
Abstract
Magnetic resonance imaging (MRI) is used rarely in the acute evaluation of traumatic brain injury (TBI) but may identify findings of clinical importance not detected by computed tomography (CT). We aimed to characterize the association of cytotoxic edema and hemorrhage, including traumatic microbleeds, on MRI obtained within hours of acute head trauma and investigated the relationship to clinical outcomes. Patients prospectively enrolled in the Traumatic Head Injury Neuroimaging Classification study (NCT01132937) with evidence of diffusion-related findings or hemorrhage on neuroimaging were included. Blinded interpretation of MRI for diffusion-weighted lesions and hemorrhage was conducted, with subsequent quantification of apparent diffusion coefficient (ADC) values. Of 161 who met criteria, 82 patients had conspicuous hyperintense lesions on diffusion-weighted imaging (DWI) with corresponding regions of hypointense ADC in proximity to hemorrhage. Median time from injury to MRI was 21 (10–30) h. Median ADC values per patient grouped by time from injury to MRI were lowest within 24 h after injury. The ADC values associated with hemorrhagic lesions are lowest early after injury, with an increase in diffusion during the subacute period, suggesting transformation from cytotoxic to vasogenic edema during the subacute post-injury period. Of 118 patients with outcome data, 60 had Glasgow Outcome Scale Extended scores ≤6 at 30/90 days post-injury. Cytotoxic edema on MRI (odds ratio [OR] 2.91 [1.32–6.37], p = 0.008) and TBI severity (OR 2.51 [1.32–4.74], p = 0.005) were independent predictors of outcome. These findings suggest that in patients with TBI who had findings of hemorrhage on CT, patients with DWI/ADC lesions on MRI are more likely to do worse.
Introduction
Cerebral edema contributes to the pathogenesis of secondary injury after traumatic brain injury (TBI) and stroke. 1 –3 The failure of energy-dependent processes can lead to cytotoxic edema, which appears on acute magnetic resonance imaging (MRI) as a hyperintense signal on diffusion-weighted imaging (DWI), caused by a correlated decrease in the apparent diffusion coefficient (ADC) of water. With hemorrhagic transformation, a mix of cytotoxic and vasogenic edema occurs, with an evolution toward the latter over 5 to 10 days, accompanied by normalization of the ADC as water mobility increases. 4 –12
The cause of the vasogenic edema remains an area of active investigation, potentially attributable to the acute immune response and amenable to therapy. Because MRI and especially serial MRI are used rarely in the acute setting for TBI, it is unknown whether traumatic lesions undergo a similar transformation from cytotoxic to vasogenic.
Identification of acute cytotoxic edema after TBI has important clinical implications. While vasogenic edema is, in principle, reversible, lesions identified as cytotoxic on acute MRI may represent non-viable tissue and be an independent predictor of poor outcome. Evidence of large hemorrhagic lesions is a known predictor of poor outcome in moderate and severe TBI, presumably in part because of concomitant parenchymal injury leading to cell death. 2 In patients with mild TBI, however, the relationship between acute hemorrhage and outcome has not been investigated thoroughly, leading to conflicting findings. Although molecular processes involved in cytotoxic and vasogenic edema are interrelated, 2 distinct therapeutic approaches would be beneficial for patients with MRI-identified acute cytotoxic edema.
After TBI of all severities, traumatic microbleeds (TMBs) predict poor outcome and may be indicative of primary traumatic vascular injury. 13,14 We hypothesized that traumatic vascular injury may be associated with early cytotoxic edema, with subsequent evolution toward vasogenic edema. Tissue ADC values in proximity to TMBs or larger traumatic lesions such as contusion or intraparenchymal hemorrhage (IPH) would then be low early after injury. With increasing time from injury, ADC values would be isointense—i.e., normalize, as described in stroke studies. We further hypothesized that cytotoxic edema associated with traumatic vascular injury could predict poor clinical outcome.
The goals of this study are to: (1) describe the concordance of DWI hyperintense lesions with the presence and type of hemorrhage and associated ADC lesions, (2) quantify acute values and temporal evolution of hemorrhage-associated ADC, in particular TMBs, over the first week after TBI, and (3) determine whether cytotoxic edema associated with vascular injury is a predictor of clinical outcome.
Methods
Additional details are available in Supplementary Methods.
Patient population and study design
This is an observational cohort analysis of adult patients with TBI prospectively enrolled in the Institutional Review Board approved Traumatic Head Injury Neuroimaging Classification (THINC) study (NCT01132937) from October 2010 to May 2017. Written informed consent was obtained before any research procedures. Enrolled patients were included for retrospective analysis if they had (i) completed baseline visit with MRI within 48 h of injury, (ii) an imaging target defined as an acute or subacute lesion on DWI, or hemorrhage on MRI or computed tomography (CT), including TMB, contusion, IPH, or subarachnoid hemorrhage, (iii) Glasgow Coma Scale (GCS) score assessed at baseline, and (iv) one-week follow-up MRI (Fig. 1). Optional follow-up visits with Glasgow Outcome Scale Extended (GOSE) occurred at 30 and 90 days.
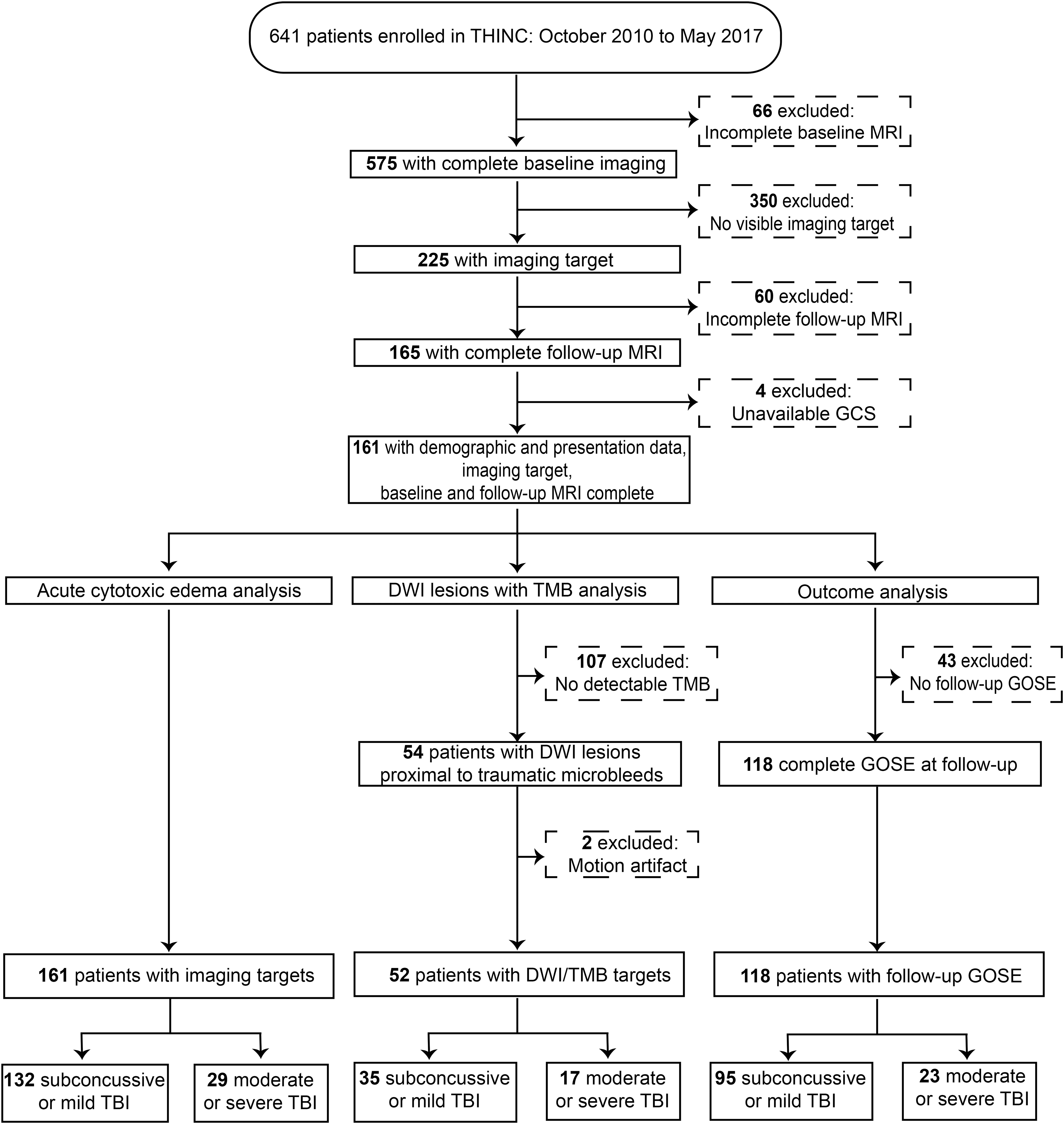
Flowchart of study patient inclusion and exclusion. THINC, Traumatic Head Injury Neuroimaging Classification study (NCT01132937); MRI, magnetic resonance imaging; GCS, Glasgow Coma Scale; DWI, diffusion-weighted imaging; TMB, traumatic microbleed; GOSE, Glasgow Outcome Scale Extended; TBI, traumatic brain injury.
Image acquisition
Patients were imaged for research purposes on a 1.5T (GE Healthcare, USA) or a 3T (Siemens, USA or Phillips, USA) MRI scanner using a standardized imaging protocol, appropriate for imaging in an acute care setting 13 and approximately 30 min in duration. The imaging protocol included (i) diffusion tensor imaging and DWI/ADC, (ii) T2*, (iii) T2-weighted fluid attenuated inversion recovery (FLAIR), (iv) three dimensional (3D)-T1 SPGR, (v) two-dimensional (2D)-T1 weighted, (vi) either dynamic susceptibility contrast perfusion or dynamic FLAIR during injection of a single weight-adjusted dose of gadolinium-based contrast agent at 5 mL/sec, (vii) post-contrast 2D-T1, and (viii) post-contrast FLAIR.
Image analysis
Image interpretation and analysis were completed in two stages with blinding to minimize investigator bias: (i) independent raters reviewed imaging for qualitative identification of focal lesions on DWI/ADC to determine their concordance with evidence of blood on T2* imaging and to classify the type of all hemorrhagic lesions observed for each patient, irrespective of association with diffusion changes; and (ii) the quantitative ADC value in areas of focal DWI hyperintensity was assessed by a separate set of trained raters independent of the findings from the qualitative consensus review. Only after quantitative measurements were complete were labels matched for statistical analysis, with each focal lesion assigned to a single type of lesion.
Statistical analysis
Interrater agreement was assessed using the Cohen kappa. Mean or median are reported, and non-parametric testing (Wilcoxon rank-sum and Mann-Whitney U) was used unless normality could be established (Kolmogorov-Smirnov test) for univariate analysis; categorical variables are presented as proportions (chi-square or Fisher exact tests). Baseline variables were compared between patients with and without evidence of cytotoxic edema, for all patients and excluding moderate and severe TBI.
Univariate analysis was performed on predictors of residual disability (defined as GOSE score ≤6 from latest available of 30- or 90-day follow-up), for all patients and excluding moderate and severe TBI. Stepwise logistic regression was used to test for independence using p = 0.05 for entry and p = 0.1 for removal. Statistical analysis was performed in IBM SPSS™ (Version 26).
Results
Patient population
One-hundred sixty-one patients met criteria and were included in this study as follows: consent was obtained from 641 patients from October 2010 to May 2017, 575 completed baseline imaging, 225 had an imaging target (defined as acute or subacute lesion on DWI, or hemorrhage on MRI or CT), 165 completed follow-up MRI, and four were excluded because of unavailable GCS score (see flowchart in Fig. 1).
Demographics and baseline data are presented in Table 1. Patients were predominantly male (73%). Twenty-nine (18%) were classified as having moderate or severe TBI. Median times from injury to clinical CT and to research MRI were 1.7 (1.1–6.4) and 21 (10–30) h. A majority of the included patients (59%) had evidence of acute blood on CT, largely attributable to extra-axial hemorrhage. Of the 20% of patients who were CT negative but MRI positive, 94% had TMBs.
Patients Stratified by Absence or Presence of Cytotoxic Edema

Temporal evolution of cytotoxic edema
Figure 2 displays examples of DWI hyperintense lesions on research MRI, stratified by proximity of hemorrhagic findings on T2* imaging. Most lesions, except those associated with IPH, were small and punctate or linear appearing (Fig. 2A, in reconstructed multi-planar view). One hundred seventeen (73%) patients had lesions conspicuous on DWI, and 82 (51%) had corresponding visible regions of hypointense ADC, suggestive of cytotoxic edema.
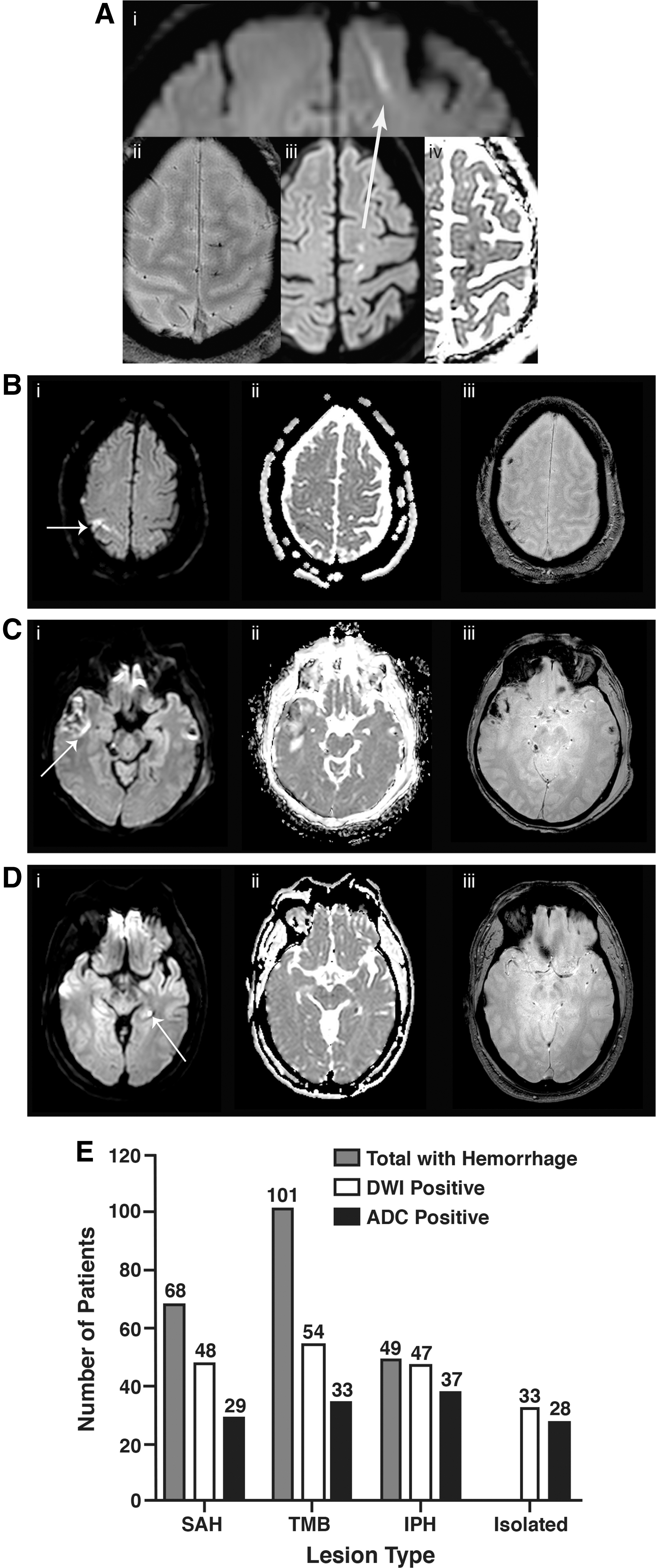
Types of acute traumatic brain injury lesions associated with magnetic resonance imaging findings. White arrows indicate the areas of interest. (
Interrater agreement for presence of DWI hyperintensity and ADC hypointensity was k = 0.78 and k = 0.73, respectively. Agreement on association with hemorrhagic lesion type varied from k = 0.38 to 0.8. Approximately half of patients with TMBs, in comparison with ∼95% of patients with IPH, also had DWI hyperintense lesions. Of 33 isolated DWI lesions, 28 (85%) were correspondingly hypointense on ADC.
Figure 3 shows a patient with DWI hyperintensity in proximity to a TMB at initial presentation and follow-up. The TMB conspicuity appears similar on gradient recalled echo (i) and DWI (ii). The lesion on ADC (iii) transitions from hypointense to hyperintense and increases in conspicuity on follow-up T2 FLAIR (iv).
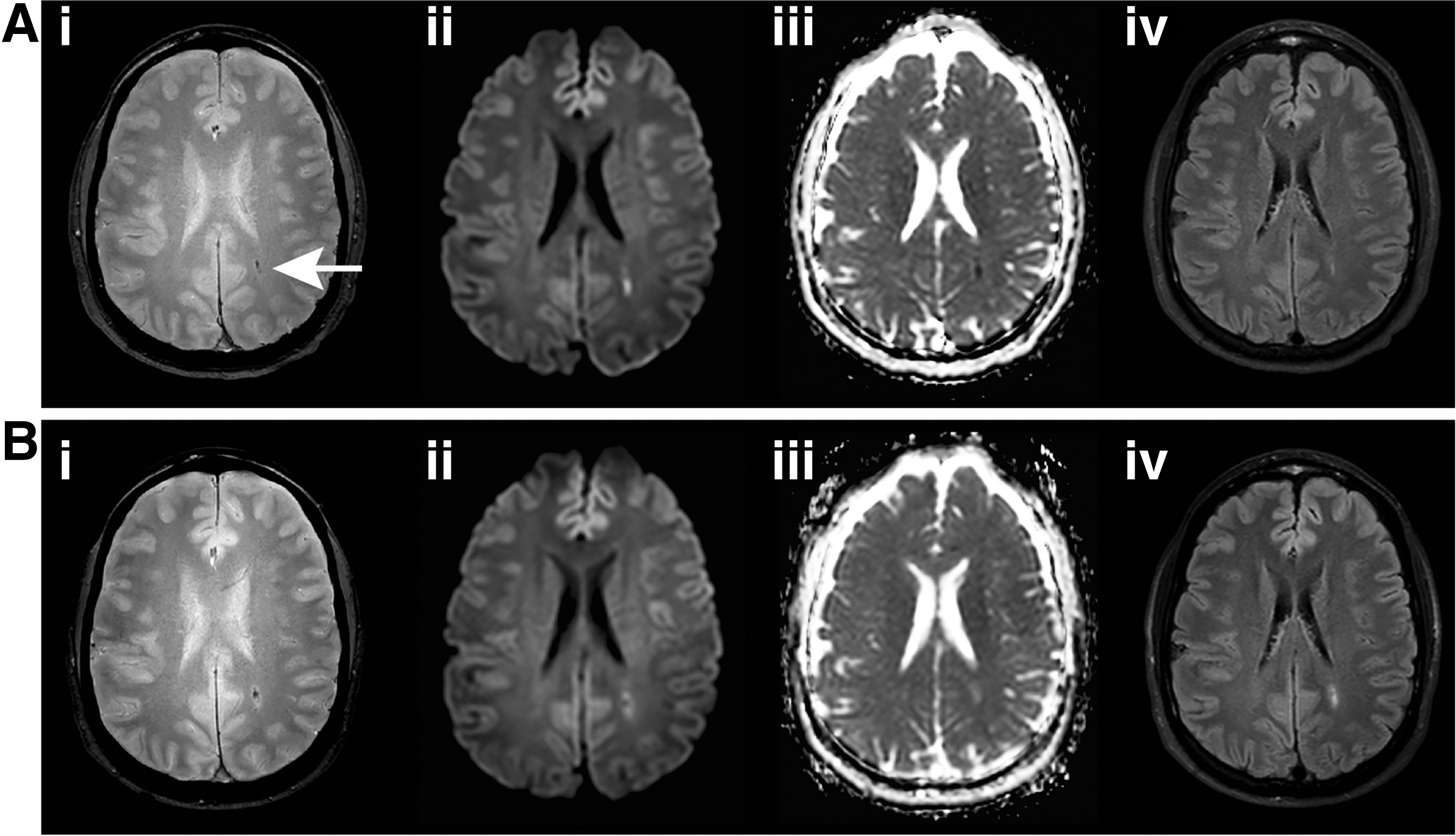
Representative example of the evolution of magnetic resonance imaging findings associated with a traumatic microbleed from acute presentation to follow-up. (
Of 54 patients identified as having DWI lesions associated with TMBs, two were excluded from quantitative analysis because of motion artifact. Values of ADC were not normally distributed. The median ADC value at baseline for all volumes of interest (VOIs) was 0.77 (0.68–0.83), significantly lower than the ADC value at follow-up 0.82 (0.76–0.93), p < 0.001. Values of ADC from reference VOIs in deep gray matter were similar between time points (p = 0.98). ADC values for all VOIs stratified by hemorrhagic lesion type did not differ from each other at baseline, but significantly increased over time (Fig. 4A).

Quantification of apparent diffusion coefficient (ADC) of water for all lesion types.
Lesions with lower ADC values at baseline, suggesting cytotoxic edema, had increased ADC values at follow-up (Fig. 4B). The ADC values for all TMB-associated VOIs were averaged per subject and plotted along with reference VOIs against time from injury to imaging for both baseline and follow-up (Fig. 5A). The per patient average ADC value of DWI hyperintense TMBs imaged within 24 h was 0.70 (0.65–0.80), which was significantly lower than those obtained between 24–72 h, 0.83 (0.79–0.90), p < 0.001, and those after 72 h, 0.82 (0.79–0.84), p < 0.001 (Fig. 5B). Lesion ADC values did not differ between 24–72 hour and >72 h groupings (p = 0.801).
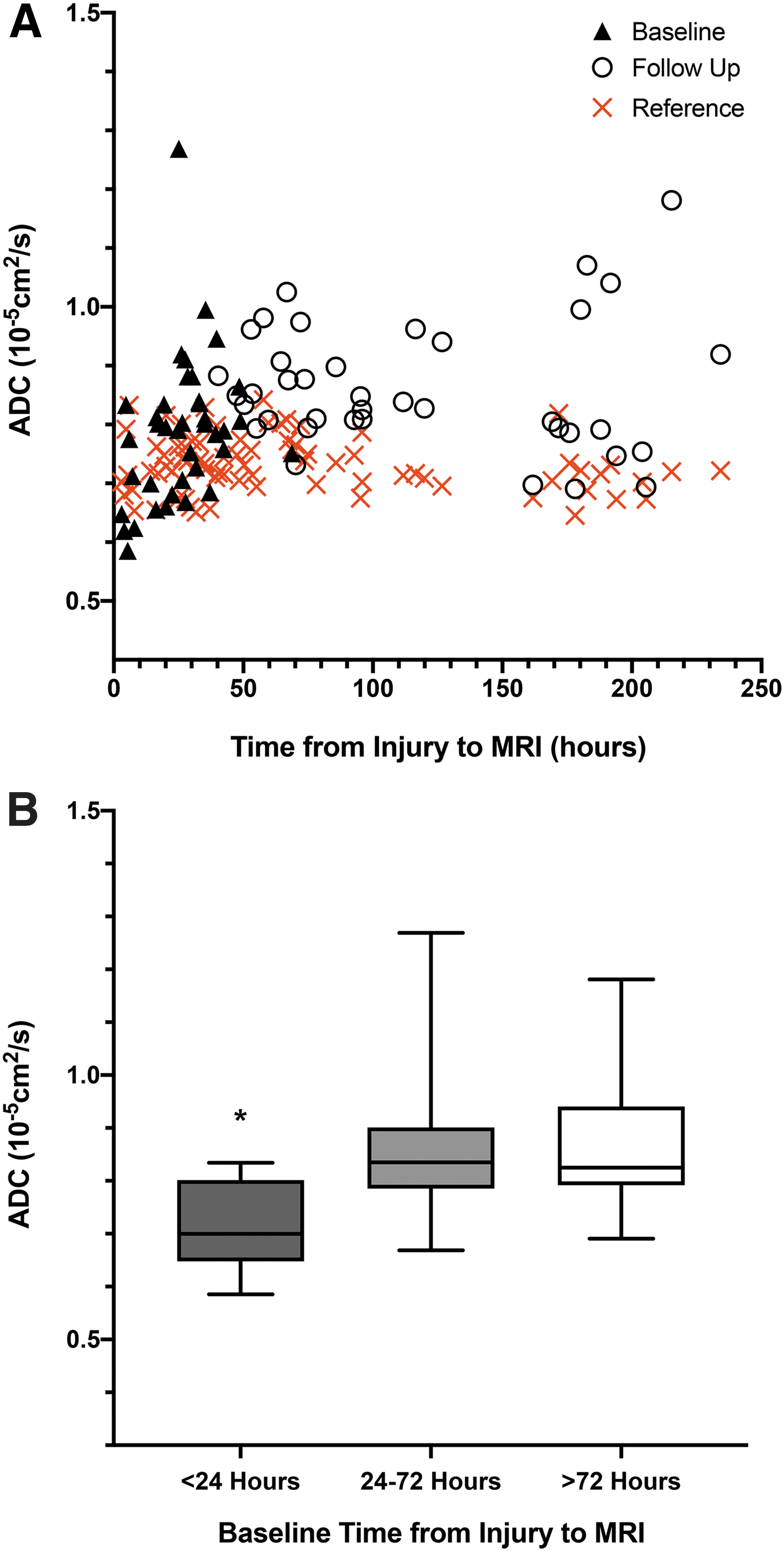
Quantification of apparent diffusion coefficient (ADC) of water for lesions in proximity to traumatic microbleeds. (
Cytotoxic edema: predictors and clinical outcome
Table 1 is stratified by the presence or absence of cytotoxic edema, regardless of association with hemorrhagic lesions. Univariate predictors of cytotoxic edema included GCS score, documented loss of consciousness, and hemorrhagic findings on CT and MRI, but not baseline TBI severity, even for the mild TBI population (Supplementary Table 1).
Clinical outcome assessed by GOSE was available for 118 (73%) patients (19 with 30-day only, 16 with 90-day only, 83 with both), with approximately half having some degree of disability (GOSE score ≤6). The univariate predictors of outcome trauma center level, TBI severity, presence of TMB or intraparenchymal hematoma/contusion on MRI, DWI hyperintensity, and ADC hypointensity were associated with disability (Table 2).
Predictors of Clinical Outcome at 30 or 90 Days
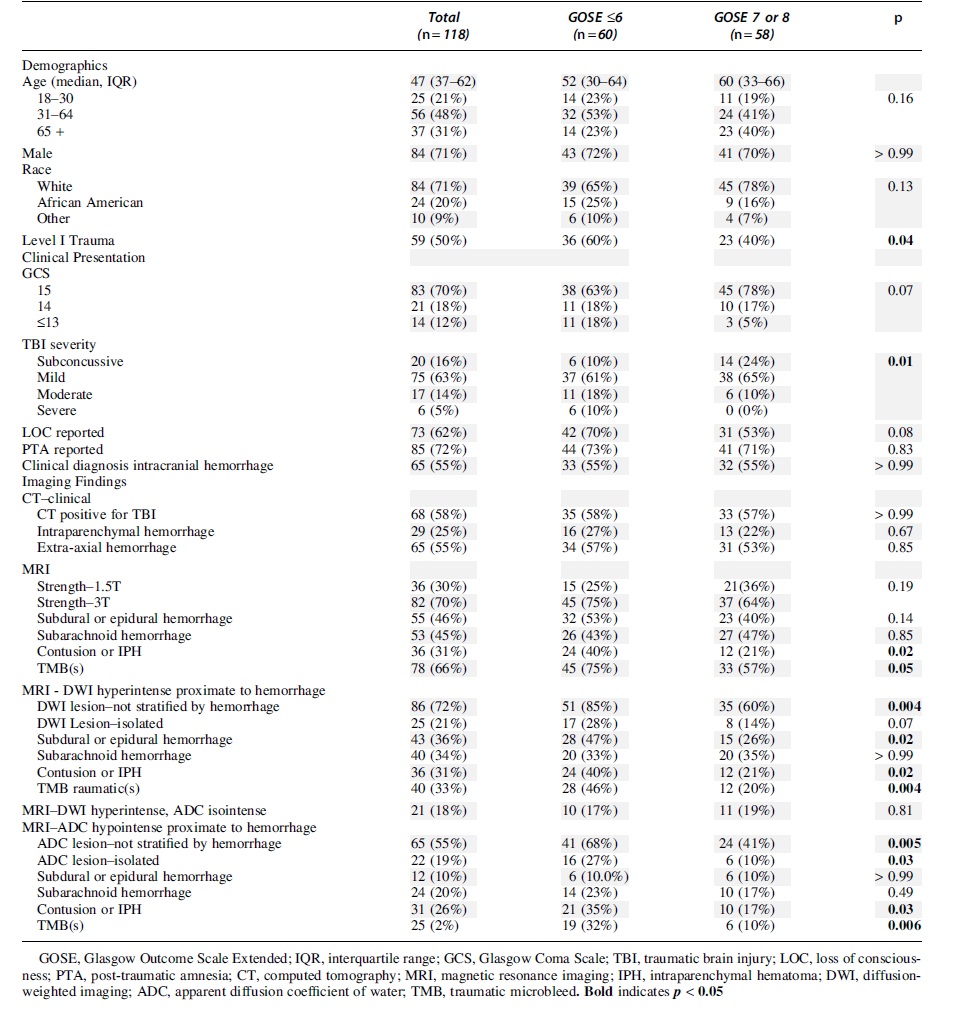
Acute findings on CT and MRI field strength were not associated with outcome. The MRI findings, specifically TMBs and DWI hyperintensity and ADC hypointensity associated with TMBs, were predictors for the mild TBI population (Supplementary Table 2). In a stepwise logistic regression that considered trauma center level, TBI severity, evidence of intraparenchymal hemorrhage/contusion or TMBs, cytotoxic edema seen on MRI, and ADC hypointensity, only TBI severity (OR 2.51 [1.32–4.74], p = 0.005) and cytotoxic edema (OR 2.91 [1.32–6.37], p = 0.008) were independently associated with outcome.
At presentation to the emergency department, 41% (66/161) patients were documented as having polytrauma, with no significant differences in the outcome of cytotoxic edema between those with and without polytrauma (p = 0.084). There were no significant differences in GOSE outcomes between those with and without polytrauma, whether the effects were attributed to head injury alone (p = 0.819), illness or injury to other parts of the body (p = 0.522), or to a mixture of head injury and other (p = 0.219). Two patients in the study had cranial surgery (one with hemicraniectomy before acute MRI, and another with cranial burr holes after acute MRI), with one reporting a GOSE score ≤6 and the other reporting GOSE score >6 at this study's end point.
Discussion
We present evidence of cytotoxic edema in clinically mild patients imaged early after head trauma. Lesions appearing as focal hyperintensities on DWI were found in isolation, but more commonly near areas of hemorrhage seen on T2* MRI, including TMBs. Approximately two-thirds of patients with hyperintense lesions on DWI had corresponding regions of ADC hypointensity, similar to findings seen in acute stroke.
Quantitative analysis of ADC values demonstrated a temporal evolution from low values (visually identifiable as hypointensity) early after injury to elevated values at follow-up, suggesting evolution from cytotoxic to vasogenic edema. Patients with evidence of cytotoxic edema, regardless of the strata of hemorrhagic lesion, were more likely to have residual disability in subsequent months. Collectively, the data suggest that primary traumatic injury to cerebral vasculature can be associated with cytotoxic edema and poor outcome.
During initial enrollment in this protocol, small lesions with DWI hyperintensity and corresponding ADC hypointensity were observed in clinically mild trauma patients with negative CT. These radiological findings were initially interpreted as suggestive either of ischemic stroke or diffuse axonal injury (DAI), 15 –19 resulting in further clinical subspecialty consultation. As cases accumulated, many of these DWI lesions were seen in proximity to hemorrhagic lesions, but the clinical relevance of this observation in clinically mild patients with TBI remained unclear. The current analysis suggests that when DWI hyperintense/ADC hypointense lesions are seen on MRI early after injury, the patient is at greater risk of incomplete recovery.
The mechanism behind these DWI/ADC changes remains speculative at this point and may be multi-factorial. As part of our quantitative analysis, we investigated TMBs in particular, which have become known to signify traumatic vascular injury, serving as distinct lesions where mechanical forces to vessels can result in vascular injury and extravasation of blood into the perivascular space and parenchyma. 13,14
Cytotoxic edema detected in proximity to TMBs could reflect any of the following: focal ischemia from interruption in blood flow, anoxic depolarization as a cascade initiated by the presence of blood and free radicals in direct contact with the neuropil, direct traumatic disruption to cellular/axonal elements, or a combination of these mechanisms. A recent positron emission tomography study of cerebral physiology in moderate/severe TBI observed cerebral ischemia in structurally normal tissue in two-thirds of patients within the first 24 h. 20 Perihematomal ischemia and edema are often observed in primary IPH 21 or contusion. 22
Hemorrhagic lesions after TBI, however, may reside on a continuum of severity. Even relatively discrete lesions such as TMBs can be associated with parenchymal edema.
Direct mechanical injury to parenchyma may result in lesions on DWI MRI. Traditionally, TMBs have been linked with DAI, 15 –19 a hallmark of TBI across injury severities and a significant predictor of outcome. 23 –25 The DAI may result from shearing forces at the moment of injury, causing extensive damage to neurons, glia, and blood vessels and ultimately resulting in neurologic deficits. 26,27
Recent studies call into question whether TMBs are always associated with axonal injury. Across injury severity, TMBs that appear punctate in the axial plane are often revealed as linear structures that may be specific to TBI. 13 We demonstrated that acute TMBs correspond with post-mortem pathological features consistent with secondary injury surrounding injured vessels, but not with traditional markers of DAI. 14 Other MRI studies have reported limited colocalization of TMBs with diffusion evidence of axonal injury in TBI. 28,29
In the region adjacent to TMBs, we observed hyperintense DWI signal colocalizing with ADC hypointensity during the acute period, which can be characteristic of failures of energy-dependent processes and ischemic tissue. At follow-up, nearly 70% of these TMBs had increased normalized ADC values. Lesions with the lowest ADC values at baseline also had larger changes in ADC values between baseline and follow-up. The increase in ADC surrounding TMBs was similar to the increases seen with IPH and subarachnoid hemorrhage (SAH). In IPH and SAH, extravasated blood triggers secondary injury through a cascade of endothelial swelling, vasospasm, vasoconstriction, and evolution toward vasogenic edema in the subacute phase of injury. 22,30,31
Our results indicate that primary traumatic vascular injury can be associated with cytotoxic edema evolving over time into vasogenic edema. While further investigation is needed to determine the underlying mechanisms of these changes, the patterns of ADC evolution appear strikingly similar to the changes seen on acute and subacute MRI in ischemic stroke.
The ability to detect ADC hypointense (i.e., cytotoxic) lesions after TBI also depends on the timing of acute MRI. The earliest scans detected VOIs with the lowest ADC values, consistent with the hypothesis that cytotoxic edema predominates in these VOIs acutely after injury, while vasogenic edema becomes more prevalent with time. This reinforces the importance of obtaining acute and follow-up scans after injury and has implications for therapeutic interventions targeting the vasculature. Cytotoxic edema early after injury typically results in irreversible cell death unless energy substrates can be restored. Conversely, vasogenic edema is, in principle, reversible when detected early enough to administer treatments to restore blood–brain barrier function and integrity. Left untreated, however, cytotoxic edema may lead to secondary injury and cell death.
Previous studies of diffusion-related changes in TBI were conducted in both animal models and humans, with conflicting results. Animal models showed both overall increases 32 and decreases 33 in ADC acutely after injury, while other studies reported a progressive decrease from the acute to subacute period. 34 Early studies of DWI MRI in human TBI attributed decreased ADC values between one and 18 days post-injury 16 and reduced white matter diffusion anisotropy within 24 h of injury 35 to DAI.
Another investigation of early (<14 day) DWI lesions in the context of DAI found a mixture of lesions that could be differentiated as either increased or decreased diffusion, reflecting vasogenic and cytotoxic edema, respectively. 36 A group classifying lesion load as either vasogenic or cytotoxic found that both edema types were associated with poor outcome, despite more severe injury in those with predominantly cytotoxic edema, and saw both cytotoxic and vasogenic lesions in the corpus collosum, an area susceptible to DAI. 37 An early serial MRI study and a case report suggest an association between temporal resolution of edema-associated DAI lesions of the corpus callosum and better outcomes. 38,39
Several studies examined whole-brain and regional ADC values as predictors of outcome after TBI. Whole-brain ADC values on MRI at 1–23 days post-injury significantly correlated with admission GCS scores, 40 while others reported significant correlations between injury severity and ADC values of normal-appearing white matter. 41 Another group reported lower ADC values in deep white and gray matter in patients with unfavorable outcome compared with those with favorable outcome, with all regions except peripheral gray matter showing an increase in ADC relative to controls. 42
In contrast, pediatric TBI studies reported reduced ADC values in peripheral white matter predicted poor outcome in severe TBI, while deep white matter ADC values were reduced relative to controls. 43 Paradoxically, a subset of this pediatric population excluding the most severely injured patients demonstrated that increased ADC values in peripheral white and gray matter predicted worse long-term neurocognitive outcomes. 44 Although maturational changes might complicate interpretation of diffusion-related MRI outcomes between adults and children, these divergent findings highlight the difficulty of using early ADC values to predict outcome in TBI.
The TRACK-TBI study reported that contusion and hemorrhagic axonal injury 45 and decreases in fractional anisotropy 46 on MRI at two weeks after injury predict poorer GOSE scores at three months post-injury. Our finding that hemorrhage-associated cytotoxic edema on acute MRI predicts outcome is consistent with those results and suggests there may be therapeutic targets for intervention. Once the biological mechanisms are better understood, future targeted therapies could be administered to those patients presenting with acute hemorrhage and diffusion changes.
Approximately 50% of those presenting to two civilian emergency departments with criteria for mild TBI were not initially recognized as having TBI. 47 While in sports and the military implementation of standard screening protocols has improved identification of patients, in the general population even many of those recognized as having mild TBI with ongoing symptoms do not receive appropriate education and follow-up care. 48 This lack of early identification and education, except in the most severely impaired, may contribute to worse outcomes. 49
Patients found to have small amounts of hemorrhage on CT are more likely to have worse outcome (defined by GOSE) if evidence of diffusion changes are found on MRI. This prognostic value, in itself, may provide evidence needed to support the clinical utility of MRI in select patients. In the present study, TMBs were the most common finding seen on acute MRI that was not detected on acute CT. This, combined with our previous work demonstrating poorer outcomes in patients with TMBs, 14 suggests that acute MRI may be warranted to screen for microbleeds in CT negative patients, although additional research is needed. Further, there may be targeted therapies that could, one day, be applied to reduce the risk of edema, or, at a minimum, to flag these patients as being potentially in need of early education, connection with outpatient care, and possibly ongoing follow-up to assess their need for rehabilitation services.
In this study, we examined ADC changes in conspicuous DWI lesions during initial hospitalization as opposed to during a subsequent outpatient visit. This allowed us to confirm that: (i) acute ADC values can be used to predict outcome, and (ii) acute cytotoxic edema associated with lesions such as TMB and IPH may contribute to poor outcome. We also characterized the temporal evolution of ADC values associated with hemorrhage by comparing baseline and follow-up MRI, demonstrating a pattern of ADC evolution that indicates lesion evolution between the acute and subacute periods.
Limitations
Our findings must be interpreted in comparison with the literature by considering the time course of MRI used in the present study, with a median time to baseline MRI of 21 h far earlier than previously described studies, possibly accounting for the ADC evolution differences. There is also the potential for selection bias in our patient cohort, with patients being more likely to return for follow-up visits if they had clinical findings or symptoms.
Cranial surgery was not an exclusion criterion for this study and may have affected outcomes, although GOSE outcomes were split for the two patients who underwent cranial surgery during their acute visits. Patients with polytrauma were included in this dataset and outcomes analysis, and an association between polytrauma and poorer GOSE outcomes has been reported previously. 50 In the present study, patients were asked to attribute their GOSE answers in the context of their head injury, but difficulties in their doing so may have confounded results.
Whether MRI is quantifiably superior to CT for the detection of TBI-related lesions such as contusions and TMBs is not directly addressed in the present study and is the focus of ongoing research. Additional studies of patients with acute MRI with larger sample sizes are needed to confirm and extend these findings. Further investigation is also required to determine which of the potential underlying biological mechanisms are causing these acute ADC changes.
Conclusion
An emerging body of literature indicates that traumatic vascular injury is associated with chronic pathophysiological processes and poor neurological outcome. The current study, by identifying acute injury processes associated with intracranial hemorrhage on clinically relevant in vivo acute and subacute MRI, supports the hypothesis that traumatic vascular injury is a key contributor to the pathogenesis of TBI.
Footnotes
Acknowledgments
We would like to thank our patients and their families for their willingness to participate in clinical research. We are also grateful for the clinical and administrative teams who have supported the THINC study.
Authors' Contributions
L.C.T., M.L, R.P.H.B., G.P., and L.L.L. contributed to the study conceptualization and design. N.J, A.G., and D.G. participated in the data collection. L.C.T., R.P.H.B., G.P., and L.L.L. provided neurological and/or neuroimaging expertise. L.C.T., M.L., N.J., A.G., D.G., N.P., and L.L.L. analyzed and interpreted the data. L.C.T., M.L., N.J., D.G., N.P, M.W., and L.L.L. drafted the manuscript and/or figures. All authors critically revised the manuscript.
Funding Information
Funding for this work was provided by Intramural Research Program of the National Institute of Neurological Disorders and Stroke, National Institutes of Health, and by the Department of Defense through the Center for Neuroscience and Regenerative Medicine.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Methods
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.