
Abstract
Some patients after mild traumatic brain injury (mTBI) experience microstructural damages in the long-distance white matter (WM) connections, which disrupts the functional connectome of large-scale brain networks that support cognitive function. Patterns of WM structural damage following mTBI were well documented using diffusion tensor imaging (DTI). However, the functional organization of WM and its association with gray matter functional networks (GM-FNs) and its DTI metrics remain unknown. The present study adopted resting-state functional magnetic resonance imaging to explore WM functional properties in mTBI patients (108 acute patients, 48 chronic patients, 46 healthy controls [HCs]). Eleven large-scale WM functional networks (WM-FNs) were constructed by the k-means clustering algorithm of voxel-wise WM functional connectivity (FC). Compared with HCs, acute mTBI patients observed enhanced FC between inferior fronto-occipital fasciculus (IFOF) WM-FN and primary sensorimotor WM-FNs, and cortical primary sensorimotor GM-FNs. Further, acute mTBI patients showed increased DTI metrics (mean diffusivity, axial diffusivity, and radial diffusivity) in deep WM-FNs and higher-order cognitive WM-FNs. Moreover, mTBI patients demonstrated full recovery of FC and partial recovery of DTI metrics in the chronic stage. Additionally, enhanced FC between IFOF WM-FN and anterior cerebellar GM-FN was correlated with impaired information processing speed. Our findings provide novel evidence for functional and structural alteration of WM-FNs in mTBI patients. Importantly, the convergent damage of the IFOF network might imply its crucial role in our understanding of the pathophysiology mechanism of mTBI patients.
Introduction
Traumatic brain injury (TBI) is a public health challenge of vast proportions but is insufficiently recognized. More than 50 million people have a TBI worldwide each year, and it is estimated that about half of the world's population will suffer one or more TBIs in their lifetime. 1,2 Mild TBI (mTBI) accounts for 80% ∼ 90% of all TBI cases in both civilian and military populations. 3
Increasing evidence suggests that insufficient structural and functional communication of large-scale functional networks underlies cognitive impairments after mTBI. 4 -6 It has been speculated that microstructural damage of white matter (WM) fiber tract elicits large-scale functional networks disconnection mainly through the WM tracts' vulnerability for deformation. 7 Previous study of mTBI showed decreased fractional anisotropy (FA) and increased mean diffusivity (MD) in the internal capsule, corpus callosum, anterior corona radiata, anterior thalamic radiation, external capsule, and cingulum after mTBI. 8 Significantly, the long WM tracts connections are particularly vulnerable to the mechanical trauma 7 and thus disrupt the functional communication of large-scale networks that support cognition. 9 For instance, the inferior fronto-occipital fasciculus (IFOF), which mediates feed-forward propagation of visual input to anterior frontal regions, 10 was documented to have reduced WM integrity in mTBI patients. 11 Although previous studies sufficiently revealed the alterations in WM tracts in mTBI patients using diffusion tensor imaging (DTI), functional organization of WM and its association with gray matter functional networks (GM-FNs) across whole brain remains unknown.
Recently, increasing studies have evidenced the possible existence of functional information in WM, which also can be detected by resting-state functional magnetic resonance imaging (rs-fMRI). 12 -14 For instance, Ding and colleagues uncovered that resting-state blood oxygen level–dependent signals in WM reflect neural coding and information processing. 12 Several studies further indicated that the WM would be activated in direct response to multiple tasks, like perceptual and motor tasks. 15 -17 In addition, the large-scale functional organization of WM has been built in healthy population. 18,19 Further, recent studies sufficiently revealed that the functional connectivity (FC) in WM is related to the underlying pathophysiological mechanism of neuropsychiatric disorders, like Parkinson's disease, 20 schizophrenia, 21 and epilepsy. 22 Collectively, all previous studies have suggested the possible involvement of functional network of WM in cognitive and disorder progression. Therefore, the present study constructed the WM functional networks (WM-FNs) of mTBI patients, and further investigated the functional properties and DTI metrics of WM-FNs to deepen our understanding of the pathological mechanism in mTBI patients.
The present study aims to: 1) construct large-scale WM-FNs by k-means clustering analysis on rs-fMRI data of a large cohort of 108 acute mTBI patients (of which 48 patients followed-up at 6 months to 1 year, which were considered as chronic stage patients) and 46 healthy controls (HCs); 2) investigate the FC within the resulting large-scale WM-FNs and its interaction with the known GM-FNs in both acute and chronic mTBI patients; 3) evaluate the DTI metrics of WM-FNs in both acute and chronic mTBI patients; and 4) measure the correlations between altered imaging with cognitive and neuropsychological symptoms assessments of mTBI patients.
Methods
Participants
One hundred and eight consecutive patients suffering from head trauma were recruited from the local emergency department between August 2016 and May 2018 as the initial population. The inclusion and exclusion criteria of mTBI were based on the World Health Organization's Collaboration Center for Neurotrauma Task Force. 23 The detailed inclusion and exclusion criteria of mTBI patients are described in the Supplementary Material. Forty-eight of mTBI patients in the acute stage were followed up for 6 months to 1 year, with repeat MRI and cognitive and neurobehavioral symptoms assessments.
Forty-six age-, gender-, and education-matched HCs were recruited by advertisement. Screening was performed based on the physical examination by licensed medical staff and self-reported medical history. In detail, the HCs were screened with following criteria: 1) without neurological impairment or psychiatric disorders based on history and physical examination by licensed medical staff; 2) no history of alcohol or substance abuse; 3) no history of head injury, regardless of cause; and 4) 18 years of age or older.
MRI scans of patients with mTBI were initially assessed in acute stage (within 7 days post-injury) and followed up at chronic stage (6 months to 1 year post-injury). The cognitive and neurobehavioral symptoms assessments (see below) were carried out within 48 h of MRI scans. All HCs participants also underwent an identical MRI scanning and cognitive and neurobehavioral symptoms assessments.
Written informed consent was obtained from each individual before the experimental procedures. The research procedures have been approved by the Ethical Committee of The School of Life Science and Technology in Xi'an Jiaotong University and conducted in line with the Declaration of Helsinki.
Image acquisition
A non-contrast computed tomography (CT) scan was performed on all consecutive patients following acute head injury with a 64-row CT scanner (GE, Lightspeed VCT). All participants underwent MRI scanning in a 3.0 T MRI scanner (GE 750) with a 32-channel head coil. Resting-state fMRI data was acquired using a gradient-recalled echo planar imaging sequence with a total 180 volumes of 54 slices covering the whole brain, and the scan parameters were as follows: repetition time (TR) = 2500 msec; echo time (TE) = 30 msec; slice thickness = 3 mm; flip angle = 90°; field of view (FOV) = 216 mm × 216 mm; matrix size = 64 × 64; voxel size = 3 mm × 3 mm × 3 mm; acquisition time = 7:30 min. The scan parameters of High-resolution T1-weighted three-dimensional Magnetization Prepared Rapid Gradient Echo (MPRAGE) sequence were as follows: TR = 8.15 msec; TE = 3.17 msec; slice thickness = 1 mm; flip angle = 9°; FOV = 256 mm × 256 mm; matrix size = 256 × 256; acquisition time = 4:30 min. The scan parameters of diffusion-weighted imaging represent as follows: TR = 7300 msec; TE = 99 msec; slice thickness = 3 mm; flip angle = 90°; slices = 50; FOV = 256 mm × 256 mm; matrix size = 128 × 128; two averages; voxel size = 2 mm × 2 mm × 3 mm. DTI scan (b = 1000 sec/mm2) were acquired with 30 diffusion gradient orientations and the b = 0 repeated two times (acquisition time = 9:28 min). During scanning, all participants were instructed to relax, close their eyes, keep awake, and try not to think of anything in particular.
Cognitive and neurobehavioral symptoms assessments
Cognitive assessments included: 1) Trail-Making Test Part A (TMT-A) and Wechsler Adult Intelligence Scale (WAIS)-III Digital Symbol Coding score (DSC), which were used to evaluate cognitive information processing speed 24 ; 2) WAIS-III Forward Digit Span (DS) and Backward DS, which were used to measure working memory 25 ; and 3) Verbal Fluency (VF) Test, which was used to examine language ability, semantic memory, and executive function. 26 Neurobehavioral symptoms assessments included:1) post-concussive symptoms evaluated based on Rivermead Post-Concussion Symptom Questionnaire (RPCS) 27 ; 2) the Insomnia Severity Index (ISI) 28 ; and 3) the Post-traumatic Stress Disorder (PTSD) Checklist-Civilian Version (PCL-C). 29
Data pre-processing
Pre-processing steps of rs-fMRI and T1 data were carried out using DPABI 30 and Statistical Parametric Mapping. Figure 1 demonstrated the pre-processing steps. Of note, spatial smoothed of WM and gray matter (GM) signals separately within individual WM mask or GM mask to avoid the mixture of WM and GM signals. Detailed pre-processing steps were described in the Supplementary Material.
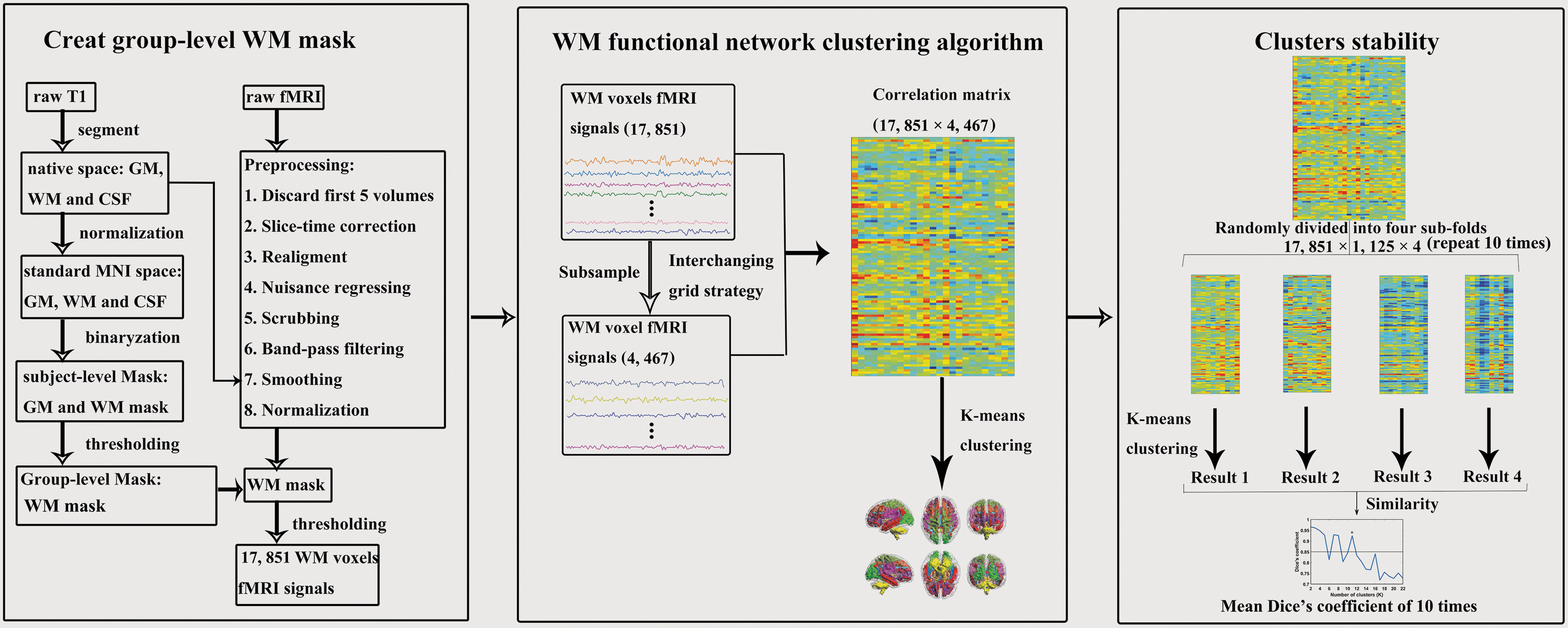
Method overview of white matter functional networks clustering analysis. WM, white matter; GM, gray matter; CSF, cerebrospinal fluid; MNI, Montreal Neurological Institute; fMRI, resting-state functional magnetic resonance imaging. Color image is available online.
Pre-processing of DTI data was performed using FMRIB Software Library (FSL) software. 31 Detailed pre-processing steps were described in the Supplementary Material.
Clustering WM-FNs
The processed resting-state data of mTBI patients in the acute stage and HCs subjects were used to cluster WM-FNs. The steps of WM-FNs clustering analysis were shown in Figure 1. The pipeline of clustering WM-FNs was similar to a previous study 19 and is briefly described here. To begin with, the segmentation results about the T1 image were used to generate the group WM mask. Voxel with a percentage greater than 60% of subjects was identified as a group-level WM mask. The subcortical areas (according to the Harvard-Oxford Atlas) 32 were excluded from the WM mask. Besides, voxels that were identified as WM but without functional data in more than 20% of the subjects were also excluded. Next, WM-FNs were identified by the K-means clustering algorithm (distance metric-correlation, 10 replicates) based on the averaged group-level Pearson's correlation matrix between WM voxels that group masks restricted. The numbers of clusters ranging from 2 to 22. Finally, averaged Dice's coefficient (the threshold was set at 0.85) was used to identify the most reliable number of WM-FNs. The detailed steps were described in Supplementary Material.
The WM-FNs atlas at the acute stage was equally used to analyze the pathological changes of WM-FNs in the chronic stage. To avoid the alteration of the results by the functional reconstruction of WM-FNs in the chronic stage, the WM-FNs clustering of the chronic stage were added (see Supplementary Material). To further investigate the similarity between the identified WM-FNs and the known WM structures, we compared the WM-FNs to structural WM tracts identified using DTI data (see Supplementary Material).
Functional connectivity
To evaluate the interaction within the resulting WM-FNs, the average signal time-courses from WM-FNs were extracted by averaging the signal values across all voxels which were belonged to each network. The Pearson's correlation between any two WM-FNs' time-courses for each individual was computed. Besides, to evaluate the interaction between the WM-FNs and GM-FNs, the GM-FNs atlas that was generated by the same clustering procedure 33 was used, and Pearson's correlation between the WM-FNs and GM-FNs was also computed. These correlation coefficients were averaged across subjects to obtain a group level matrix representing the relationship between WM and GM-FN. Of note, the Pearson's correlation coefficients were transformed into the Fisher z score before statistical analysis.
DTI metrics of WM-FNs
To determine whether WM abnormalities could be revealed by DTI, we extracted mean FA, MD, axial diffusivity (AD), and radial diffusivity (RD) in each of the WM-FNs.
Statistical analysis
The normality distribution of all cognitive and neurobehavioral symptoms continuous variables was tested by the Shapiro-Wilk W test. The group differences about cognitive and neurobehavioral symptoms continuous variables were calculated by the independent two-sample t-test and Mann-Whitney test based on data normality, respectively. Chi-squared was used to compare categorical variables, with significance set at p < 0.05.
An independent two-sample t-test was used to show the differences between the mTBI and HCs about the z-score of FC (Pearson's correlation coefficient), with a significance set at p < 0.05 (false discovery rate [FDR] corrected).
In addition, Mann-Whitney test was performed to show the differences between the mTBI and HCs about DTI metrics, with a significance set at p < 0.05 (FDR corrected).
Correlation between altered WM-FNs and cognitive and neurobehavioral symptoms assessments
To evaluate the relationship between altered imaging results and cognitive and neurobehavioral symptoms assessments, we calculated the Spearman correlation between altered FC or DTI metrics with cognitive and neurobehavioral symptoms variables since the cognitive and neurobehavioral symptoms variables were not normally distributed.
Results
Demographic, cognitive, and neurobehavioral symptoms characteristics
Sixteen patients with mTBI in the acute stage and four HCs with head motion scans exceeding 2 mm and/or 2° rotation were excluded. The final analysis included 92 mTBI patients in the acute stage, 48 mTBI patients in the chronic stage, and 42 HCs. The mTBI patients did not differ from HCs with regard to age, education, gender, and mean framewise displacement (Table 1). The cognitive and neurobehavioral symptoms assessments of all participants are shown in Table 1.
p1 represents the p values from statistical test between mTBI in acute stage and HCs.
p2 represents the p values from statistical test between mTBI in chronic stage and HCs.
Continuous variables are expressed as mean±standard deviation (range) and categorical variables are expressed as frequency.
mTBI, mild traumatic brain injury; HCs, healthy controls; M, male; F, female; FD, framewise displacement; TMT-A, trail making test A; DSC, digit symbol coding; DS, digit span; VF, verbal fluency; RPCS, Rivermead Post-Concussion Symptom questionnaire; ISI, insomnia severity index; PCL-C, Posttraumatic Stress Disorder Checklist-Civilian Version.
WM-FNs
The coefficient of Dice was adopted to evaluate the stability of WM-FNs number. The results demonstrated the most stable with the largest number of WM-FNs was 11 (Fig. 2). The WM-FN is given a putative network name based on the anatomical location (Table 2). In addition, based on the spatial distribution, we defined middle/superficial WM-FNs (WM-FN 2, 3, 45, 7, 8, 9, 10, 11) and deep WM-FNs (WM-FN 1, 6; Fig. 2; Table 2). Besides, the spatial similarity between WM-FNs and DTI fiber tracts were offered in Supplementary Material (Fig. S1).

White matter functional networks. 1. Inferior fronto-occipital fasciculus network; 2. Corona radiate network; 3. Anterior temporal network; 4. Orbitofrontal network; 5. Pre/postcentral network; 6. Superior longitudinal fasciculus network; 7. Ventral frontal network; 8. Temporoparietal network; 9. Rolandic network; 10. Cerebellar network; 11. Occipital network. WM, white matter. Color image is available online.
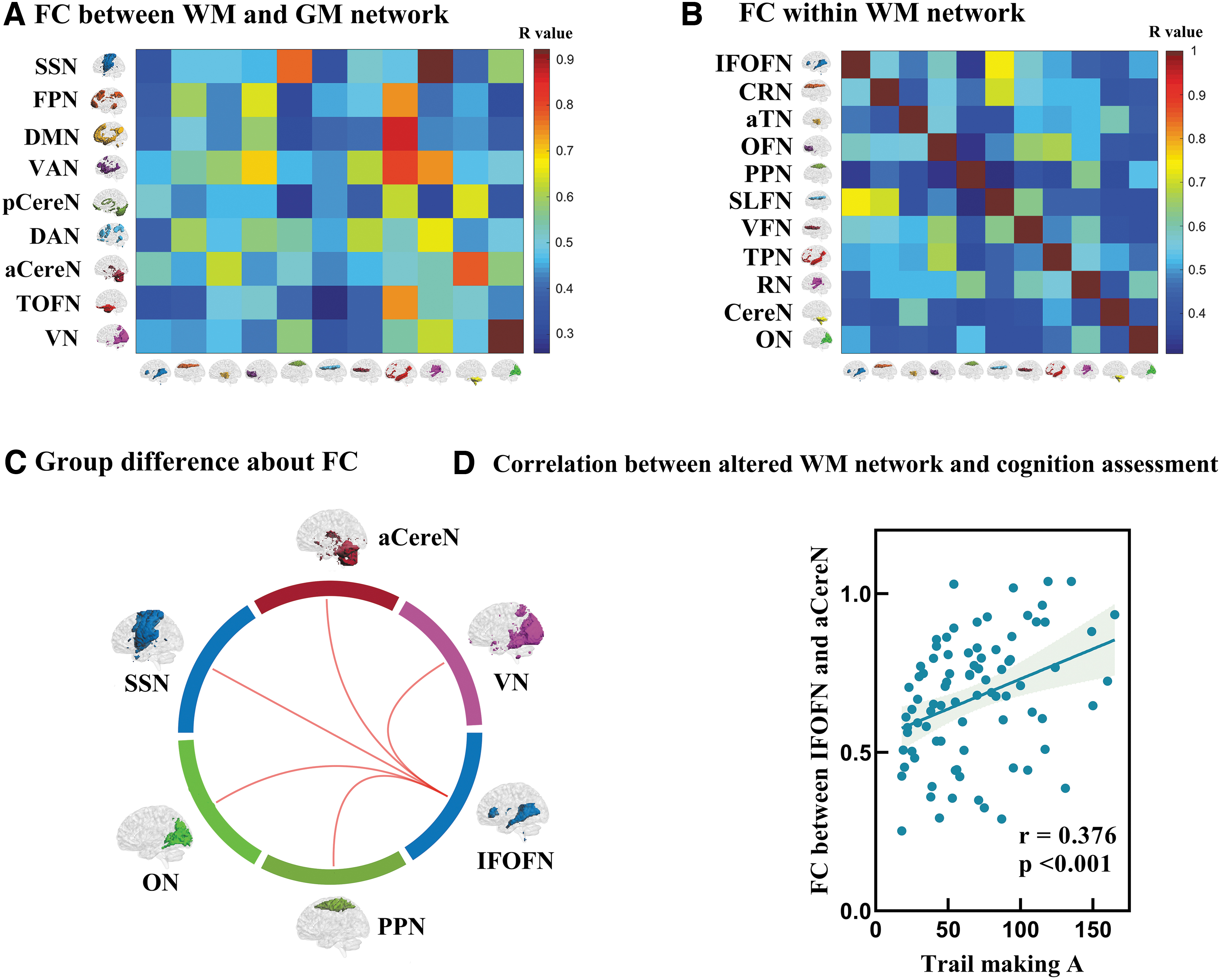
WM-FNs, white matter functional networks; GM-FNs, gray matter functional networks; IFOF, inferior fronto-occipital fasciculus; SLF, superior longitudinal fasciculus; SSN, sensorimotor network; DMN, default mode network; VAN, ventral attention network; FPN, frontoparietal network; TOFN, temporal-orbitofrontal network; aCereN, anterior cerebellar network; VN, visual network.
Functional connectivity
Functional connectivity in the acute stage
Across subjects, middle/superficial WM-FNs demonstrated strong correlation in their spontaneous activity with their adjacent GM-FNs and some distributed GM-FNs, such as occipital network and visual network (r = 0.92), rolandic network and sensorimotor network (r = 0.92), temporoparietal network and default mode network (r = 0.86; Fig. 3A; Table 2). Further, a relatively weak correlation (r < 0.55) was revealed between the deep WM-FNs and GM-FNs (Fig. 3A).
Functional connectivity (FC) of white matter functional networks (WM-FNs) in the acute stage mild traumatic brain injury (mTBI) patients and healthy controls (HCs).
Across subjects, between adjacent WM-FNs, such as the superior longitudinal fasciculus network and IFOF network, observed a strong correlation (r = 0.74; Fig. 3B; Table 2). Between distant WM-FNs, such as cerebellar WM-FN and the other WM-FNs, revealed relatively weak correlation (r < 0.60; Fig. 3B).
Compared with HCs, patients with mTBI showed increased FC between the deep WM-FN and low-level primary sensorimotor cortical GM-FNs. In detail, mTBI patients showed increased FC between IFOF WM-FN and visual GM-FN, IFOF WM-FN and anterior cerebellar GM-FN, IFOF WM-FN and sensorimotor GM-FN (Fig. 3C; Table 3).
mTBI, mild traumatic brain injury; HCs, healthy controls; FC, functional connectivity; WM-FNs, white matter functional networks; GM-FNs, gray matter functional networks; WM-FN, white matter functional network; GM-FN, gray matter functional network.
Compared with HCs, patients with mTBI also showed increased FC between deep WM-FN and low-level primary sensorimotor superficial WM-FN. In detail, patients with mTBI showed increased FC between IFOF WM-FN and occipital WM-FN, IFOF WM-FN and pre/postcentral WM-FN (Fig. 3C; Table 3). Taken together, the IFOF WM-FN is the most affected WM-FN, which showed increased connectivity with low-level primary sensorimotor functional networks in acute mTBI patients.
Functional connectivity in the chronic stage
Similar to the acute stage, the interaction between WM-FNs and GM-FNs in the chronic stage demonstrated a relatively strong correlation between middle/superficial WM-FNs and adjacent GM-FNs, and a relatively weak correlation was revealed between the deep WM-FNs and GM-FNs (Fig. 4A). The interaction between pair of WM-FNs in the chronic stage was also similar to the acute stage with a strong correlation between adjacent WM-FNs, and a relatively weak correlation was presented between distant WM-FNs (Fig. 4B). The mTBI patients did not differ from HCs regarding FC between WM and GM-FNs (Fig. 4C) and did not differ regarding FC within WM-FNs (Fig. 4D). Moreover, even the WM-FNs were constructed by the patients in chronic stage and HCs, and the results remained stable (see Supplementary Material, Fig. S2 and Fig. S3).

Functional connectivity (FC) of white matter functional networks (WM-FNs) in the chronic stage mild traumatic brain injury (mTBI) patients and healthy controls (HCs).
DTI metrics of WM-FNs
DTI metrics in the acute stage
Compared with HCs, acute stage mTBI patients showed significantly increased MD, RD, and AD in deep WM-FNs and higher-order cognitive WM-FNs, and no significant changes in FA were observed. In detail, mTBI patients showed increased MD in orbitofrontal network, temporoparietal network and ventral fontal network. (Fig. 5A; Table 4). In addition, mTBI patients showed increased RD in orbitofrontal network and temporoparietal network (Fig. 5B; Table 4). Besides, mTBI patients showed increased AD in IFOF network, ventral frontal network, temporoparietal network, orbitofrontal network, and superior longitudinal fasciculus network (Fig. 5C; Table 4).
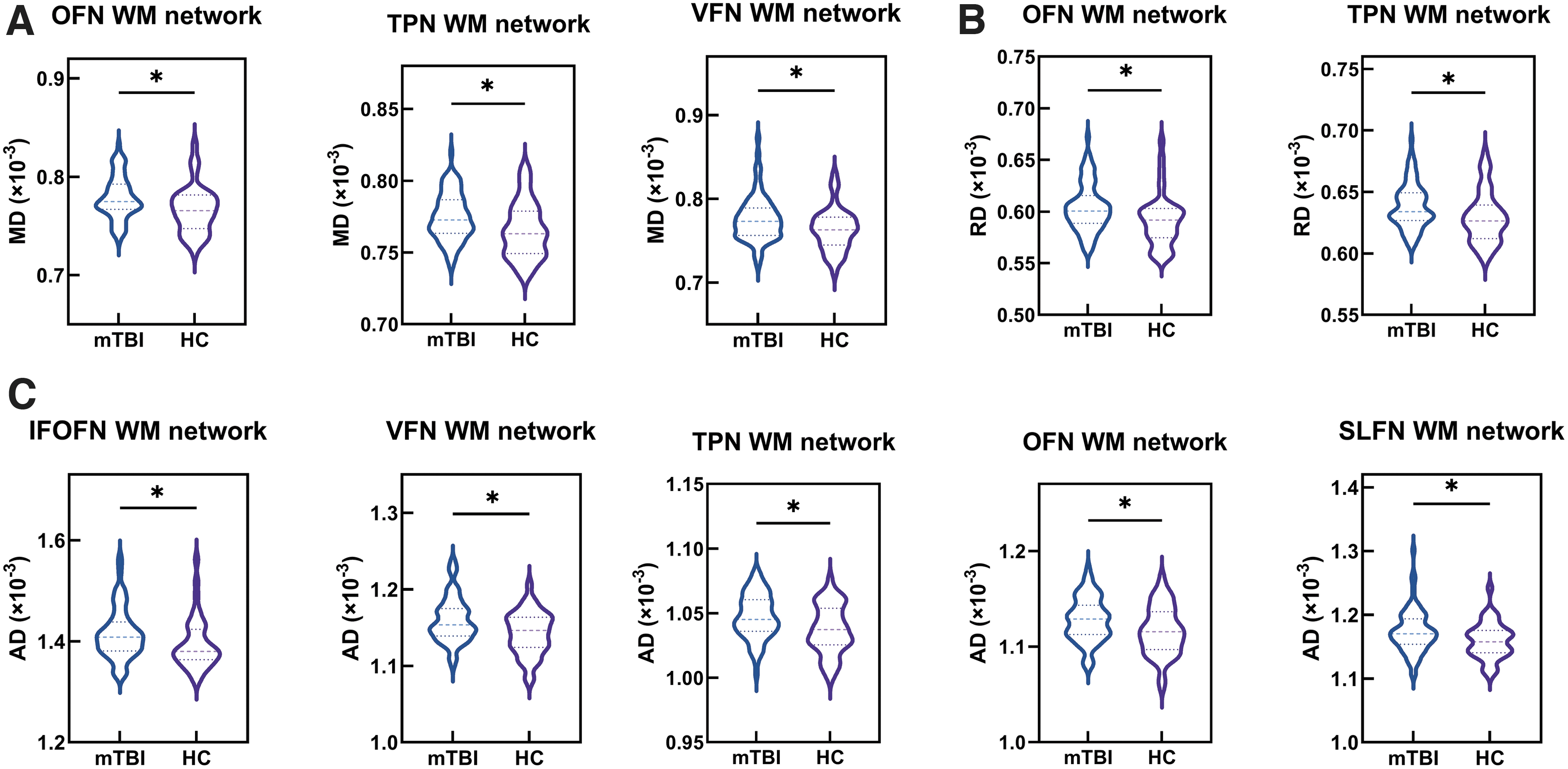
Group differences about diffusion tensor imaging metrics between the acute stage mild traumatic brain injury (mTBI) patients and healthy controls (HCs).
DTI, diffusion tensor imaging; mTBI, mild traumatic brain injury; SD, standard deviation; HCs, healthy controls; WM-FNs, white matter functional networks; MD, mean diffusivity; RD, radial diffusivity; AD, axial diffusivity.
DTI metrics in the chronic stage
Compared with HCs, chronic stage mTBI patients still showed significantly increased AD in deep WM-FNs and higher-order cognitive WM-FNs, but no significant differences in RD, MD, and FA were found. In detail, mTBI patients showed increased AD in ventral frontal network, orbitofrontal network, IFOF network, superior longitudinal fasciculus network, and temporoparietal network (Fig. 6; Table 5). Moreover, even the WM-FNs were constructed by the patients in chronic stage and HCs, and the results remained stable (Fig. S4).

Group differences about DTI metrics between the chronic stage mild traumatic brain injury (mTBI) patients and healthy controls (HCs). *Significant differences after false discovery rate correction. VFN, ventral frontal network; OFN, orbitofrontal network; IFOF, inferior fronto-occipital fasciculus network; SLFN, superior longitudinal fasciculus network; TPN, temporoparietal network; WM, white matter; AD, axial diffusivity. Color image is available online.
DTI, diffusion tensor imaging; mTBI, mild traumatic brain injury; SD, standard deviation; HCs, healthy controls; WM-FNs, white matter functional networks; AD, axial diffusivity.
Correlation between altered imaging data and cognitive and neurobehavioral symptoms assessments
The FC between IFOF WM-FN and anterior cerebellar GM-FN of acute stage mTBI patients was positively correlated with information processing speed (measured by TMT-A score; Fig. 3D). The other cognitive data or neurobehavioral symptoms assessments did not reveal a significant correlation with altered imaging data.
Discussion
The present study, for the first time, investigated the change of WM-FN in mTBI within a longitudinal study. Eleven distinct WM-FNs were identified by clustering voxel-wise WM functional connectivity. The altered FC and DTI metrics of WM-FN were observed in the acute stage mTBI patients, but full recovery of FC and partial recovery of DTI metrics were found in the chronic stage mTBI patients. Importantly, the IFOF WM-FN demonstrated enhanced FC both with the low-level GM primary sensorimotor networks, and with the low-level WM primary sensorimotor networks in acute mTBI patients. This enhanced FC might represent a compensatory or protective mechanism in response to cognitive deficits in acute mTBI. Intriguingly, mTBI patients also showed increased AD in IFOF network both in the acute stage and the chronic stage. The convergent damage of the IFOF network might highlight its crucial role in our understanding of the pathophysiology mechanism of mTBI patients.
WM-FNs analysis in the acute stage
Intriguingly, the IFOF WM-FN was found to be the most affected deep WM-FN both in functional and structural analysis in mTBI patients. The IFOF WM-FN showed enhanced FC both with the low-level GM primary sensorimotor networks (visual network, anterior cerebellar network, and sensorimotor network), and with the low-level WM primary sensorimotor networks (occipital network and pre/postcentral network) in patients with mTBI at the acute stage. Previous studies have reported the damaged structure property in IFOF in patients with mTBI. 11,34 Here, for the first time, the present study showed that increased FC between IFOF with low-level WM and GM primary sensorimotor networks in patients with mTBI. In general, the increased FC reflects an increased integrative ability sub-serving similar goals. 35 Hence, the increased FC between IFOF and sensorimotor networks may reflect a compensatory mechanism in mTBI.
As a long-distance associative tract, the IFOF plays a crucial role in sending the processed visual information from the occipital lobe to frontal lobe, where information was further translated into semantic information. 36 The observed increased FC between IFOF with low-level WM and GM primary sensorimotor networks may represent a compensatory effect in response to cognitive deficits. These enhanced FCs may indicate mTBI patients employed higher cognitive effort in integrating dynamic environmental sensory information and high-order cognitive function to coordinate their behaviors and thoughts to fit with contextual information. This interpretation is supported by previous studies to some extent which demonstrated abnormal activation of the intrinsic rich-club network in mTBI patients 37 and greater network strength in mTBI patients, 38 might suggest a potential compensatory or protective mechanism in mTBI patients.
In addition, consistent with previous study which showed altered diffusion metrics in fronto-parieto-temporal association fibers in mTBI patients, 39 we also found impaired diffusion metrics in deep WM-FNs (IFOF and superior longitudinal fasciculus network) and higher-order cognitive WM-FNs. This result might relate to the axonal and myelin sheath abnormalities of these WM-FNs in the acute stage mTBI. The current findings highlighted the importance of the IFOF WM-FN in such a compensatory mechanism, in which IFOF WM-FN may excessively contribute to integrating sensory information from GM and WM primary sensory-related network with high-order cognitive information in acute mTBI patients. The most affected damage in mTBI was located in IFOF network, which might imply the crucial role of IFOF network in our understanding of the pathophysiology mechanism of mTBI patients.
WM-FNs analysis in the chronic stage
Further, mTBI patients at the chronic stage did not differ from HCs in FC within WM-FNs or between GM-FN and WM-FN. Besides, the DTI metrics of WM-FNs in mTBI patients at the chronic stage also showed a partial recovery. These results are consistent with previous studies that reported partial recovery of functional connectivity after 6 months 38,40 and partial recovery of DTI metrics after 3-5 months. 41
A previous meta-analysis indicated that the damage effects for memory and fluency were greatest in the acute stage (less than 3 months post-injury) and no residual impairment by 3 months post-injury. 42 Besides, a recent large-sample longitudinal neuroimaging study of TBI revealed a “U-shaped” curve in sub-acute, 1 year and 5 years post-injury in the number of fractional anisotropy abnormalities. 43 Further, a previous study demonstrated a functional and structural abnormal connectivity in acute stage of mTBI patients, but a partial recovery of functional and structural connectivity patterns was revealed in chronic stage (after 1-year post-injury). 44 Combining previous studies and the current findings, our results might reflect compensatory mechanism of brain function and structure contributed to the recovery of cognition deficits in mTBI patients at the chronic stage.
The association between altered WM-FNs and cognitive and neurobehavioral symptoms assessments
The FC between IFOF WM-FN and anterior cerebellar GM-FN was positively correlated with information processing speed (IPS) in mTBI patients at acute stage. Previous studies reported that reduced IPS are pervasive and form the core of TBI-associated cognitive impairment. 45,46 Our results indicated the impaired IPS associated with the abnormal FC between IFOF WM-FN and anterior cerebellar GM-FN. In addition, previous studies mainly focused on the correlation between IPS with GM-FNs, 4,47 or white matter structural networks. 48 Our results, for the first time, suggested that the FC between WM-FN and GM-FN also was correlated with the impairment of IPS and offered separate novel evidence to support the cognitive impairment of mTBI patients. In addition, our neurobehavioral results indicated that compared with HC, mTBI patients showed significantly increased neurobehavioral symptoms, including post-concussive symptoms, insomnia and post-traumatic stress symptoms (Table 1).
However, we did not observe any correlation between the altered FC or diffusion metrics of WM-FNs and neurobehavioral symptoms. No significant relationship between the neurobehavioral symptoms and altered FC or diffusion metrics of WM-FNs after mTBI found here is consistent with previous studies, 49,50 in which altered WM integrity did not show the significant relationship with neurobehavioral symptoms. Thereby, we speculated that the altered FC or diffusion features of WM-FNs observed in the present study might be more likely to relate to cognitive impairment rather than neurobehavioral symptoms. Future studies with large sample size focusing on the investigation of the neural correlates of neurobehavioral symptoms would deepen our understanding the neurobehavioral symptoms in mTBI patients.
Limitations
Notwithstanding its implication, limitations of the current study should be acknowledged and addressed. Some researchers have speculated that the WM signals might have infiltrated from the GM for partial volume effect. To avoid the influence of GM signals, the spatial smooth of WM and GM signals were separately carried out within individual WM mask or GM mask to avoid the mixture of WM and GM signals. Besides, only the data of mTBI patients in the acute stage and the chronic stage (6-12 months post-injury) were collected; the data for longer follow-up such as 5 years post-injury should be collected as a follow-up. Based on a previous study, 43 the significant abnormalities of FA in TBI were observed at the sub-acute and 5 years post-injury, but not 1-year post-injury. Therefore, it is necessary to follow patients for a more sustained period to explore the development of the observed deficits of WM-FNs.
Conclusion
In summary, this study constructed WM-FNs of mTBI based k-means clustering algorithm. Our results revealed an excessive interaction between deep WM-FNs and low-level primary sensorimotor networks. In addition, we also found impaired DTI metrics in deep WM-FNs and high-order cognitive WM-FNs, which might relate to axonal damage of these regions in mTBI. Of note, mTBI patients showed full recovery of FC and partial recovery of DTI metrics in the chronic stage, suggesting a possible compensatory mechanism of brain function contributed to the recovery of cognition deficits in mTBI patients at the chronic stage. The convergent damage of IFOF network might highlight its key role in our understanding of the pathophysiology mechanism of mTBI patients.
Footnotes
Authors' Contributions
Xiaoyan Jia, Xuebin Chang, and Lijun Bai generated the idea of this study. Xiaoyan Jia, Xuebin Chang, Shuoqiu Gan, Shan Wang, Xuan Li, Xuefei Yang, Yingxiang Sun, Tianhui Li, Feng Xiong, and Xuan Niu designed this study, finished the calculation, and interpreted imaging data. Xiaoyan Jia, Xuebin Chang, Yulin Wang and Debo Dong drafted the manuscript. Xiaoyan Jia, Yulin Wang, Debo Dong, Lijun Bai and Hao Yan revised the manuscript.
Funding Information
This study was supported by the National Science Foundation of China (grant number 81771914, 82071993), the National Social Science Foundation of China (grant number 20BYY097), the Humanities and Social Science Foundation of Ministry of Education of China (grant number 19YJC740100), and the Fundamental Research Funds for the Central Universities (grant number RW180178, Xjj 2018229, xzy022019045).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.