
Abstract
Children frequently present to an Emergency Department (ED) after concussion, and headache is the most commonly associated symptom. Recent guidelines emphasize the importance of analgesia for post-concussion headache (PCH), yet evidence to inform treatment is lacking. We sought to characterize abortive therapies used to manage refractory PCH in the pediatric ED and factors associated with treatment. A scenario-based survey was distributed to ED physicians at all 15 Canadian tertiary pediatric centers. Participants were asked questions regarding ED treatment of acute (48 h) and persistent (1 month) PCH refractory to appropriate doses of acetaminophen/ibuprofen. Logistic regression was used to assess factors associated with treatment. Response rate was 63% (137/219). Nearly all physicians (128/137, 93%) endorsed treatment in the ED for acute PCH of severe intensity, with most selecting intravenous treatments (116/137, 84.7%). Treatments were similar for acute and persistent PCH. The most common treatments were metoclopramide (72%), physiologic saline (47%), and nonsteroidal anti-inflammatory agents (NSAIDS; 35%). Second-line ED treatments were more variable. For acute PCH of moderate intensity, overall treatment was lower (102/137, 74%; p < 0.0001), and NSAIDS (48%) were most frequently selected. In multi-variable regression analyses, no physician- or ED-level factor was associated with receiving treatment, or treatment using metoclopramide specifically. Treatment for refractory PCH in the pediatric ED is highly variable. Importantly, patients with severe PCH are most likely to receive intravenous therapies, often with metoclopramide, despite a paucity of evidence supporting these choices. Further research is urgently needed to establish the comparative effectiveness of pharmacotherapeutic treatments for children with refractory PCH.
Introduction
Concussions are a serious public health concern and Emergency Department (ED) visits for concussion have risen markedly across all age groups. 1 Pediatric ED visits for concussion increased approximately 25% between 2006 and 2010, reaching an estimated incidence of 886/100,000 among children and adolescents aged 3–17 years. 1 Post-concussion headache (PCH) is the most common presenting symptom, 2 –4 affecting nearly 80% of children seeking ED care. 5
Children and adolescents are at elevated risk of prolonged symptoms after concussion. Data suggest that 31% of children report persistent post-concussion symptoms at 28 days after injury, 6 with 8% to 43% still experiencing PCH at three months. 4,7,8 Acute PCH is thought to be explained by direct trauma, axonal injury, and altered cerebral metabolism and hemodynamics, 9 whereas persistent PCH may involve pathways related to chronic pain leading to progressive increases in pain intensity. 10 Despite potential differences in pathophysiology, both acute and persistent PCH are associated with significant detriments to daily functioning and quality of life for many children and adolescents. 11
Current guidelines emphasize the importance of managing PCH using nonopioid analgesics. 12,13 No evidence-based treatment recommendations for PCH exist, 9,14,15 however, particularly when common first-line therapies such as acetaminophen and ibuprofen have failed. There remains an urgent need for studies defining safe and effective treatments for those with refractory pediatric PCH. 12,16 In the absence of evidence, understanding physician treatment practices is important to inform future therapeutic trials and comparative effectiveness studies. The objective of this study was to describe abortive therapies most frequently reported by pediatric ED physicians for the management of acute and persistent PCH refractory to nonopioid analgesia, and to characterize factors affecting physician treatment decisions.
Methods
The study population included ED physician members of the Pediatric Emergency Research Canada (PERC) network. PERC is a consortium of all 15 Canadian academic pediatric hospitals aimed at facilitating multi-center research studies and which maintains an e-mail list of full-time ED physicians at affiliated EDs. 17 The number of children cared for at PERC sites ranges from 12,000–84,000 annual ED visits (median 52,000; interquartile range [IQR] 38,000–78,000), and physician membership ranges from 29–86% by site. 17 Physicians were contacted using the 2018 PERC member list as described previously, 18 and participants were able to complete the survey between January 11, 2018 and April 8, 2018.
The ED physician treatments for PCH were assessed using a scenario-based electronic survey consisting of multiple-choice and open-ended questions (Supplement S1). Participants were presented two cases of an adolescent assessed in the ED for PCH affecting daily activities and refractory to appropriate use of acetaminophen and ibuprofen. To focus on treatment choices, the scenarios pre-specified a clear PCH diagnosis with normal neuroimaging. To elicit responses reflecting the possible different pathophysiology of acute and persistent pain, the scenarios differed only with respect to timing of presentation after injury—acute PCH at two days and persistent PCH at one month, in keeping with recognized definitions. 16 All questions and response options were identical for both scenarios.
Participants were asked which abortive treatments they would offer in the ED initially and after 2 h of ongoing pain, as well as how their management would differ for the treatment of severe (9/10) versus moderate (4/10) pain intensity. Response options did not include acetaminophen and ibuprofen, and respondents were specifically limited to a maximum of two treatment options per scenario to identify the most prioritized treatments. In addition, respondents were asked to predict the effectiveness of their selected treatments.
Survey design followed methodology as described previously. 18,19 Item generation for multiple-choice responses was achieved through a detailed literature review of treatments offered for post-traumatic and primary headaches. Item reduction was an iterative process by the research team with expertise in concussion diagnosis and management. 5,6,11 In addition to the treatment list provided, participants were able to select “Other” and specify details using free-text.
The electronic survey was developed in both Canadian national languages (French and English) and pilot tested for technical usability and clarity. The pilot group comprised 10 individuals not included in the study. The final survey was administered using a web-based platform (LimeSurvey Software, Hamburg, Germany). Survey distribution used a modified Dillman tailored design, 20 which included an initial invitation e-mail, followed by two automatically generated reminder e-mails for nonrespondents at two-week intervals.
Each participant was assigned a personalized survey link and could complete the questionnaire only once. Participants were able to review their responses until the survey was submitted. Consent was obtained before commencing the survey, and group data were extracted anonymously by investigators blinded to individual responses.
Descriptive statistics were tabulated, and McNemar testing was used to compare paired proportions among individual physicians between case scenarios. All survey fields were mandatory such that there were no missing data. We performed univariable and multi-variable regression to explore factors associated with treatment of severe acute PCH. Covariates of interest included physician training, years in practice, proportion of practice with pediatric patients, PCH treatment frequency, and availability of institution-specific PCH or status migrainosus clinical decision tools (any protocol, guideline, or clinical pathway).
Candidate predictors were graphically inspected using scatter plots to ensure the underlying assumptions of logistic regression were met. Variables were assessed for multi-collinearity using the variance inflation factor (VIF) and retained in the final model VIF <10. Regression modeling was performed using Stata v.14.1 (StataCorp, College Station, TX). Results are reported in accordance with the CHERRIES checklist for internet e-surveys. 21 The study was approved by the Research Ethics Board of the McGill University Health Centre.
Results
Survey response rate was 62.6% (N = 137/219). Demographic characteristics of survey participants are summarized in Table 1. Two-thirds of participants (88/137, 64.2%) were trained in Pediatrics with Pediatric Emergency Medicine subspecialty training. The majority of physicians reported that 76–100% of their ED practice is with pediatric patients. Nine (6.6%) participants from six centers reported having some form of institutional clinical decision tool for the management of PCH in the form of a protocol, guideline, or clinical pathway. Clinical decision tools for status migrainosus were reportedly more common (81/137, 59.1%; 10 centers); however, routine use of these tools was variable.
ED, Emergency Department; PCH, post-concussion headache
Clinical decision tool in the form of a protocol, guideline. or clinical pathway.
For patients with severe PCH presenting acutely, 128/137 (93.4%) respondents endorsed providing some form of abortive treatment in the ED. Treatment selections for severe acute PCH were highly variable (Fig. 1A). The most commonly selected treatments were intravenous (IV) metoclopramide (99/137, 72.3%), followed by an IV fluid bolus of physiologic saline (65/137, 47.4%) and administration of nonsteroidal anti-inflammatory agents (NSAIDS; 48/137, 35.0%). Two respondents endorsed using IV hypertonic 3% saline. At least one IV treatment was favored for severe acute PCH (116/137, 84.7% overall), with IV routes selected by 58% of NSAID users (IV ketorolac) and all but one respondent for metoclopramide. Medications selected for treatment of ongoing headache after 2 h (second-line treatment) were more variable still, with an increase in the use of corticosteroids.

Abortive therapies for post-concussion headache (PCH); Treatment of severe acute (panel
For treatment of severe persistent PCH, therapeutic selections were largely unchanged from selections for severe acute PCH (Fig. 1B). Again, a majority of respondents (125/137, 91.2%), provided some form of treatment. The most commonly selected treatments for severe persistent PCH were IV metoclopramide (87/137, 63.5%), IV physiologic saline bolus (56/137, 40.9%) and NSAIDS (43/137, 31.4%).
For acute PCH of moderate intensity, two-thirds of respondents (86/137, 62.8%) reported that their choice of first-line abortive treatment would differ from what was offered for severe pain. Fewer respondents provided ED treatment compared with severe acute PCH (102/137, 74.5%; p < 0.0001), and more than half would administer only oral treatments (58/102, 56.9%). The most commonly selected medications were oral NSAIDS (66/137, 48.2%), followed by IV metoclopramide (41/137, 29.9%) and IV physiologic saline bolus (28/137, 20.4%). First-line treatment selections were similar for moderate PCH whether seen at 48 h or at one month.
When selecting an initial treatment for acute severe PCH, participants were asked to subjectively forecast the analgesic effectiveness of their selection (Fig. 2). There was highest confidence for analgesia among metoclopramide users, with 69/99 (69.7%) anticipating effectiveness greater than 50%. Despite being the second-most selected abortive therapy, IV physiologic saline was anticipated by 52/73 (71.2%) users to have analgesic effectiveness below 50%.
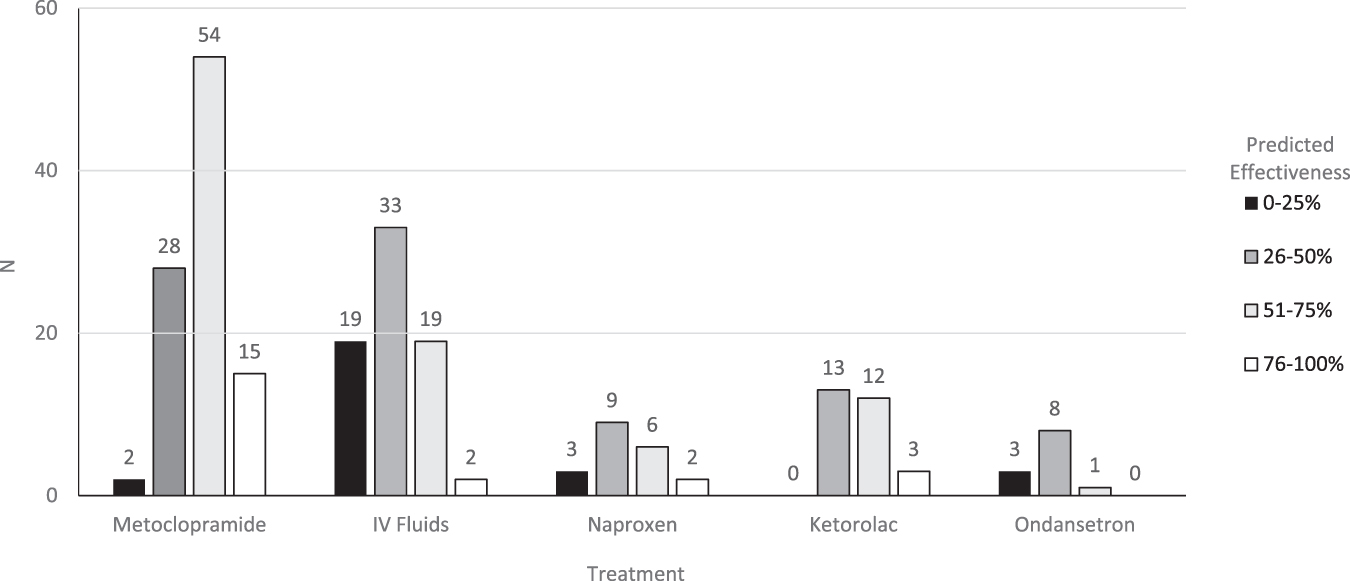
Physician-predicted analgesic effectiveness of treatment for acute severe post-concussion headache.
Metoclopramide was the single most frequently selected treatment, and IV metoclopramide was selected by respondents across all 15 pediatric EDs for management of both acute and persistent PCH. Individual participants were more likely to select metoclopramide for severe PCH pain 99/137 (72.3%) than for moderate PCH pain 41/137 (29.9%, p < 0.0001; Supplement S2). Also, for acute severe PCH, among participants selecting metoclopramide as part of their initial treatment strategy, 26.3% would use a repeat dose as second-line treatment for ongoing pain after 2 h.
To explore the potential drivers of reported practice patterns, logistic regression was used to test the strength of association of physician- and ED-level factors with the provision of treatment for acute severe PCH (Table 2). In univariable analyses, proportion of practice with pediatric patients was associated with the odds of any treatment (odds ratio [OR] = 0.73; 95% confidence interval [CI] 0.49–0.99); an association was no longer statistically significant in multi-variable regression after controlling for additional measured covariates (aOR = 0.65; 95% CI 0.27–1.55). No other measured covariates were associated with treatment. In addition, regression analyses did not reveal any significant associations between measured covariates and the odds of treatment with metoclopramide specifically. Participants also reported multiple factors that may influence their choice of abortive therapy for acute severe PCH (Table 3).
OR, odds ratio; CI, confidence interval; aOR, adjusted odds ratio; PCH, post-concussion headache.
Clinical decision tool in the form of a protocol, guideline, or clinical pathway.
Discussion
Children frequently require treatment in the ED for PCH that is refractory to common first-line analgesics. Results from this scenario-based survey of Canadian pediatric ED physicians demonstrate a lack of consensus among analgesic treatments for PCH. For severe PCH, more than 90% of physicians would provide abortive therapy for both acute and persistent pain; however, there was significant practice variation in terms of treatment selection. Overall, IV treatments, and IV metoclopramide specifically, were most frequently selected by ED physicians. Second-line treatment was even more variable. Moderate PCH pain was most frequently managed using oral NSAIDS. Physician- and ED-level factors did not predict treatment nor the use of metoclopramide.
Analgesia is a vital component of pediatric ED care 22 ; however, evidence to guide pharmacotherapy for PCH is critically lacking. 14,16,23,24 Consensus-based guidelines for pediatric concussion recommend analgesia for PCH with acetaminophen and NSAIDS as part of a multi-modal management plan. 9,13,23 In terms of high quality evidence to guide treatment choice, only two small randomized trials have studied pharmacological treatment for pediatric PCH, and these suggest that oral NSAIDS and IV hypertonic 3% saline may be effective acute abortive ED treatments. 25,26 NSAIDS are used frequently for PCH in the pediatric ED. 5,27
Importantly, though, there exists no evidence or recommendations for abortive therapies for PCH refractory to NSAIDS administered in the ED or outpatient setting. Our survey directly addresses this very common clinical scenario and highlights the need for well-designed prospective trials defining optimal analgesia tailored to pain severity and chronicity of symptoms. 28
The frequent selection of IV metoclopramide as first-line therapy may reflect the extension of common strategies for the management of primary headaches and migraines. When managing PCH, several authors recommend tailoring treatment to the primary headache phenotype. 8,29 –35 It has also been hypothesized that PCH may share pathophysiological features to migraines, 7,34,36 and migraine has been found to be the most common subtype of PCH. 8 This might explain the frequent use of metoclopramide in our study.
There are very few studies of metoclopramide for PCH, however. Chan and colleagues 37 conducted a retrospective study of 254 children aged 8–21 years presenting to the ED with post-traumatic headache and who received an IV medication. The mean time to presentation was 48 h, and treatment with metoclopramide (or prochlorperazine), ketorolac, or combination therapy was associated with 93%, 80%, and 89% success in decreasing headache pain score by half. 37 In a prospective open label study of IV metoclopramide and diphenhydramine, 38 20/21 adults treated for post-traumatic headache reported headache improvement acutely; however, 37% experienced symptom recurrence at 48 h, and 26% were symptomatic after one week. 38
In a large multi-center prospective study of pediatric PCH, metoclopramide was the most frequently used IV medication for pain management; however, abortive effectiveness was not assessed. 6 In a planned secondary analysis of this same cohort, metoclopramide use in the ED did not reduce persistent PCH at one and four weeks post-injury. 39 In summary, there may be a role for metoclopramide in the acute setting for pain control, but the available evidence is insufficient to inform treatment guidelines.
In the present study, opioids were selected by a minority of respondents. Management of PCH with opioids similarly has been reported among children presenting to EDs across the United States from 2007–2015. 5 Recent pediatric concussion guidelines from the US Centers for Disease Control and Prevention emphasize the importance of providing nonopioid analgesia for concussion pain, 23 and it remains to be seen whether opioid administration will decrease for children with PCH.
Of note, triptans were also infrequently selected among respondents. Reviews on the management of pediatric post-traumatic headache support a trial of triptans, 33,40 as do recent guidelines for pediatric migraine treatment. 41 Further study of triptans for PCH is required, and limited availability of this medication in the ED currently may contribute to its low usage. It is also possible that a preference for IV medications among respondents may have impacted the low use of triptans, which are only currently available in oral formulations.
Our results must be interpreted in light of several limitations. Foremost, we did not assess clinical outcomes directly. Physician self-reported treatments may not correlate perfectly with true clinical practice patterns, a limitation inherent to the survey study design. Nonetheless, data collected herein are important to inform future trials based on clinician practices and anecdotal experiences.
To identify leading candidate medications for prospective study, our survey instrument deliberately limited participant responses to just two treatments per scenario. This only allows for a characterization of monotherapy approaches and not medications or modalities in combination. We did not assess nonpharmacological treatments (e.g., physiotherapy, exercise, cognitive behavioral therapy) 2 that have been shown to also reduce concussion symptoms including headache, but which require longitudinal therapy and are not typically provided in the ED.
All participants were from Canadian tertiary pediatric EDs with the majority having completed a fellowship in Pediatric Emergency Medicine and practicing predominantly at pediatric institutions. As such, these results may not be generalizable to physicians whose previous training differs or who work in other clinical environments including nonpediatric EDs or outpatient clinics. Also, the survey scenario may not reflect a typical patient who might present to an outpatient clinic setting, where a majority of patients seek care after concussion.
A 2013 survey of pediatrician members of the American Academy of Pediatrics Sections on Adolescent Health, Sports Medicine and Fitness, Community Pediatrics and School Health, however, found a similar rate of self-reported medication use for concussed children in the outpatient setting (89%), most frequently using common medications such as acetaminophen and NSAIDS. 42 In multi-variable regression analyses, we found no physician- or ED-level factors associated with treatment; however, unmeasured covariates may influence reported treatment strategies.
Conclusion
There remains significant ongoing practice variation for analgesic treatment of acute and persistent pediatric PCH. Children presenting to an ED with severe PCH are most likely to receive IV medications, notably IV metoclopramide, despite a paucity of data demonstrating efficacy of these treatments. There is an urgent need for well-designed prospective trials to establish the comparative efficacy of these and other treatments for short- and long-term pain control outcomes. Treatment strategies reported here should inform future intervention trials for pediatric PCH to establish evidence-based recommendations.
Footnotes
Acknowledgments
The authors thank the Pediatric Emergency Research Canada network and Ms. Rebecca Emerton for their assistance with this research project.
Authors' Contributions
KL, BB, and ASD conceived the study, designed the survey instrument, and conducted statistical analysis on collected data. All authors reviewed the content of the questionnaire and provided feedback. KL drafted the manuscript, and all authors contributed to its revision. BB takes responsibility for the article as a whole.
Funding Information
No funding was associated with this project.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplement S1
Supplement S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.