
Abstract
It is increasingly reported that a history of concussion may be associated with chronic deleterious consequences. While the pathophysiology that contributes to these consequences is not well understood, neuroinflammation is postulated to be critical. Activation of multi-protein complexes termed inflammasomes, a key component of this inflammatory response, has been reported in more severe TBIs; however, it has not been investigated in milder TBIs, such as concussion. This study investigated serum levels of interleukin (IL)-1β and IL-18 (key proteins activated downstream of these inflammasomes) at acute, sub-acute, and chronic time-points post-concussion. We recruited 105 Australian footballers (65 male, 40 female) during the pre-season, then prospectively followed these players for the occurrence of concussion during the season. At baseline, 58 footballers reported a previous concussion history, and 47 reported no previous concussion history. Additionally, 25 players sustained a mid-season concussion and were sampled at 2, 6, and 13 days post-concussion. Serum levels of IL-1β and IL-18 were quantified using highly sensitive Simoa HD-X Analyzer assays. At baseline, IL-1β levels were higher in male, but not female, footballers with a previous concussion history compared with footballers with no concussion history. There was also a positive correlation between years of collision sport participation and IL-18 levels in males. No evidence was found in males or females to indicate that IL-1β or IL-18 levels differed at 2, 6, or 13 days post-concussion. These findings provide novel insights into potential sex-specific physiological consequences of concussion, and suggest that neuroinflammation may be persistent chronically following concussion in male athletes.
Introduction
Concussion, a highly prevalent subset of traumatic brain injury (TBI), is a global health concern, with increasing evidence linking a history of concussion (HoC) and sub-concussive impacts to chronic deficits. 1 –6 Australian football is the most participated collision sport in Australia, with male and female competitions following similar rules. The incidence of concussion in Australian football is reported as 6.13 concussions per 1000 match hours. 7 Although the prevalence of sub-concussive injuries in Australian football is unlikely to be as prominent as in American football, these injuries are a common consequence of routine match-play. 8 Despite the high prevalence of mild brain injuries in Australian football, few studies have investigated the potential neurological consequences associated with its participation. 8
Although the pathophysiology of concussion is poorly characterized, 9 neuroinflammation, and particularly microglial activation (a critical component of neuroinflammation), is widely hypothesized to be a key contributor to mild traumatic brain injury (mTBI)–associated deficits. 10 –12 Activation of multi-protein complexes termed inflammasomes is a critical component of this neuroinflammatory response. 13 The activation of this inflammasome facilitates the downstream cleavage and activation of the pro-inflammatory cytokines interleukin (IL)-1β and IL-18. 14 As such, these proteins are commonly employed as indicators of inflammasome activation. Multiple different inflammasomes have been previously described to effect cleavage and activation of these cytokines, of which the NOD-like receptor pyrin domain-containing protein 3 (NLRP3) inflammasome is the most extensively studied. 13 While well documented in more severe TBI, studies investigating the contribution of these inflammasomes to the pathophysiology of concussion are limited. 10
There has been increased study into the use of circulating proteins as biomarkers of concussion. 15 As such, alterations in peripheral IL-1β and IL-18 may provide an avenue to study inflammasome activation after concussion. Using highly sensitive immunoassays, we quantified serum IL-1β and IL-18 in male and female Australian footballers. We used years of collision sport participation as a surrogate measure of sub-concussive impact exposure and self-reported concussion history to investigate the association of these factors with levels of IL-1β and IL-18 in pre-season serum samples. Additionally, we assessed the temporal profile of these cytokines in the acute and sub-acute setting of concussion.
Methods
Participant recruitment
A total of 134 Australian footballers (82 male and 52 female) were recruited between 2016–2020 from amateur Australian football clubs. Baseline assessments of footballers were performed during the pre-season and any players reporting a history of neurosurgery or severe psychiatric disturbances were excluded. Additionally, to minimize the confounds of potential residual concussion, footballers that had sustained a concussion in the previous 6 months were also excluded. Serum samples from 105 (65 male, 40 female) footballers were included in baseline cytokine analysis. To investigate chronic changes relating to a HoC, footballers recruited at baseline were divided into two groups; 58 players with a self-reported HoC (38 male, 20 female); and 47 players with no HoC (27 male, 20 female).
Additionally, 34 players (23 male, 11 female) were diagnosed at side-line as having sustained a concussion. These participants were re-tested at 24–72 h (2 days), 6 days, and 13 days post-concussion. Any participants that participated in two or less collection points were excluded. Additionally, two players were diagnosed as concussed twice in one season. For these players, only their first concussion samples were included. As such, 25 participants (17 male, eight female) were included in the acute post-concussion cytokine analysis. Of these 25 participants, two male footballers were diagnosed as sustaining a concussion in two separate seasons. As these players had participated in two separate baseline collections, they were included in the acute cytokine analysis. A small number of post-concussion collections were missed due to logistical reasons such as participant unavailability. As such, 21 samples were analyzed at baseline (15 male, six female), 24 at 2 days (17 male, seven female), 25 at 6 days (17 male, eight female) and 24 at 13 days (16 male, eight female). The study was approved by the Human Research Ethics Committee of Melbourne and all participants provided written informed consent.
Clinical interview
Participants completed a survey relating to their demographic information, previous concussion history, collision sport involvement and personal/family medical history.
In addition, the Sports Concussion Assessment Tool (SCAT) was administered to all participants as a baseline measure of concussion-related symptoms. The tool consists of three sections; the first section is a self-reported symptom evaluation which includes both number of symptoms (max of 22) and severity of symptoms (max of 132); the second termed the standardized assessment of concussion (SAC) is a basic cognitive screening tool; the final is a balance examination which utilizes a modified version of the Balance Error Scoring System (BESS). Participants recruited in 2016–2018 undertook the 3rd edition of the SCAT, whereas participants recruited in 2019–2020 undertook the 5th edition. The SAC differs slightly between the two editions. As such, only the symptom evaluation and BESS scores were compared in subsequent analyses.
Blood collection
A total of 50 mL of blood was collected via venipuncture following standard phlebotomy procedures. Blood was drawn directly into vacutainer tubes containing a thixotropic gel (BD Vacutainer® SST™ II Advance) and immediately inverted. Blood clotted at room temperature for 30 min, then was centrifuged at 1500 g for 10 min at room temperature. The separated serum was immediately aliquoted, flash-frozen and stored at −80°C until analysis.
IL-1β and IL-18 serum quantification
Quantification of serum IL-1β and IL-18 was conducted on a Simoa HD-X Analyzer™ (Quanterix, Billerica, MA), using commercially available kits (IL-β: Ref 101605, IL-18: Ref 102700; Quanterix, Billerica, MA). Samples were run in duplicate and protocols followed following manufacturer instructions. All samples measured above the lower limit of detection; however, one sample (male HoC) was found to have an IL-1β level above the upper limit of quantification and was excluded from subsequent analysis. To minimize any impact of inter-plate variance, groups were balanced across plates, longitudinal samples were run on the same plate, and samples were run across all plates to verify inter-plate reliability.
Statistical analysis
Normality of continuous variables (age, years of collision sport, IL-1β, and IL-18) were tested utilizing the Anderson Darling test for normal distribution. Due to the spread of serum IL-1β and IL-18 levels, cytokines levels underwent a natural logarithmic transformation. Additionally, all transformed cytokine values underwent a ROUT outlier test within their respective group with a false discovery rate of 1%. For acute IL-1β analysis, one female 2- and 13-day sample were determined to be outliers. For the baseline IL-1β analysis, one male HoC and one male noHoC sample, and for IL-18, one male HoC sample, were determined to be outliers. These five values were subsequently removed from all analyses. The results from the Anderson-Darling test on the transformed data were not significant (p > 0.05) for all baseline cytokine levels indicating that the transformed data fit the normal distribution. The raw (untransformed and outliers included) cytokine levels at baseline and acute time-points are presented in Supplementary Figure S1.
Two-way analysis of variance (ANOVA) with variables of sex and HoC were utilized for most demographic variables (age, years of education, years of collision sport), SCAT measures, and baseline cytokine comparisons. Bonferroni multiple comparisons were conducted where appropriate. Mann-Whitney U-test was utilized to compare number of concussions and time since last concussion in male and female footballers with a HoC. Correlation analyses were performed to assess the relationship between cytokines and demographic data with parametric (Pearson's; male years of collision sport) and non-parametric distribution (Spearman's; all other demographic information). For the variables that were found to have a statistically significant correlation, a subsequent simple linear regression was also performed. Due to a variable number of samples at post-concussion time-points, acute measures (SCAT, IL-1β and IL-18 levels) were analyzed with a mixed model utilizing a compound symmetry covariance matrix and fit using restricted maximum likelihood with Geisser-Greenhouse correction. All statistical analyses were performed utilizing SPSS 26.0 (IBM Corp., Armonk) and GraphPad Prism version 8.3.1 for Windows (GraphPad Software, CA). Significance was set at p < 0.05.
Results
Demographics
For male and female participants at baseline (Table 1), there were no main effects for sex or HoC on age. There was a main effect of sex on years of education (F1, 99 = 5.704, p = 0.019) and years of collision sport participation (F1,92 = 36.614, p < 0.001), with males reporting a higher number of years of education and greater collision sport participation than females. Males with a HoC had a higher number of previous concussions than females with a HoC (p = 0.002). There was no difference in time since most recent concussion (p = 0.407).
Demographic Information of Participants Involved in Baseline HoC Assessment
Participants are grouped by sex (male and female) and previous concussion history (HoC or noHoC). Main-effects are bolded (p < 0.05). For number of concussions and time since last concussion only male HoC and female HoC are compared. ** represents a group difference to male HoC (p = 0.002). Data is presented as mean ± standard error of the mean.
HoC, history of concussion.
Male and female participants diagnosed with concussion did not differ by age, years of education, or years of collision sport. Recently concussed males however, reported a greater number of prior concussions than females (p = 0.007; Table 2).
Baseline Demographic Information for Male and Female Acute Concussion Participants
Males had higher number of previous concussions than females. ** p < 0.01. Data are presented as mean ± standard error of the mean.
Concussion-related symptom assessment (SCAT)
For footballers at baseline, there were no main effects for HoC, sex, or HoC × sex interaction for number of symptoms (F1,102 = 1.800, p = 0.183; F1,102 = 2.173, p = 0.144; F1,102 = 3.693, p = 0.698; Fig. 1A) or severity of symptoms (F1,102 = 0.179, p = 0.673; F1,102 = 2.888, p = 0.092; F1,102 = 0.002, p = 0.967; Fig. 1B). For number of BESS errors there was no main effect of HoC or a HoC × sex interaction (F1,94 = 0.179, p = 0.690; F1,94 = 0.379, p = 0.540; Fig. 1C). There was, however, a main effect of sex (F1,94 = 6.808, p = 0.011), with females having more errors on the BESS than males.
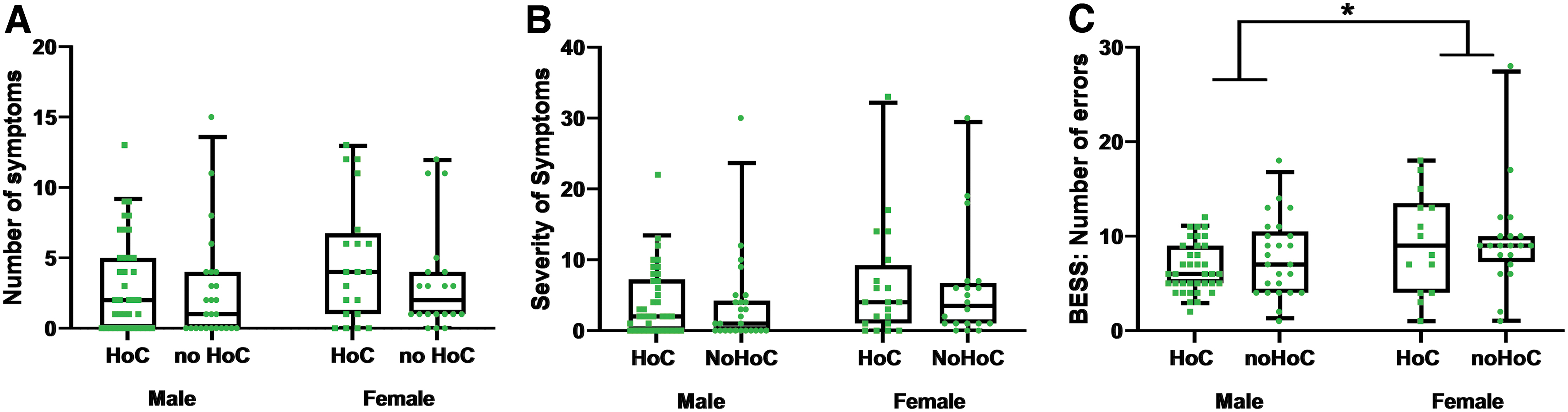
Baseline concussion-associated symptom assessment of players with and without a history of concussion (HoC) and sub-concussive impacts. Number of symptoms
For male and female concussion participants, two-way ANOVAs revealed a main effect of time for number of symptoms (F2.25, 47.16 = 6.859, p = 0.002; Fig. 2A), severity of symptoms (F2.22,46.66 = 6.532, p = 0.002; Fig. 2B), and number of BESS errors (F2.48, 49.62 = 3.086, p = 0.044; Fig. 2C). Post hoc analyses determined that number of symptoms was higher at 2 days when compared with baseline (95% CI: 0.379–9.038, p = 0.039), 6 days (95% CI: 0.783-7.380, p = 0.014), and 13 days (95% CI: 3.300-8.366, p < 0.0001). Severity of symptoms was higher at 2 days compared with baseline (95% CI: 1.065-19.10, p = 0.032), 6 days (95% CI: 1.699-15.75, p = 0.014), and 13 days (95%CI: 6.052-18.53, p = 0.0001). No other time-points were different for symptom number or severity. Despite an overall effect of time for BESS, post hoc analyses revealed no differences across time-points. No main effect of sex or sex × time interaction was found for number of symptoms (F1,23 = 1.544, p = 0.227; F3,63 = 0.809, p = 0.494), severity of symptoms (F1,23 = 0.7503, p = 0.395; F3,63 = 1.610, p = 0.196), or number of BESS errors (F1,23 = 2.409, p = 0.134; F3,60 = 0.2234, p = 0.880).
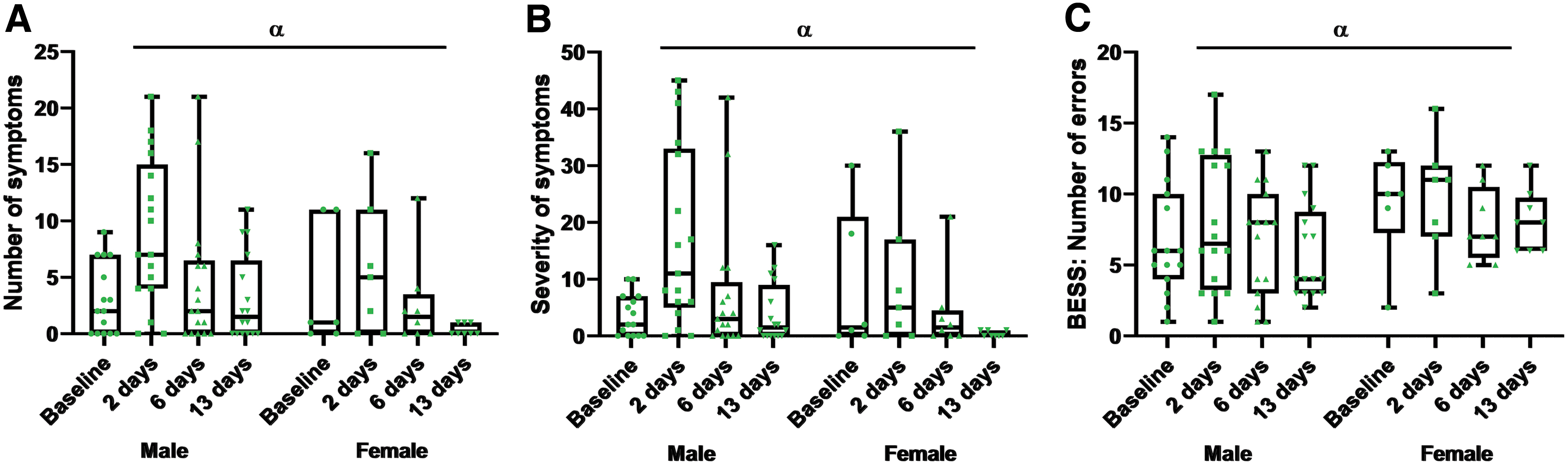
Acute concussion-associated symptom assessment. Number of symptoms
Concussion history and cytokine levels
For the pre-season serum IL-1β levels (Fig. 3A) of participants grouped by previous concussion history, there were no main effects of HoC (F1,98 = 0.243, p = 0.623) or sex (F1,98 = 1.588, p = 0.211); however, a HoC × sex interaction was found (F1,98 = 4.981, p = 0.030). Post hoc analysis revealed that males with a HoC had higher serum IL-1β levels than males with noHoC (95% CI: 0.037-1.080, p = 0.036) and females with a HoC (95% CI: 0.158-1.277, p = 0.012). Serum IL-1β levels in females with noHoC were not different from females with a HoC (95% CI: -0.991-0.284, p = 0.525) and males with noHoC (-0.410–0.799, p = 0.525). For serum IL-18 levels (Fig. 3B), no main effects of HoC (F1,100 = 1.082, p = 0.301) sex (F1,100 = 1.062, p = 0.305), or HoC × sex interaction (F1, 100 = 3.295, p = 0.072) were found. No correlations were found relating number of previous concussions to cytokine levels (Supplementary Fig. S2).

Circulating interlelukin (IL)-1β and IL-18 levels in the context of history of concussion (HoC) and sub-concussive impacts. Circulating IL-1β
Collision sport involvement and cytokine levels
No associations were found between years of collision sport involvement and IL-1β in males (Pearson's r: -0.179, p = 0.170; Fig. 4A) or females (Spearman's r: 0.143, p = 0.427; Fig. 4B). For serum IL-18 levels, there was a positive correlation between years of collision sport involvement and serum IL-18 levels in males (Pearson's r: 0.284, coefficient = 0.022, p = 0.024; Fig. 4C), but no association in females (Spearman's r: -0.253, p = 0.156; Fig. 4D). Additionally, no associations were found between age and cytokine levels (Supplementary Fig. S3).

Correlation of circulating interleukin (IL)-1β and IL-18 with years of collision sport. The relationship between years of collision sport and IL-1β in
Acute temporal profile of IL-1β and IL-18
For serum IL-1β in male and female concussion participants (Fig. 5A), there were no main effects for time (F1.96,38.46 = 0.993, p = 0.378), sex (F1,23 = 0.546, p = 0.468), or time × sex interaction (F3,59 = 0.823, p = 0.487). Similarly, for IL-18 (Fig. 5B), there were no main effects for time (F0.83, 16.80 = 0.792, p = 0.363), sex (F1,23 = 0.291, p = 0.595), or time × sex interaction (F3,61 = 0.248, p = 0.862).

Acute and sub-acute temporal profile of circulating interleukin (IL)-1β and IL-18 following concussion. Circulating IL-1β
Discussion
This study investigated circulating levels of IL-1β and IL-18 (proteins downstream of inflammasome activation) in the acute, sub-acute, and chronic stages of concussion in male and female Australian footballers. At baseline, serum IL-1β levels were higher in males, but not females, who reported a previous HoC. Serum IL-18 levels also were correlated with years of collision sport participation in males only. Acutely following concussion, serum IL-1β and IL-18 levels at 2, 6, and 13 days were found to be no different to baseline. Overall, these findings suggest that a history of mild brain injury may be associated with chronic elevation of serum IL-1β and IL-18 in a sex-specific manner.
Circulating cytokine alterations relating to HoC and collision sport participation
Multiple studies have provided evidence that chronic neuroinflammation, and specifically microglial activation, may be prominent in collision sports athletes. For example, a positron emission tomography imaging study of retired male American football players with a significant HoC found that cerebral levels of the 18kDa translocator protein (a marker utilized as a measure of microglial activation) were higher in athletes with a HoC than age matched controls. 16 Moreover, numerous rodent studies have revealed that repeated mTBI exposure can lead to persistent microglial activation. 17 –20 Given IL-1β and IL-18 can be produced in response to inflammasome activation, particularly in microglia, 14,21 our findings may provide further evidence of chronic microglial activation due to concussive or sub-concussive impacts. Nonetheless, it is important to recognize that the cellular source, central nervous system specificity, and mechanisms responsible for the observed serum cytokine changes are unknown. To further elucidate the exact role of inflammasomes in the chronic setting of mild head injuries, future biomarker studies should incorporate markers specific to individual inflammasomes such as NLRP3, as well as how these peripheral changes correlate to central markers of inflammation.
Intriguingly, analysis of serum IL-1β and IL-18 in female baseline samples revealed no associations with a HoC or collision sport participation. It is increasingly recognized that biological sex plays a critical role in the pathophysiology of concussion, and that the neuroinflammatory response may differ between males and females. 22,23 Of particular relevance, one study similarly reported a sex-specific serum inflammatory profile chronically following concussion. 24 Males with a history of multiple concussions had higher serum levels of MCP-4 than those with no previous HOC. Conversely, females with a history of multiple concussions were found to have higher MCP-1 levels. 24 Pre-clinical investigations have similarly demonstrated sex-specific physiological alterations following TBI.
For example, one study found that following murine moderate-to-severe TBI, the microglial response in males occurred earlier and was exaggerated when compared with females. 25 Additionally, the current finding that IL-1β and IL-18 may have a more prominent role in males is supported in a murine model of post-operative pain. 26 This study demonstrated that following surgery, male mice received greater benefit from NLRP3 inflammasome knock-out than females, exhibiting diminished hypersensitivity to stimuli. 26 While the findings of the current study may be further evidence of a sex-specific inflammatory profile, due to the relatively recent uptake of Australian football in females, the self-reported history of collision sport participation and number of concussions of our study population was greater in males than female. It is thus possible that a greater collision sport involvement and concussion history is required to elicit chronic alterations in IL-1β and IL-18.
There are a few important considerations regarding the presented baseline alterations in circulating IL-1β and IL-18 levels. It is important to consider the highly homogenous ages of the participants enrolled in this study. The translatability of the current findings to the general population is not known and should be replicated in heterogeneous populations. Further, while we found no association between player age and cytokine level, IL-18 has been shown to be increased in aged populations, 27 and as such may confound the association between IL-18 levels and collision sport. Additionally, concussion history and collision sport involvement for this study was estimated by footballers self-reporting and is consequently unlikely to be precise. While we reported no SCAT deficits in participants with a history of concussion, it is possible that neuropsychological tests with higher sensitivity to detect subtle deficits are necessary to investigate how these peripheral cytokines are associated with chronic affective deficits. Further, years of collision sport involvement is an inexact measure of sub-concussive impact history. The association between IL-18 levels and sub-concussion should be replicated with a robust measure of sub-concussive impacts such as accelerometers, which can be placed in the mouthguards of collision sport athletes.
Temporal profile of IL-1β and IL-18 in the acute setting of concussion
Despite the presence of symptoms at 2 days post-concussion, we found that serum levels of IL-1β and IL-18 were comparable at baseline to 2, 6, and 13 days post-concussion. Although IL-1β has several important physiological roles, multiple studies have reported that elevated brain levels of this cytokine can be a key contributor to mTBI outcomes. 28 –30 A number of studies have attempted to quantify circulating IL-1β following concussion; however, these studies are commonly plagued by undetectable levels of circulating IL-1β, 24,31 –33 As such, IL-1β is frequently unreported in studies investigating fluid biomarkers of concussion. Two studies have quantified and reported opposing findings for IL-1β acutely following concussion. 34,35 One study that recruited patients within seven-days of their concussion found serum IL-1β levels to be higher in concussed patients than controls. 34 Conversely, one study that investigated pediatric concussion patients, reported no differences in plasma IL-1β at hospital admission (within 48 h) and through sub-acute time-points. 35 The inclusion of a pre-concussion (baseline) time-point in the current study is unique to previous studies of circulating IL-1β and is a key strength of this study design.
Limited studies have investigated IL-18 in the context of concussion. Studies following more severe TBIs have, however, reported increased IL-18 levels in the brain parenchyma, cerebrospinal fluid (CSF), and peripheral circulation. 36 –38 Further, these studies have provided preliminary evidence into a potential diagnostic utility of IL-18, with one study demonstrating a strong discriminative ability of CSF (but not serum) IL-18 at acute time-points. 38 While no clinical studies have investigated IL-18 in concussion, a pre-clinical model of repeat mTBI has demonstrated increased expression of IL-18 and IL-1β in the brain endothelial cells of adolescent mice 11-days after the final injury, however blood levels of these proteins were not investigated. 39
One explanation for the lack of serum cytokine changes observed acutely post-concussion may be the insufficient passage of IL-1β and IL-18 into the circulation. Although pre-clinical studies have demonstrated alterations in these cytokines after mTBI, 28 –30 the magnitude of these changes may be insufficient to be detectable in blood concentrations and as such higher severity mTBIs may be required to elicit serum changes in IL-1β and IL-18. While the current study utilizes the SCAT to quantify symptom burden, there are no sophisticated measures to determine injury severity. To investigate the effect of injury severity on peripheral IL-1β and IL-18 levels, future studies should include objective outcomes (such as neuropsychological testing) to assess the effect of injury severity on these cytokines. Additionally, neuroinflammation is known to be induced in minutes-to-hours following TBI. 40 As such, when considered alongside the relatively short half-life of IL-1β and IL-18, 41,42 it is possible that our sampling time-points may have been inappropriate to capture alterations in these proteins. Future studies featuring more acute time-points (e.g., 4 h) may be required to assess the utility of these serum cytokines in the context of acute concussion.
Conclusion
This study investigated circulating IL-1β and IL-18 in male and female Australian footballers. In males, circulating levels of IL-1β and IL-18 were related to a reported HoC and collision sport participation respectively. Interestingly, these findings were not observed in females, which may be due to a sex difference in the chronic inflammatory response to mild brain injury or to the lower exposure to collision sport participation and concussion history in the female participants. Our findings suggest that in males, mild brain injury may instigate a chronic neuroinflammatory state, however future studies are required to determine whether the activation of IL-1β and IL-18 may contribute to the chronic neurological consequences that have been linked to a HoC and collision sport participation.
Footnotes
Authors' Contributions
W.T.O., D.M.C., R.M., T.J.O., M.M., S.R.S., and S.J.M were responsible for the conception and design of the study. W.T.O., G.F.S., J.B., B.P.M., M.S., J.S.K., Z.C., R.D.B, M.M., S.R.S., and S.J.M were responsible for the acquisition and analysis of data, W.T.O., M.M., S.R.S., AND S.J.M. were responsible for drafting a significant proportion of the manuscript and figures. All authors edited and approved the final draft of the manuscript.
Funding Information
This study acknowledges research funding and support from Monash University and grants and fellowships awarded to S.R.S., T.O.B., and R.M. by the Australian National Health and Medical Research Council.
Author Disclosure Statement
Zhibin Chen reports an Early Career Fellowship from the National Health and Medical Research Council (NHMRC) of Australia (GNT1156444). His institution has received consultancy fees and/or research grants from Arvelle Therapeutics and UCB Pharma.
Terence J. O'Brien reports grants from Eisai Pharmaceuticals, UCB Pharma, grants from Biogen, ES Pharmaceuticals, Supernus Pharmaceuticals.
For the other authors, no competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.