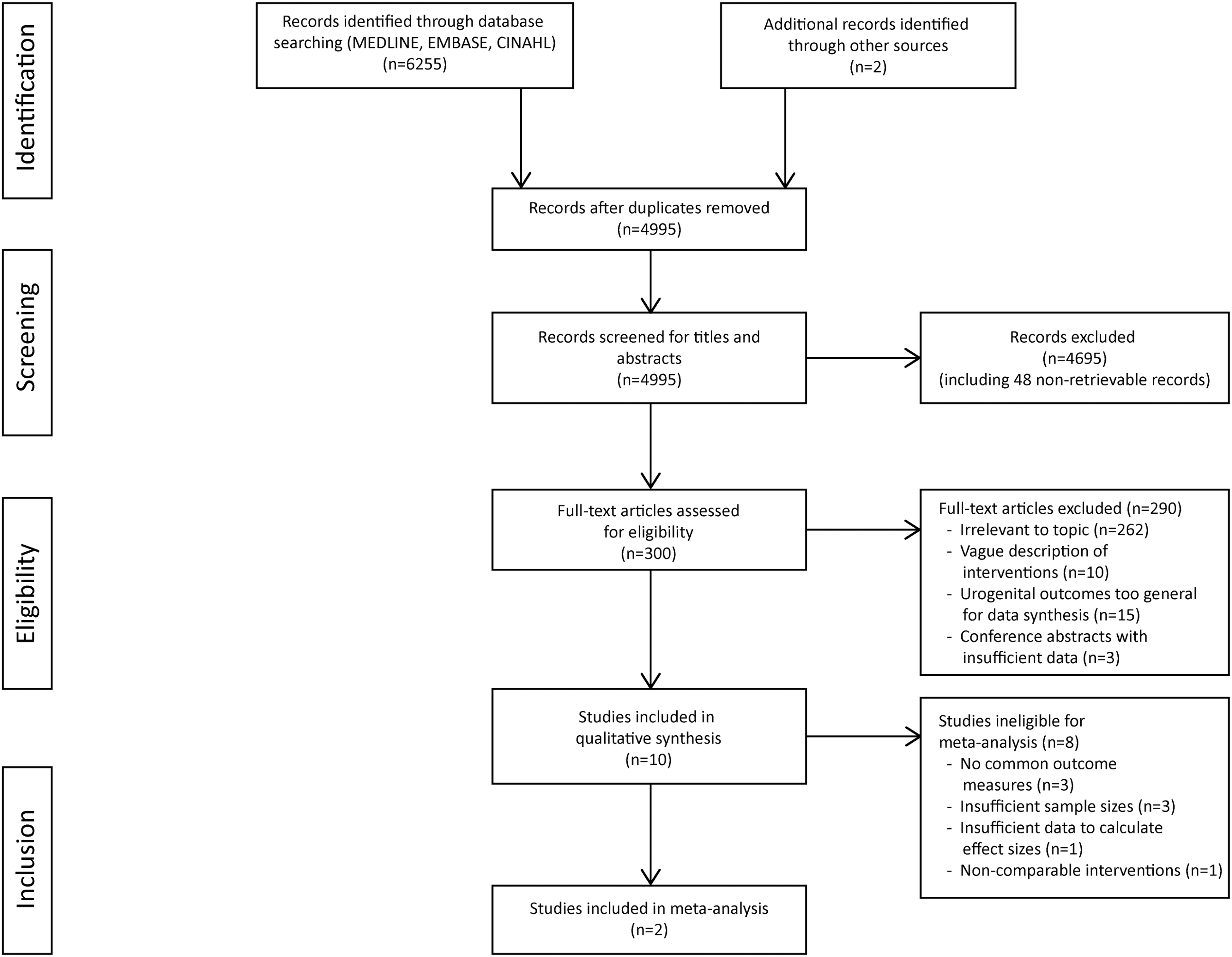
PRISMA flow diagram of study selection process.
Risk of bias analysis
Risk of bias within studies, as assessed by the JBI critical evaluation tools, are summarized in the Supplementary Materials. The overall quality of included studies was relatively low, but there were two cohort studies, 41,42 two case reports, 38,44 and one RCT 36 that were well designed and had most checklist items properly reported. A search of clinical trial registries found two protocol registrations of our included studies, and all outcome measures were reported as planned. 36,42
Study characteristics
Participant characteristics
A total of 228 participants were involved with study sample sizes ranging from 2 to 69. Mean age of participants was 37 years. Cervical (n = 87) and thoracic (n = 110) were the most common levels of injury, and the majority (n = 158) were classified as having a motor-incomplete SCI. Details regarding study and participant characteristics are summarized in Table 2.
Study Characteristics and Interventions
Unless specified elsewise, age and TPI are group mean values, and data were based on participants who completed the training protocol.
Median (interquartile range).
Data for sex, age, and injury characteristics were based on all participants, including 1 participant who dropped out.
AIS, American Spinal Injury Association Impairment Scale; BMI, brain-machine interface; BWS, body-weight supported; BWSTT, body-weight–supported treadmill training; EES, epidural electrical stimulation; ES, electrical stimulation; IVES, intravaginal electrical stimulation; LT, locomotor training; NA, not available; NLI, neurological level of injury; NMES, neuromuscular electrical stimulation; PFBFB, pelvic floor biofeedback; PFMT, pelvic floor muscle training; RCT, randomized controlled trials; TENS, transcutaneous electrical nerve stimulation; TPI, time post-injury.
Intervention
The interventions used in the included studies could be broadly classified into two modalities: PFMT and LT. Three studies 36 –38 examined the effects of PFMT and its variations (i.e., combination with electrical stimulation 36,37 and/or biofeedback 37 ), but training protocols were not consistent across studies. All programs consisted of daily practices, but the total number of contractions, types of exercises (maximal contraction, endurance- or speed-focused), and practice positions (supine, sitting, or standing) differed across studies, and overall length of the intervention varied from 4 to 12 weeks. The other seven studies 39 –45 involved different types of LT, primarily body-weight–supported gait training. The training was done either overground or on a treadmill, and sometimes in conjunction with standing exercises, 42 –44 brain-machine interface (BMI) training, 40 and/or electrical stimulation. 39,44 LT interventions tended to be longer in duration (range, 8 weeks to 28 months), but less frequent (one to five times per week), compared to PFMT (Table 2).
Outcome measures
Details of outcome measures are presented in Table 3. Data related to feasibility were reported or could be inferred in eight studies, 36,38,39,40,42 –46 and measures included adverse events, dropouts, and losses to follow-up.
Adverse Events, Dropout, Urogenital Outcome Measures, and Results
EES, epidural electrical stimulation; FSFI, Female Sexual Function Index; ICIQ-OAB, International Consultation on Incontinence Questionnaire-Overactive Bladder; ICIQ-UI-SF, International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form; IDC, involuntary detrusor contraction; IIEF, International Index of Erectile Function; IVES, intravaginal electrical stimulation; LPP, leak point pressure; LT, locomotor training; LUT, lower urinary tract; MDP, maximum detrusor pressure; NA, not available; NBSS, Neurogenic Bladder Symptom Score; OUP, opening urethral pressure; PFBFB, pelvic floor biofeedback; PFMT, pelvic floor muscle training; Qmax, maximum flow rate; QoL, quality of life; SCI, spinal cord injury; SCIM-III, Spinal Cord Independence Measure; TENS, transcutaneous electrical nerve stimulation; UI, urinary incontinence; UTI, urinary tract infection.
All studies evaluated LUT outcomes through at least one of the following: objective measures of LUT function such as urodynamic studies; measures of LUTS through 24-h pad tests, bladder diaries, or questionnaires; and self-reported bladder-related QoL assessments using questionnaires. Sixteen different urodynamic variables were reported across the included studies. The most commonly reported parameters were maximum bladder capacity, bladder compliance, bladder volume at first contraction, and leak point pressure. Four 38,39,42,44 of the seven studies 36 –39,42,44,45 that involved urodynamics reported bladder filling rates, which varied between 20 and 60 mL/min. Commonly used questionnaires to assess urinary outcomes included The International SCI Data Sets Questionnaires for LUT Function and International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form (ICIQ-UI-SF).
Sexual function and QoL outcomes were only measured in four studies, 37,40,42,43 all with questionnaires (IIEF, FSFI, The International SCI Data Sets Questionnaires for Male Sexual Function, and the Autonomic Standards Assessment Form).
Synthesis of evidence
Dropouts and adverse events
Dropouts and losses to follow-up
Only one of the three included PFMT studies explicitly stated their dropout rates. Elmelund and colleagues reported a dropout rate of 25%, with the primary reason being the demands of participation. 36
With respect to LT, dropout data were available in three studies. 40,45,46 The pilot RCT conducted by Lam and colleagues 45 reported that 1 (of 5) participant dropped out because of fracture unrelated to the intervention; additionally, post-intervention data were missing for 1 participant because of self-reported illness. Shokur and colleagues 40 reported a 12.5% dropout rate, but did not specify reasons, whereas Baunsgaard and colleagues 46 reported a dropout rate of 13.3% with training-related ankle swelling being the most common reason.
Adverse events
None of the studies investigating PFMT reported adverse events. In LT programs, minor skin abrasions were common with initial use of exoskeleton devices, but usually did not result in dropouts. 45,46 Ankle swelling and other medical side effects occurred less often, but were sometimes responsible for terminating participation. 46 In addition, participants experienced symptomatic UTIs that might have been associated with the implant of electrodes for epidural electrical stimulation in one study. 44 All adverse events received early recognition, clear documentation, and appropriate management.
Lower urinary tract outcomes
Lower urinary tract function
Across the three studies that used PFMT interventions, maximum bladder capacity decreased by 67 mL after 12 weeks of PFMT and by 9 mL after PFMT plus intravaginal electrical stimulation (IVES), as measured by voiding diary. 36 In contrast, bladder capacity, as assessed by urodynamics, increased or did not change after a program of the same length, but involving PFMT combined with transcutaneous electrical stimulation (TENS; +26.8 mL) or biofeedback training (+0.6 mL). 37 Shendy and colleagues 37 also measured other urodynamic parameters (maximum flow rate [Qmax], detrusor pressure at Qmax, and bladder volume at first desire to void) and observed significant increases on all measures in the PFMT + TENS group only.
With respect to different variations of LT, programs that involved overground training tended to provide consistent benefits or otherwise have no effect, 40,41,45 whereas treadmill training 42 –45 and addition of electrical stimulation 39,44 produced conflicting results. Urodynamic findings after LT were mixed. Forest plots showed some positive effects on maximum bladder capacity (Hedges' g = 0.50) and bladder compliance (Hedges' g = 0.37), with considerable within-study variability (Fig. 2A,B), but other cystometric measures (maximum detrusor pressure, leak point pressure) remained unchanged 45 or decreased. 42 Bladder volume at first involuntary detrusor contraction was reduced regardless of the type of LT in Lam and colleagues, 45 but increased in another study 39 that utilized gait training with neuromuscular stimulation. However, sample sizes were small and the changes were not significant.

Overall pre-post change in LUT function and symptoms after LT interventions. Effect estimates (Hedges' g) for changes in LUT function in (
Lower urinary tract symptoms
Incontinence symptoms, as assessed by questionnaires, bladder diaries, and pad tests, improved in most cases after PFMT. Two male participants with motor-incomplete SCI reported 0–10% reduction in ICIQ-UI-SF scores after a 6-week PFMT program. 38 In another study 36 involving females with motor-incomplete injuries who received 12 weeks of training, ICIQ-UI-SF scores were lowered by 22% and 17% in PFMT and PFMT + IVES groups, respectively.
Despite differences in training modalities and intervention lengths, fairly consistent improvements were noted in bladder awareness 40 –43 and urine leakage 40 –42,44 after LT, when reported as the number or percentage of participants with awareness/sensation and the number of daily incontinence episodes, respectively. However, there was substantial individual variability, and the overall improvements across studies were minimal (Fig. 2C,D).
Lower urinary tract quality of life
LUT QoL was not assessed in any of the included PFMT studies. With respect to the studies using LT interventions, only one pilot RCT examined LUT QoL with Qualiveen-30 and produced distinct results in the two groups. 45 Three weekly sessions of overground exoskeleton training for 45 min over 12 weeks resulted in neutral or positive changes, but Lokomat training might have had no effect or even worsened the participants' QoL perceptions. However, the results were based on a very small sample of males with motor-complete SCI and should therefore be interpreted with caution. 45
Sexual outcomes
Sexual function
Only one study in the PFMT category examined sexual function outcomes, where participants had significant improvements in ED as measured by IIEF-5 after a 6-week PFMT + TENS program. 37 Among the three LT studies 40,42,43 that assessed sexual outcomes, four elements of male sexual function (ejaculation, sensitivity during sexual intercourse, psychogenic erection, and reflex) and two elements of female sexual function (orgasm, sensitivity during sexual intercourse) were examined. No change in erectile function was observed after a 4-month body-weight–supported treadmill training/standing protocol 42 ; however, minor improvements in genital sensitivity and motor function were possible for both sexes after 120 LT sessions (including standing, stepping, and community integration tasks) 43 or a 28-month LT program combined with BMI (Table 3). 40
Sexual quality of life
Only 1 of the 13 included studies reported sexual QoL changes after LT as reflected by domain subscores in IIEF and FSFI questionnaires. 42 Sexual desire and overall satisfaction scores increased in both males and females, but only the change in sexual desire was statistically significant (Table 3). 42
Subgroup analyses
With respect to urodynamic outcomes, maximum bladder capacity and bladder compliance were commonly measured across sexes and degrees of injury severity. In terms of LUTS, changes in bladder awareness and incontinence episodes were most commonly reported.
Among the different aspects of sexual function and QoL examined by questionnaires, only sensitivity during sexual intercourse was measured in both sexes, and only ejaculation was measured in both injury severity categories. Sexual desire and overall satisfaction data were available from IIEF/FSFI subdomain scores and separated by sex and injury severity.
Given that there was limited information regarding dropouts and adverse events in included studies, we were unable to conduct any sex- or injury-severity–specific analyses. Nonetheless, the pre-post changes based on individual study results were organized into subgroup by sex and injury severity for LUT (Fig. 3) and sexual (Fig. 4) outcomes. These plots are presented for descriptive purposes only to provide an overview of the data found in the literature.
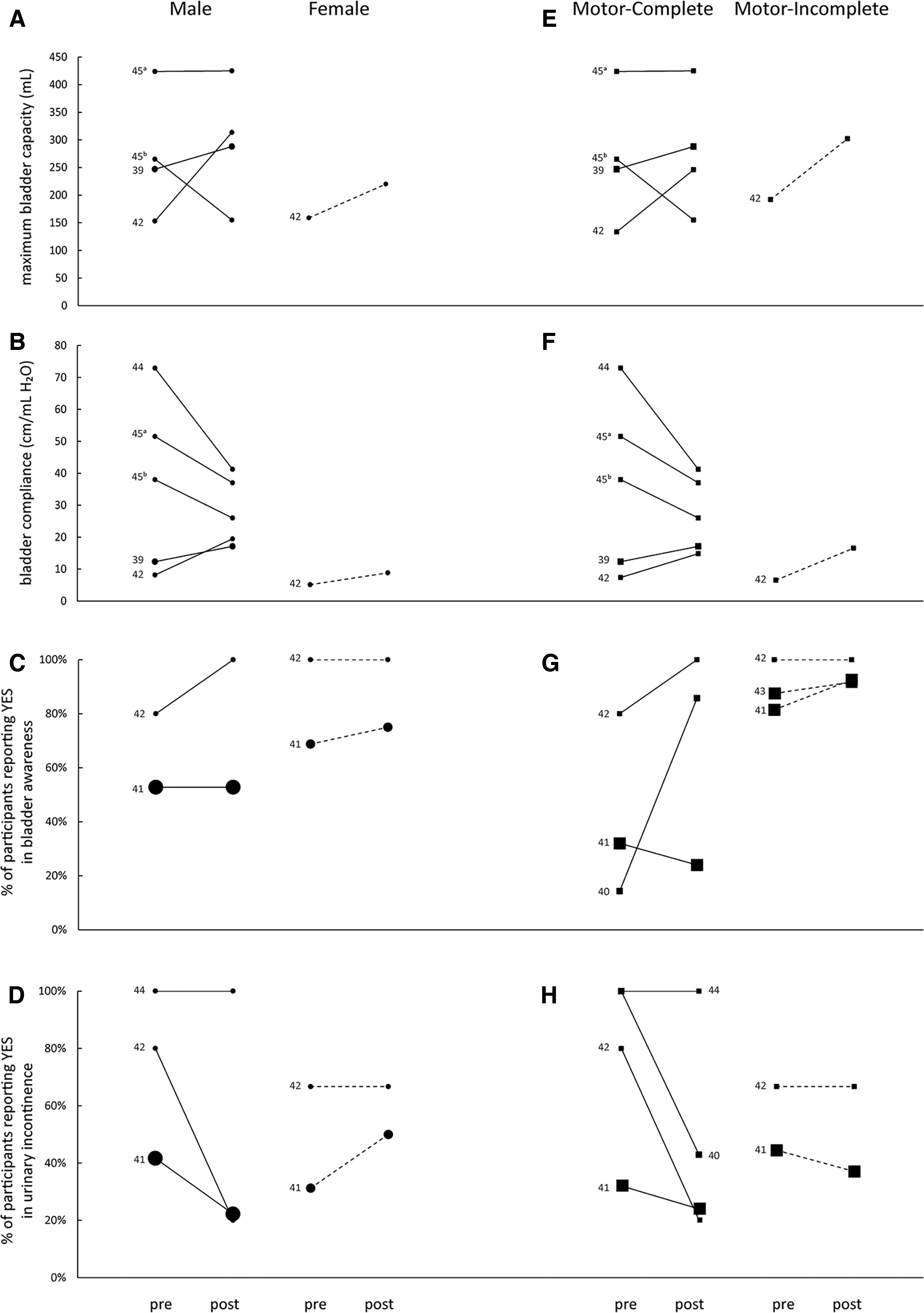
Subgroup analyses of LUT outcomes. Pre-post changes in maximum bladder capacity (

Subgroup analyses of sexual outcomes. (
Discussion
In this systematic review, we examined the effects of exercise training on urogenital function and QoL in persons with SCI. Because of the relatively small number and low quality of the available and included studies, we do not yet have enough evidence to conclude whether there are positive effects of exercise training on urogenital outcomes. PFMT could lead to positive changes, 38 but adjunctive treatments, such as electrical stimulation or biofeedback, may 37 or may not 36,37 bring additional benefits. LT interventions seemed to yield improvements in maximum bladder capacity, bladder compliance, bladder awareness, and incontinence, even though results from other aspects of LUT outcomes were mixed. For sexual health measures, both PFMT and LT were potentially beneficial, even though the data were sparse. 37,40,42,43 More rigorous study designs with larger sample sizes should be considered in future studies; in addition, better documentation of feasibility measures and more standardization in choosing and reporting urogenital outcomes are important for further investigation of the use of exercise-based interventions in people with SCI.
Mechanisms underlying exercise training
Pelvic floor muscle training
The mechanisms behind PFMT on urogenital health have been extensively investigated. It is widely accepted that engaging in a PFMT program improves the strength and tonicity of the PFM to support the bladder neck, 19 and that PFM contractions may inhibit detrusor activity. 47 For sexual function, PFM strength and contraction are likely to play a role in supporting relevant organs (e.g., clitoral erectile tissue, base of penis) and facilitating sexual responses such as orgasm. 48,49 In comparison to LT, the mechanisms and intention behind PFMT are more directly linked to urogenital function.
Locomotor training
The neurophysiology underlying the potential effects of LT on urogenital function is not well understood. Previous investigations of standing training after SCI suggested that increases in bladder pressure while in the upright position helped improve bladder emptying, 50 and it is possible that the effect of upright posture on bladder pressure from standing also extends to LT. In addition, peripheral sensory inputs during task-specific gait training activates the lumbosacral spinal segments, which are also involved in controlling bladder and sexual functions. Thus, LT may indirectly benefit the neural circuitry of the urogenital system through afferent feedback pathways. 42 There is also evidence from the able-bodied literature that the PFMs are active during gait activities 19,32 ; however, given that the PFMs are functionally involved in postural control, 31 if they are weak or unable to contract in the correct sequence (e.g., because of SCI), LT may place too much demand on these muscles and offset the potential positive effects. Therefore, it remains unclear whether activation of PFMs during ambulation could act as a means to train the PFMs and ultimately improve urogenital outcomes.
The role of cognitive engagement
Besides the different neurophysiological mechanisms, the degree of cognitive engagement also differs between these two intervention types. In PFMT, persons are instructed to actively engage in, and explicitly attend to, the contractions of the PFMs. 19 In LT, however, the emphasis tends to be on maintaining upright posture and producing the locomotor pattern as opposed to directly focusing on the PFMs or other urogenital structures. We do not have adequate evidence to conclude the superiority of one method over the other, but these reasons could partially explain why LT protocols tended to be longer yet failed to produce consistently desirable outcomes. Collectively, this implies that a regular LT program of <12 weeks 41,45 might be too short to elicit noticeable positive changes, and that novel forms of LT involving more task-specific sensory stimuli and cognitive engagement require further investigation. Nonetheless, it should be acknowledged that although the urogenital-specific improvements may not be obvious, there is considerable evidence that LT still brings positive changes to other bodily systems (e.g., musculoskeletal, cardiorespiratory, and emotional well-being) for persons with SCI. 51
Severity of injury
Even though evidence was limited to make decisive comparisons between motor-complete and motor-incomplete SCI in terms of urogenital responses to exercise training, our preliminary findings did reveal the potential for persons with various levels of injury severity to improve. All of the participants involved in the selected studies had suprasacral SCI, indicating that they would experience overactivity-type bladder dysfunction. 7,52 In this context, exercise training may facilitate the recovery of bladder function by two pathways. First, local neuromodulation during PFMT and processing of sensory stimuli during LT might help stimulate reflexive inhibition and downregulation of detrusor overactivity. 53 In addition, PFMT could improve voluntary control through positively modulating the strength and endurance of PFM contractions and thereby reducing incontinence episodes. This latter point should appear self-evident in persons with motor-incomplete SCI attributable to the presence of sacral sparing, 1 which accounts for the majority of the participants involved in this review. However, the rehabilitation potential for persons with motor-complete SCI should not be underestimated. Previous studies have shown detectable trunk muscle activation below the level of injury using electromyography (EMG) in response to balance perturbations, attempted voluntary activation, transcranial magnetic stimulation (TMS), and exoskeleton-assisted overground walking in persons with cervical or thoracic motor-complete SCI. 54 –56 Even though early observations were restricted to the abdominal muscles and diaphragm, recent work has demonstrated that PFM activity can be detected in persons with motor-complete SCI by surface EMG through coactivation of trunk muscles and by the presence of motor-evoked potentials in response to TMS over the primary motor cortex. 57 Collectively, these findings imply the potential preservation of PFM innervation and thus residual cortical control over and trainability of the PFM, even for those with motor-complete SCI. Therefore, there are potential opportunities and conceptual bases for exploring exercise-based interventions for both motor-complete and -incomplete SCI.
Sex considerations
Males and females might respond differently to the same exercise intervention, 40,43 but very limited data were available to draw definitive conclusions, especially for females. Previous research using PFMT interventions has been primarily conducted in females for the prevention and treatment of pregnancy-related incontinence. 14,58 Similarly, most research exploring PFMT in other neurological patient groups (e.g., MS, stroke survivors) has also primarily focused on females. 33 However, the majority of the SCI population is male, 59 and it is therefore of importance to evaluate whether PFMT can provide the same degree of efficacy in this population as has been shown in females. Two 37,38 of the three studies using PFMT (and its variations) in our review involved male participants; in fact, across the included studies, there were a comparable number of males (n = 32) and females (n = 28) who received PFMT. Given the improvements in ED 37 and improvements or stability in LUTS, 36,38 we may infer that males with SCI could be as responsive to PFMT as females. We also aimed to collect and analyze data on aspects of feasibility (adverse events, dropout rates, and loss of follow-up) divided by sex, based on the assumption that males and females might have different experiences and concerns when receiving the same treatment.
Yet, despite the encouraging fact that, overall, dropout rates were generally low, the one PFMT RCT 36 that reported a 25% dropout enrolled only female participants, and the other RCT 37 comparing different forms of PFMT enrolled only male participants and did not report their dropout rate. Thus, we were not able to evaluate whether there are any discernible sex differences with respect to feasibility measures. Nonetheless, these findings highlight the importance of explicit focus and study design based on sex for future research.
Issues in the current literature
Variations in training protocols
Within the two broad intervention categories, there was substantial variation in training protocols and modalities. Despite the fact that PFMT alone yielded some positive effects on LUT function in two 36,38 of the three studies we examined, the evidence was too sparse to compare the superiority of different modes of PFMT for persons with SCI. Only two studies 36,37 aimed to compare the effects between different types of PFMT, but they used different PFMT protocols in terms of length and types of exercises, and one included exclusively female participants 36 whereas the other only included males. 37 Although both involved electrical stimulation as the experimental group, different electrode placements (intravaginal vs. transcutaneous) and stimulation protocols (intermittent vs. continuous) were used. 36,37
There is some evidence from the wider literature that the added neuromodulation provided through stimulation could benefit people with neurogenic bladder symptoms, 60 but our results showed that there is not enough evidence to make similar conclusions for people with SCI at this point. Similarly, LT programs used different exoskeleton and body-weight–supported training interventions. They also involved various adjunctive treatments, including standing exercises, 42 –44 virtual reality devices, 40 neuromuscular electrical stimulation, 39 and epidural stimulation, 44 which undermined our ability to synthesize the results. It is unclear what modality and frequency of LT training, and subsequent adjunctive treatments, may provide the best mechanism to alleviate urogenital dysfunction.
Variations in outcome measures
Lower urinary tract outcomes
Although LUT outcomes were comprehensively assessed and reported, they were measured inconsistently across the 13 studies and thus further complicated the highly variable results. Self-reported changes measured by bladder diaries and/or questionnaires tended to improve after training in the majority of the participants; however, the objective urodynamic findings were less consistent. Although patients' perceived benefits are clinically meaningful, more objective measures are essential in understanding the mechanisms of underlying physiological changes produced by training. There has been standardization of urodynamic practices for able-bodied persons and persons with SCI. 61,62 According to the International Continence Society, a standard urodynamic test should include uroflowmetry, transurethral cystometry, and a pressure-flow study. These results should be reported at minimum and preferably supplemented with EMG, imaging, or urethral pressure measurements. 62 All of our included studies that involved urodynamics stated that they followed good practice guidelines, 37,39,42,44,45 but different studies chose different parameters and bladder filling rates, which might partially explain the heterogeneity of urodynamic findings and our limited ability to generate overall effect sizes.
Sexual outcomes
Sexual outcomes were considerably underassessed (reported in only 4 of the 13 studies), and different instruments were used to measure these outcomes. Specifically, we found two studies using IIEF questionnaires, but one used the original version 42 whereas the other chose the short form (IIEF-5). 37 Given that most participants in Hubscher's study 42 reported no sexual activity, there were no common questions between studies. For studies using The Autonomic Assessment Form 43 and International SCI Data Sets, 40 sexual and reproductive functions were examined from a wide range of aspects with limited overlap, leaving the overall change pattern difficult to interpret. There was evidence supporting the use of IIEF and FSFI as preferred instruments in the context of SCI, but they still failed to capture certain aspects of human sexual function (e.g., ejaculation in males) 63 and were not widely used in included studies. Therefore, more investigation in sexual function questionnaires for SCI and more standardization in choosing and reporting questionnaire outcomes in clinical practice should be considered.
Overall quality of included studies
Of the studies included in this review, the overall quality was relatively low. The most common deficits in study design among the RCTs were associated with blinding and intention-to-treat analysis; however, considering the nature of exercise training, double-blinding is not always possible. The major problem associated with the two quasi-experimental studies 39,40 and three cohort studies 41 –43 was the lack of a matched control group, making them vulnerable to the potential impact of confounding variables. In addition, most of the included studies had very small sample sizes with large intersubject variability, which limited our ability to confidently attribute the changes in urogenital outcomes to the exercise training or make any generalization to the broader SCI community.
Limitations
The major limitation of this review was that the analysis was based entirely on pre-post interventions as opposed to RCTs or studies with well-matched control groups. This may introduce substantial biases, and our results should thus be interpreted with caution. However, this was unavoidable because of the understudied nature of the topic and highlights the need for further investigation using high-quality study designs. Unpublished studies were not systematically sought, making our results subject to some degree of publication bias. In addition, as a result of the heterogeneity of LUT outcome measures, our ability to synthesize overall effect sizes were greatly undermined. Even though combining different subjective and objective measures could possibly offer a more thorough view of the bladder outcomes of interest, the lack of standardization when reporting and summarizing the results is problematic. It should also be noticed that very little data were found for exercise-related sexual function/QoL changes in persons with SCI, leaving the topic open for future research. Finally, our ability to conduct subgroup analyses based on sex and injury severity, and make direct comparison between the effects of PFMT and LT interventions, was limited by data quality and availability.
Conclusion
In summary, no clear conclusion could be made regarding the effects of exercise training on urogenital outcomes because of the low quality and small sample sizes of the available studies. However, our findings support further investigations of various forms of PFMT and gait training as a strategy of choice, given the low risk of adverse events and potential improvements in urogenital outcomes in both sex and injury severity groups. To better understand the role of exercise training and responses of persons with different injury characteristics, standardization of outcome measures is recommended, and studies with more robust design and larger sample sizes are needed, especially in the domain of sexual function and QoL.
Footnotes
Acknowledgments
We thank Dr. Janice Eng for her comments on earlier drafts of the manuscript for this article and the Spinal Cord Injury Research Evidence (SCIRE) Team for their guidance and support with the search strategies.
Authors' Contributions
X.Z. conducted the systematic search, performed record screening, study appraisal, data extraction, synthesis and interpretation, and drafted and revised the manuscript. A.M.M.W. performed study screening and appraisal, verified data extraction, and made significant contributions to drafting and revisions of the manuscript. T.L. conceived of the study and made significant contributions to the interpretation of the data and revisions of the manuscript.
Funding Information
This work was supported by the Canadian Institutes of Health Research (PJT-166040). X.Z. was supported by a UBC Work Learn International Undergraduate Research Award.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.