
Abstract
Mild traumatic brain injury (mTBI) initiating long-term effects on white matter integrity resembles brain-aging changes, implying an aging process accelerated by mTBI. This longitudinal study aims to investigate the mTBI-induced acceleration of the brain-aging process by developing a neuroimaging model to predict brain age. The brain-age prediction model was defined using relevance vector regression based on fractional anisotropy from diffusion tensor imaging of 523 healthy individuals. The model was used to estimate the brain-predicted age difference (brain-PAD) between the chronological and estimated brain age in 116 acute mTBI patients and 63 healthy controls. Fifty patients were followed for 6 ∼ 12 months to evaluate the longitudinal changes in brain-PAD. We investigated whether brain-PAD was greater in patients of older age, post-concussion complaints, and apolipoprotein E (APOE) ɛ4 genotype, and whether it had the potential to predict neuropsychological outcomes. The brain-age prediction model predicted brain age accurately (r = 0.96). The brains of mTBI patients in the acute phase were estimated to be “older,” with greater brain-PAD (2.59 ± 5.97 years) than the healthy controls (0.12 ± 3.19 years) (p < 0.05), and remained stable 6–12 month post-injury (2.50 ± 4.54 years). Patients who were older or who had post-concussion complaints, rather than APOE ɛ4 genotype, had greater brain-PADs (p < 0.001, p = 0.024). Additionally, brain-PAD in the acute phase predicted information processing speed at the 6 ∼ 12 month follow-up (r = -0.36, p = 0.01). In conclusion, mTBI accelerates the brain-aging process, and brain-PAD may be capable of evaluating aging-associated issues post-injury, such as increased risks of neurodegeneration.
Introduction
Mild traumatic brain injury (mTBI), accounting for 80 ∼ 90% of all TBI, 1 is typically associated with white matter integrity loss that persists chronically after the initial injury. 2 The long-term sequelae of mTBI initiate risks for neurodegeneration and age-associated conditions, 3 making it a clinically important topic. A large-scale (n = 2,794,852) observational study with a 15-year follow-up showed that chronic mTBI was associated with a higher risk of dementia (hazard ratio: 1.17). 4 However, neuroimaging biomarkers that evaluate individual-based risks of age-associated or neurodegenerative deterioration in the brain for mTBI patients are still scarce.
MRI metrics strongly relate to chronological age, 5,6 making brain age predictable. The brain-predicted age difference (brain-PAD = predicted brain age - chronological age) reflects how far a brain deviates from the normal aging trajectory under a given disease. 7 –10 Increases in brain-PAD indicate that the brain-aging process accelerated and imply the risks of neurodegeneration and other age-related issues, 11 which have been widely revealed in psychiatric disorders and neurological diseases, 12 –15 including TBI. Recently, Cole and coworkers observed a 4.66-year increase in brain-PAD estimated by morphometrics in white matter and a 5.97-year increase estimated by gray matter morphometrics in chronic moderate/severe TBI patients compared with mild cases. 15 However, these results provide limited understanding of how mTBI accelerates the brain-aging process, because only 17 patients with mTBI were included in these authors' research. The majority of TBIs are within the mild range, and sustain insults from diffuse axonal injury. 16 They usually manifest as a brain-wide distribution of abnormalities on diffusion tensor imaging (DTI) metrics, such as fractional anisotropy (FA) value decreases. 17,18 Such deterioration in white matter integrity is thought to be responsible for further neurodegenerative and aging-related issues. 19 –21 Therefore, we hypothesized that mTBI might accelerate the aging process by decreased integrity in white matter microstructure.
Herein, relevance vector regression 22 was applied to build the brain-age prediction model based on DTI metrics to estimate brain age in mTBI patients and healthy controls (HC). The patients were followed into their chronic phase to evaluate the longitudinal changes in brain-PAD. We also investigated whether brain-PAD was prone to be greater in patients of older age, post-concussion complaints, and apolipoprotein E4 genotype, 3,23 –25 and whether it could predict neuropsychological outcomes. In addition, we hypothesized that white matter tracts contributing to brain-PAD in mTBI patients were primarily located in degenerative-vulnerable regions.
Methods
Participants
Training set
DTI scans from 523 anonymized healthy individuals were used to build the brain-age prediction model (details in Table S1). Exclusion criteria for DTI scans included poor quality leading to image processing failure. Ethical approval and informed consent were obtained from each original study.
Test sets
Ethics approval was obtained from the Second Affiliated Hospital of Wenzhou Medical University, and data collection was conducted between May 2016 and April 2018. The flow of participants through the study is shown in Figure 1. There were 116 acute mTBI patients with negative head computed tomography (CT) scans and Glasgow Coma Scale (GCS) scores of 15 recruited from the local emergency department. Sixty-four patients consented to participate in the follow-up investigations, and 50 of them were ultimately followed up 6 ∼ 12 month post-injury into their chronic phase. Screening for mTBI was based on the World Health Organization's Collaborating Centre for Neurotrauma Task Force 26 (details of inclusion and exclusion criteria listed in Table 1). The retrospective baseline health conditions of the patients were recorded at their first visit. HCs (n = 63) were recruited through advertisements and carefully screened for any neurological or psychiatric disorders. In addition, an independent cohort including 70 patients with acute mTBIs, with imaging from a different magnetic resonance imaging (MRI) scanner was included for replication use (details in Supplementary Methods). All subjects gave written, informed consent in person, and the study was approved by the local institutional review board and conducted in accordance with the Declaration of Helsinki.

Flow diagram shows the inclusion process for participants of test sets. brain-PAD, brain-predicted age difference; mTBI, mild traumatic brain injury; HCs, healthy controls; DTI, diffusion tensor imaging.
The Inclusion and Exclusion Criteria for mTBI
mTBI, mild traumatic brain injury; MRI, magnetic resonance imaging.
Clinical symptom and neuropsychological assessments
Clinical symptoms were assessed at the first patient visit (n = 116). The post-concussive symptoms (PCS) were evaluated by the International Classification of Diseases, 10th edition (ICD-10) clinical criteria. 27 Patients with three or more symptoms were classified as having PCS (PCS+) or not having (PCS-). According to the anterograde amnesia (AA) duration, patients were divided into those with AA (AA+) and those without AA (AA-).
The information processing speed (IPS) was assessed by the Digit Symbol Coding test 28 and the Trail-Making Test (Part A) 29 for HCs and patients at both the first and follow-up visits. The Z-score calculated from these two tests summarized IPS performance.
Apolipoprotein E (APOE) genotyping
Two milliliters of peripheral blood was collected from each of 81 mTBI patients for APOE genotype analysis. DNA was extracted from peripheral blood samples using Omega D3494-01 Blood DNA Midi Kit (Omega Bio-tek, Inc., United States). Two single-nucleotide polymorphisms (SNPs) (rs429358 and rs7412) were genotyped to identify APOE genotypes composed of the APOE-ɛ2, -ɛ3, and -ɛ4 alleles using Assay Design Suite v2.0 (Agena Bioscience, Inc., San Diego, CA). All genotypes containing the ɛ4 allele (ɛ4/ɛ4; ɛ4/ɛ3; ɛ4/ɛ2) were combined as the composite APOE ɛ4+, and others (ɛ2/ɛ2; ɛ2/ɛ3; ɛ3/ɛ3) were combined as the composite APOE ɛ4-.
Neuroimaging data acquisition and pre-processing
The training data sets were collected from multi-centers, by using different MRI scanners (Table S1). The intraclass correlation coefficient (ICC) as the homogeneity index for training data sets was calculated on FA after pre-processing, showing “excellent” homogeneity (ICC = 0.84) for multi-center data sets. 30,31
The DTI scans for test sets were acquired from a 3T MRI scanner (GE750) by a single-shot, spin echo-based and diffusion-weighted echo planar imaging sequence (repetition time [TR] = 8000 ms, echo time [TE] = 68 ms, flip angle = 90 degrees, thickness = 2 mm, slices = 75, field of view [FOV] = 256 mm × 256 mm, matrix size = 128 × 128, two averages, voxel size = 2 mm × 2 mm × 2 mm). DTI scans (b = 1000 sec/mm2) were acquired with 30 diffusion gradient directions, and diffusion imaging without weighting (b = 0) was repeated five times.
All raw DTI data were quality controlled and preprocessed using the FSL5.0.9 software package (
Brain-age prediction modeling procedure
The brain-age prediction was performed by defining a relevance vector regression (RVR) to model the relationship between FA values and chronological age in the training set, using Scikit-learn Python library. RVR derives from the Relevance Vector Machine based on Bayesian formulation, which extends linear regression models into probabilistic computation. Specifically, in the current study, the regression model for brain-age prediction was built by estimating the relevance vectors and their corresponding weight distributions through the type-II maximum likelihood algorithm. The relevance vectors were derived from the input data (i.e., FA values), which represented the prototypical examples associated with the regression target instead of solely separating attributes. The training process was visualized in Figure 2A–D (details in Supplementary Methods). The prediction accuracy was assessed using the Pearson correlation (r) between chronological age and predicted brain age, the proportion of the variation (R 2 ) was explained by the trained model, the mean absolute error (MAE), and root mean squared error (RMSE) of the brain-PAD scores.
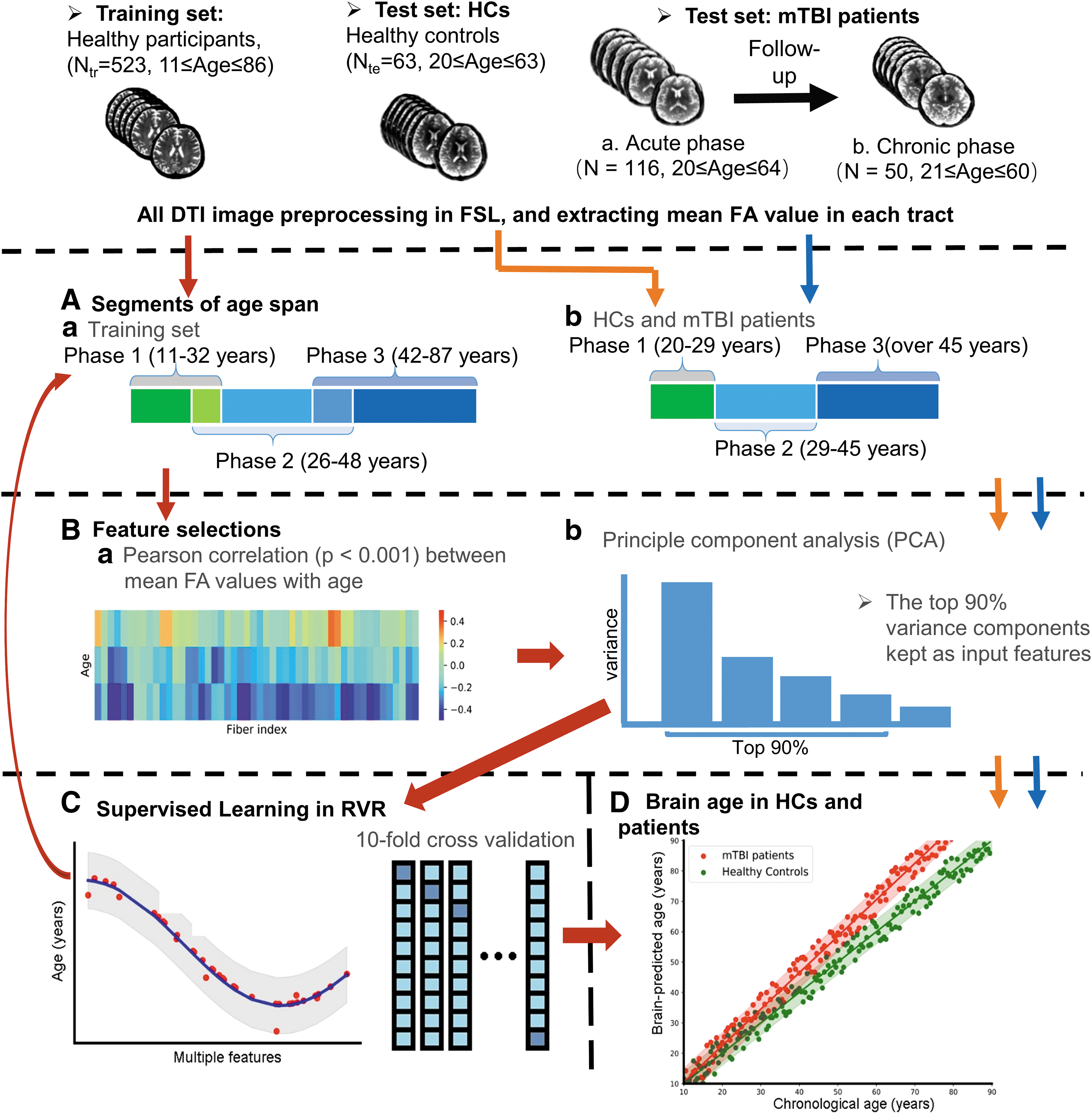
Overview of brain-age prediction model
Statistical analysis
All statistical analyses were conducted in SPSS (version 21.0; IBM, Armonk, NY). To examine the increased brain age in the test sets, we compared the brain-PAD scores with zero using the Wilcoxon Signed-rank test. Between-group comparisons in brain-PAD scores for mTBI samples versus HCs were conducted by analysis of covariance (ANCOVA), adjusting for sex, education, and age. Longitudinal comparison analysis was performed on brain-PAD between the acute and chronic phases with linear mixed-effects (LME) model analysis. Between-group comparisons in brain-PAD scores for mTBI PCS subgroups (PCS+ vs. PCS-), APOE genotypes (APOE ɛ4+ vs. APOE ɛ4-), AA subgroups (AA+ vs. AA-), and chronological age subgroups (youth: ≤30 years, middle-aged: 30 ∼ 50 years, elderly: ≥50 years) were also conducted by ANCOVA, adjusting for sex, education, and/or age. Spearman rank-order correlation (r) was conducted to examine the associations of brain-PAD scores with the post-injury time and Z-score for IPS performance. For the mTBI cohort, the r between brain-PAD and FA values of white matter tracts (WMTs) involved in model training was calculated to evaluate the related WMTs contributing to increased brain age. The results were considered significant at p < 0.05 (two-tailed). Effect sizes for ANCOVA and LME analysis were quantified using partial η 2 ; effect sizes for the Wilcoxon signed-rank test were quantified by the rank biserial correlation coefficient (rrb).
Results
Demographic and clinical characteristics of mTBI patients and HCs
Demographic and clinical information for the test sets is reported in Table 2. The mTBI cohort included 116 acute patients (58 males, 39.7 ± 11.9 years of age; education: 7.9 ± 3.9 years; first-visit post-injury: 3.5 ± 3.4 days; all presented as mean ± standard deviation [SD]). There were eight patients with a history of health issues (i.e., hyperglycemia, hypertension, and hyperlipidemia). Sixty-four patients consented to participate in the follow-up investigations and 50 of them (78.1%) were ultimately followed 6–12 months to their chronic phase (216.2 ± 117.8 days). Sixty-three HCs were enrolled (31 males, 36.7 ± 12.4 years of age; education: 10.9 ± 6.6 years). Patients showed worse performance on IPS tests than HCs (p < 0.001).
Demographic and Clinical Characteristics of mTBI Patients and Healthy Controls
P values were derived from with the χ 2 test or Mann–Whitney U test, as appropriate.
P value indicates a significant difference.
mTBI, mild traumatic brain injury; HCs, healthy controls; PCS +, with post-concussion symptom complaints; PCS -, without post-concussion symptom complaints; AA duration, anterograde amnesia duration; IPS, information processing speed; DSCT, Digit Symbol Coding Test; TMT_A = Trail-Making Test Part A
Chronological age predicted by FA values
The RVR model could accurately predict individual chronological age for both the training set and the HC test set. For the training set, age was accurately predicted by FA values (r = 0.96, R 2 = 0.93, MAE = 3.74, RMSE = 5.03). The mean PAD for the training group was -0.18 (± 5.03) years. For the HC test set, brain age was also accurately predicted (r = 0.97, R 2 = 0.94, MAE = 2.57, RMSE = 3.16), and the mean PAD was 0.12 (± 3.19) years.
mTBI accelerated brain-aging process
The predicted brain age significantly correlated with chronological age in both HCs (R 2 = 0.93, p < 0.001) and mTBIs (R 2 = 0.87, p < 0.001) (Fig. 3A). mTBI patients had predicted brain age older than their chronological age in the acute phase (PAD = 2.59 ± 5.97 years; W = 4854, p < 0.001, rrb = 0.431), which was replicated in an independent mTBI cohort (PAD = 3.26 ± 4.55 years; W = 2158, P < 0.001, rrb = 0.737). Acute mTBI patients had higher brain-PAD scores (2.59 ± 5.97 years) than HCs (0.12 ± 3.19 years) (F 1, 173 = 7.23, p = 0.008, partial η 2 = 0.041; Fig. 3B). Additional analyses showed that the educational level and baseline health conditions of patients had no confounding effects on brain-PAD in the acute phase (Details in Supplementary Results).

Mild traumatic brain injury (mTBI) increased the brain-aging process.
mTBI patients had relatively stable brain-PADs (2.50 ± 4.54 years) in their chronic phase. Their brain-PAD scores (2.50 ± 4.54 years) in the chronic phase were also higher than those for HCs (0.12 ± 3.19 years) (F 1,108 = 8.16, p = 0.005, partial η 2 = 0.07). Longitudinal comparison of brain-PADs between the two phases showed no statistical differences (F 1, 112 = 0.436, p = 0.51; Fig. 3C). In addition, brain-PAD scores were not associated with post-injury days in either the acute or chronic phase (acute phase: r = -0.045, p = 0.634; chronic phase: r = -0.015, p = 0.920). Moreover, brain-PADs derived from the acute phase were inversely related to IPS performance in both the acute phase (r = -0.294, p = 0.001; Fig. 4A) and the 6–12 month follow-up (r = -0.356, p = 0.011; Fig. 4B).

Predicted age difference (PAD) in the acute phase predicted neuropsychological outcomes.
Neurodegeneration-vulnerable tracts associated with brain-PAD scores
The r between brain-PAD and FA values of WMTs involved in model training (n = 33) was calculated to evaluate the related WMT contribution to increased brain age. The FA value in 16 WMTs was significantly correlated with the brain-PAD scores in the acute phase. They were mainly located in the commissural, association, and projection fibers (r: -0.305 ∼ -0.473, p < 0.05 after familywise error (FWE) correction for multiple comparisons) (Table 3), primarily including the corpus callosum, fornix, corona radiate, and superior longitudinal fasciculus. In the chronic phase, the FA value in the body of the fornix was still significantly related to the brain-PAD at 6 ∼ 12 month follow-up, after FWE correction for multiple comparisons (r = -0.434, p < 0.05) (Table 3).
Correlation between FA value of Age-Sensitive WMTs and Brain-PAD in Acute and Chronic Phases
Statistical significance after familywise error (FWE) correction for multiple comparisons (p < 0.05).
WMT, white matter tract; brain-PAD, brain-predicted age difference.
Factors affecting brain-PAD scores
The patients' chronological age at mTBI affected their PAD derived from the acute phase (F 2, 111 = 10.05, p < 0.001, partial η 2 = 0.15), after adjusting for sex and education (Table 4). The brain-PAD scores in the elderly patients (n = 27, 6.74 ± 5.61 years) were higher than those in the middle-aged (n = 57, 1.98 ± 5.44 years) and young patients (n = 32, 0.18 ± 5.66 years) (multiple comparisons for Bonferroni correction, p < 0.05) (Fig. 5A).

Individual differences in predicted age difference (PAD).
Individual Differences in Brain-PAD Scores Post-Injury
Statistical significance after multiple comparisons for Bonferroni correction (p < 0.05).
PCS, post-concussion symptoms; PCS +, with PCS complaints; PCS -, without PCS complaints; AA, anterograde amnesia; AA +, with AA; AA -, without AA; APOE, apolipoprotein E; ɛ4+, APOE ɛ4 carriers; ɛ4- , APOE non-ɛ4 carriers
The PCS severity post-injury also affected the PAD in the acute phase (F 1, 111 = 5.26, p = 0.02, partial η 2 = 0.05), after adjusting for sex, education, and age. Patients with PCS complaints (i.e., PCS+) had higher brain-PAD scores (n = 91, 3.21 ± 5.44 years) than the PCS- group (n = 25, 0.34 ± 5.50 years) (Fig. 5B) (Table 4).
The AA and APOE genotypes did not affect PAD in the acute phase (AA: F 1,111 = 0.86, p = 0.35; APOE: F 1, 111 = 0.46, P = 0.49), after adjusting for sex, education, and age (Table 4).
Discussion
Our study revealed that mTBI triggered an accelerated aging process in the brain, deviating from its chronological trajectory. Increased brain age was observed in the early acute phase and remained stable within a 6 ∼ 12 month follow-up. The WMTs relevant to the accelerated-aging process were primarily located in the connecting aging-related and neurodegeneration-vulnerable regions. Also, the brain-PAD of patients measured in the acute phase could predict the individual performance of IPS at the 6 ∼ 12 month follow-up. Patients with older chronological age and more severe PCS complaints were more vulnerable to having “older” brain age.
Unlike one recent study about increased brain-PAD observed in chronic patients, 33 the observations in our research took place during a relatively early phase of mTBI. The results showed that the discrepancy between predicted brain age and chronological age (i.e., brain-PAD >2 years) was detectable even at the acute phase post-injury. Moreover, the increased brain age cannot simply be explained as a transient physiological pattern in response to traumatic events. Instead, the current longitudinal observation of brain-PAD further demonstrated that such an accelerated brain-aging process was a stable change. As described in neurological and neuropsychiatric studies, increases in brain age have been considered to be a surrogate neurobiomarker of vulnerability to neurodegeneration. 7,34 Likewise, the brain-PAD score may be a candidate biomarker for mTBI. No significant correlations between the brain-PAD score and time since injury in either the acute or chronic phase were observed, which further supplemented the explanation that such increases in brain age might reflect vulnerability to an accelerated aging process.
For both the acute phase and the follow-up, the increases in brain age were inversely related to the integrity of the fornix, implying that the persistent brain-aging process accelerated by mTBI might be caused by the deteriorated integrity of the fornix. The fornix, connecting the hippocampal formation in the limbic system, is responsible for neurodegeneration progression. 35 Its integrity alterations were observed in mild cognitive impairment and chronological aging processes. 36,37 Moreover, a recent theory about the Alzheimer's disease (AD) pathway suggests that transmission initiates in the hippocampus regions, spreading latterly to the rest of the brain, 38,39 implying that the fornix may serve as a common origin of neurodegeneration in the transmission pathway. Therefore, based on the current findings on the steady association between the integrity of the fornix and increased brain age, we can infer that the brain-PAD score derived from WMT integrity was informative in evaluating the potential neurodegeneration effects.
We explored factors affecting brain-PAD in patients with mTBI, which could explain the individual differences in the acceleration of brain-aging post-injury. A relative higher variance of PAD was presented in the present study as well as the previous studies 8,10,15 (e.g., PAD of HCs: 0.07 ± 7.41 years; PAD of TBIs: 4.66 ± 10.8 years in Cole and coworkers 15 ), which may be the result of individual differences affecting the PAD. The present results showed that patients with older chronological age and more severe PCS complaints were more vulnerable to developing greater brain-PAD. These results, on the one hand, were consistent with some retrospective studies' findings that post-concussion syndrome and older age increased the risks of developing dementia for patients with mTBI. 3,23 On the other hand, these results revealed the possibility that age at exposure to TBI and PCS severity may explain such high variance of PAD. Therefore, PAD may potentially be used as an index to reflect the individual differences of outcome in mTBIs. In our study, the APOE genotypes and AA showed non-significant effects on brain-PAD following mTBI. Both APOE ɛ4 and AA are generally considered to be risk factors for AD. 24,25 Those results provide some indications that the neurodegeneration-vulnerable aging process accelerated by mTBI may be different from AD pathology. 40 However, there still need to be further studies to explore the common and dissociated factors contributing to neurodegeneration in mTBI and AD.
Our model explained the variations in the chronological aging process as aging-related changes in WMTs. Unlike previous studies using macroscopic morphometrics to predict brain age in moderate to severe TBI patients, 15,33 we adopted subtler microstructural features, considering that mTBI usually causes diffuse axonal injury 16 and long-distance white matter disconnections. 19 This damage, thereafter, results in degradation in communication efficiency among brain regions, and contributes to cognitive dysfunctions during the brain-aging process, commonly reflected as a slow speed of information processing and transferring. 41 Moreover, our results demonstrated that the brain-PAD of the acute phase could predict the individual profiles of IPS in the chronic phase. A greater brain-PAD was relevant to poorer IPS performance, suggesting that white matter integrity loss underlying the accelerated aging process contributed to the cognitive impairments following mTBI.
There are limitations to the present study. First, our brain-age prediction model was trained with DTI metrics with respect to injury characteristics of mTBI. The brain-aging process is biologically complex, which may be explained further by the multi-modality of neuroimaging. Second, the follow-up loss and insufficient APOE ɛ4 samples limited our understandings of the association between the accelerated brain-aging process following mTBI and neurodegenerative diseases. Third, the increased brain-PAD in our study only provided the evidence in neuroimaging to support the potentially accelerated brain aging post-injury. The accelerated brain aging may also involve a series of complex processes, such as Wallerian degeneration of white matter, 42 deposition of amyloid-β proteins in the brain, 43 and increases in neurofilament light chain caused by diffuse axonal injury. 44
Conclusion
In summary, acceleration of the brain-aging process underlying deterioration in WMTs is detectable even in the acute phase of mTBI, and persists into the chronic phase, which provides insights into the risks of mTBI for neurodegeneration-vulnerable conditions. Moreover, the increases in brain age are related to clinical characteristics and are capable of predicting neuropsychological outcomes.
Footnotes
Acknowledgments
We thank all patients and healthy volunteers who participated in the study. We also acknowledge the data sharing from IXI (
Funding Information
This study was funded by the National Natural Science Foundation of China (Grant Nos. 82071993, 81771914, 81871331, 61971451, 81671671), Key projects in Hunan Province (Grant Nos. 2020SK4001, 2019SK-2131), Natural Science Foundation of Zhejiang Province (Nos. LY19H180003), Wenzhou Science and Technology Bureau in China (No. Y20180112), Fundamental Research Funds for the Central Universities (Grant Nos. Xjj2018229, xzy022019045).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Text (includes Methods and Results)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.