
Abstract
Persons living with spinal cord injury (SCI) are potentially at risk for severe COVID-19 disease given that they often have decreased lung capacity and may lack the ability to effectively evacuate their lungs. Known risk factors for negative outcomes after COVID-19, such as obesity, diabetes, and cardiovascular disease, disproportionally affect people with SCI and raise concerns for the mortality risk among persons with SCI. A rapid systematic review of English, Spanish, Portuguese, and Chinese literature on COVID-19 and SCI was performed using the keywords “spinal cord injury” and “COVID-19.” We included studies that provided information on clinical presentation, characteristics, course, and outcomes of COVID-19 disease in SCI. We excluded studies on patients who did not have an SCI before severe acute respiratory syndrome coronavirus-2 infection or did not report clinical information. We included 10 studies in total: nine studies with a total of 171 patients and a survey study of 783 healthcare professionals. Fever (74%), cough (52%), and dyspnea (33%) were the most frequently reported symptoms, and 63% showed abnormalities on X-ray imaging. In the included case series and reports (N = 31), only 1 patient required mechanical ventilation, but 3 patients died (10%). The mortality rate in a large registry study (N = 140) was 19%. Clinical presentation of COVID-19 in SCI patients was similar to the general population, and though adverse events and intensive care unit admission were low, the mortality rate was high (10–19%). No prognostic factors for severe disease or mortality could be identified. Registration (PROSPERO): CRD42020196565.
Introduction
With >63 million cases worldwide as of December 1, 2020, 1 severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection leading to COVID-19 disease has had an immense impact since it first emerged in Wuhan, China in December 2019. 2 Researchers and clinicians have identified the clinical characteristics as well as risk factors for disease severity of COVID-19. Patients present with fever (79–94%), cough (57.6–79.0%), 3 –7 and other flu-like symptoms, such as fatigue (23.0–44.5%), dyspnea (21.4–45.6%), myalgia (15.0–21.1%), sore throat (11%), and headache (8%). 3 –7 Infection with SARS-CoV-2 can give rise to a variety of other symptoms, from gastrointestinal (GI) issues like diarrhea, nausea, and vomiting 4,7 to neurological sequelae ranging from polyneuropathy to post-viral Guillain-Barré syndrome. 8 –12
In more-severe cases, COVID-19 can lead to acute cardiac injury, coagulopathy, acute cardiac or renal failure, and acute respiratory distress syndrome (ARDS). 3,4,6 These severe complications may result in intensive care unit (ICU) admission in 18.0–20.3% of cases and correspond to an ICU mortality rate of 13.9%. 4 A total case-mortality rate is estimated at 2.0–4.4% 3 whereas a significantly higher mortality rate of 25.5% has been reported for the most critically ill patients. 5 Identifying the response of vulnerable groups to COVID-19 will be important in order to prevent suffering and unnecessary deaths.
Persons with spinal cord injury (SCI) are potentially at risk for severe COVID-19 disease for a number of reasons. 13 People with higher SCI lesions often have decreased pulmonary capacity and may lack the ability to effectively clear their lungs. 14 Persons with higher cervical lesions may develop respiratory insufficiency and become ventilator dependent on a long-term basis, requiring intensive nursing care. 15 Persons with SCI often have sedentary lifestyles and are at higher risk for chronic health conditions, such as obesity, 16 diabetes, 17 and cardiovascular disease, 18,19 compared to persons without physical disabilities. Further, there is pre-clinical evidence that persons with SCI may have a compromised immune system, 20,21 making them vulnerable to infection and adding to their risk of severe COVID-19 disease. 6,22,23 Additionally, presentation of symptoms of COVID-19 in persons with SCI may be different from persons without SCI, which may cause a delay in SARS-CoV-2 testing and the timely start of treatment. 24,25
Given that there are concerns about the possibility of a different clinical presentation of COVID-19 in persons with SCI, as well as evidence that those with the aforementioned chronic diseases have an increased risk of severe disease, ICU admission, and mortality, 5,6 it is important to assess clinical evidence on COVID-19 in persons with SCI. To aid in clinical care for this potentially vulnerable group, we should review clinical characteristics and course, as well as mortality rate and risk factors, for disease severity and mortality in this population. In this rapid review, we systematically searched the available literature on COVID-19 and SCI thus far to provide an overview of the clinical presentation, course, and outcomes of COVID-19 in persons with SCI and identify risk factors for severe disease- and COVID-19-related mortality.
Methods
Protocol and registration
The protocol for this rapid review follows the recommendations by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement 26 and has been registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42020196565).
Eligibility criteria
We included all published studies thus far on the clinical characteristics, course, and outcomes of COVID-19 disease in persons with SCI. We were specifically interested in studies on risk factors for severe COVID-19 and COVID-19-related mortality in the SCI population.
Information sources and search strategy
For this rapid review, we searched the Chinese, Spanish, Portuguese, Latin-American, and English literature on SCI and COVID-19. The Chinese literature was searched because of the origin of the SARS-CoV-2 virus and first epidemic being in Wuhan, China. Most early scientific publications on COVID-19 in the general population come from China. The Spanish literature was searched to reflect Spain and Spanish-speaking South American countries, whereas the Portuguese/Latin-American literature was searched to capture cases related to the high incidence in Brazil. We assumed that most literature from Italy would be published in English and thus identified through our English search strategy.
We searched the Chinese literature (up to August 16, 2020) by searching “Google Scholar (Simplified Chinese)” and the “Chinese Medical Journal Network” (中华医学期刊全文数据库), using the keywords “COVID-19” and “Spinal Cord Injury.” Additionally, we searched the Spanish, Portuguese, and Latin-American literature (up to November 30, 2020) by searching SciELO, LILACS, Redylac, E-revistas, Imbiomed, and Google Scholar (Portuguese and Spanish), using the Spanish and Portuguese keywords “spinal cord” or “paraplegia” or “quadriplegia” or “tetraplegia” and “COVID” or “corona virus” or “SARS-CoV-2.” Finally, we searched the English literature (up to November 30, 2020) by searching MEDLINE (PubMed), MEDLINE (Ovid), Embase (Ovid), CINAHL (EBSCOhost), Cochrane Central Register of Controlled Trials (CENTRAL), and Joanna Briggs Institute Evidence Based Practice Database (Ovid) using the keywords “spinal cord injury” or “SCI” or “paraplegia” or “quadriplegia” or “tetraplegia” and “COVID-19” or “SARS-CoV-2” or “corona virus.” See Supplementary Appendix SA1 for the full search strategies used for each database.
Study selection
We included publications in Mandarin, Spanish, Portuguese, or English published in 2019 or 2020 on COVID-19 disease in persons with SCI that reported on clinical characteristics (symptomatology, imaging, laboratory, and microbiological data), clinical course, and/or clinical outcomes. We included cohort studies, case-control studies, cross-sectional studies, case series, and case reports. We excluded all non-clinical study types that did not include a case report or series, as well as studies on persons who developed SCI, infection (myelitis, spondylodiscitis), or neurological dysfunction (including post-viral Guillain-Barré disease) after being infected with COVID-19.
Data extraction
After the search, the first author (B.H.) screened the Chinese, Spanish, and Portuguese literature with assistance from affiliated researchers who are native speakers. All English-identified records were collated and uploaded into Covidence, 27 duplicates were removed, and title and abstract screening was done by the first author (B.H.). Full text eligibility was screened by a minimum of two independent reviewers (B.H., M.Q.). The full texts of potentially relevant studies were reviewed using the inclusion and exclusion criteria. Conflicts were resolved through discussion between the reviewers. The first author (B.H.) extracted all relevant data from the included articles, and a second reviewer (M.Q.) verified the extracted data. Differences were resolved through discussion until consensus was achieved.
Assessment of methodological quality and risk of bias
As per our protocol, critical appraisal of individual studies was done using the Joanna Briggs Institute critical appraisal checklist for case-control series, case series, and case reports. 28 Additionally, we used the risk-of-bias tool for studies of overall prognosis by the Cochrane Prognosis Review Methods Group to assess risk of bias across different study types. 29
Statistical analysis
Extracted data was organized in tabular form using Excel (Microsoft, version 2012), after which total numbers and percentages were calculated for all measures. We calculated the median age and interquartile range using SPSS statistics for Windows version 26 (IBM Corp., 2019). No meta-analysis or formal statistical tests for significance or were performed.
Results
Study selection and characteristics
We identified 2221 articles using our search strategies in Chinese, Spanish, Portuguese, and English. One additional case report was sent to us by a colleague. After screening by abstract and title, 26 articles were selected for full text assessment and assessed for eligibility. We excluded 11 studies that did not include clinical information on COVID-19 disease in SCI patients and five case reports that were on COVID-19 and SCI, but the SCI occurred after the infection.
Ten studies with a total of 171 patients were included for analysis. We included a case-control series from Italy, 30 a case series from Spain, 31 four case reports from Thailand, 32 Italy, 33 Turkey, 34 and the United States, 35 and two editorial pieces containing short case reports from Spain 36 and from the United States. 37 The total number of patients in the case-control series, case series, and case reports is 30. We also included a cross-sectional registry study of the Veterans Health Administration Registry (United States) 38 of 140 SARS-CoV-2+ SCI patients and an international cross-sectional survey study among 783 healthcare professionals working in SCI care from the United States 39 (see Fig. 1). Articles were published between March 30, 2020 and August 28, 2020.
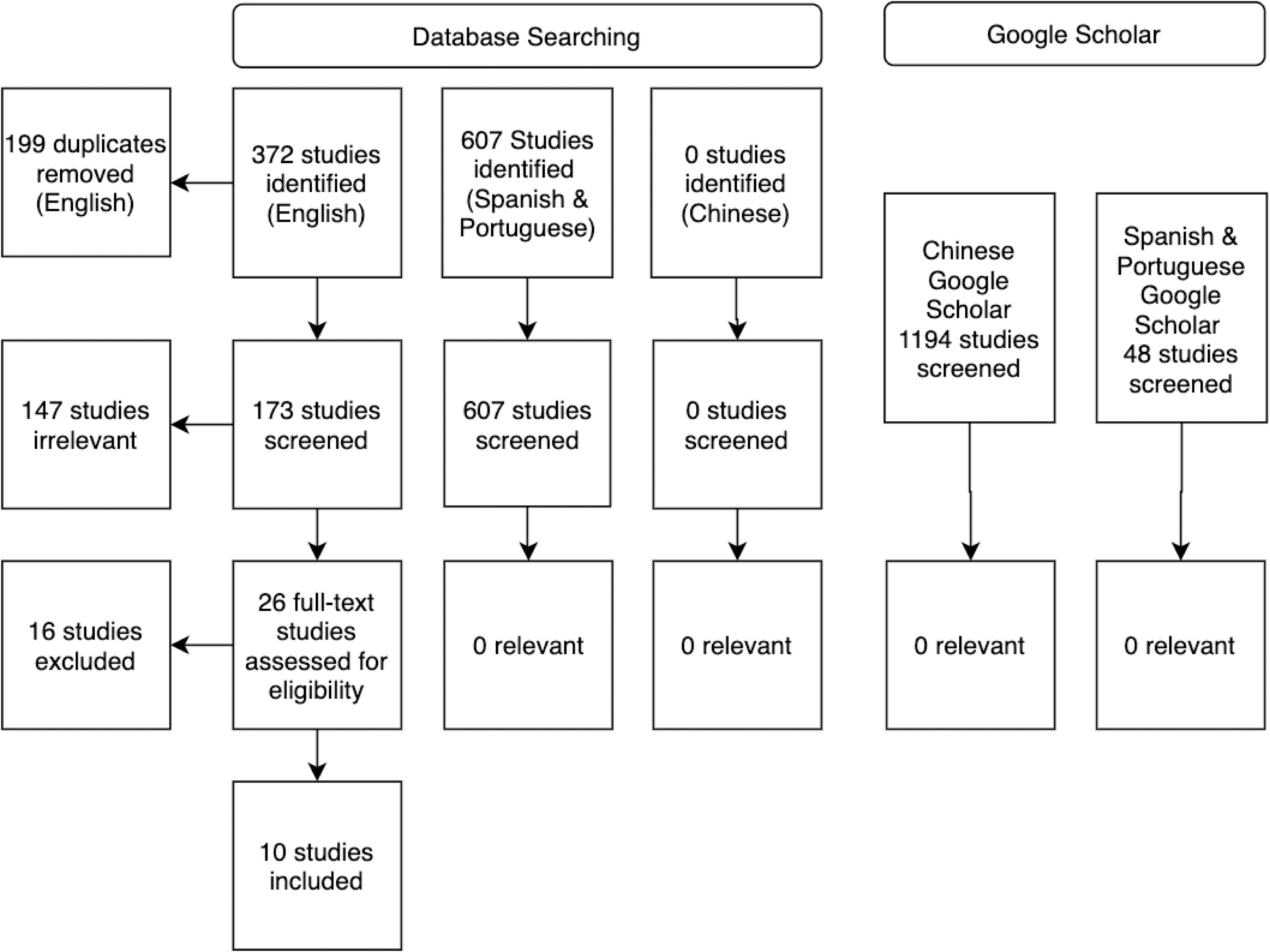
Flow diagram of article selection process.
Quality of evidence and risk of bias
Overall, quality was high for all included studies except the short case reports in the editorial pieces. 36,37 Risk-of-bias assessment showed high risk of bias, with all studies being clinical samples with no blinded study designs, and most studies were descriptive retrospective studies with incomplete reporting of data. Results are summarized in Supplementary Appendix SA2.
Case-control series, case series, and case reports
Most cases were male (22 of 28; 79%) and had a chronic SCI (12 of 15; 80%) and a high level of injury, with 16 of 29 cervical lesions (55%) and 12 of 29 thoracic lesions (34%; see Table 1). Average age of participants in the case reports that specifically reported age was 48 years (interquartile range [IQR], 41-57); 2 cases were reported as being >80 years of age, but did not report age specifically. Average ages in the case-control series 30 and case series 31 were 58 (IQR, 53.5–59.0) and 68 (IQR, 34–75), respectively. Race was not reported in the case-control series, case series, and case reports. Fourteen of 26 (54%) had a motor complete lesion, classified as American Spinal Injury Association (ASIA) Impairment Scale (AIS) A or B. The most prevalent comorbidities were obesity (11 of 25; 42%), dyslipidemia (9 of 26; 35%), metabolic syndrome (8 of 26; 31%), hypertension (4 of 26; 15%), and diabetes (4 of 26; 15%). Four of 26 patients had a history of smoking (15%), and 3 of 26 were current smokers (12%).
Demographics and Medical History
Metabolic syndrome criteria include BMI ≥ 22 and two or more of the following features: triglycerides ≥ 150 mg/dL (or current treatment), HDL < 50 mg/dL, hypertension (or current treatment), fasting glucose ≥ 100 mg/dL, or diabetes mellitus type, ASIA, American Spinal Injury Association; SCI, spinal cord injury, UTI, urinary tract infections.
The most prevalent clinical manifestations of COVID-19 were fever (20 of 27; 74%), cough (14 of 27; 52%), dyspnea (9 of 27; 33%), and fatigue (6 of 27; 22%). Six of 27 cases (22%) were asymptomatic (see Table 2). Most cases had a Modified Early Warning Score (MEWS) of <3 points (18 of 24; 75%), corresponding with less-severe disease. A majority showed abnormalities on X-radiography imaging (17 of 27; 63%). Twelve of 27 (44%) showed a ground-glass pattern on either X-radiography or computed tomography imaging, a total of 6 of 27 patients showed signs of pneumonia (22%), and 1 patient showed pleural effusion (4%). Elevated C-reactive protein was the most prevalent laboratory finding (10 of 11; 91%), followed by lymphocytopenia (6 of 11; 55%). A diagnostic delay was reported between the first symptoms and testing positive for SARS-CoV-2 that varied between 1 and 14 days, with a mean of 4 days (IQR, 1–10) in the case series 31 by Rodríguez-Cola and colleagues 31 (N = 7) and 1, 7, 13, and 14 days in the case reports that reported time between first symptoms and SARS-CoV-2 test. Diagnostic delay was not reported in the case-control series by D'Andrea and colleagues 30 (N = 15), in the case report by Pisano and colleagues, 35 and the short case reports (N = 4) by Sánchez-Raya and Sampol. 36
Clinical Characteristics
GI, gastrointestinal; MEWS, Modified Early Warning Score; CRP, C-reactive protein.
Treatment and clinical outcomes are summarized in Table 3. Thirteen of 19 patients (68%) received hydroxychloroquine treatment, and 11 of 19 patients (58%) received either antivirals, azithromycin, or anticoagulants, not always in that combination. In the series by D'Andrea and cllleagues, 30 hydroxychloroquine, azithromycin, and anticoagulants were given to all symptomatic patients (10 of 15; 66%). Twelve patients received anticoagulants (63%), among them a person with an acute non-traumatic SCI who developed a bilateral pulmonary embolism and extensive bilateral lower-extremity deep vein thrombosis under chemoprophylaxis, likely related to the acute SCI as well as to hypercoagulability, which is associated with COVID-19 infection. 35 Almost one half of the cases required low-flow oxygen treatment (14 of 30; 47%), and 1 person required high-flow oxygen therapy (1 of 30; 3%). One person needed invasive ventilation and ICU admission. 34
Treatment and Outcomes
Other includes enteric nutrition, furosemide and IV immunoglobulin; ICU, intenstive care unit; MICU, medical intensive care unit; CCU, critical care unit.
The mortality in this series of 31 patients was 3 (10%), which included 2 SCI patients 80+ years of age with central cord lesions and relevant comorbidity 36 and a 28-year-old previously healthy male with an acute complete cervical SCI case who died of acute cardiac arrest. 32 The patient died 10 days after undergoing anterior cervical discectomy and fusion with plates and screws for a C5–C6 burst fracture and subsequently developing a mild COVID-19 pneumonia. The presumed cause of death was cervical spinal injury post-surgery, but no autopsy was performed because of safety concerns during the COVID-19 pandemic.
Cross-sectional studies
We identified two cross-sectional studies that added to the literature on symptomatology 39 and mortality rate. 38
Stillman and colleagues 39 did an international survey (N = 783) on all six continents among participants who self-identified as physicians (67%), therapists (13.1%), nurses (8%), and researchers (5.7%), which showed that 5.8% of respondents had tested their outpatients with SCI or disease (SCI/D) for COVID-19 and 4.4% had had a patient with SCI/D and the virus. Most respondents (53.3%) reported that only persons with symptoms were being tested, and a minority (29.9%) said that no screening occurred in their region. The most commonly listed presenting symptoms were fever (86.2%), shortness of breath/dyspnea (62.1%), body aches/worsening pain (20.7%), sweats (20.7%), and chest pain (13.8%). Moreover, 10.3% reported that their patients with SCI/D and COVID-19 had presented with an increase in spasticity, 6.9% reported that their patients with a fever with shivering chills, and 6.9% that their patient had been asymptomatic. A number of respondents (20.7%) replied that their patients had used over-the-counter medications for symptom relief, and 27.6% replied that their patients had been on hydroxychloroquine and/or azithromycin.
Burns and colleagues 38 retrospectively analyzed the Veterans Health Administration registry to calculate the case fatality rate of patients with SCI/D who tested positive for SARS-CoV-2 and were enrolled in their care plan in the period March 9 and June 30, 2020. A total of 140 of 17,452 (0.94%) veterans with SCI/D tested positive for SARS-CoV-2 in the United States. Their mean age was 67 years (standard deviation, 12) and more than one half were registered as Caucasian (80 of 140; 57%), 36% as African American (50 of 140), and 7% as other/declined/unknown. Injury classifications were recorded for 82 patients: 13 patients had a C1–C4 tetraplegia AIS A–C (16%), 14 had C5–C8 tetraplegia AIS A–C (17%), 15 had paraplegia AIS A–C (18%), and 40 were AIS D (49%). Twenty-six of 140 SARS-CoV-2-infected patients had died (19%; 95% confidence interval [CI], 13-26). Among veterans with SCI/D who tested positive for SARS-CoV-2, the case fatality rate was 19%, 2.4 times higher than the non-SCI/D population of which 1564 of 20,369 non-SCI/D veterans who tested positive for SARS-CoV-2 had died (case fatality rate, 7.7%).
Discussion
Based on the 31 patients documented in the case series and reports, 140 patients involved in a cross-sectional study and the survey of 783 clinicians, the clinical presentation of COVID-19 in SCI patients is similar to the general population 4, (see Figs. 2 and 3). Most SCI patients in this review showed signs of fever, which alleviates the concern that thermodysregulation might mask fever in SCI patients who contract the disease. 24 Half of the patients in our review had a cough, which is slightly lower than the reported 57.64–65.7% 3 in the general population. Less patients in our review showed dyspnea than in the general population, but the cross-sectional results show that healthcare professionals do see shortness of breath in 62.1% of SCI/D patients with COVID-19. 39 Even though for most patients in these case series and reports no secondary health effects specific to SCI were reported, the survey study by Stillman and colleagues 39 shows that 10.3% of patients reported an increase of spasticity and 20.3% reported body aches/an increase in pain, which indicates that an increase in spasticity and/or pain is part of the presenting symptoms of COVID-19 disease in SCI patients. Though partially reported, the available laboratory and imaging findings in this review do not deviate from those of the general population. 4,41
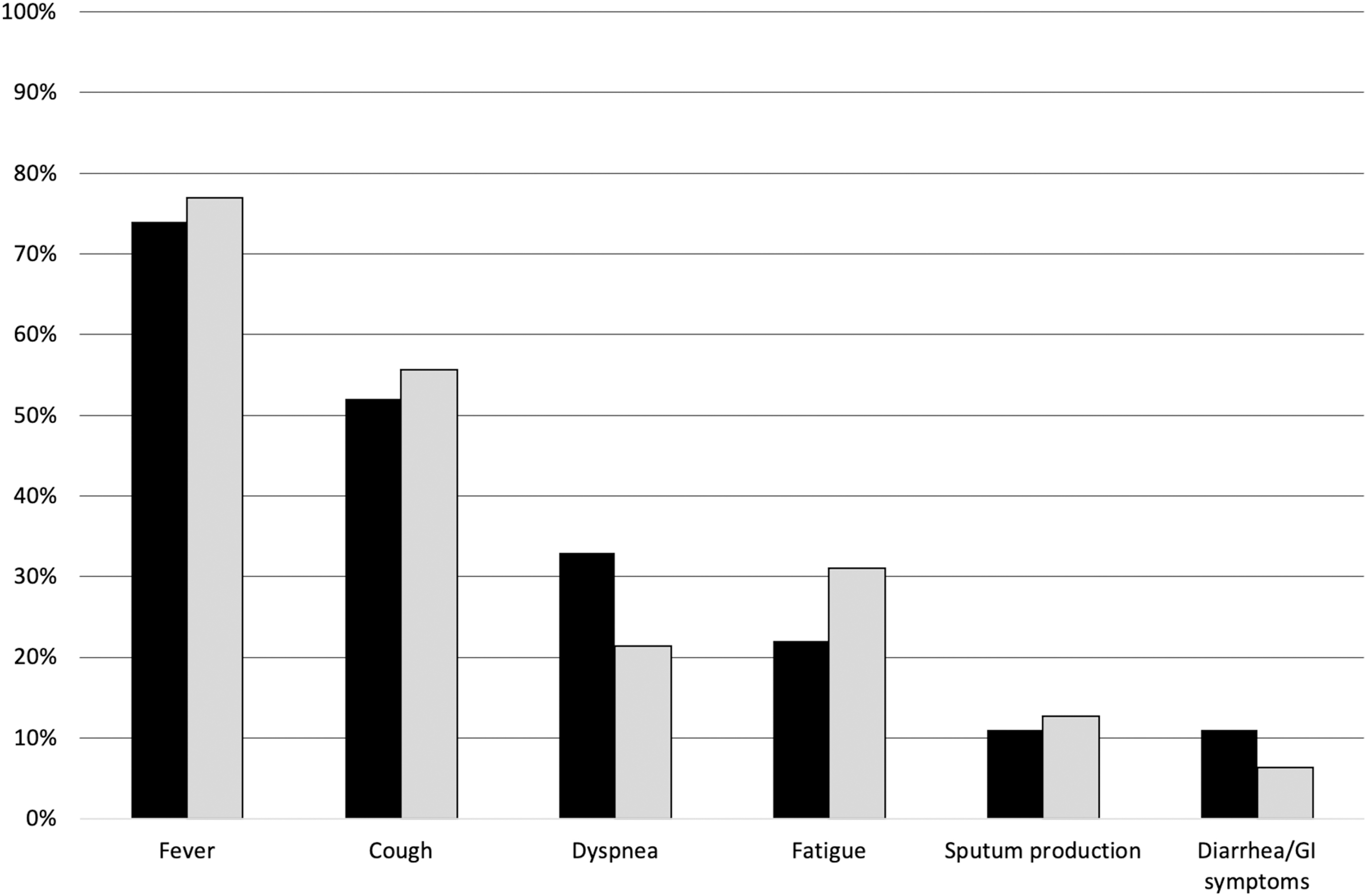
SCI population (black) compared to the case series and cross-sectional study data from a recent systematic review on COVID-19 in the general population (grey). GI, gastrointestinal; SCI, spinal cord injury.
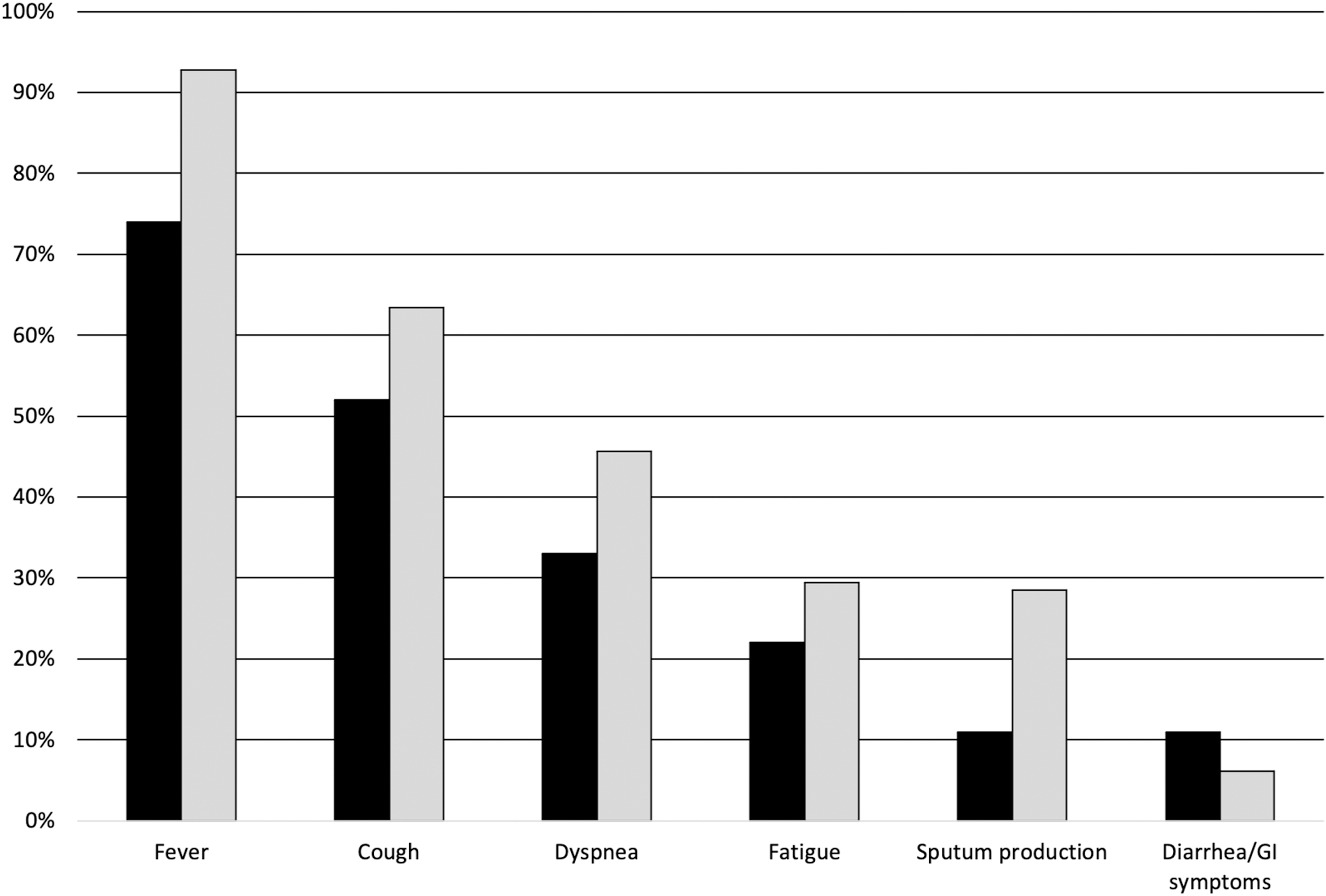
Symptoms of COVID-19 in the SCI population (black) compared to the case report data from a recent systematic review on COVID-19 in the general population (grey). GI, gastrointestinal; SCI, spinal cord injury.
Because of the relatively small number of patients in this review and incomplete reporting of information, we could not formally identify prognostic factors or risk factors for severe COVID-19 disease specific to the SCI population. In a recent correspondence piece, Dicks and colleagues 24 wrote that they expected SCI patients to be at higher risk of ARDS and respiratory decompensation. In this review containing mostly cervical SCI patients and some with tracheostomy, only 1 case required mechanical ventilation and the majority could be treated with low-flow oxygen therapy. The literature published thus far indicates that severe respiratory decompensation is not prevalent in the SCI population with COVID-19. Two cases described by Sánchez-Raya and Sampol 36 that resulted in death were incomplete in reporting treatment and could have required mechanical ventilation and admission to the ICU.
Literature published on SARS-CoV-2 clinical outcomes in the general population should alert clinicians and researchers to particular consequences that could adversely affect people with SCI. Increasing evidence shows that obesity/higher body mass index (BMI) are risk factors for contracting COVID-19, and that higher BMI is associated with more-severe COVID-19 disease and higher mortality 41,42 ; it is estimated that 65% of persons with SCI are overweight and 30% are classified as obese. 43 A meta-analysis of six published studies from China including 1527 patients with COVID-19 reported 16.4% prevalence of cardio-/cerebrovascular disease (CVD) and 17.1% prevalence of hypertension. 44 The overall case fatality rate was 2.3% in the entire cohort, but was significantly higher in patients with hypertension (6%) and CVD (10.5%). 44 In a large Canadian community sample of people with SCI (N = 60,959) study on health, 17.1% of respondents with SCI had heart disease compared to 4.9% of those without SCI. 45 After adjusting for age and sex, the likelihood of a person having heart disease was 2.7 times greater in people with SCI versus those without SCI. 45
Additionally, a study of 100 recovered COVID patients found ongoing myocardial inflammation in 60% of patients independent of any pre-existing conditions. 46 Though we do not yet know how long these effects last in those who have recovered from COVID-19, additional cardiac damage to persons with SCI, who have established higher rates of CVD, may be a cause for concern.
The case series and reports included in this review, though they are mainly descriptive studies of a small number of patients, do not show a high percentage of severe COVID-19 disease, ICU admission, mechanical ventilation requirement, or adverse events, but do show a high mortality rate. The mortality rate of 10% (3 of 31 patients) in the case series and reports is higher than the 6.6% reported in a recent meta-analysis of 10 studies in the general population hospitalized because of COVID-19. 47 The Veterans Health Administration registry study 38 reports an even higher case fatality rate of 19%, which is twice as high as that of the non-SCI/D population in the same registration system and almost 3 times the fatality rate reported by Javad Nasiri and colleagues. 47
The higher mortality rate we found could be partially explained by the higher percentage of males in our clinical sample (22 of 29; 79%) given that the case fatality rate is reported to be higher in men compared to women 47 (pooled odds ratio of 3.4 with 95% CI, 1.2-9.1). Another impactful factor that has been found to have been of substantial influence and partially explains our high mortality rate is age. The 4C Mortality Score is a mortality prediction instrument for COVID-19 that has been developed and validated in an N = 57,824 general population sample in the United Kingdom. 48 It uses an eight-item mortality index corresponding to a mortality score between 0 and 21, where age >80 years adds 7 points to the index.
Another factor is that most cases included in this review are or are likely to be cases from the early pandemic and therefore come from a time when hospitals and clinicians were less prepared and fewer effective treatment options had been identified, such as dexamethasone treatment. 49 Nonetheless, the mortality among persons with SCI/D who are infected by SARS-CoV-2 and develop COVID-19 disease found in this review is substantially higher than in the general population.
Uncertainties exist about the exact mortality attributable to COVID-19 in our review, mainly attributable to the lack of cause of death reporting in the Veterans Health Administration registry study (N = 140). In 2 cases described by Sánchez-Raya and Sampol, 36 COVID-19 was reported as the probable cause of death. Both patients were 80+ years of age and had relevant comorbidity. Pattanakuhar and colleagues 32 are unclear about whether or not COVID-19 was the cause of death in the patient described in their case report. The latter patient who did not show signs of ARDS, dyspnea, or other severe signs of respiratory decompensation nor were there signs of (multi-)organ failure. No abnormal electrocardiography pattern was observed on admission. The researchers provided cardiac sudden death (under enoxaparin prophylaxis) associated with the post-operative state after traumatic cervical SCI with comorbid mild COVID-19 pneumonia as the legal cause of death. It is important to recognize that acute myocardial injury is associated with COVID-19, even in mild cases, and could still have contributed to or caused death in this patient. 50
With acute pressure on all healthcare services because of COVID-19 outbreaks, care for SCI patients has been challenging in many jurisdictions, as has been articulated in the editorial piece by Lopéz-Dolado and Gil-Agudo 25 that accompanies the case series from the outbreak in their SCI center. 31 A further strain on rehabilitation services could be expected given that a growing body of literature shows that COVID-19 could lead to neurological complications that may require rehabilitation, such as encephalitis, 51 vasculitis, 52 stroke, 8,9 neuropathy, 9,53,54 transverse myelitis, 55 –59 and Guillain-Barré syndrome. 8,10 –12,60 –72
Given that more and more SCI patients experience COVID-19 around the world, more case reports, case series, and cohort studies will be published. Analytical observational studies with larger numbers of patients or retrospective case-control studies would add greatly to the evidence base and help answer the research questions posed in this review. Further studies should be as inclusive as possible in reporting given that little is known about risk factors in the SCI population and questions on differences in presentation, course, and outcomes have unfortunately not yet been answered. Until COVID-19 and all of its impacts are fully understood, it is important that vulnerable populations, including those with neurological disorders, strictly adhere to physical distancing and elevated hygiene practices to minimize initial transmission of the disease. 73
Conclusion
In this rapid review, we found that clinical presentation of COVID-19 disease in SCI patients does not differ much from the general population. Whereas the numbers of adverse events, ICU admissions, and patients requiring mechanical ventilation were low, the mortality rate of COVID-19 for SCI patients was 10% in the identified case series and reports and 19% in a large, cross-sectional registry study—both substantially higher than mortality rates reported for the general population, but comparable to at-risk populations. No prognostic factors for severe disease or mortality could be identified in this review.
Limitations
Although our review provides insight into the clinical characteristics and outcomes of COVID-19 disease in persons with SCI, there are limitations to our study. Although supplemented with cross-sectional studies, the small number of patients in the clinical studies included in this review and the mainly descriptive observational nature of those studies make drawing reliable conclusions on clinical characteristics and course of COVID-19 in SCI difficult. Incomplete reporting of data on SCI-specific secondary health conditions, as well as treatment modalities used in the included studies, further complicates drawing conclusions on questions related to prognostic factors relevant to the SCI population.
Although we did a comprehensive literature search in multiple languages, we did not search the Italian literature, assuming that the Italian literature would mostly be published in English and would thus be identified through our English database searches. Further, we did not include gray literature or pre-print servers in our search because of the time constraints for this rapid review.
Footnotes
Acknowledgments
We thank Jessica Archibald, Luis Dias, Chihya Hung, and Hui-Ling Lin for their aid in searching the Spanish, Portuguese, and Chinese literature, respectively.
Funding Information
This work was funded by the Praxis Spinal Cord Injury (SCI) COVID-19 Award, awarded by the Praxis Spinal Cord Institute. The funding agency had no role in developing this protocol. Dr. Eng is supported by the Canada Research Chair Program.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.