
Abstract
Susceptibility weighted imaging (SWI) and resting state functional magnetic resonance imaging have been highlighted as two novel neuroimaging modalities that have been underutilized when attempting to predict whether a child with concussion will recover normally or have a delayed recovery course. This study aimed to investigate whether there was a difference between children who recover normally from a concussion and children with delayed recovery in terms of SWI lesion burden and resting state network makeup. Forty-one children who presented to the emergency department of a tertiary level pediatric hospital with concussion participated in this study as a part of a larger prospective, longitudinal observational cohort study into concussion assessment and recovery. Children underwent neuroimaging 2 weeks post-injury and were classified as either normally recovering (n = 27), or delayed recovering (n = 14) based on their post-concussion symptoms at 2 weeks post-injury. No participants showed lesions detected using SWI; therefore, no group differences could be assessed. No between-group resting state network differences were uncovered using dual regression analysis. These findings, alongside previously published work, suggest that potential causes of delayed recovery from concussion may not be found using current neuroimaging paradigms.
Introduction
Concussion and mild traumatic brain injury (mTBI) are common during childhood, comprising almost 90% of all pediatric brain injuries. 1,2 A recent estimate of the incidence rate of concussion in American children, is between 1.1-1.9 million per year. 3 While most children will recover from their concussion within 2 weeks, 11-30% continue to experience symptoms 3 months or longer after injury, 4 –7 leading to school absences, social withdrawal, and increased family stress. Early detection of those children that are more likely to suffer a delayed recovery from concussion would facilitate earlier intervention, and reduce the negative impacts associated with a protracted recovery course.
Concussion, as defined by the Concussion in Sport Group's (CISG) Berlin Consensus statement, 8 is a traumatic brain injury induced by biomechanical forces that results in short-lived impairment of neurological functioning (e.g., headache, dizziness, nausea). If concussion symptoms last for longer than a 2-week period, they are termed persistent post-concussive symptoms (PPCS) and may require intervention by trained clinicians. 9 The symptoms of concussion are reflective of a functional disturbance rather than a structural injury. Therefore, by definition, a concussion has no neuroimaging correlate on conventional structural neuroimaging. 8 However, researchers have utilized novel neuroimaging techniques to explore potential neurobiological correlates for post-concussion symptoms. A recent literature review 10 discussed the use of novel structural and functional imaging in the context of mTBI and concussion; with two MRI modalities—susceptibility weighted imaging (SWI) and resting state functional magnetic resonance imaging (rs-fMRI)—highlighted as having particularly disparate findings.
Susceptibility-weighted imaging
Susceptibility weighted imaging (SWI) is a structural MRI sequence that has the ability to detect the paramagnetic signature of hemosiderin deposits remaining after red blood cells have pooled and broken down in brain parenchyma. 10 These deposits are therefore reflective of previous bleeding events and can be used as evidence of prior damage to blood vessel integrity, which can occur during a concussive head strike; Beauchamp and colleagues 11 demonstrate that SWI can detect microbleeds that are not identifiable on standard neuroimaging. Most studies reporting SWI imaging data in the context of pediatric concussion have been limited to qualitative analysis of their findings. 10,12 -14 Studies utilizing SWI with quantitative methods do so in the context of mixed-severity brain injury samples and do not differentiate the efficacy of SWI for concussion. 15,16 Moreover, many studies that report on SWI findings in pediatric concussion have very low sample sizes such that the median sample size for studies reviewed by Rausa and colleagues, 10 which reported SWI findings, was only 12 participants. Einarsen and colleagues 17 used SWI as a part of their model predicting delayed recovery from concussion in an adult population, although this was of limited success, and the study did not report the unique contribution of SWI to the model. To the authors' knowledge, no study to date has ascertained whether the difference in recovery time between children with normal recovery and delayed recovery can be explained by the presence and prevalence of SWI lesions.
Resting-state functional magnetic resonance imaging
Resting state functional magnetic resonance imaging (rs-fMRI) utilizes the close coupling of blood oxygenation and brain activation to estimate the strength of connectivity of neural networks while the brain is at rest. Several studies have used rs-fMRI in the context of pediatric concussion and have shown that, relative to controls, concussed children show alterations in functional connectivity in the occipital pole visual network, 18 the cerebellar network, 18 executive function network, 19 ventral attention network, 19 and the “posterior and anterior brain regions.” 20 There are conflicting accounts as to whether the default brain network is similarly affected. 18,19,21 Recently, in a clinical trial, Iyer and colleagues 22 demonstrated that children with delayed recovery from concussion showed an increase in functional connectivity within the anterior default mode network and limbic regions, compared with those who recovered as a part of their active melatonin supplementation trial. This would suggest a possible resting state functional imaging correlate of delayed recovery from concussion. However, more research is needed outside of the context of an intervention trial to establish this effect. 9
As yet, there is no objective method by which to diagnose a child with PPCS. Zemek and colleagues 7 developed a PPCS risk score based on a combination of patient demographics and symptom profile; however, it suffers the same limitation of all current PPCS diagnostic tools—namely, there is no objective marker of disease pathology by which to validate the scoring system. Our study's aim was to investigate the structural and functional differences between children who recover from concussion normally, and those with delayed recovery, in an attempt to locate a neuroimaging correlate of PPCS. We hypothesized that: 1) children with delayed recovery would have a higher SWI lesion burden compared with children with normal recovery, and 2) there would be a significant difference in the resting state networks between normally recovering children and children with delayed recovery.
Method
Design
This study formed part of a larger prospective, longitudinal study (Take CARe Biomarkers—Concussion Assessment and Recovery research) 23 conducted at The Royal Children's Hospital (RCH), a tertiary level pediatric hospital in Melbourne, Australia. The study recruited and assessed children presenting with concussion to the hospital emergency department (ED), and performed follow-up in person assessments at 1-4 days, 2 weeks, 1 month (if symptomatic), and 3 months post-injury. Multiple domains were assessed at each time-point (concussive symptoms, neurocognition, behavior, quality of life, fatigue, etc.), with neuroimaging acquisition occurring at the 2-week assessment. The full Take CARe study protocol can be found in Takagi and colleagues 23 with the results of the diffusion-based neuroimaging analysis previously reported in Shapiro and colleagues. 24
Participants
Participants were a subset (n = 45) of the Take Care Biomarkers concussion sample that underwent neuroimaging. 25 Concussion was defined as per the CISG Berlin Consensus Statement. 8 Table 1 outlines the inclusion and exclusion criteria for this study.
ED, emergency department.
Participants above the age of 12 years and their parents/guardians gave written informed consent to participate in the study at the time of recruitment. For children 12 years and younger, written informed consent was obtained from the parent/guardian and verbal assent from the child. Ethics approval for this study was given by The RCH Human Research Ethics Committee.
One participant was excluded from the sample due to poor-quality image acquisition caused by their orthodontic braces and another participant was excluded due to MRI acquisition error; these participants were excluded listwise. One participant was excluded pairwise from the SWI analysis due to poor quality image acquisition and two participants did not complete the rs-fMRI protocol. This left a final sample of n = 42 participants in the SWI analysis and n = 41 participants in the fMRI analysis.
Measures
The Post-Concussive Symptoms Inventory (PCSI) 26 is a self-report measure of post-concussive symptoms with strong psychometric properties. 27 It includes both a parent and child self-report Likert scale endorsing levels of post-concussive symptomology, with age-appropriate versions of the child self-report scale adjusted for younger (5-12 years) and older (12-18 years) children.
All imaging was conducted on a research-dedicated 3T Siemens Magnentom TimTrio running B17 software with a 32-channel head coil. Structural T1-weighted, motion corrected, 3D magnetization-prepared rapid acquisition gradient echo imaging was acquired; repetition time (TR) = 2530 msec, echo time (TE)1 = 1.77 msec, TE2 = 3.51 msec, TE3 = 5.32 msec, TE4 = 7.30 msec, inversion time (TI) = 1260 msec, flip angle = 7°, matrix size = 256 × 256, field of view (FOV) = 230.00 × 208.38 mm, voxel size = 0.9 × 0.9 × 0.9 mm3, sagittal slice orientation, total acquisition time = 6 min 52 sec. In the same session, SWI imaging was acquired with a slice thickness = 1.75 mm, TR = 48 msec, TE1 = 12.3 msec, TE2 = 39.36 msec, voxel size = 0.9 × 0.6 × 1.8 mm, flip angle = 90°, number of averages = 1, FOV = 230 mm, acquisition time = 5 min 52 sec. Resting state fMRI was acquired with a single 6 min 33 sec acquisition with: TR = 1500 msec, TE = 33.0 msec, echo spacing = 0.69 msec, multi-band acceleration factor = 3, number of slices = 60, slice thickness = 2.5 mm, voxel size = 2.5 × 2.5 × 2.5mm, FOV = 255 mm, flip angle = 85°, temporal high-pass filter = 4, acquisition time = 6 min 33 sec.
Procedure
The study procedure has been previously published. 24 In brief, patients were screened in the ED by trained research assistants (weekdays 9 am-10 pm, weekends 12 pm-10 pm). If a patient met the inclusion criteria and their treating physician confirmed their eligibility, families were approached to participate in the study.
Once consent was granted, pre-injury and demographic information were obtained from parents in the ED and parent and the child completed the PCSI. Injury-related information was obtained from the treating clinician. Participants were then followed up, either by attending a concussion clinic in person or by responding to questionnaires online, at the 1-4 day, 2-week, 1-month (if symptomatic), and 3-month time-points. For those attending the concussion clinic in person, neuroimaging was acquired at the 2-week time-point for all participants (range = 9-24 days post-injury). Participants were classified as normally recovering (n = 27) or delayed recovering (n = 14) at the 2-week time-point. Children were classified as having a delayed recovery if, at the 2-week period, parent responses on the PCSI showed that two or more of the child's symptoms showed increased severity when compared with reported pre-injury levels, in accordance with the criteria set out in Hearps and colleagues. 9
Statistical analysis
SWI analysis
SWI lesions were identified using a publicly available semi-automated SWI lesion detection tool (CMBdetection-LupoLab) created by the Department of Radiology and Biomedical Imaging at the University of California San Francisco. 28 Training data provided with the SWI lesion detection toolkit were created on adult brain tumor patients with radiological evidence of cerebral microbleeds following radiation therapy, and as such it was deemed necessary to create training data based on the current dataset to ensure the detection tool was properly calibrated. Lesion count and size were compared between the normally recovering children and the children with delayed recovery.
Rs-fMRI analysis
Resting state fMRI images were preprocessed using FSL MELODIC independent component analysis (ICA): motion correction was applied using MCFLIRT, followed by 5 mm full width half maximum spatial smoothing, and high-pass temporal filtering. 29,30 Single session ICAs were conducted on each participant with variance-normalized time-courses and unconstrained automatic dimensionality estimation. Component maps were thresholded at 0.5. The component maps for all subjects were visually inspected with noise artifacts removed from the data using FSL_regfit. The images were then registered in one step from subject space to MNI standard space using FSL packages FLIRT, FNIRT, and applywarp. 30 The cleaned subject data was then combined to generate a group average ICA for all 127 remaining components using FSL's MELODIC before being prepared for group level analysis using dual regression (FSL's dual_regression). FSL's permutation testing tool Randomize 31 was used using default parameters to assess whether there was a difference in the resting state networks between normally recovering children and children with delayed recovery as a part of the dual_regression package. Figure 1 displays the rs-fMRI analysis pipeline as a flow diagram.
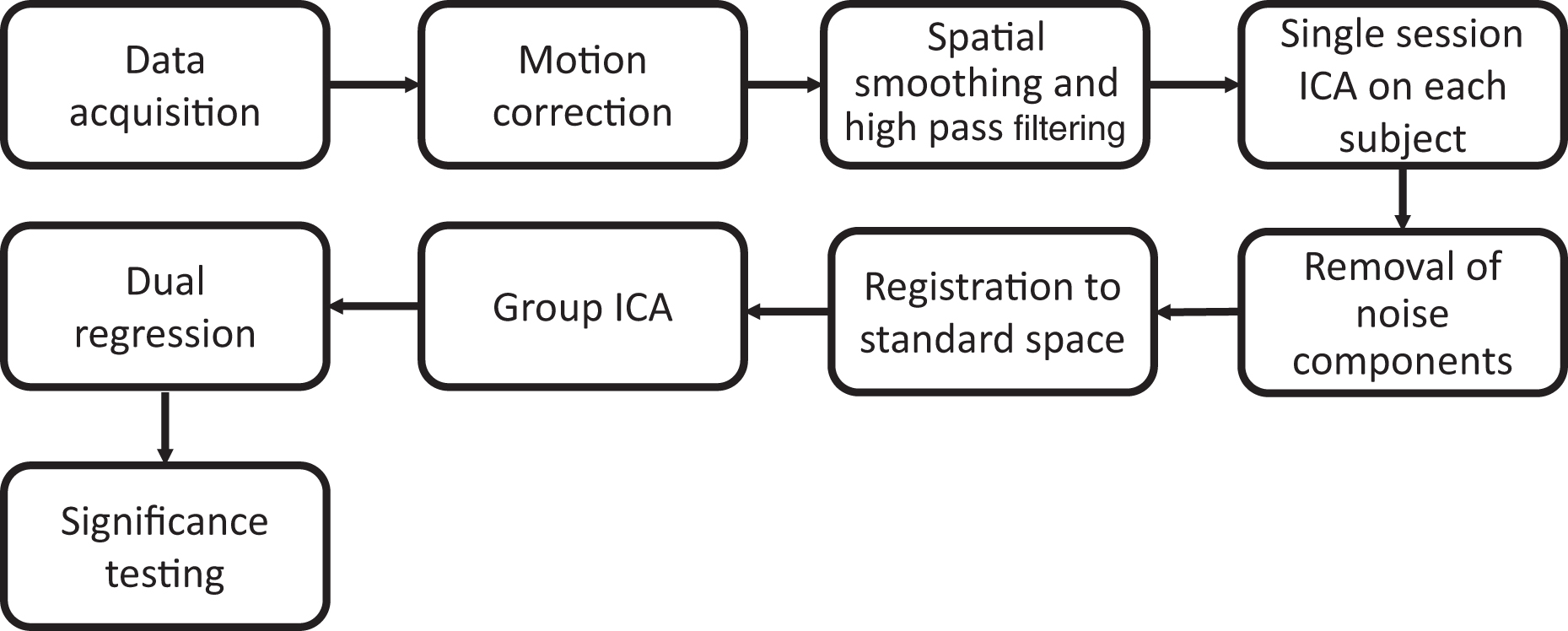
Flow diagram of resting state functional magnetic resonance imaging analysis pipeline.
Results
Participant demographic information is presented in Table 2. On visual inspection, none of the participants were found to have lesions on SWI, which was confirmed by a certified neurosurgeon. We were therefore unable to use the semi-automated SWI lesion detection toolkit because there were insufficient data to train the SWI lesion classifier.
Age, number of days between recruitment and imaging, and number of previous concussions analyzed with independent samples t tests. Sex, Handedness, CT scan analyzed with χ 2 tests. Method of injury not analyzed due to participants belonging to multiple groups and missing data.
SD, standard deviation; M, mean.
For the resting state functional connectivity, dual regression independent component analysis was unable to find significant differences between normally recovering children and children with delayed recovery in any of the 127 group level components (p > 0.05).
Discussion
This study aimed to investigate the structural and functional neuroimaging differences between children who recover from concussion normally and those with delayed recovery. We hypothesized that children with delayed recovery would have a higher lesion burden as compared with normally recovering children, and there would be a significant difference between normally recovering children, and children with delayed recovery in terms of resting state network activation. There were no SWI lesions detected with which to conduct a comparison between the normal and delayed recovery groups. No significant difference was found in the resting state networks between the normally recovering group and delayed recovery group.
There is ongoing debate as to whether SWI imaging is sufficiently sensitive to acutely identify lesions in concussed children who present to the ED. On the one hand, Beauchamp, and colleagues 11 detected lesions on SWI imaging in six children with mTBI that were not detected with standard CT or MRI, as well as detecting lesions in six other children with mTBI who did not undergo CT imaging in the ED. In a follow up study, Beauchamp and colleagues 16 found that in their sample of 58 children with mTBI, 19% had lesions detected using SWI when imaged 2-8 weeks post-injury. On the other hand, Babcock and colleagues 12 did not find any SWI lesions in their sample of children with mTBI when imaged within 96 hours of injury, while Wilde and colleagues 32 found only one child with mTBI who showed evidence of a SWI lesion on scanning, however this child also showed evidence of cerebral hemorrhagic contusion on standard clinical MRI, which according to the Berlin consensus statement 8 would indicate that the injury was more severe than a concussion.
This study utilized a homogenous sample of children with concussion, consistent with the CISG definition, 8 and as such did not include any children with positive findings on computed tomography. Thus, it is possible that the presence of SWI lesions found in previous studies supports the notion that mTBI is a separate and more severe injury compared with concussion, as defined by the CISG.
It can be concluded that for children who present to the ED with concussion, SWI is unlikely to be clinically useful in diagnosis or tracking of recovery, given current technological capability, a conclusion which is in line with Bonow and colleagues. 33 While this conclusion goes further than that made by our recent systematic review into neuroimaging and mTBI, 10 it should be highlighted that this study specifically recruited children who met the criteria for diagnosis of concussion, 8 and not those that meet the criteria for non-concussive mTBI. While there is significant overlap between the criteria, it is beyond the scope of this paper to comment on the utility of SWI for use in patients with mTBI as it is possible that positive relationships between SWI lesions and recovery are more likely when more severe mTBIs are sampled.
This study did not establish a difference in resting state brain networks between normally recovering children and children with delayed recovery. This finding gives further weight to the findings by Iyer and colleagues 22 by suggesting that the cause of the increased functional connectivity within anterior default mode network and limbic regions shown in children with delayed recovery from concussion is not related to changes in the network makeup itself. At this stage, there is insufficient literature utilizing resting state functional neuroimaging to interrogate delayed recovery from concussion. While there is some literature demonstrating neural activation changes using task-based fMRI paradigms in children with delayed recovery compared with normally recovering children, 34,35 more research is required to assess whether these changes in the active brain are reflected in the resting state brain as well.
Although this study did not demonstrate a difference between normally recovering children and delayed recovery children resting state network makeup, it is important to note that as there was no healthy control sample to compare with, it cannot be assumed that a control group's resting state network makeup would be similar to these groups' results. While it may be argued that children who have symptomatically recovered from concussion should show a recovery in terms of their resting state networks as well to approach that of healthy children, this study cannot demonstrate that this is the case, and therefore can make no comment as to how these rs-fMRI findings compare to healthy children. Further, while this study has a relatively large sample of concussed children, it is possible that it was still insufficient to detect significant differences between the groups. This limitation further emphasizes the need for coordinated multi-site collaborations to ensure future studies are sufficiently powered.
This study employed a robust prospective, longitudinal cohort design, gold standard concussion definition, standard assessment protocols (imaging, symptom reports, recovery classification) conducted at consistent time points post-injury and state-of-the-art imaging technology. Despite this, we failed to demonstrate a difference in rs-fMRI or SWI metrics between children recovering normally from concussion, and children with delayed recovery, measured at a 2-week time-point. The current findings add to our previous research that demonstrated no difference between the groups in terms of diffusion imaging metrics as well. 24 In summary, this study was unable to detect a SWI or rs-fMRI correlate of PPCS. It is suggested that causal factors behind delayed recovery from concussion in pediatric populations may not be identifiable using current neuroimaging techniques/paradigms.
Footnotes
Acknowledgments
This study has been approved by the Human Research Ethics Committee of the Royal Children's Hospital Melbourne.
Authors' Contributions
Jesse Shapiro, Vicki Anderson, Franz Babl, Michael Takagi, Marc Seal: Drs. Anderson, Takagi, Babl, and Seal conceptualized and designed the study, Mr. Shapiro analyzed the data and drafted the initial manuscript.
Stephen Hearps, Nicholas Anderson, Cathriona Clarke, Gavin A Davis, Kevin Dunne, Vera Ignjatovic, Marc Seal, Tim Silk, and Vanessa Rausa made substantial contributions to the conception of the study, the acquisition of data, and critically revising the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding Information
The study is funded by a project grant from Royal Children's Hospital Foundation, Melbourne, Australia (2014-370). Near miss funding from the Clinical Sciences Theme, MCRI. Murdoch Children's Research Institute is supported by the Victorian Government's Operational Infrastructure Support Program. Hearps was funded by an Australian National Health and Medical Research Council (NHMRC) Development grant; Babl was funded by the Royal Children's Hospital Research Foundation, an NHMRC Practitioner Fellowship, and a Melbourne Campus Clinician Scientist Fellowship; and Anderson by an NHMRC Senior Practitioner Fellowship. The funding organizations did not have a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.