
Abstract
Traumatic brain injury (TBI) is a major clinical and public health problem with few therapeutic interventions successfully translated to the clinic. Identifying imaging-based biomarkers characterizing injury severity and predicting long-term functional and cognitive outcomes in TBI patients is crucial for treatment. TBI results in white matter (WM) injuries, which can be detected using diffusion tensor imaging (DTI). Trauma-induced pathologies lead to accumulation of free water (FW) in brain tissue, and standard DTI is susceptible to the confounding effects of FW. In this study, we applied FW DTI to estimate free water volume fraction (FW-VF) in patients with moderate-to-severe TBI and demonstrated its association with injury severity and long-term outcomes. DTI scans and neuropsychological assessments were obtained longitudinally at 3, 6, and 12 months post-injury for 34 patients and once in 35 matched healthy controls. We observed significantly elevated FW-VF in 85 of 90 WM regions in patients compared to healthy controls (p < 0.05). We then presented a patient-specific summary score of WM regions derived using Mahalanobis distance. We observed that MVF at 3 months significantly predicted functional outcome (p = 0.008), executive function (p = 0.005), and processing speed (p = 0.01) measured at 12 months and was significantly correlated with injury severity (p < 0.001). Our findings are an important step toward implementing MVF as a biomarker for personalized therapy and rehabilitation planning for TBI patients.
Introduction
Traumatic brain injury (TBI) is one of the leading causes of death and disability around the world, 1 frequently requiring long-term medical care and intensive rehabilitation. 2 The pathogenesis of TBI is complex and the impact of injury evolves over a period of time, frequently leading to long-term functional and cognitive deficits. 3,4 Predicting outcome in TBI is challenging because of its inherent heterogeneity, rooted in cause, pathology, and etiology. 5,6 Therefore, there is a need to identify biomarkers to assist clinicians in evaluating the severity of injury as well as outcomes that will help clinical investigations and guide targeted therapeutics customized to patients.
TBI results in both focal and diffuse injury to brain tissues. 7 Focal injuries result when the surface of the brain impacts bony protuberances of the skull, resulting in hemorrhage and contusion. These injuries are usually macroscopic and are identifiable on routine neuroimaging techniques such as computerized tomography (CT) or magnetic resonance imaging (MRI). 8 Diffuse injuries are caused by inertial rotational or shearing forces that cause rapid acceleration, deceleration, and rotational head motions, leading to axonal damage, 9 predominant in deep white matter (WM) structures. In the first few days after TBI, vasogenic and cytotoxic edema 10 from either focal or diffuse injuries can result in elevated intracranial pressure (ICP), cisternal effacement, and herniation, which can be lethal or result in severe disability. 11 –13 In the chronic phase of injury, diffuse WM injury induces distinct pathological features like blood–brain barrier (BBB) disruption, microvasculopathy, and chronic inflammation, leading to accumulation of free water (FW) in brain tissue. 14 –16 Elevated water content of the brain in TBI has long been associated with unfavorable outcome. 13
Diffusion tensor imaging (DTI), which models WM microstructure based on the diffusion of water molecules, has been widely used to characterize diffuse WM injury in TBI patients. 17 However, widely used DTI measures, such as fractional anisotropy (FA) and mean diffusivity (MD), are often difficult to interpret, because of the complex interplay between vasogenic and cytotoxic edema affecting these measures. 10 Most studies have reported increased MD and reduced FA in TBI patients, 17 but these measures are sensitive to multiple physiological processes that occur in WM injury and do not specifically address the FW content of tissue. 18 FW imaging is a method to estimate the FW present in the brain as a free water volume fraction (FW-VF) map, especially in the presence of pathology. 19,20 These methods compartmentalize the diffusion signal into a tensor describing WM tissue and an isotropic compartment which describes FW, such as in cerebrospinal fluid or edema, where fluid accumulates in the extracellular space. 19
In TBI, FW-VF may represent subtle degrees of vasogenic edema, chronic neuroinflammation, gliosis, and BBB disruption, depending on the stage of injury. Thus, investigating FW-VF in TBI and its association to injury severity and long-term outcomes is expected to provide insight into the underlying pathology, but has never been explored before in moderate-to-severe TBI. Moreover, the presence of FW obscures standard measures, such as FA and MD, which may explain the mixed findings with regard to group-based investigations in TBI. 18,21 Finally, the clinical meaningfulness can only be established if a patient-specific summary score of these measures is indicative of injury severity and outcome. Mahalanobis distance, a multi-variate analysis approach, 22 has been previously used as a summary score to discriminate patients with mild TBI and controls and correlating with cognitive measures. 23
In this study, we define a patient-specific summary score for each patient, derived from their FW-VF. We hypothesize that: 1) VF will be elevated in TBI patients and 2) patient-specific summary score of FW-VF will predict functional and cognitive outcomes in patients and will correlate with injury severity. In subsequent exploratory analysis, we investigate whether: 1) patient-specific summary scores derived from standard FA, MD, and FW-estimated FA have the same association with injury severity and prediction of outcome as that of VF and 2) patient-specific summary scores of FW-VF, FW-estimated FA, and standard FA and MD change over the 1 year post-injury.
Methods
Participants
Forty-two patients with moderate-to-severe TBI were recruited from the outpatient clinical programs at the Drucker Brain Injury Center of the MossRehab Hospital from 2012 to 2016 for MRI scanning and neuropsychological evaluations 3, 6, and 12 months after their injuries. Inclusion criteria were age between 18 and 64 years and a diagnosis of non-penetrating moderate-to-severe TBI, as defined by at least one of the following: 1) Glasgow Coma Scale score <13 in the emergency department; 2) loss of consciousness ≥12 h; or 3) prospectively documented post-traumatic amnesia (PTA) ≥24 h. To ensure that TBI was predominantly diffuse, participants were excluded if the total estimated volume of focal intraparenchymal lesions on acute MRI or CT exceeded 5 cm3 for subcortical lesions and 50 cm3 for cortical lesions. One patient underwent a craniotomy and was excluded from the study. Patients with hypoxic injury were also excluded. Additionally, 7 patients were excluded after data quality-control (QC) procedures, because of low MR image quality from excessive motion and/or flow artifacts during scanning. As a result, the final analysis included data from 34 TBI patients at 3 months; 28 and 27 of these also had QC-approved data at 6 and 12 months, respectively. Thirty-five healthy controls matched for age, years of education, and sex with good general health and no known neurocognitive disorders were also recruited. Informed consent was obtained from all participants or their legally authorized representative.
Clinical measures
Clinical measures were collected from medical records or measured prospectively during hospitalization. Duration of PTA was calculated as the number of days between TBI and the first of two occasions within 72 h that the participant was fully oriented. Full orientation was defined as a score above 25 on the Orientation Log 24 or documentation of consistent orientation for 72 h in the acute medical record (i.e., before rehabilitation admission). PTA was selected as the injury severity measure because PTA has been shown to be a superior predictor of TBI outcome. 25 Functional outcomes were determined 3, 6, and 12 months after injury using the Glasgow Outcome Scale-Extended (GOSE), 24 a measure that is commonly used as a global assessment of functional abilities in multiple domains after a TBI 26 Neuropsychological tests were performed 3, 6, and 12 months after injury across three domains: mental processing speed (PS) as indexed by the Processing Speed Index from the Wechsler Adult Intelligence Scale IV 27 ; verbal learning (VL) administered by Rey Auditory Verbal Learning Test (RAVLT) 28 ; and executive functioning (EF) as indexed by a composite measure consisting of an average across T-scores of the following five tests 29 : the Trail Making Test-Part B 30 ; the Color Word section of the Color Word Interference Test 31 ; the Controlled Oral Word Association Test 32 ; the Letter-Number Sequencing subtest; and the Digits Backward section of the Digit Span subtest of the Wechsler Memory Scale IV. 33
Image acquisition
Both patients and healthy controls underwent brain MRI on a Siemens 3T Tim Trio scanner (Siemens, Erlangen, Germany), with patients scanned at 3, 6, and 12 months post-injury. The DTI protocol included two identical acquisitions of 30 gradient directions at a b-value of 1000 s/mm2, with seven b0 images spaced throughout the acquisition (voxel size = 2.18 × 2.18 × 2.20 mm, echo time [TE] = 84 ms, repetition time [TR] = 6500 ms, flip angle = 90 degrees). A structural magnetization-prepared rapid gradient echo sequence was also acquired (voxel size = 1 × 1 × 1 mm, TE = 3.08 sec, TR = 1620 ms, flip angle = 15 degrees).
Image processing
All T1 and DTI data were manually inspected for artifacts before pre-processing. T1-weighted images were bias corrected using the N4BiasCorrection tool from ANTs, 34 followed by brain extraction using a multi-atlas segmentation tool, MUSE. 35 DTIs were concatenated and pre-processed in three steps: 1) Local-PCA Denoising 36 implemented in MATLAB (The MathWorks, Inc., Natick, MA); 2) motion and distortion correction through “eddy” from the FMRIB Software Library 37 ; and 3) bias field correction using N4BiasCorrection. A tensor model was fit to the data 38 in DIPY, 39 and standard fractional anisotropy (FA) and mean diffusivity (MD) were derived.
We used FERNET (Freewater EstimatoR using iNtErpolated iniTialization), 19 a recent method for FW correction in clinically acquired DTI data, to estimate the FW-VF and FW-corrected FA (fernet-fit FA or ff-FA). The code used to apply FERNET on DTI data is available online. 40 Using the deformable SyN registration algorithm of ANTs, 41 the data were registered to the JHU-MNI-ss (Eve) template. 42 Median values of each scalar were calculated in 90 regions of the Eve WM parcellation. Cerebellum was excluded from analysis because the acquisition did not include it in all scans. Fornix and tapetum regions were also excluded because of their small size and proximity to the ventricles.
Patient-specific summary score of free water volume fraction and other diffusion measures
We utilized Mahalanobis distance (M), a multi-variate generalization of the z-score which incorporates the covariance between the variables, as a summary measure of DTI measures. 23 M was calculated for each of the four DTI scalars (denoted MVF, Mff-FA, Mstd-FA, and Mstd-MD henceforth), using the following formula:

where s = [Xr 1, Xr 2… Xr 90] is the vector of DTI measures in each WM region in a single participant, where Xr i represents the residuals of age-regressed-out DTI measures (VF, ff-FA, std-FA, or std-MD) in region i for a participant; μ is the vector of mean Xr of each WM region in a healthy control population; and C is the covariance matrix between WM regions across the control population. To compute the covariance, 25 controls were randomly selected and permuted 1000 times. M of patients was calculated individually relative to each of the 1000 control distributions, for each DTI measure, and the median values are reported.
Statistical analysis
To test the primary hypothesis that FW-VF would be elevated in patients, we performed ordinary least squares (OLS) regression on the average FW-VF for 90 ROIs with terms for group, age, and sex. Group differences were assessed as t-statistics and associated p values of the regression. Results were corrected for multiple comparisons at the p < 0.05 level using the Benjamini-Hochberg procedure. 43 The same regression was used to assess group differences in ff-FA, std-FA, and std-MD between patients and healthy controls.
To test the second hypothesis that MVF could predict functional and cognitive outcomes at 12 months post-injury and its association with injury severity, OLS regression was used with terms for MVF, age, and sex. Dependent variables were PTA, GOSE, and cognitive scores (EF, VL, and PS). Significance for these comparisons was set at p = 0.01 (0.05/5) after Bonferroni correction for five comparisons.
For the exploratory analyses, we compared Mff-FA, Mstd-FA, and Mstd-MD in predicting functional and cognitive outcomes at 12 months post-injury and their associations with injury severity, using the same regression adjusted for age and sex. Longitudinal variations in MVF, Mff-FA, Mstd-FA, and Mstd-MD from 3, 6, and 12 months were assessed using a linear mixed-effects regression model controlling for age and sex. Group effects in demographics and neuropsychological functions were tested using an independent-sample t-test. These tests were assessed at the uncorrected p < 0.05 level.
Linear mixed-effects models were fitted using the R package, lme4 1.1-26, in R 1.3.1093 (The R Foundation for Statistical Computing, Vienna, Austria). OLS analyses were performed with statsmodels 0.9.0 in python 3.6.8. 44
Results
Demographics and clinical characteristics of the TBI and control groups are summarized in Table 1. There were no significant demographic differences between groups. At 3 months post-injury, patients exhibited significantly poorer performance in EF, PS, and VL than controls; VL was impaired relative to healthy controls at 6 months post-injury, and by 12 months post-injury, no significant differences in neuropsychological performance between groups were noted (Table 2).
Demographic and Clinical Characteristics of the Sample
Based on 25 patients, 9 patients did not show any macroscopic focal lesion.
Based on 25 patients, 2 patients were intubated, and 7 patients were on sedation.
Based on 33 patients, information was unavailable for 1 patient. N represents the number of patients showing that type of injury.
PTA, post-traumatic amnesia duration; GCS, Glasgow Coma Scale; GOSE, Glasgow Outcome Scale–Extended; CT, computerized tomography; N, number of subjects; SD, standard deviation; TBI, traumatic brain injury.
Performance Scores of Neuropsychological Tests
Significant differences between TBI patients and control subjects are indicated.
p < 0.05, uncorrected for multiple comparisons.
EF, executive function; PS, processing speed; VL, verbal learning; SD, standard deviation; TBI, traumatic brain injury.
Regional differences between patients and healthy controls
Eighty-four out of 90 WM regions were found to have significantly elevated FW-VF in patients 3 months post-injury compared to healthy controls (Fig. 1; see Supplementary Table S1). Fernet-fit FA was decreased in 46 WM regions and increased in one WM region in patients (Supplementary Fig. S1A; see Supplementary Table S2). Standard FA was reduced in 64 WM regions (Supplementary Fig. S1B; see Supplementary Table S3), and standard MD was increased in 68 WM regions (Supplementary Fig. S1C; see Supplementary Table S4) in patients.
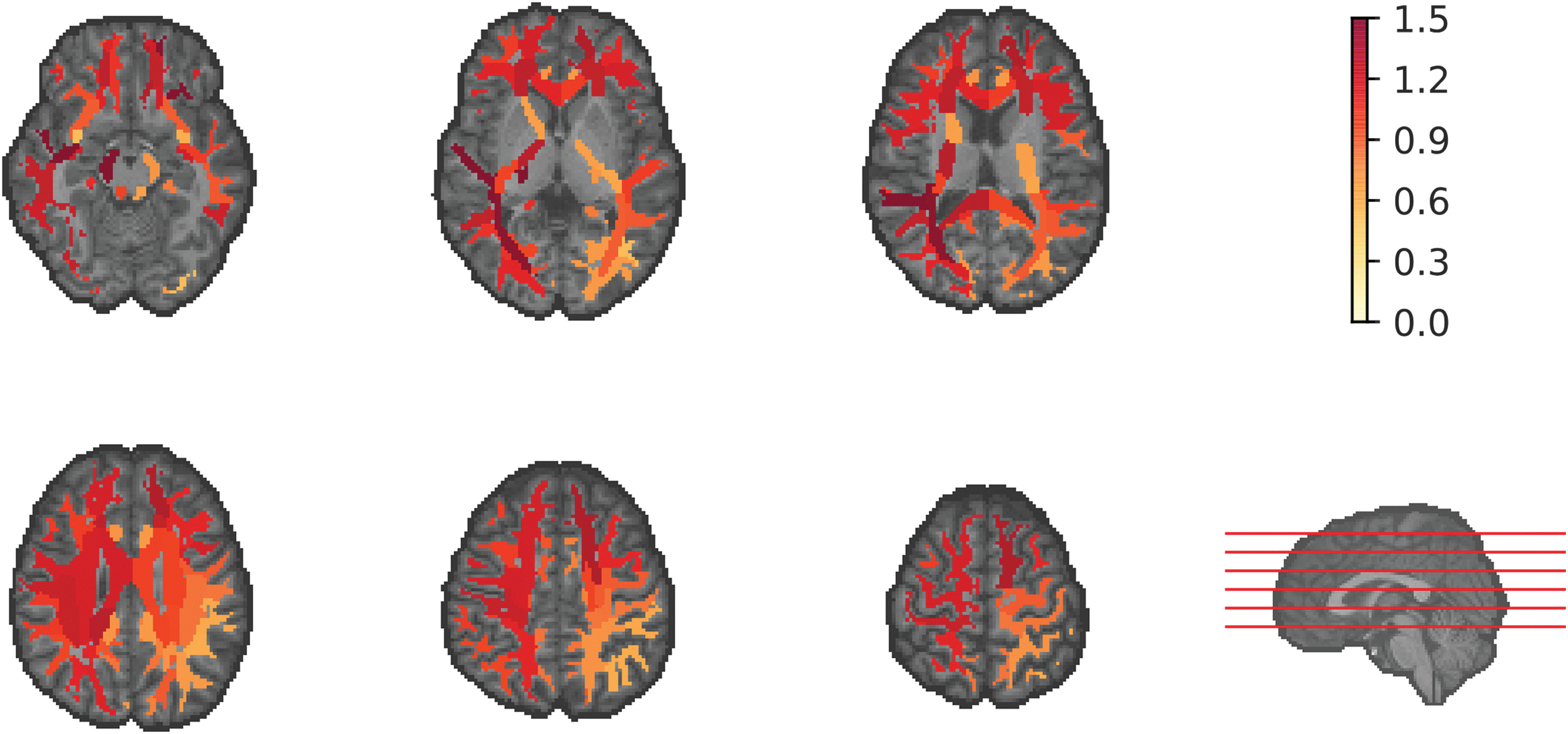
Elevated free water volume fraction observed across many white matter regions in patients with moderate-to-severe TBI (n = 34) compared to age-, years of education–, and sex-matched healthy controls (n = 35) after correcting for age and sex. Group differences are overlaid on the JHU-MNI-ss (Eve) template T1-weighted image. Locations of displayed axial slices are shown by red lines on the template brain at bottom right. The color map represents the effect size (Cohen's d). TBI, traumatic brain injury.
Outcome prediction analysis by patient-specific summary scores
MVF significantly predicted GOSE (β = −0.55; p = 0.008), EF (β = −0.64; p = 0.005), and PS (β = −0.55; p = 0.01), measured at 12 months, and was significantly correlated with PTA (β = 0.64; p < 0.001). However, MVF did not predict VL (β = −0.40; p = 0.11; Table 3).
Linear Regression Model Analysis of MVF, Mff-FA, Mstd-FA, and Mstd-MD Predicting Functional, Cognitive, and Injury Severity
p values <0.01 after Bonferroni correction for five dependent variables.
p values <0.05, uncorrected for multiple comparisons.
GOSE, Glasgow Outcome Score-Extended; EF, executive function; PS, processing speed; VL, verbal learning; PTA, post-traumatic amnesia duration; CI, confidence interval; MVF, Mahalanobis distance of free water volume fraction; Mff-FA, Mahalanobis distance of FERNET fit fractional anisotropy; Mstd-FA, Mahalanobis distance of standard fit fractional anisotropy; Mstd-MD, Mahalanobis distance of standard fit mean diffusivity.
Mff-FA predicted EF (β = −0.42; p = 0.03) at 12 months and was correlated with PTA (β = 0.52; p = 0.002). Mstd-FA was observed to correlate with PTA (β = 0.46; p = 0.007), but it did not predict functional or cognitive outcomes with statistical significance. Mstd-MD significantly predicted EF (β = −0.57; p = 0.008) and PS (β = −0.48; p = 0.02) and was correlated with PTA (β = 0.62; p < 0.001). Mff-FA, Mstd-FA, and Mstd-MD did not predict GOSE or VL (Table 3).
Longitudinal analysis of patient-specific summary scores
Longitudinal analyses from 3, 6, and 12 months post-injury revealed a significant increase in MVF over a period of 1 year (β = 0.14; t = 2.51; p = 0.01) as shown in Figure 2. Mff-FA decreased over a period of 1 year (β = −0.11; t = −3.30; p = 0.002), but not Mstd-FA (β = 0.001; t = 0.04; p = 0.97). The Mstd-MD increased with time (β = 0.16; t = 2.92; p = 0.005; Supplementary Table S5; Supplementary Fig. S2).

Longitudinal plot showing the changes in the patient-specific summary score of VF (MVF) from 3, 6, and 12 months post-injury. MVF, Mahalanobis distance of Free water volume fraction; VF, volume fraction.
Discussion
In the present study, we first demonstrated a widespread increase in FW-VF in most WM regions 3 months after moderate-to-severe TBI. We then presented a patient-specific summary score of FW-VF, MVF derived at 3 months post-injury which predicted functional outcome (GOSE) and cognitive outcomes (EF and PS) at 12 months post-injury and correlated with injury severity (PTA). To the best of our knowledge, the present study is the first to apply FW estimation in patients with moderate-to-severe TBI and develop a patient-specific summary score of FW-VF to characterize injury severity and predict functional and cognitive outcomes.
After brain injury, inflammatory responses caused by microglial and astrocytic reactivity, formation of vasogenic edema attributable to disruption in BBB, neuronal cell death, axonal swelling, and disconnection are known to continue for months to years. 14,45,46 Moreover, post-mortem and neuroimaging studies have demonstrated extensive WM volume loss, 47 –49 which can increase the interstitial spaces. These processes increase fluid content in the brain, making FW-VF a prime candidate for quantifying these phenomena. We observed increased FW-VF in widespread WM regions, suggesting increased extracellular water driven by pathologies, such as atrophy, inflammation, or cellular changes, that persisted 3 months post-injury. Our finding is in agreement with previous FW DTI studies that reported elevated FW as an indicator of neuroinflammation, cerebral edema, or atrophy in various brain disorders. 50 –54
We used a multi-variate statistic, Mahalanobis distance (denoted M), 22 for parsing the spatial heterogeneity of injury in persons by comparing 1 patient to a group of controls and found that increased MVF was associated with injury severity and worse long-term functional and cognitive outcomes. Although MVF predicted cognitive outcomes such as EF and PS, it failed to predict VL significantly, which may be related to the application of M in whole-brain WM ROIs, including regions not specifically related to memory and language. Previous studies on specific WM pathways have also established an association of increased FW with poor outcomes in various brain disorders. 52,55 –57
Taylor and colleagues 23 showed that Mstd-FA measured from various WM tracts in acute stages of mild TBI was associated with cognitive functioning. Our patient cohort scanned in the chronic stages of moderate-to-severe TBI revealed that Mff-FA, but not Mstd-FA, was correlated with EF. These differences could be attributable to the differences in TBI severity, choice of WM atlases, and application of FW correction on the DTI data. In contrast to Mstd-FA, Mstd-MD predicted EF and PS 12 months post-injury. We also noted differences in standard FA (decreased), MD (increased), and ff-FA (decreased and increased) in 90 WM regions studied in patients compared to controls. FW correction leaves ff-FA sensitive to detecting cellular pathological alterations. Standard FA and MD are obscured by FW, and we cannot conclude that these findings are related to TBI pathology. The patient-specific summary scores of all diffusion measures correlated with duration of PTA. Of the potential diffusion measures investigated, MVF performed the best in predicting the long-term functional and cognitive outcomes and correlated with injury severity in patients with TBI. In the future, MVF may act as an imaging-based marker to help guide clinical decisions to improve patient prognosis.
Longitudinal analyses of MVF showed an increase from 3 months to 1 year post
Limitations of our study include relatively small sample size, and to use a patient-specific summary score of FW-VF as a prognostic biomarker, studies in larger samples must be tested to be used for precision medicine. Given that data from large data sets like multi-center Transforming Research and Clinical Knowledge in TBI (TRACK-TBI) 58 become publicly available, creation of large sets of control data by data harmonization 59 can further refine MVF into a subject-specific biomarker. This sample of patients were initially scanned during the chronic stage of TBI (3 months), whereas the need for prognostic prediction is early after injury. Future studies investigating inflammatory, BBB disruption, and axonal damage processes by FW-VF in earlier stages of TBI are warranted.
Conclusion
In conclusion, we identified a promising DTI biomarker based on a patient-specific summary score of FW-VF, which characterized injury severity and predicted functional and cognitive outcomes in patients with moderate-to-severe TBI. Our findings are an important step toward implementing personalized therapy and rehabilitation planning for TBI patients.
Footnotes
Acknowledgments
We thank patients and their families for the time and effort they have dedicated to our research.
Authors' Contributions
Drs. Verma and Kim had full access to all the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis. Concept and design: Vijayakumari, Parker, Osmanlioglu, Kim, Verma. Acquisition of data: Whyte, Kim. Analysis, or interpretation of data: Vijayakumari, Parker, Osmanlioglu, Alappatt. Drafting of the manuscript: Vijayakumari, Parker, Osmanlioglu. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: Vijayakumari, Parker, Osmanlioglu, Alappatt. Obtained funding: Kim. Supervision: Diaz-Arrastia, Kim, Verma.
Funding Information
This work was supported by the National Institutes of Health (NINDS R01NS065980; PI: Junghoon J. Kim).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.