
Abstract
Prognosis evaluation is crucial for the effective management of patients with acute traumatic brain injury (TBI). However, there is still a lack of routinely available blood indicators for mortality risk in clinical practice. To investigate whether blood red cell distribution width to platelet count ratio (RPR) correlates with hospital mortality of TBI, clinical data of 2220 patients with TBI were extracted from two large intensive care unit cohorts (MIMIC-III and eICU Database), and were integratively analyzed using our developed method named MeDICS. We found that higher RPR can be observed among non-survivors than survivors of TBI (p < 0.001). It had a moderately good prognostic performance for mortality with an area under receiver-operating characteristic curve (AUC) of 0.7367, which was greater than that of Glasgow Coma Scale (GCS; AUC = 0.6022). Besides, the nomogram consisting of RPR, GCS, and other risk factors was developed, where 10-fold cross-validation was performed to protect it against overfitting. A Harrell's C-index of 0.8523 was determined, suggesting an improved prognostic value based on RPR. The in vivo experiments further confirmed the association between RPR and neuro-outcome after TBI. It indicated that the continuous change in RPR post-injury is attributed to the development of inflammation, which emphasized the importance of controlling inflammatory response in clinical treatment. Taken together, RPR is a promising routinely available predictor of mortality for acute TBI. The nomogram generated from it can be used in resource-limited settings, thus be proposed as a prognosis evaluation aid for patients with TBI in all levels of medical system.
Introduction
Traumatic brain injury (TBI) is one of the leading causes of disease that induced death and long-term disability, especially in children and young adults. 1 More than 50 million people worldwide are affected by a new TBI case annually, with an overall economic cost in the United States of about $406 billion. 2 As a growing public health problem, the incidence of TBI increases rapidly each year with the acceleration of urbanization, the increase of traffic accidents, and the frequent occurrence of local wars. Although great progress in clinical management has been made in the past few decades, there are still many clinical problems that need to be resolved.
Predicting outcome is crucial for the effective management of patients with acute TBI in neurosurgical intensive care unit (ICU), neurological ICU, and emergency ICU. On the one hand, early recognition of the disease severity contributes to inform and improve decision making for TBI patients. On the other hand, the medical information provided to relatives should be based on solid clinical and scientific evidence, which will help them prepare for the future and understand the unpredictable risks that the patients need to undergo. Intracranial pressure (ICP) and Glasgow Coma Scale (GCS) are classic indicators to evaluate the severity of TBI. However, management of ICP is invasive, while the GCS score alone cannot predict the outcome well in the early stage post-injury, as it can be influenced by multiple factors, such as alcohol drinking, intermediate awake of epidural hematoma, and past history of neurological diseases. 3 In addition, various researches have focused on exploring diagnostic and prognostic biomarkers for TBI in recent years. Although the potential biomarkers, including S100B, glial fibrillary acidic protein ubiquitin carboxyl-terminal hydrolase L1, neurofilament light chain, and tau have been reported with diagnostic or prognostic values in clinical trials, most of them have not been used in clinical work due to the lack of clinically compatible measurement platforms that ensure standardization and reproductive testing, except for S100B which was only used in diagnosis of mild TBI. 4 –7
Routine complete blood count (CBC) analysis is one of the most extensively applied noninvasive laboratory tests in clinical practice. Although some parameters of CBC analysis have been studied to determine the severity and mortality risk of TBI, there is still a lack of reliable and routinely available blood indicators with sufficient clinical evidence until now. 8 Red blood cell distribution width (RDW) and platelets (Plt) count represents the heterogeneity of peripheral circulating red blood cells and the pathophysiology of hemostasis individually. As previously reported, RDW was increased at 1–7 days after TBI. Although some scientists suggested that RDW could be a prognostic indicator for acute TBI, the research with larger study population indicated that it was a poor predictor (area under receiver-operating characteristic curve [AUC] = 0 · 66) for the mortality risk. 9,10 Besides, Plt count was observed to be decreased after TBI, and its lowest value appeared at 1–5 days after TBI, followed by a rebound to the admission level by Days 5–9. 11 However, Plt count and other parameters of routine coagulation tests, including prothrombin time and activated partial thromboplastin time, demonstrated poor sensitivity to the clinical outcome of patients with TBI. 12 In addition, the RDW to Plt count ratio (RPR) is a potential powerful predictor for the severity and mortality risk of acute TBI in theory because it amplifies the imbalances between RDW and Plt count.
In view of the fact that the CBC parameters, including RDW and Plt count may be interfered by shock, acute stress reaction, and emergency treatments at the first day after TBI, we selected 3–5 days after admission as the main time-point to study the prognostic value of RPR. The time-point is also the peak period of brain edema with central nervous system (CNS) and peripheral inflammation following injury. 13 In addition, we employed one of the largest reported cohorts in the present study. The findings are expected to provide solid evidence for RPR in predicting the mortality risk of patients with acute TBI as a routinely available blood indicator in all levels of medical system.
Methods
Database introduction
All data in the current study were extracted from the online international databases—the Multiparameter Intelligent Monitoring in Intensive Care III (MIMIC-III, version 1.4) database and the eICU Collaborative Research Database (eICU-CRD, version 2.0)—that are maintained by the Laboratory for Computational Physiology at the Massachusetts Institute of Technology (Cambridge, MA). The MIMIC-III database was approved by the institutional review boards of Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center (Boston, MA). It contains 61,532 ICU admissions of 46,476 patients at this medical center from 2001 to 2012. The eICU-CRD was released under the Health Insurance Portability and Accountability Act safe harbor provision, and the re-identification risk was certified as meeting safe harbor standards by Privacert (Cambridge, MA; Certification no. 1031219-2). It covers 200,859 ICU admissions of 139,367 patients in 2014 and 2015 at 335 ICUs from 208 hospitals across the USA. Specifically, the source hospital of MIMIC-III does not participate in the eICU-CRD program.
The data from the MIMIC-III database and the eICU-CRD are openly available. All personal information has been removed to protect the privacy of the patients. To access the databases, author Ge completed the National Institutes of Health's web-based course Protecting Human Research Participants (certification number: 36320014). Data extraction was performed using Navicat Premium Version 12.1.11 (PreimumsoftTM CyberTech Ltd., Hongkong SAR, China).
Study population
Patients with a diagnosis of TBI, defined as intracranial wound in the MIMIC-III database, and intracranial injury in the eICU-CRD, were potentially eligible for inclusion. Only those of the first ICU admission were chosen if they had more than one ICU stay record. Patients were excluded if they met the criteria: had no records of GCS within 24 h after admission, younger than 18 years old, had no binary sex, and/or had no records of whole blood RDW and Plt count at 72–120 h after admission.
Data extraction using the MeDICS method
Structure Query Language was used to extract and integrate data from the two databases. The following information was extracted: age, sex, GCS, pupil size and light reaction (< 24 h after admission), RDW and Plt count (72–120 h after admission), hospital mortality, ICU and hospital length of stay (LOS), neurosurgical operations, important past history, and comorbidities. The neurosurgical operations include therapeutic craniotomy, intracranial pressure monitoring, intracranial hemorrhage evacuation, burr-hole drainage of subdural hematoma, and external ventricular drainage. The past history and comorbidities include arteriosclerotic heart disease (ASHD), chronic obstructive pulmonary disease (COPD), high blood pressure (HBP), stroke, hematopathy/coagulopathy, hypotension (≤ 90/60 mm Hg within 24 h after admission), CNS infection, and pneumonia. The primary outcome of the study was hospital mortality, and the secondary outcomes included ICU LOS and hospital LOS.
For patients with GCS that recorded more than once within the first 24 h after admission, the lowest score was employed as the first-day GCS. For patients with pupil size or light reaction that recorded more than once within the first 24 h after admission, once there is a record that pinpoint or dilated pupil was observed, it would be included as pinpoint or dilated pupil. Besides, if there is a record indicating that the pupil light reaction is sluggish or non-reactive, it would be regarded as inactive for further analysis. In addition, the average RDW and Plt count of 72–120 h (approximately 4 days) after admission for each patient were calculated respectively, and the RPR value (4-DAA RPR) was then figured out using the two values.
To integrate the data from the MIMIC-III database and the eICU-CRD, ICU-stay-ID or patient-unit-stay-ID was regarded as the unique ID for each patient. Incompatible data such as patient-health system-stay-ID was excluded. The two databases have different definitions of the same diseases; thus, they were unified by manual review, and the disease codes were extracted accordingly. Besides, the same variables with inconsistent data types in the two databases, such as numbers and strings were also unified. Through the above method, the data quality could be greatly improved. This procedure of data integration and procession was developed and named as MeDICS (MIMIC-III and eICU Database Integrated Cohort Study) by our team.
Subgroup analysis and stratification
Subgroup analysis was conducted to explore the possible interaction between RPR, TBI severity, first-day pupil size and light reaction, neurosurgical operations, and other important factors affecting hospital mortality in clinical practice. Stratification was performed according to the first-day GCS (9–15, mild-moderate TBI; 3–8, severe TBI), first-day pupil size (not dilated, = 2 or 3 mm; unilateral dilated, ≥ 4 mm; bilateral dilated, ≥ 4 mm; pinpoint, ≤ 1 mm) and light reaction (bilateral reactive; unilateral inactive or sluggish; bilateral inactive or sluggish), whether underwent neurosurgical operations, past history and comorbidities.
Management of missing data and outliers
Variables with missing data are common in the MIMIC-III database and the eICU-CRD. As described in the “Study population” section, patients with missing records of first-day GCS, RDW, and Plt count were excluded from the analysis. Variables with more than 20% missing values such as patients' height and weight also were excluded. Besides, the RPR outliers that more than 0.36, the 85% quantile of (upper quartile +1.5 × interquartile range) were excluded as an erroneous entry.
Animals and grouping methods
Adult male C57BL/6 mice (aged 12 weeks, weighing 20–25 g) were purchased from the Chinese Academy of Military Science (Beijing, China). All experimental procedures in accordance with the National Institutes of Health Guide for the Care and Use of Laboratory Animals, and approved by the Tianjin Medical University Animal Care and Use Committee. The mice were quarantined and housed for 1 week before being randomly divided into four groups: Sham, TBI, TBI+SC75741, and TBI+MCC950. The treatment was first administered at 1 h post-injury. Briefly, SC75741 (Selleckchem, Houston, TX,), the NF-κB selective inhibitor, was applied to the mice (15 mg/mL, intraperitoneal injection) every 2 days until 14 days post-injury (DPI) according to the manufacturer's instructions. MCC950 (Selleckchem), the specific inhibitor of pyroptosis initiating receptor NLRP3, was dosed in the mice (10 mg/kg, intraperitoneal injection) daily for the first 3 days post-injury, and then every other day until 14 DPI. 14
Controlled cortical impact (CCI) mouse model
The CCI mouse model used in this study can result in injury to the cerebral cortex and hippocampus, and lead to vestibulomotor deficits and long-term neurocognitive dysfunctions as previously described. 15,16 Although animals do lose body weight, they rapidly regain spontaneous ventilation, righting reflex, and the ability to ambulate. Briefly, the mice were anesthetized with 10% chloride hydrate (3.0 mL/kg, intraperitoneal injection). They were then positioned in a stereotaxic device using ear bars. Following a midline scalp incision, a 3.0-mm craniotomy was performed centrally over the right parietal bone. The impounder tip of the injury device (eCCI model 6.3, American Instruments, Richmond, VA) was then extended to its full impact distance, positioned on the surface of the exposed dura mater, and reset to impact its surface. To induce moderate brain injury, the impact parameters were set as: 4.5 m/sec velocity, 2.0-mm depth, and 200-msec dwell time. After the impact, the craniotomy was closed with bone wax, and the mice were placed in a well-ventilated cage at 37°C until they regained consciousness. Sham-operated mice underwent the same procedures except for the cortical impact.
RDW and Plt count determination
The mice were anesthetized with 10% chloride hydrate by intraperitoneal injection at 1 and 3 DPI. Whole–blood samples were then collected via cardiac puncture, and were anticoagulated with heparin. RDW and Plt count determination were obtained using Sysmex XN-2000 automated Hematology Analyzer (Kobe, Hyogo, Japan).
Enzyme-linked immunosorbent assay
Brain extracts from cerebral cortex of the mice were collected at 3 DPI. Enzyme-linked immunosorbent assay of the inflammatory mediators, including tumor necrosis factor (TNF)-α, interleukin (IL)-1β, and IL-10 were determined referring to the manufacturer's instructions (Cat# MTA00B, MLB00C, M1000B; R&D, Minneapolis, MN).
Modified Neurological Severity Score (mNSS) test
The mNSS test includes motor, sensory, reflex, and balance evaluations. It was conducted pre-injury and at 1, 3, 7, and 14 days post-CCI by an observer who was blinded to the experimental conditions and treatments.
Morris Water Maze (MWM) test
The MWM test was performed to evaluate spatial learning and memory ability of TBI mice as we previously reported. 17,18 For the spatial acquisition trial, the mice were placed in a pool (105 cm diameter) filled with room temperature water, and allowed up to 90 s to locate a submerged platform. The mice performed four trials a day with a 30-min inter-trial interval for four consecutive days (14–17 DPI). They were introduced in varying quadrants (northwest, northeast, southwest, and southeast) of the pool for each trial, but the location of the platform was fixed. The latency-time to reach the platform was recorded, and the four trials were averaged. For the probe trial conducted at 18 DPI (24 h after the last spatial acquisition trial), the mice were allowed to swim freely without the platform for 60 sec. The percentage of the time spent in goal quadrant was measured. In addition, SC75741 and MCC950 treatment were not administered during the test.
Novel Object Recognition test
The Novel Object Recognition (NOR) test was carried out to evaluate cognitive function of TBI mice at 14 DPI as reported. 19,20 Briefly, the mice were administered to freely explore a 40 × 40 × 50 cm open-field box for 10 min at the beginning. In the familiarization session, the mice were allowed to explore two similar objects. A stopwatch with two channels was used to record the time spent exploring each object until 20 sec of total exploration time or 10 min of the session time has been reached. In the test session conducted 6 h later, one of the two objects was replaced by a novel object, and the mice were allowed to explore them for 10 min. The amount of time that the mice spent on exploring each object was recorded, and the index of exploring time on the novel object over the total exploring time was calculated.
Statistical analysis
For the data collected from the MIMIC-III database and the eICU-CRD, continuous variables were expressed as mean ± standard deviation (SD), and compared using the Student's t-test, Wilcoxon rank sum test or Kruskal-Wallis rank sum test, as appropriate. Categorical data were expressed as number (percentage) and compared using the chi-square test.
The association between RPR and hospital mortality, ICU LOS as well as hospital LOS was determined using the logistic regression model and presented as odds ratio (OR) with 95% confidence interval (CI). The RPR values were divided into quartiles, with the first quartile (< 0.057) selected as the reference group. Multivariable logistic regression analyses were used to control confounders. Model 1 was adjusted for the confounders age and sex. Model 2 was adjusted for the confounders age, sex, first-day GCS, first-day pupil size and light reaction, and neurosurgical operations. Model 3 was adjusted for the confounders age, sex, first-day GCS, first-day pupil size and light reaction, neurosurgical operations, past history, and comorbidities including ASHD, COPD, HBP, stroke, hematopathy/coagulopathy, hypotension, CNS infection, and pneumonia. These confounders were selected based on their potential influences on RPR or hospital mortality. Potential multicollinearity was tested using the variance inflation factor, with a value of ≥ 5 indicating the presence of multicollinearity.
The Lowess Smoothing technique was used to explore the crude relationship between RPR and hospital mortality. A receiver-operating characteristic (ROC) curve was depicted to show the prognostic performance and confirm the best cut-off value. The stepwise backward elimination method with a significance level of 0.05 was used to develop a nomogram. The Harrell's C-index was determined to evaluate its discriminative ability, and the Hosmer-Lemeshow test was used to test the goodness of fit. Ten-fold cross-validation was performed to confirm the prognostic value of the model, and protects against overfitting by RStudio Version 1.3.1056 (Rstudio Corp., Boston, MA).
All data from the in vivo study were based on at least three independent experiments. The data were expressed as mean ± SD, except for that of the spatial acquisition trials of the MWM test, which are expressed as mean ± standard error of mean (SEM). Data of the mNSS test and the spatial acquisition trials of the MWM test were analyzed using a two-way analysis of variance (ANOVA), followed by the least square difference (LSD) post hoc test. For other data, statistical comparisons were analyzed using Student's t-test or one-way ANOVA followed by LSD post-hoc test, as appropriate. Pearson's correlation test was utilized to calculate the correlation coefficients between RPR and the neurological outcome of TBI mice.
All statistical analyses were performed using Stata/MP Version 14.0 (Stata Corp., College Station, TX) and PASW Statistics Version 18.0 (IBM, Armonk, NY). A two-tailed p value of less than 0.05 was considered to be statistically significant.
Results
Study population and baseline characteristics
In all, 2220 patients who met the selection criteria were enrolled, including 1966 survivors and 254 non-survivors, establishing a hospital mortality rate of 11.4%. The detailed procedure for population selection was shown in Figure 1. Demographic characteristics of the survivors and non-survivors were presented in Table 1 (the study population with the data of first-day RDW and Plt count were shown in Supplementary Table S1). Patients with TBI who presented to MIMIC and eICU-CRD research program (63.2 years old) were older than those in previous studies (45–55 years old) and often had more comorbidities, because most of the patients in the two ICU cohorts are critically ill, and patients younger than 18 years old were excluded. Given that this data feature will not affect statistical analysis and results interpretation, we found that the survivors of TBI tended to be younger than non-survivors, with a higher first-day GCS, a higher rate of dilated or pinpoint pupil with inactive light reaction, and a lower neurosurgical operation rate, suggesting that the survivors had milder primary injury than the non-survivors. In addition, there were fewer survivors with past history of hematopathy/coagulopathy, and complication of hypotension or pneumonia. For the indicators of the laboratory tests, RPR and RDW were lower for survivors than non-survivors, and Plt count was higher for survivors.

Flow chart of the study population. In all, 2220 patients who met the selection criteria were enrolled. GCS, Glasgow Coma Scale; Plt, platelet; RDW, red cell distribution width; RPR, RDW to Plt count ratio, TBI, traumatic brain injury.
Baseline Characteristics of the Patients with TBI (72–120 h after Admission)
p < 0.001; * p < 0.05
TBI, traumatic brain injury; GCS, Glasgow Coma Scale; ICU, intensive care unit; LOS, length of stay; ASHD, arteriosclerotic heart disease; COPD, chronic obstructive pulmonary disease; HBP, high blood pressure; CNS, central nervous system; RDW, red cell distribution width; Plt, platelet; RPR, red cell distribution width to platelet count ratio.
High RPR associates with increased hospital mortality of TBI
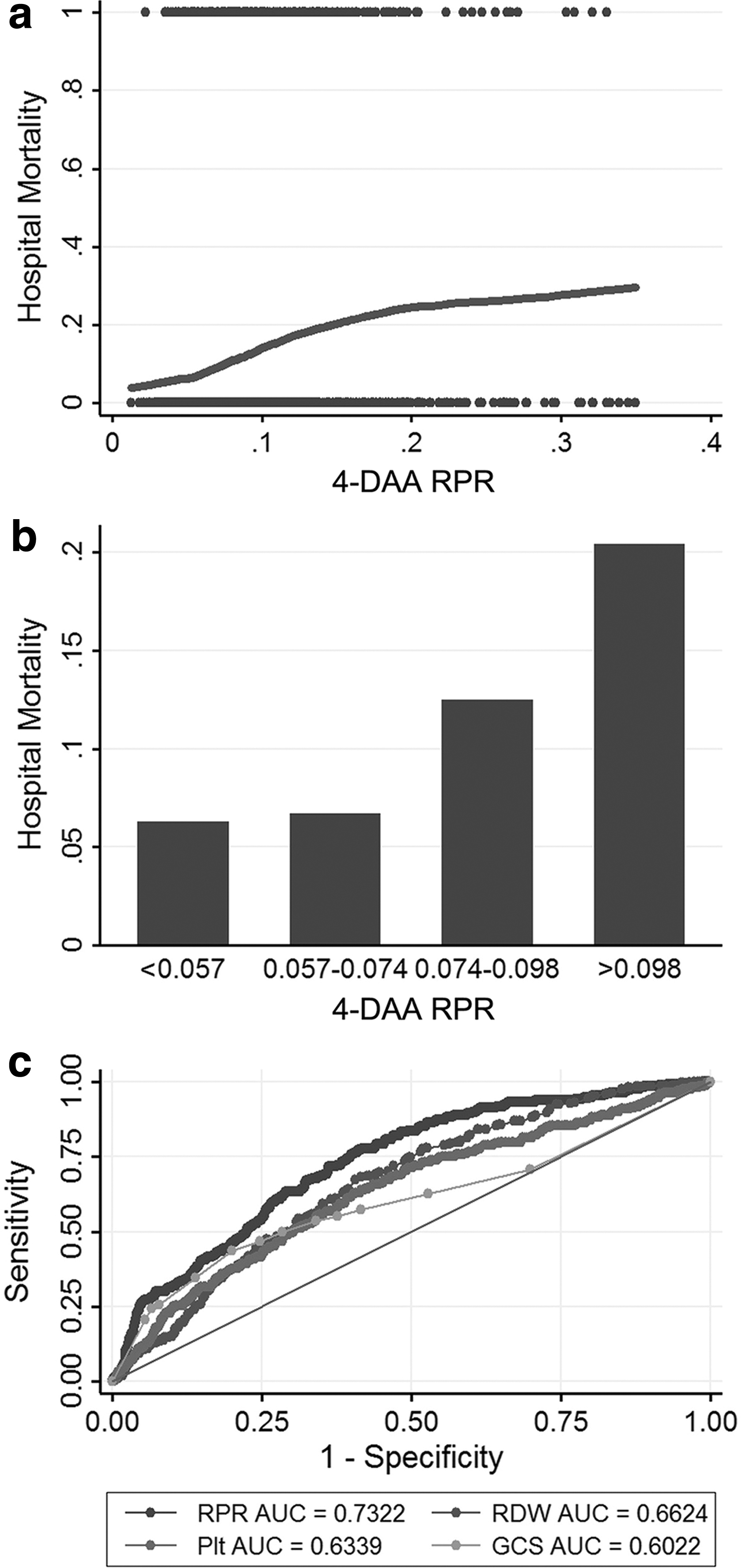
The relationship between 4-DAA RPR and hospital mortality for patients was shown in Figure 2A using the Lowess Smoothing technique (the Lowess Smoothing for the first-day RPR and hospital mortality was shown in Supplementary Fig. S1A). It yielded an approximate linear relationship, with the largest slope in the RPR interval of 0.05–0.2. In addition, 4-DAA RPR was also correlated with ICU length of stay (F = 39.16, regression coefficients ± SEM = 19.56 ± 3.13; p < 0.001) and hospital length of stay (F = 21.94, regression coefficients ± SEM = 21.81 ± 4.66; p < 0.001). Further, the group with the first RPR quartile (< 0.057) was selected as the reference for all comparisons in multivariable logistic regression models. As shown in Table 2, the odds ratio (OR) with 95% confidence interval (CI) for the second (0.057–0.074), third (0.074–0.098), and fourth (> 0.098) quartile in the crude model was 1.07 (0.67–1.73), 2.13 (1.39–3.28), and 3.82 (2.55–5.72), respectively. Therefore, high RPR was associated with increased hospital mortality, and the association between them was more significant in the relatively higher RPR quartiles (> 0.074), while the second quartile showed no increased mortality risk (also shown in Fig. 2B). A similar trend was also observed in Model 1, Model 2, and Model 3, in which the confounders including age, sex, first-day GCS, first-day pupil size and light reaction, neurosurgical operations, past history, and comorbidities were successively adjusted. For example, the fourth quartile had a higher OR (95% CI) and a lower p value than the third quartile in all models.
Association between 4-DAA RPR and hospital mortality of patients with TBI.
The ORs for All-Cause Mortality across Groups of the 4-DAA RPR
p < 0.001; ** p < 0.01; * p < 0.05
Multivariable logistic regression models were used to calculate ORs with 95% CI. Model 1 was adjusted for the confounders age and sex. Model 2 was adjusted for the confounders age, sex, first-day GCS, first-day pupil size and light reaction, and neurosurgical operations. Model 3 was adjusted for the confounders age, sex, first-day GCS, first-day pupil size and light reaction, neurosurgical operations, past history and comorbidities including ASHD, COPD, HBP, stroke, hematopathy/coagulopathy, hypotension, CNS infection, and pneumonia. The mean variance inflation factor was 4.44 and 2.72 for Model 2 and Model 3, respectively.
OR, odds ratio; DAA, days after admission; RPR, red cell distribution width to platelet count ratio; CI, confidence interval.
The outcome prediction value of 4-DAA RPR was examined using the ROC curve. As shown in Figure 2C, its prognostic performance was moderately good for hospital mortality (AUC = 0.7362) with a cut-off value of 0.0734. Besides, compared with RDW (AUC = 0.6624), Plt count (AUC = 0.6339) and first-day GCS (AUC = 0.6022), which could not be regarded as an effective indicator for the poor outcome of TBI, 4-DAA RPR had an obvious advantage on prognosis prediction.
For the first-day RPR analysis, its association with the mortality was shown in Supplementary Figure S1B. The results indicated that only the 4th RPR quartile (> 0.089) referred to increased risk of mortality, while the second (0.055–0.069) and the third (0.069–0.089) quartile showed no significance in all models (Supplementary Table S2). In addition, the AUC value for first-day RPR was 0.6065 (Supplementary Fig. S1C), and the cut-off value was 0.0915 (higher than that of 4-DAA RPR). These results suggested poor sensitivity and discrimination of first-day RPR for predicting the mortality of acute TBI. Moreover, linear correlation could not be observed between first-day RPR and ICU length of stay (F = 1.88, regression coefficients ± SEM = 3.73 ± 2.72; p = 0.171), as well as hospital length of stay (F = 1.68, regression coefficients ± SEM = 5.36 ± 4.13; p = 0.195).
Subgroup analysis confirms the association between RPR and hospital mortality of TBI
As shown in Table 3, subgroup analysis revealed the associations between 4-DAA RPR and the mortality risk of TBI patients with different injury severities, first-day pupil size and light reaction, neurosurgical operations, past history, and comorbidities. After adjusting for covariates, the interactive effects were detected in the first-day GCS (p = 0.005), pupil light reaction (p < 0.001), neurosurgical operations (p = 0.015), and hematopathy/coagulopathy (p = 0.002). The forest plot for subgroup analysis with RPR of 0074–0.098 and > 0.098 were shown in Figure 3.
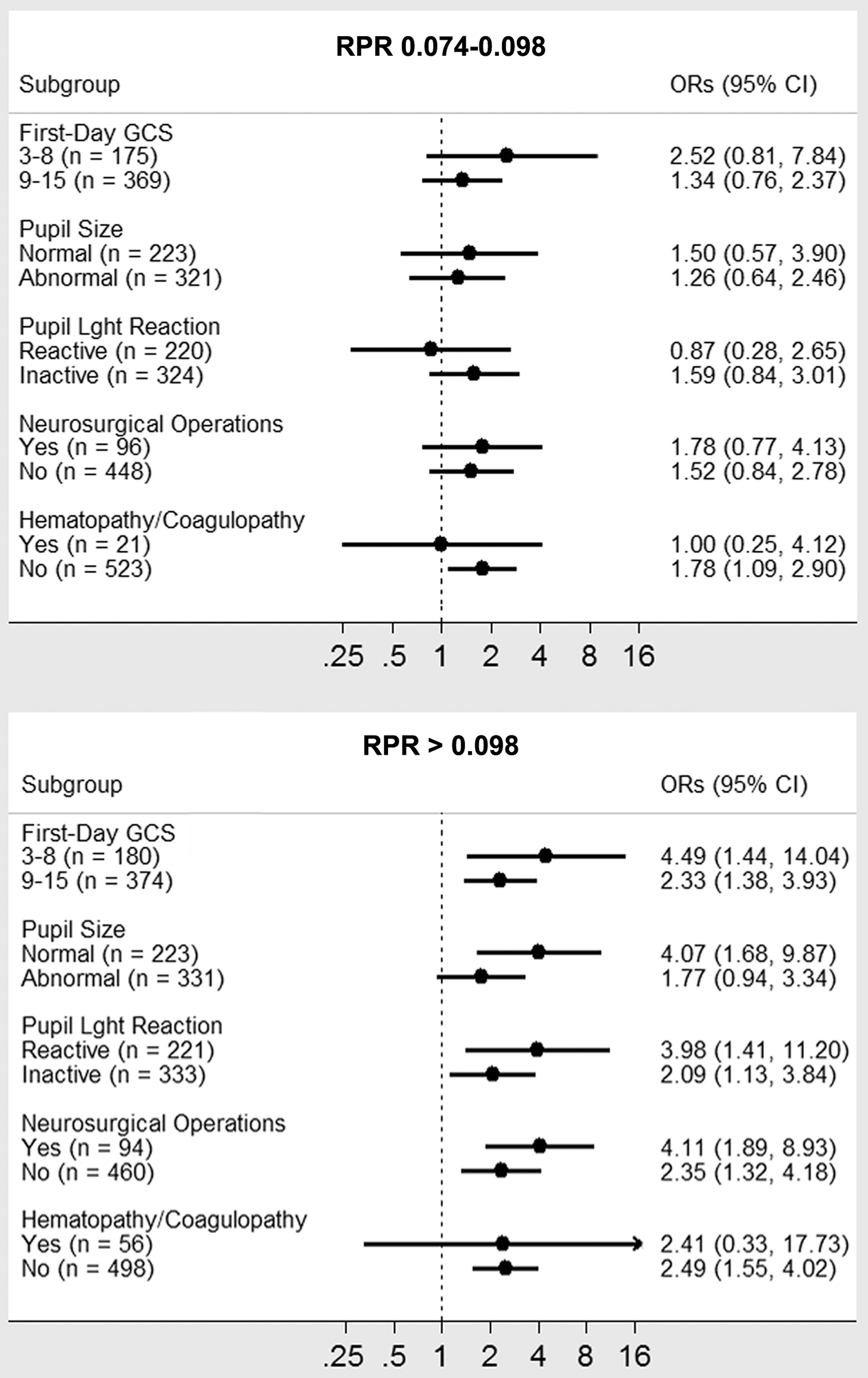
Forest plot for subgroup analysis of the association between hospital mortality and RPR. The interactive effects were detected in the first-day GCS, pupil size, pupil light reaction, neurosurgery, hematopathy/coagulopathy, hypotension, and pneumonia subgroups. GCS, Glasgow Coma Scale; RPR, red cell distribution width to platelet count ratio.
Subgroup Analysis of the Associations between 4-DAA RPR and Mortality
p < 0.001, ** p < 0.01, * p < 0.05
Confounders adjustment were performed as in Model 3. Multivariable logistic regression models were used to calculate ORs with 95% CI.
DAA days after admission; RPR, red cell distribution width to platelet count ratio; OR, odds ratio; CI, confidence interval; GCS, Glasgow Coma Scale; ASHD, arteriosclerotic heart disease; COPD, chronic obstructive pulmonary disease; NA, not applicable; HBP, high blood pressure; CNS, central nervous system.
For subgroup analysis of the associations between first-day RPR and hospital mortality (Supplementary Table S3), the interactive effects were only detected in the first-day GCS (p < 0.001), pupil size (p < 0.001), pupil light reaction (p < 0.001), hypotension (p = 0.001), and hematopathy/coagulopathy (p < 0.001) subgroups, indicating that 4-DAA RPR was more applicable than first-day RPR in clinical practice.
Development of multivariate prognostic nomogram
Although the discriminative ability of RPR is moderately good, a monogram was constructed to further improve the prognostic value for TBI mortality. Nine factors that found correlated with hospital mortality of TBI, including RPR, age, first-day GCS, first-day pupil size, first-day pupil light reaction, neurosurgery, hematopathy/coagulopathy, hypotension, and pneumonia were included in the stepwise backward eliminating logistic model (Fig. 4). Nomogram weightings for each factor were derived from the β coefficients. The factors contributed points; therefore, increased total points were associated with greater probability of mortality. A C-index of 0.8716 was obtained. It suggested that the nomogram had a good discriminative ability with respect to the C indices of the univariable models incorporating each of the individual variables used to construct the nomogram. In addition, the Hosmer-Lemeshow test showed a p value of 0.2497, which indicated no reason to reject the null hypothesis of no difference between predicted and observed mortality probabilities. Ten-fold cross-validation suggested that the mean C-index was 0.8695 and the mean Brier Score was 0.0717, thus confirmed the model does not have overfitting, and has a high prognostic value.

Nomogram to predict hospital mortality of patients with TBI. To estimate the mortality risk for a given patient, locate the RPR value and draw a line straight up to the Points axis to determine the associated score. Repeat the process for 4-DAA RPR, age, GCS, pupil size, pupil light reaction, neurosurgery, hematopathy/coagulopathy, hypotension, and pneumonia. Then, sum the scores and locate them on the Total Points axis. Finally, draw a vertical line to the Mortality Risk axis and read off the probability. DAA days after admission; GCS, Glasgow Coma Scale; RPR, red cell distribution width to platelet count ratio; TBI, traumatic brain injury.
Anti-inflammatory treatments decrease RPR after TBI on mice model
To validate the clinical findings on in vivo model, the whole–blood RDW and Plt count of TBI mice were determined. We observed that RPR was decreased at 1 and 3 DPI, which was more significant at 3 DPI than 1 DPI (Supplementary Fig. S2A). Meanwhile, changes with marginal statistical differences in the RDW and Plt count were observed at 3 DPI, but not 1 DPI (Supplementary Fig. S2B). In addition, the anti-inflammatory agents SC75741 and MCC950 that inhibited the expression levels of inflammatory mediators (TNF-α, IL-1β, and IL-10) in brain and serum (Supplementary Fig. S2C-S2H), could reverse the level changes on RPR at 1 and 3 DPI (Supplementary Fig. S2A, S2B). These results suggested that increased RPR after TBI were a manifestation of CNS and systemic inflammatory response.
RPR is negatively correlated with the neurological outcome of TBI mice
The neurological outcome of TBI mice was evaluated by the mNSS, MWM, and NOR test. In the mNSS test, lower neurological scores demonstrate better neurological function. As shown in Supplementary Figure S3A, no difference on the neurological score at 1 DPI was observed in the experimental groups. The recovery of neurological function began at 3 DPI, and lasted to 14 DPI, when the injured mice still had residual neurological deficiencies. Compared with the TBI group, the neurological score was decreased in the TBI+SC75741 and TBI+MCC950 group at 14 DPI, suggesting that the anti-inflammatory treatments improved the neurological score of TBI mice.
In the MWM test, the spatial acquisition trials were performed to test spatial learning ability. Escape latency, which represents the capability to navigate from a starting location to a submerged platform, was gradually decreased in the testing procedure, indicating that a spatial memory was established [F (3, 128) = 327.7, p < 0.001; Supplementary Fig. S3B]. The probe trials were conducted to test the retrograde reference memory, in which more time spent in goal quadrant indicates better memory. Compared with the TBI group, TBI+SC75741 and TBI+MCC950 group showed shortened escape latency in the spatial acquisition trials and prolonged time spent in goal quadrant in the probe trials (Supplementary Fig. S3C). It indicated that the anti-inflammatory treatments improved the spatial learning and memory ability of TBI mice.
In the NOR test, the amount of time taken to explore the new object provides an indicator for cognitive memory. We found that the index of exploring time on the novel object over the total exploring time was increased in the TBI+SC75741 and TBI+MCC950 group, compared with the TBI group (Supplementary Fig. S3D). Hence, the anti-inflammatory treatments contributed to the recovery of cognitive function after TBI.
As the anti-inflammatory treatments could decrease RPR in TBI mice, the Pearson's correlation coefficients for RPR and the neurological outcome were further calculated. The results suggested strong associations between the following: 1) RPR and latency-time in the MWM test; 2) RPR and time spent in goal quadrant in the MWM test; and 3) RPR and NOR index (Supplementary Fig. S3E). To sum up, RPR was negatively correlated with the neurological outcome of TBI mice. These results further confirmed the results of our clinical findings.
Discussion
Hemodynamic changes and systemic inflammation are always observed in patients with acute TBI. The release of inflammatory mediators following injury could induce tissue damage, red blood cell destruction and structural changes, as well as platelet aggregation and accelerated consumption, which finally result in the dysfunction of neurovascular unit and increased risk of poor prognosis. 21 Routinely conducted during hospitalization, the CBC analyses contain several parameters that reflect the above pathological changes. Of these parameters, RDW and Plt count which have potential to indicate the mortality risk of TBI was selected to be investigated in this research. Using the MeDICS method, we found that their ratio—RPR, a novel easily accessible index—is a reliable predictor for the outcome of acute TBI.
RDW represents the heterogeneity in size of erythrocytes, of which the higher values indicate greater variation. Recently, it has gained substantial attention as an indicator of inflammation, 22 and a prognostic marker for various diseases independent of hemoglobin values. 23 A research on the association between aging of hematopoietic stem cells and oxidative stress molecules, such as reactive oxygen species, super-oxide dismutase, and glutathione peroxides, revealed that abnormally increased RDW can well indicated the above pathological changes. 24 It has also been suggested that elevated RDW was related to suboptimal health status that involves chronic inflammatory response and impairment of red cell generation. Specifically, pro-inflammatory cytokines can affect the survival of erythrocytes in circulation, damage the membranes, suppress maturation, and accelerate the entry of newer, larger reticulocytes into the peripheral circulation, thereby leading to the increase of RDW. 25 In the present study, RDW was observed to be increased in patients with TBI at 3–5 days post-admission. However, although the RDW value were lower in survivors than in non-survivors, further statistical analysis found that it had no effect on predicting the prognosis of acute TBI.
Platelets, along with their well-known roles in hemostasis, are active participants in regulating inflammation. Specifically, while adhering to coagulation factors, platelets also carry a large number of inflammatory factors such as TNF-α, interleukins, and serotonin, which are involved in tissue damage and repair. Decreased Plt count is a common pathological phenomenon in patients with acute and critical illness. Its underlying mechanism may involve: 1) reduced platelet production due to infectious and inflammatory damage to megakaryocytes, and bacterial endotoxins that inhibit the function of bone marrow megakaryocytes; 2) increased platelet destruction and consumption caused by severe infection-induced diffuse intravascular coagulation; and 3) destruction of platelet production led by complement activation through immune pathways. 26 Studies on sepsis observed a reduction of Plt count in patients, which was correlated with the severity of the disease, and a risk factor for poor prognosis. 27 Besides, platelets played a pivotal role in the inflammatory response in hepatic injury and burn injury. 28, 29 In the present study, a substantial decline in Plt count was observed at 3–5 days post-admission, and the decrease of Plt count in non-survivors were lower than that of survivors. Even so, similar to RDW, Plt count could not independently infer prognostic information of acute TBI.
RPR has been recently considered as an index that reflects inflammation severity by combining the diagnostic/prognostic advantages of RDW and Plt count. As a routinely available marker, RPR was recognized as a strong predictor for hepatic fibrosis and hepatitis, 30,31 acute pancreatitis, 32 ascending thoracic aortic aneurysm, 33 and myocardial infarction. 34 In addition, high RPR on Days 3 and 7 could be observed in patients with severe burn injury, which indicated poor prognosis of the disease. 35 Parallel to these studies, the increased RPR also was reported to be correlated with the severity (disease scores) of inflammatory factors in systemic lupus erythematosus. 36 From this, RPR would be a powerful indicator for inflammation.
The present study provided solid evidence for early recognition on the mortality risk of TBI using RPR. Although the exact mechanism underlying the poor prognosis of TBI patients with elevated RPR remains unclear, it may be partially attributed to the development inflammation following injury. In vivo experiments were thus designed to explore related mechanisms. As an upstream switch of inflammatory response, NF-κB signaling exerts important effects on regulating the development of neuroinflammation in acute TBI 37 and chronic traumatic encephalopathy. 38 In addition, our previous researches found that pyroptosis in injured brain after TBI can trigger the inflammatory cascade, and lead to the dysfunction of neurovascular unit. 14,39 In the present study, we used specific inhibitors that block NF-κB and pyroptosis-activated receptor NLRP3 to observe the level changes on RDW, Plt count, and RPR under the condition of inflammatory suppression. RDW decline and Plt count increase with marginal statistical differences were observed after anti-inflammatory treatments at 3DPI. Meanwhile, RPR was also decreased notably after the treatments, suggesting that it is a powerful indicator of inflammation in acute TBI. In addition, the results of neuro-functional tests indicated that RPR value was closely related to the neurological outcome of TBI mice receiving anti-inflammatory treatments. These findings confirmed the association between RPR, post-traumatic inflammation, and neuro-outcome after TBI, and further emphasized the importance of controlling inflammatory response in clinical treatment.
Our research simultaneously explored the association between RPR and the mortality risk of acute TBI at two important time-points post-injury. We found that 4-DAA RPR turned out to be strongly associated with the endpoint of TBI, but first-day RPR had no prognostic value. Besides, similar results also were observed in in vivo experiments. We believe that these findings could be explained by the development of inflammation. Specifically, the inflammation peak after TBI mostly occurs at 3–5 days post-injury. This time-point is also the peak period of brain edema with massive activation of microglia and astrocytes, release of inflammatory mediators into the CNS and peripheral circulation, and homing of activated neutrophils and immune cells (e.g., T cells and NK cells) to the injured brain tissue. 13 However, in the hyper-acute phase of TBI (< 24 h post-injury), the CBC parameters may be interfered by shock and acute stress reaction. In addition, the glial cells in the brain are not widely activated at this time, and the peripheral inflammatory and immune cells have not completed their homing, leading to the limitation of focal brain inflammation to the injury site. 40 Consequently, the prognostic value of 4-DAA RPR for TBI was much higher than that of first-day RPR. Moreover, with the use of our nomogram that consisted of RPR, GCS, pupil size and light reaction, and other risk factors, the predicting value of RPR can be further improved. The strength of this nomogram is that it was built from physical examination and easily diagnosed medical history or comorbidities. Therefore, it can be used in resource-limited settings, where clinicians are still likely to have all the data required to use it effectively.
Several limitations of this study should be taken into account when interpreting the results. First, the retrospective nature of the design limited the research. Patients' information of head CT scan images, Abbreviated Injury Scale - Injury Severity Score at admission, and Glasgow Outcome Scale-Extended were not designed to be collected in the databases. Second, this research failed to include other risk factors, such as chronic liver disease, chronic renal disease, diabetes mellitus, sepsis, and malignancy, as well as other endpoints such as ICU mortality and hospital/ICU length of stay. Third, except for the 10-fold cross-validation on our datasets, an external dataset for validation needs to be built in the future in order to further avoid overfitting. To address above questions, a multi-center prospective study is being organized in several neurological centers in China to confirm the findings of this research and promote its clinical implementation.
Conclusion
Due to the low cost, highly reproducible and routinely available RPR can be a useful clinical predictor of mortality for patients with acute TBI. The level change of RPR after TBI is attributed to the development of inflammation, which further emphasizes the importance of controlling inflammatory response in clinical treatment. In addition, the nomogram generated from RPR, GCS and other risk factors can further improve the prognostic value of RPR, thus be proposed as a prognosis evaluation aid for TBI in all levels of medical system.
Footnotes
Acknowledgments
The manuscript has been posted to a preprint server (DOI: 10.21203/rs.3.rs-80607/v1). The authors express acknowledgement to Prof. Rongcai Jiang from Department of Neurosurgery, Tianjin Medical University General Hospital, and Prof. Yongmei Li from School of Basic Medical Sciences, Tianjin Medical University for their support.
Funding Information
This research was supported by grants from National Natural Science Foundation of China (No. 82071394, 82072166, and 81930031) and Natural Science Foundation of Tianjin Municipal Science and Technology Commission (No. 18JCQNJC81100).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.