
Abstract
Domestic violence (DV) is a chronic societal epidemic that often involves physical assault to the head, neck, and face, which increases the risk of traumatic brain injuries (TBIs) in DV victims. However, epidemiological data on the extent of TBI-DV at the population scale remain sparse. We performed a statewide, multi-institution, retrospective review of all medical records for patients diagnosed with a concussion, the most common type of TBI, at health care facilities in Arizona, USA, that were licensed by Arizona Department of Health Services (ADHS) during 2016-2018. De-identified records were extracted from discharge data reported to ADHS, which we decoded and transformed to spatiotemporal demographic data of patients who were diagnosed with concussion concurrent with DV. Among 72,307 concussion diagnoses, 940 were concurrent with DV. Sixteen patients died as a result of TBI-DV injuries, where TBI is defined as concussion. Although females were most of the TBI-DV diagnoses, median ages for males and females were 1 and 32 years, respectively, demonstrating that males were predominantly child abuse victims. Whites and Hispanics were victims most diagnosed with concussion and DV, but Native Americans and Blacks comprised a much greater proportion of diagnoses compared with the representative state demographics. Although likely underreported, approximately half of the cases were inflicted by intimate partners, which corresponded closely to marital status. Surprisingly, 61% of victims sought medical treatment for non-concussion injuries and then concussion was entered as a primary diagnosis. The demographic and health care facility disparities demand TBI/concussion screening in suspected DV patients, education and training of care providers, and potential redistribution of resources to select health care facilities.
Introduction
Domestic violence (DV) is violence or other abuse in a domestic setting, such as a marriage or cohabitation, and includes violence against children, adolescents, parents, and the elderly. DV is a serious public health problem that annually affects approximately 10 million people in the United States, with a national economic cost estimated at > $12 billion per year. 1 DV can result in physical injuries but victims often forego medical care and the circumstances surrounding injury remain unreported to health care providers or law enforcement. 1 This under-reporting has led to a hidden public health epidemic.
Physical injuries from DV are common to the head, neck, and face, 2 which increase the risk of traumatic brain injuries (TBIs), such as concussions, in DV victims. For these DV victims, repeated assault to the head and neck exacerbate the risk of both short- and long-term neurological consequences, beyond those reported for athletes and soldiers. 3,4 The physical impacts or forces applied to the head lead to cognitive, 5 neurological, and behavioral deficits, 6 as well as elevated risk for developing neurodegenerative disease, 7 post-traumatic headaches, 8 and/or psychiatric disorders. 9,10 Women who suffer intimate partner violence–related TBIs often have compromised cognitive function, 4 depression, anxiety, and post-traumatic stress disorder. 10 Child abuse inflicted on the head or neck (abusive head trauma) results in neurological complications that can include acquired hydrocephalus, cortical blindness, and developmental delays. 11 DV survivors have a high prevalence of repetitive TBIs that can span months to years, where any chronic long-term effects of brain injury may be exacerbated by more recent acute and sub-acute effects of TBIs. 12,13
Despite a presumably high prevalence of TBIs that result from DV, a paucity of studies exists that have investigated the epidemiology, cause, risk, and consequences of DV-inflicted TBIs at the population scale. Instead, most TBI-DV studies focused on small, local cohorts of DV victims at specific care facilities or in specific sex, ethnic, or age groups. The lack of population-level epidemiological data on TBI in DV victims was recently identified by the U.S. Government Accountability Office as the primary hindrance to addressing the problem and improving care and services. 14 Further, the ongoing COVID-19 global pandemic has created physical and mental health issues that extend beyond viral infection to include high incidence of DV. 15,16
With DV prevalent among the backdrop of society, the incidence of DV-inflicted TBIs leaves countless victims in harm's way, coping with neurological symptoms. To determine the extent of the problem and the demographic groups at risk for DV-inflicted TBI, it is necessary to quantify the population frequency and demographic distributions of DV-inflicted TBI. Further, epidemiological studies on the prevalence of TBI in DV victims can inform screening and treatment of TBIs, training for health care workers to recognize TBI, and ensure sufficient resources are allocated to appropriate health care facilities and survivors of DV-inflicted TBI. Herein, we provide the first population-level evaluation of concussion, the most common type of TBI, and DV diagnoses with a multi-institution, retrospective review of all medical records for patients diagnosed with a concussion concurrent with DV at health care facilities in Arizona during 2016-2018.
Methods
Following approval from the Arizona Department of Health Services (ADHS) Human Subjects Review Board (HSRB #19-0025), we obtained selected de-identified health care facility discharge data that were reported to ADHS by licensed health care facilities (general/regional hospitals, emergency departments, outpatient medical centers, and rehabilitation centers) throughout Arizona. Reporting of this information to ADHS was required of all licensed health care facilities per Arizona Revised Statute § 36-125-05 and Arizona Administrative Code Title 9, Chapter 11. Facilities associated with Indian Health Services do not report data to ADHS. The de-identification process conducted by ADHS removed all personal identification information, but assigned each individual a unique random number identifier.
The requested data represented all occurrences of patients who were diagnosed with a concussion in Arizona during 2016–2018 (n = 72,307) and contained 279 potential data fields for each occurrence. Concussion was queried based on coding of the 10th Revision of the International Statistical Classification of Diseases, Clinical Modification (ICD-10-CM), selecting all records with S06.0 and S06.0X diagnosis code prefixes. The data also were linked by ADHS to state death records data reported by medical examiners.
We then filtered the concussion dataset based on ICD-10-CM, selecting all records with T74 and T76 diagnosis code prefixes, which correspond to confirmed and suspected abuse/maltreatment, respectively. 17,18 This filtering resulted in a statewide, population-level dataset comprised of patients who were diagnosed with a concussion concurrent with DV. We then decoded all demographic data fields and derived additional spatial data fields (e.g., geographical coordinates for each facility) to transform the dataset into spatiotemporal demographic data.
We used a combination of density, violin, box, and bar plots, and z-tests for two population proportions to describe the demographic incidence, distribution, and patterns of diagnosed concussion-DV in Arizona. All plotting and analyses were performed using the ggplot2 (v3.3.2) 19 and stats packages (v4.1.0) in the R statistical computing environment (v3.6.3), 20 via RStudio (v1.2.5033). 21 We present most demographic characteristics in the context of patient recorded sex and/or age, which often account for much of the variation in population-level DV data and therefore serve as useful descriptive grouping categories. 1,22 Specifically, we present the following demographic information: ethnicity/race, marital status, age group, mortality, and DV type. Gender and sexual orientation information did not exist in the dataset. We also present information on whether the patient was a rural or urban resident and sought care for a suspected concussion or brain injury and the type of health care facility that was visited (general, specialized, or rural). Rurality information was derived by cross-referencing ZIP codes with Rural-Urban Commuting Area (RUCA) codes. 23 Finally, we conducted a kernel density analysis at 100-meter resolution using the spatial analyst toolbox in ArcMap (v10.4.1) 24 to attempt to identify geographical hotspots of licensed health care facilities (n = 123 total, during 2016–2018) where concussion-DV diagnoses were more likely to occur. 25,26
Results
Our final dataset was comprised of 940 concussion-DV diagnoses, with 19 individuals having second diagnoses at later dates during the study period, representing a 3-year period prevalence of 1.3%. Annually, the highest monthly number of concussion-DV diagnoses tended to occur during spring and summer (March-August), with no apparent relationship between data for males and females (Fig. 1). Although 32 patients' deaths were associated with concussion-DV, the death records for 16 of those individuals indicated that other causes may have been partial contributors; for example, liver and heart disease (n = 6) and dementia and Alzheimer's disease (n = 3) were included as secondary or tertiary causes. Thus, despite the overall case fatality rate being 3.5%, the case fatality rate attributed solely to concussion-DV and no other causes was 1.7% (Fig. 2).
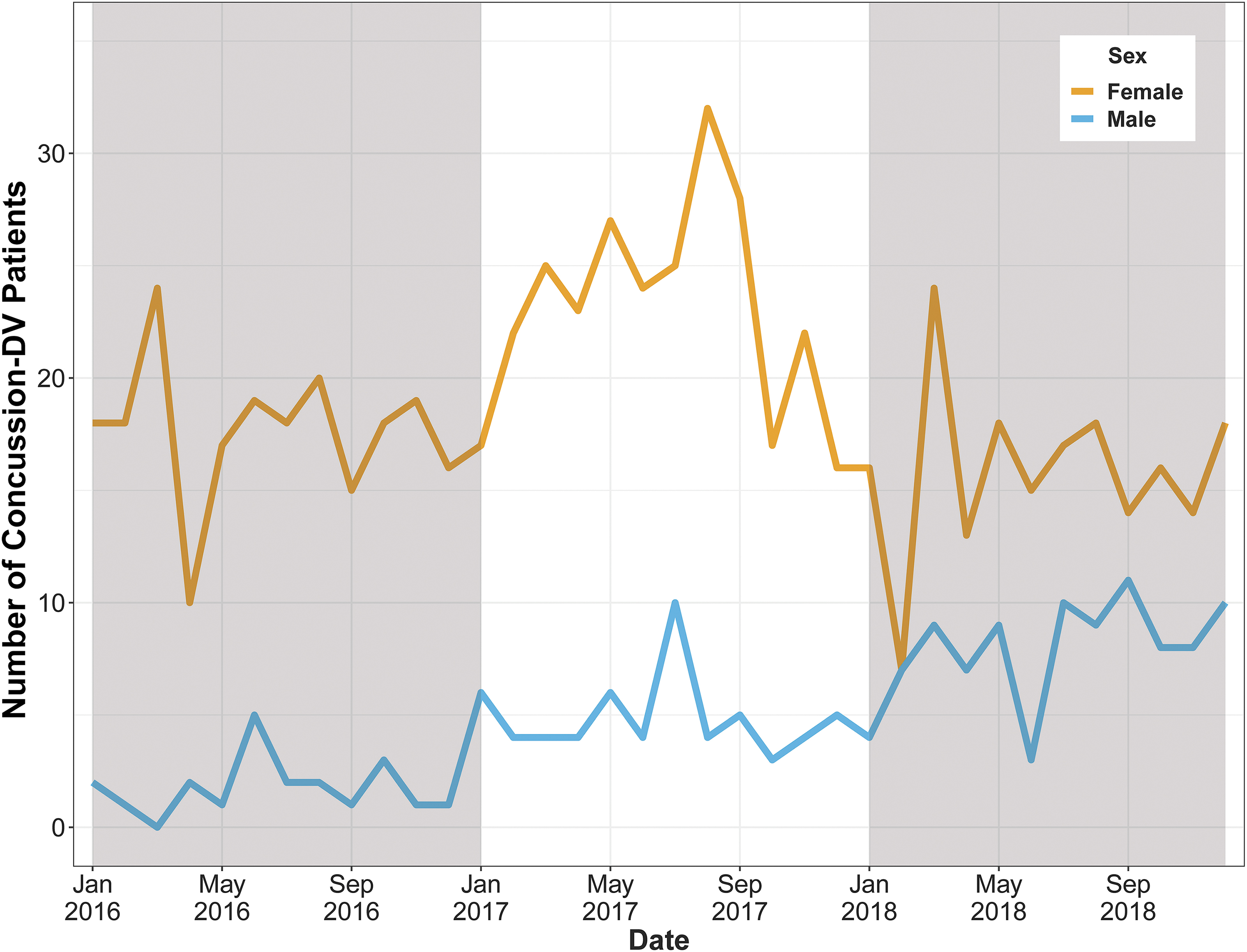
Sex-specific trend lines of the monthly number of concussion-domestic violence (DV) patients in Arizona, USA, during 2016-2018. Color image is available online.

Violin plots with overlaid box plots showing the sex-specific age distributions, medians, quartiles, and statistical outliers of patients who had concussion-domestic violence diagnoses and did not die compared to those who died in Arizona, USA, during 2016-2018. Gray dashed line indicates legal adult age (18 years). Color image is available online.
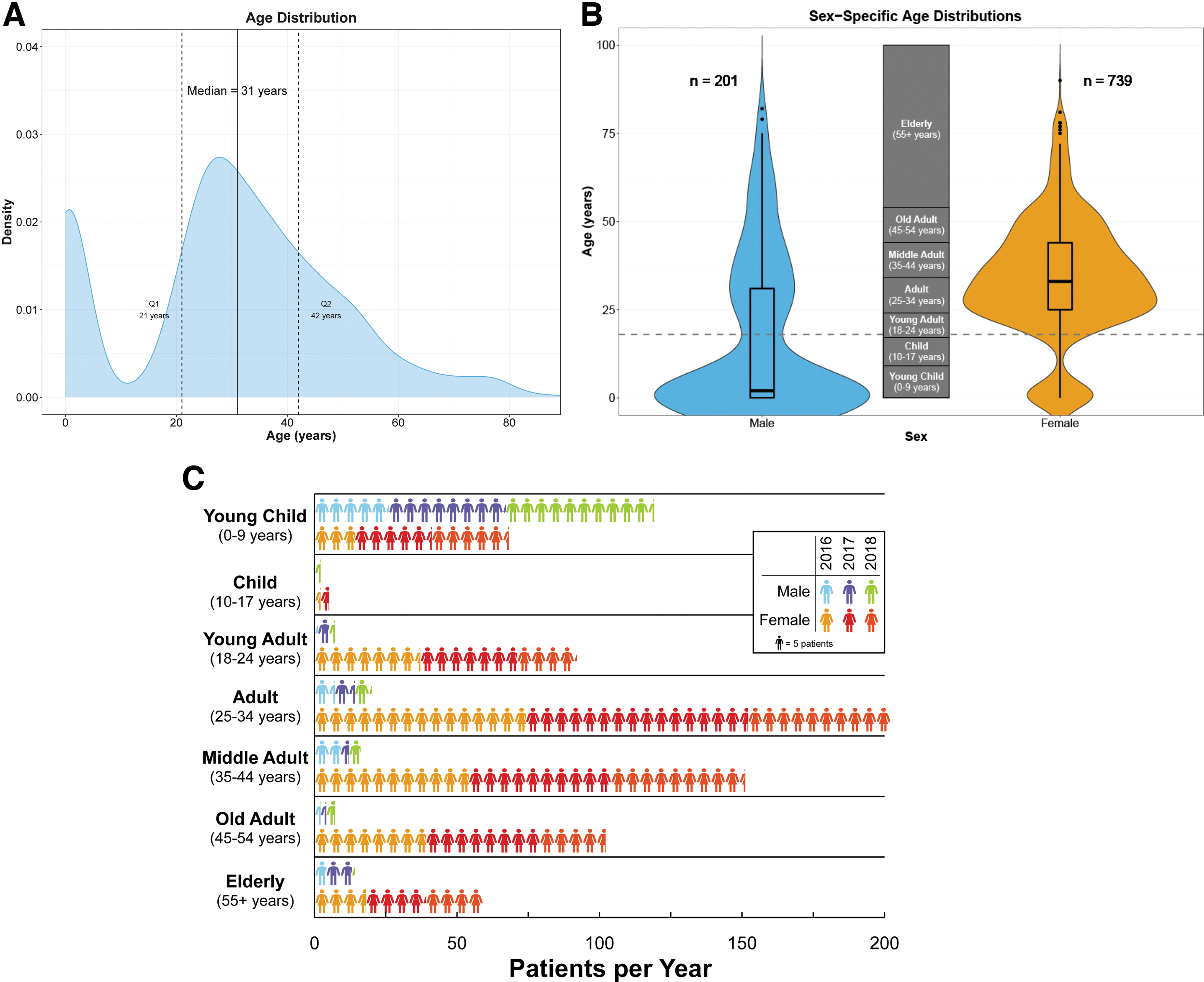
The median age of patients was 31 years, with lower and upper quartiles of 21 and 42 years, respectively (Fig. 3A). However, the age distribution was distinctly bimodal, with peaks that corresponded closely to sex, whereby the median male and female ages were 1 and 32 years, respectively (Fig. 3B). The majority of concussion-DV diagnoses were in females (79%), most of which (90%) were in one of the five adult age classes (≥ 18 years), whereas most male diagnoses were young children (< 10 years; 60%; Fig. 3C). Most concussion-DV diagnoses were of Whites (48%) and Hispanics (29%; Fig. 4A), but these ethnicities comprised smaller proportions of diagnoses compared with respective demographic representations in Arizona (Whites: z = -3.89, p = 0.0001; Hispanics: z = -2.03, p = 0.04; Fig. 4B). 27 Similarly, concussion-DV diagnoses in Asians (1.1%) were proportionally smaller than the demographic representation in Arizona (z = -4.28, p < 0.0001).
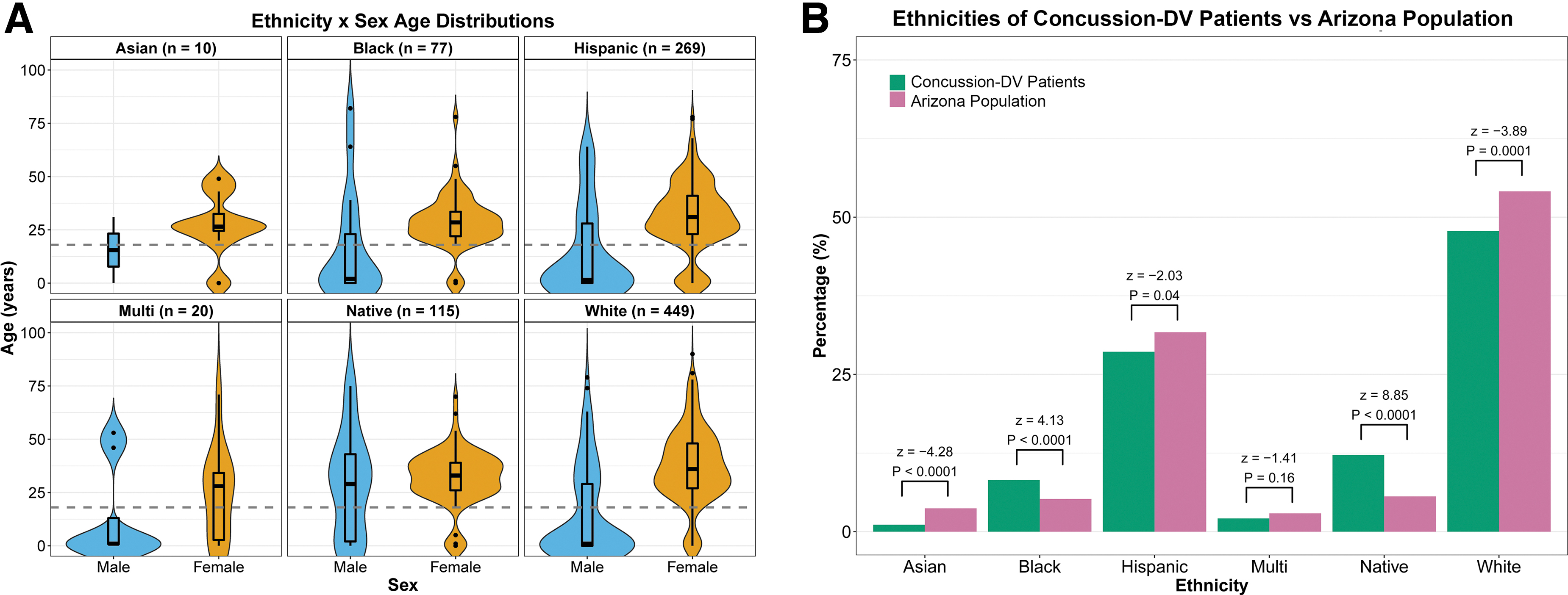
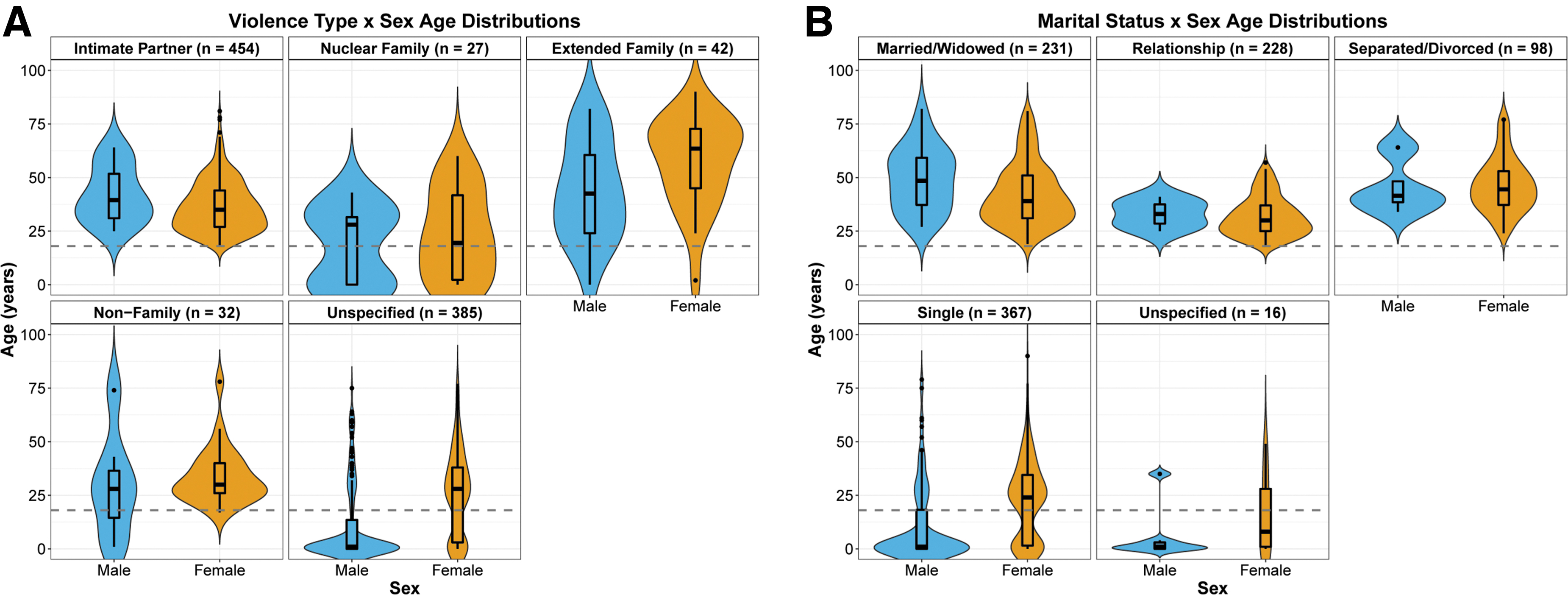
In contrast, Native Americans (12%) and Blacks (8%) comprised larger proportions of concussion-DV diagnoses compared with the demographic representations in Arizona (Natives: z = 8.85, p < 0.0001; Blacks: z = 4.13, p < 0.0001). Approximately half (48%) of the concussions were inflicted by intimate partners, although this comprised 61% of all adult (≥ 18 years) diagnoses; the perpetrator was unspecified for 41% of patients, which comprised 92% of all child abuse diagnoses (Fig. 5A). Similarly, 49% of diagnoses were in patients who were in a relationship, married, or widowed, which represented 62% of all adult diagnoses (≥ 18 years; Fig. 5B). In contrast, 51% of diagnoses for single patients were children. Approximately 61% of patients visited a health care facility for reasons unrelated to a brain injury but the concussion was a subsequent primary diagnosis; most of those patients were female adults (63%) and male children (19%; Fig. 6).

Violin plots with overlaid box plots showing the sex-specific age distributions, medians, quartiles, and statistical outliers of patients who did not (NO) and did (YES) visit a health care facility because of a suspected TBI (concussion) and were diagnosed with concussion-DV in Arizona, USA, during 2016-2018. Gray dashed line indicates legal adult age (18 years). Color image is available online.
Most adults ≥18 years were discharged from general health care facilities in urban areas (94%; e.g., general/regional hospitals, emergency departments, or outpatient facilities), whereas most children (< 18 years) were discharged from specialized facilities (70%; e.g., children's hospitals or rehabilitation centers; Fig. 7). Kernel density analysis identified two distinct hotspots of health care facilities where most concussion-DV diagnoses occurred in Arizona, the largest of which encompassed an 890-km2 portion of the greater Phoenix metropolitan area and included 17 facilities (Fig. 8). Seven of those facilities, including Phoenix Children's Hospital, were located within the epicenter of highest concussion-DV diagnosis density in Arizona. The second hotspot encompassed a 436-km2 portion of Pima County, centered on the city of Tucson, and included five facilities. Collectively, most concussion-DV diagnoses occurred at just 18% of all licensed health care facilities in Arizona.
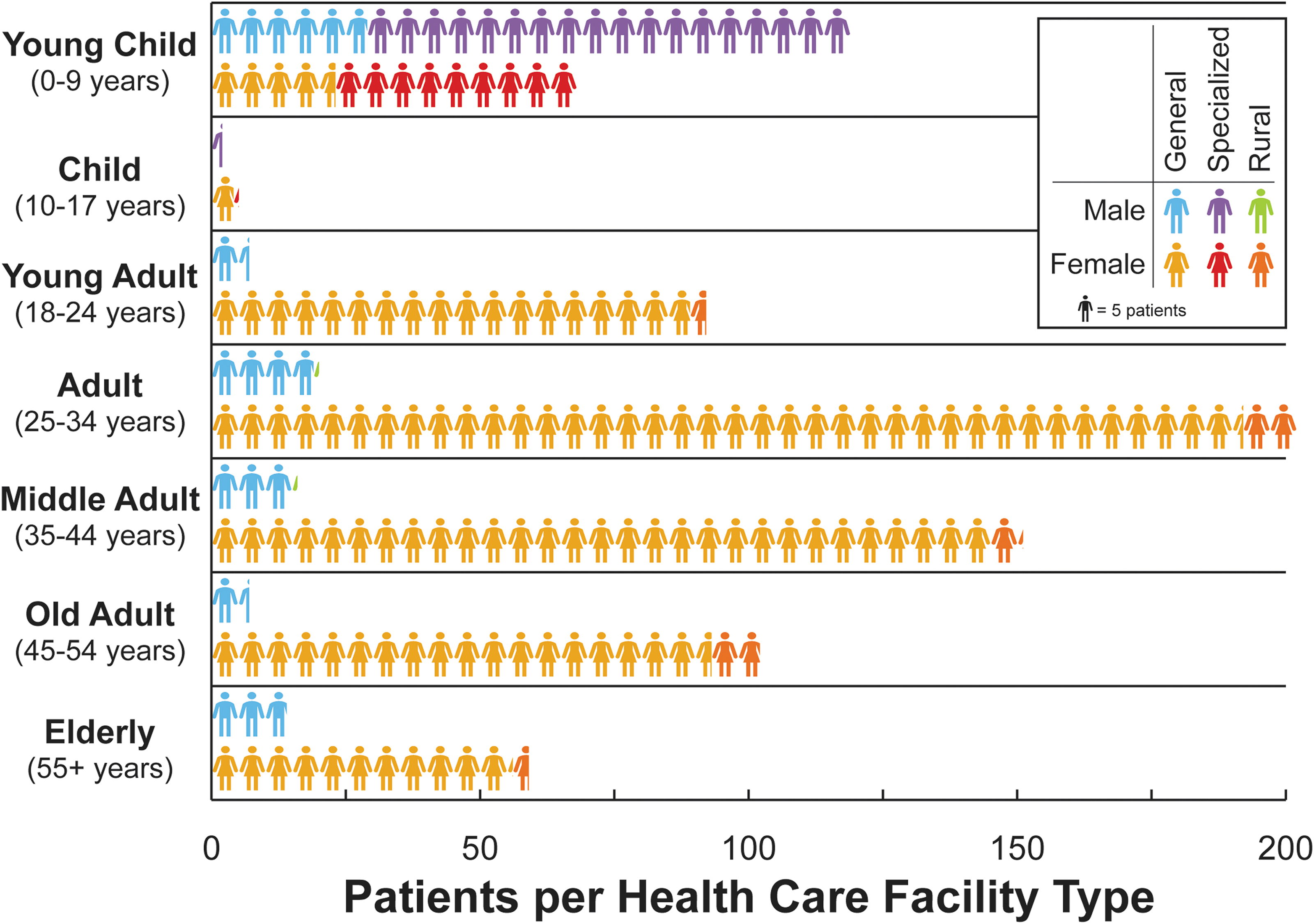
Age group- and sex-specific distributions of the number of concussion-domestic violence diagnoses at the three major types of licensed health care facilities in Arizona, USA, during 2016-2018. Color image is available online.
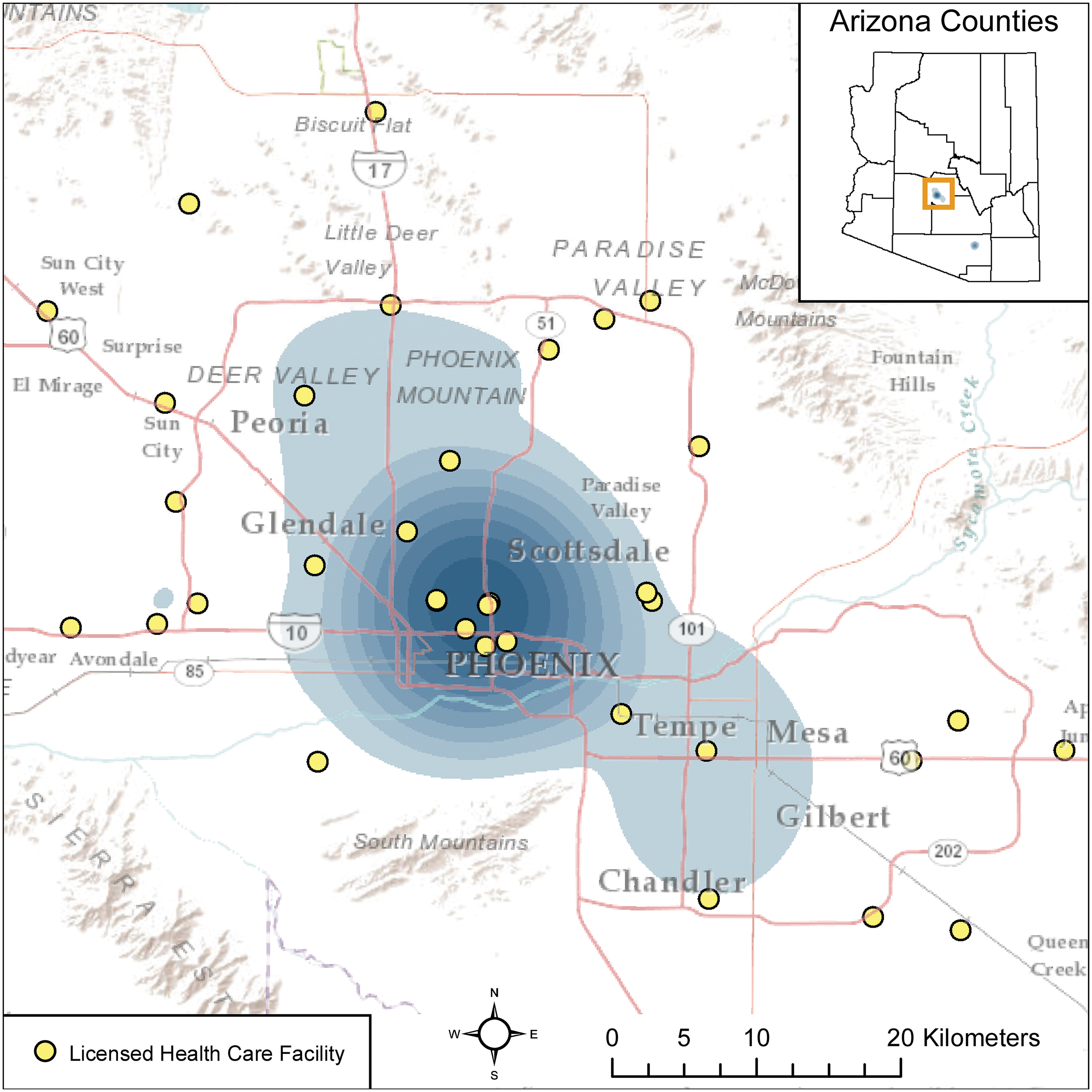
Results from a kernel density analysis showing two identified hotspots (blue shaded areas) of licensed health care facilities in Arizona, USA, where most concussion-domestic violence diagnoses occurred (inset map), and the locations of licensed health care facilities relative to the largest hotspot that was located in the greater Phoenix metropolitan area (2016-2018). Color image is available online.
Discussion
Globally, the victims of domestic violence are predominantly women and the most common form is intimate partner violence. 28 Recognized as an urgent public health issue, intimate partner violence is reported by 30% of all women ≥15 years of age. 28 Survivors of DV are at an increased risk of subsequent comorbid health conditions (e.g., cardiovascular disease, fibromyalgia, temporomandibular joint disorder) 29 -31 and compromised mental health such as anxiety and depression. 32 In a sample of 99 women who experienced intimate partner violence, 75% sustained a single TBI, including but not limited to concussions, and 50% reported multiple partner-related TBIs. 3 Similarly, in Arizona, we found that 79% of the concussion-DV diagnoses occurred in females, with the majority identifying the perpetrator as an intimate partner. Alarmingly, almost two-thirds of adult females (≥ 18 years) who had a concussion concurrent with DV visited a health care facility for reasons unrelated to a brain injury. Individuals exposed to domestic violence often avoid medical care for their injuries, whether by choice, stigma, or influence of their abuser. As of 2018, all but three states in the U.S. have laws that mandate health care providers report DV-inflicted injuries to local law enforcement. The Arizona Revised Statutes 46-454 requires health care providers to report DV to law enforcement, peace officers, or protective services. Although mandatory medical reporting can hold perpetrators accountable, unintended consequences may deter DV survivors from seeking help. Based on surveys of women who sought services from regional domestic violence shelters in Kentucky, 63.6% of the women responded that mandatory reporting requirements would make them less likely to disclose abuse to a doctor or nurse. 33 Therefore, victims may seek support from non-health organizations (e.g., shelter, social services), which compounds the underreporting in data sets of both domestic violence in adult women and subsequent TBIs, including the present report. 34 -36
Males are also victims of DV, but adult males are even less likely to report such incidents to authorities or seek medical care for DV-associated trauma than women. 37 -39 Consequently, concussion-DV diagnoses in adult males (≥ 18 years) in our dataset likely also underrepresent the true frequency of occurrence. Nevertheless, we found that the median age for males who received a concussion-DV diagnosis in Arizona was 1 year, and males comprised 62% of all concussion-DV diagnoses in children. Abusive head trauma is a significant cause of morbidity and mortality in the pediatric population, 40 impairing cognitive development, fine motor function, and language. 41 The majority of children in our dataset were seen at a specialized treatment facility, most notably Phoenix Children's Hospital. Therefore, our results encourage staff at children's hospitals to receive specific education to recognize, diagnose, and manage pediatric abusive head trauma, 42 with particular scrutiny applied to male children.
Although male concussion-DV diagnoses among ethnic groups were predominantly in children, this was not the case for Native Americans, whose median age for male victims was 28 years. The demographics of Arizona are unique in that, proportionally, Arizona has the third largest Native American population, the fourth largest Hispanic population, and the ninth smallest White population in the U.S. Despite the ethnic composition of Arizona sharply contrasting with the nationwide ethnic composition of the U.S., trends in DV observed at the nationwide scale were evident in the concussion-DV trends in Arizona. For instance, Native Americans and Blacks comprised disproportionately larger numbers of concussion-DV diagnoses relative to their population proportions in Arizona, whereas Whites, Hispanics, and Asians comprised disproportionately smaller numbers of diagnoses relative to their population proportions, all of which mirror nationwide trends for DV in general. 43 Again, the occurrences may be underreported for Native American groups, as Indian Health Services facilities do not report discharge data to the Arizona Department of Health Services. Thus, our findings lend further support for targeting intervention and education efforts in communities that serve Native Americans and Blacks to attempt to curtail DV and by association, concussion-DV. 44 –47
A substantial portion of patients who sought medical care did not report a suspected brain injury, but upon treatment were subsequently diagnosed with a concussion. In surveys, both health care workers and survivors of intimate partner violence often did not recognize the signs or symptoms of TBI. 48 Thus, the need exists for increased education and training for health care providers and frontline workers. Further, concussion-DV can be recognized, reported, and referred by other service providers, such as dentists, dental care professionals, and oral and maxillofacial surgeons, since assault often involves the head, neck, and face. 49,50
Most concussion-DV diagnoses occurred at only 18% of all licensed health care facilities in Arizona. Either these facilities have improved training and awareness to screen for and diagnose TBI or this trend reflects the population density and proximity to medical centers, given both identified hotspots were in Arizona's two largest cities. Yet, we found evidence of numerous patients who resided in rural areas had traveled to facilities in the hotspots for care rather than visiting local rural health care facilities. For example, most Native Americans in Arizona reside on tribal lands in rural areas, but 46% of these patients were diagnosed with concussion-DV at facilities located in one of the urban hotspots. Although individuals may have sought treatment in urban areas based on the severity of their injuries, since most Level 1 trauma centers in Arizona are located in urban areas; the current data prevented further insight due to de-identification from medical records or telephone interview. Nevertheless, the rationale for resource allocation can be made both for hotspots where patients primarily seek care and for rural locations to improve services provided for victims and survivors of DV. 51
Conclusion
The primary limitations of these data are that: 1) the symptoms that victims experienced were severe enough for patients to visit a health care facility, or that caretakers of children perceived the symptoms as severe enough to warrant treatment; 2) health care providers accurately diagnosed TBI and DV and subsequently coded said diagnoses accurately; and 3) the data were limited to diagnostic codes for concussions and did not include other forms of TBI, such as anoxia or skull fracture. The true rate of DV in Arizona is unknown, but an estimated 1.25 million Arizonans will experience DV at some point during their lifetime, 52 and an estimated 90% of those victims will exhibit concomitant symptoms of TBI. 53 DV victims who visit health care facilities for care often do not report, or do not accurately report, that the cause of injury was DV-related or who the perpetrator was, as evidenced by the 41% of patients with concussion-DV diagnoses in our data for which the perpetrator was unspecified. DV victims also may report a subset of TBI symptoms, which obscures a TBI or concussion diagnosis. Further, health care providers sometimes do not code DV as a primary diagnosis in the ICD-10-CM framework despite victims self-reporting the underlying cause of their visit as being DV-related. 17 Collectively, the true population size of individuals who actually had a concussion concurrent with DV was likely much larger than the discharge data reflect.
Footnotes
Acknowledgments
We thank S. Robert Bailey and Dr. Tim Flood at the Arizona Department of Health Services for their assistance with compiling, procuring, and translating the data used in this study.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Arizona Department of Health Services or the State of Arizona.
Data collected for the study require approval from a human subject review board and are available from Arizona Department of Health Services upon request and approval.
Authors' Contributions
HH and JL were responsible for the conceptualization of this study and obtaining Institutional Review Board approval. SMM was responsible for data processing and analyses. RKR was responsible for writing the first draft of the manuscript. All authors contributed to data interpretation, editing of the manuscript, and approval of the final version.
Funding Information
RKR and JL were funded by Phoenix Children's Hospital Mission Support Funds. SMM, HH, and JL were funded by a grant from the Kemper and Ethel Marley Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.